
Abstract
To support the global strategy to reduce risk factors for obesity, we synthesized the evidence on physical activity (PA) and sedentary behaviour in the Middle East and North Africa (MENA) region. Our systematic overview included seven systematic reviews reporting 229 primary studies. The meta-analysis included 125 prevalence measures from 20 MENA countries. After 2000, 50.8% of adults (ranging from 13.2% in Sudan to 94.9% in Jordan) and 25.6% of youth (ranging from 8.3% in Egypt to 51.0% in Lebanon) were sufficiently active. Limited data on PA behaviours is available for MENA countries, with the exception of Gulf Cooperation Council countries. The meta-regression identified gender and geographical coverage among youth, and the PA measurement as predictors of PA prevalence for both adults and youth. Our analysis suggests a significant PA prevalence increase among adults over the last two decades. The inconsistency in sedentary behaviour measurement is related to the absence of standardized guidelines for its quantification and interpretation. The global epidemic of insufficient PA is prevalent in MENA. Lower PA participation among youth and specifically females should be addressed by focused lifestyle interventions. The recognition of sedentary behaviour as a public health issue in the region remains unclear. Additional data on PA behaviours is needed from low- and middle-income countries in the region.
Similar content being viewed by others


Introduction
Non-communicable diseases (NCDs) kill 41 million people worldwide each year – equivalent to 71% of all deaths1. The Middle East and North Africa (MENA) region has one of the highest rates of NCDs in the world. In 2017, the region reported the second highest prevalence of diabetes in the world (10.8%)2 and is recording a rapid increase in obesity3,4. Insufficient physical activity (PA) and sedentary behaviour are key risk factors for obesity and other NCDs5,6,7,8,9,10,11,12,13,14,15 leading to premature mortality10,11,16,17,18. It has been suggested that PA has the potential to effectively control and reduce the burden of obesity during the various phases of human development19. Regular PA can also improve self-esteem, cognitive performance, and academic achievement in young people7,20,21 and is positively related to cardiorespiratory and metabolic health6. Recently, sedentary behaviour has received global attention as prolonged sedentary time is associated with an increased risk of chronic disease and an increase in all-cause mortality, regardless of individuals meeting the recommended levels of PA13,15.
The World Health Organization (WHO) and the Global Observatory for Physical Activity (GoPA) are targeting a relative reduction of 10% in the global prevalence of physical inactivity among adults by 202522,23. Currently, one of the most pressing needs to improve population health is to develop appropriate policies and implement interventions to address the global pandemic of physical inactivity24,25. However, to support this action, country-level evidence on PA behaviour in various population groups is essential. Both regional-and country-level data contribute to the continuous surveillance of PA participation and are essential to track progress towards the global PA target.
In the MENA region, the proportion of the population not engaging in sufficient levels of PA (as per the recommendation of standardized international guidelines) remains unclear. Recent reports indicate physical inactivity prevalence measures of 32.8% for adults across the MENA and Central Asia regions26 and 78.4% in boys and 84.4% in girls globally25. However, gender-stratified measures in adults and youth are needed to develop evidence-based interventions informed by local data.
The aim of our study is to: 1) synthesize evidence from published systematic reviews (SRs) on PA behaviour in MENA countries, 2) quantify country-specific PA prevalence measures and assess demographic variations among youth and the general adult population within the region, 3) summarize measurement variations of PA and sedentary behaviour in the region, and 4) identify research gaps and provide specific recommendations pertaining to PA for the region. We tested the following null hypotheses that there is no difference in the PA prevalence between males and females, before and after 2000, and among nationals and non-nationals in the Gulf Cooperation Council countries (GCC).
Methods
We conducted a systematic overview of published SRs on PA and sedentary behaviour in the MENA region. The current review is a co-product of a protocol planned for a systematic overview reporting the grey literature in systematic reviews on population health in the Middle East and North Africa (PROSPERO registration number CRD42017076736)27,28. This manuscript follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (Supplementary, Table S1)29, and the Preferred Reporting Items for Overviews of Systematic Reviews (PRIO-harms) tool (Supplementary, Table S2).
Search strategy and selection criteria
A broad search strategy was developed to systematically identify any type of review on all health issues in any MENA country. Search terms related to countries’ names, MENA populations’ names, and MENA sub-regions’ names, such as North Africa, East Africa, and the Middle East, were used. No restrictions to a specific health condition or intervention and language of publication were applied at this stage. The full search strategy with search criteria is available in the published overview protocol27. Two independent reviewers (AA and HA) systematically searched the Medical Literature Analysis and Retrieval System Online (MEDLINE) through the search engine PubMed. We included publications since 2008 – the publication year of the first version of the Cochrane Handbook for Systematic Reviews of Interventions30 up to February 21, 2017. Additionally, we also searched grey and non-grey literature sources with no date or language restriction including Google Scholar, Epistemonikos, ProQuest, OpenGrey, Bioline International, E-Marefa, ALMANHAL platform, governmental websites of all MENA countries, and the WHO website for systematic reviews relevant to our topic. The literature search was then updated to identify recent SRs published up to November 2019.
A systematic review (SR) was defined as a literature review that has explicitly used a systematic literature search of at least one electronic database to identify all studies that meet pre-defined eligibility criteria along with a study selection30. Reviews not reporting a systematic methodology, such as narrative reviews, were excluded.
Based on the relevance of grey literature in the region when studying population health outcomes27,31, we included MENA countries where Arabic, English, French, and/or Urdu are the primary official languages and/or the medium of instruction in the colleges/universities. These languages are also those spoken by the authors of this overview (see the overview’s protocol27). The 20 MENA countries included are Algeria, Bahrain, Djibouti, Egypt, Iraq, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Pakistan, Palestine, Qatar, Saudi Arabia, Sudan, Syria, Tunisia, the United Arab Emirates (UAE), and Yemen.
Data screening
Records were downloaded into Endnote (version X8.2), and duplicates were removed. Using Rayyan software32, two independent reviewers (AA and HA) conducted the multi-stage screening following a standard process. Discrepancies in the inclusion of SRs were resolved through discussion, with the involvement of a third reviewer (AA, HA, and KC).
Retrieved SRs were then categorized based on the reported population health outcome. For the purpose of this overview, we included any SR reporting measurable PA-related outcomes including physical activity or inactivity prevalence and/or sedentary behaviour pertaining to MENA population of any age group residing in a MENA country.
Data extraction
Data extraction was conducted by SC1 and checked for accuracy by KC. Extracted data included characteristics of the included SRs as well as the primary studies and were matched to PICOTS items (Population, Outcomes, Time of the study and Setting; Control and Intervention were not applicable to our overview question). From each included SR, the following characteristics were extracted: literature search terms and time period, geographical coverage, data literature sources, MENA countries with retrieved data, along with the number of included studies, inclusion and exclusion criteria, targeted review population, and reported PA-related outcomes. From each primary study included in a SR, the following characteristics were collected: study design and sample size, sampling method, study setting, years of data collection, population characteristics (type, age, gender, proportion of males and females, and response rate), and all PA-related outcomes (definition, measurement tool/administration, prevalence, and barriers to PA). In case of discordance between the reported data by the SR and data available in the primary study, the latter was retained. A consensus meeting with SC1, KC, and SC2 was held to resolve any disagreements.
In order to assess the methodological quality of the included primary studies and conduct the quantitative analyses, any relevant study characteristics not reported by the SR were extracted from the primary study publication. In addition, any additional data on PA-related outcomes from a MENA country found in an included primary study but not reported by the SR (usually not part of the objectives) was extracted and reported.
Qualitative synthesis
The qualitative synthesis was done at two levels:
Qualitative synthesis of the SRs’ data
A summary of the geographical coverage, the methodology used by each SR, the main conclusions on reported outcomes, limitations and strengths, research gaps, and recommendations from each SR were synthesized in Supplementary, Tables S3 and S4. A synthesis of the methodological quality of the included SRs and our own overview was conducted.
Qualitative synthesis of the primary studies data
The characteristics of primary studies that reported PA in the SRs were synthesized. These included physical inactivity prevalence measures and/or sedentary behaviour data among youth (≤19-year-old) and adults (>19-years-old). If these were not reported, the prevalence of the outcome among the total study population (males and/or females) was calculated using raw data available in the primary study.
We synthesized the measurement tools and definitions of PA, physical inactivity and sedentary behaviour used by the primary studies as well as the characteristics of the study population and the official primary language of the MENA country where the study was conducted. These characteristics were contrasted with the population and linguistic validation parameters of each used tool. A measurement tool was considered to be validated in a specific population or language if a validation record in the same population or language was retrieved in the literature. The objective of this synthesis was to review the variability in the outcome measurements and appropriateness of their use in the primary study population33.
Quantitative synthesis
By definition, a participant who does not meet the PA recommendations of 150 min of moderate physical activity/week or equivalent for adults and 60 min of moderate to vigorous PA daily for youth or equivalent is considered physically inactive and vice versa. Hence, in all included studies reporting physical inactivity outcomes, participants who did not meet the physical inactivity criteria were considered meeting the recommended level for PA. These measures were included in the meta-analysis as a PA-prevalence measure as long as they were not overlapping with other included data in the meta-analysis. The “poor level”, “mild level” or “low score” of PA was reported in some studies where there was a low PA participation level (lower than standard thresholds)34,35,36. These PA prevalence measures were considered as physical inactivity prevalence measures. All physical inactivity prevalence measures along with reasons for conversion or non-conversion to a PA prevalence measures are listed in Supplementary, Table S5. When two levels of PA (moderate and vigorous) were reported in the same study34,36, both levels were merged to one level of PA.
A meta-analysis of PA prevalence (proportion of participants meeting recommended levels of PA as defined by the primary studies) was conducted for the MENA countries for which data was available. The GCC subregion includes the following countries: Bahrain, Qatar, Oman, Kuwait, Saudi Arabia, and UAE. The PA-prevalence measures stratified by gender and age were prioritized for the inclusion in the meta-analysis rather than the overall measures for the entire study population. As there is no consensus on the standard definition and a threshold to quantify sedentary behaviour, no meta-analysis was conducted for this outcome. A publication of a primary study included in more than one SR and/or publications with overlapping data points were included once and all the replicates were excluded from the meta-analysis. A list of primary studies excluded from the meta-analysis with reasons is detailed in Supplementary, Table S6.
A subgroup meta-analysis of PA participation by gender (males and females) and year of data collection (before 2000 and after 2000) was then conducted for the MENA and GCC regions and for each MENA country with available data. A high proportion of the population residing in the GCC is non-national37; while in the other MENA countries, the populations are predominantly nationals. Therefore, meta-analyses according to the type of population (national population and mixed populations of nationals and non-nationals) were relevant for GCC countries only.
The threshold of data collection time was established at the year 2000 based on the demographic, socioeconomic, migration background in the GCC countries37,38, urbanization, and lifestyle transition observed in many MENA countries by the beginning of the 21st century39,40,41,42. For the PA prevalence measures where the year of data collection was missing, we considered this as prior to the publication year and the prevalence measure was then classified accordingly for the analyses.
If not reported, the total or strata sample sizes were calculated based on the percentage of males and females in the sample. Random effects modelling was used to conduct the meta-analyses. We generated forest plots using the ‘meta/metaprop’ package in R (version 3.5.0) and inspected them visually to assess the variability of prevalence estimates across subgroups. Furthermore, the heterogeneity of the prevalence estimates was assessed using: (1) the I2 statistic, (2) the Cochran’s Q statistic, and (3) the Cochran’s Q between-subgroups. The I2 statistic was used to describe the percentage of variability in the prevalence estimates resulting from the between-study heterogeneity rather than chance43. The statistical significance (p-value < 0.05) of the Cochran’s Q statistic was used to test for evidence of the overall heterogeneity between prevalence estimates44. The statistical significance (p-value < 0.05) of the Cochran’s Q between-subgroups statistic was used to test for differences between prevalence estimates across subgroups45. The prediction interval estimated the 95% interval in which the true PA prevalence in a new PA prevalence study will lie.
To continue exploring the statistical heterogeneity, univariable random-effects meta-regression analyses were conducted to identify associations of higher PA prevalence and sources of between-study heterogeneity. Associations were assessed using odds ratios (ORs), 95% Confidence Intervals (CIs), and t-tests. Relevant covariates were specified a priori and included in the models separately: gender (males vs. females), years of data collection (after 2000 vs. before 2000), geographical coverage (country level vs. local level), and PA measurement tool (standard tools vs. non-standard tools). Standard PA measurement tools included: 1) the pedometer, accelerometer and continuous heart rate monitor (gold standard tool), and 2) validated PA questionnaires among adults and youth included the International Physical Activity Questionnaire (IPAQ), the Global Physical Activity Questionnaire (GPAQ), the Arab Teens Lifestyle Student Questionnaire (ATLS), the Nurses’ Health Study II Activity and Inactivity Questionnaire (NHS II-PAQ), “How physically active are you” questionnaire, the Health Behaviour in School-aged Children Survey (HBSC), and the Adolescent Physical Activity Measure Questionnaire (PACE+)46. Any other used measurement tool that was not included in the National Institutes of Health (NIH) Database of Standardized Questionnaires About Walking & Bicycling or does not reference to a published validation study of the used tool was considered as non-validated measurement tool.
Factors with p-value <0.05 in the univariate meta-regression were considered as statistically significant covariates. These covariates were explored separately in the adult and youth MENA general populations. Meta-analyses and meta-regressions were conducted using the ‘meta/metareg’ package in the R software (version 3.5.0).
Methodological quality assessment
The methodological quality of the included SRs and primary studies was assessed by two independent reviewers.
The AMSTAR measurement tool47 was used by two independent reviewers (SC1 and AA) to perform the quality assessment of the included SRs. Discrepancies were resolved through discussion, with the involvement of a third reviewer (SC1, AA, and KC) when necessary. The methodological quality of the included SRs was then discussed according to the 11 criteria of the AMSTAR checklist48.
At primary study-level, an adapted quality assessment checklist was developed based on the PICOTS framework49 and other published tools utilized for similar contexts50,51,52,53,54,55. Our quality assessment checklist included criteria related to outcome definition, outcome measurement, population characteristics, and sampling method since the quality of PA and sedentary behavior measures are directly related to the study’s quantification method and its population characteristics. We utilized the guidelines of the World Health Organization (WHO), the Physical Activity Guidelines Advisory Committee, the Centers for Disease Control and Prevention (CDC), the American College of Sports Medicine, and the Sedentary Behavior Research Network (SBRN) to establish a list of standard definitions and valid methods utilized for PA-participation assessment. The detailed checklist and the definition of each criterion and the scoring system is presented in Supplementary, Table S7. Each of the seven included criteria was rated with a maximum score of three (0 = “Not defined”, 3 = “Clearly defined and appropriate”). Hence, a maximum quality score of 21 can be reported for one assessed PA-related outcome. The PA-related outcomes in each population subgroup were evaluated and scored by SC1 and checked by KC. Any discrepancies were resolved by discussion with the involvement of a third reviewer (SC1, KC, and SC2). The higher the quality score that was reported, the better the methodological quality of the reported outcome.
Results
A total of seven SRs and 229 primary studies on the epidemiology of PA, physical inactivity, and/or sedentary behaviour in at least one of the 20 selected MENA countries were included in the qualitative synthesis of this overview (Fig. 1). After exclusion of primary studies included in more than one SR (n = 15), primary studies with overlapping data (n = 8), primary studies reporting only sedentary behaviour data or barriers to PA data (n = 65), and those using non-standard definitions for PA or inactivity, excluded from the meta-analyses (n = 59), a total of 82 studies, including 125 PA prevalence measures were considered for the quantitative analyses.

PRISMA 2009 flowchart of the systematic reviews inclusion.
Characteristics of the included systematic reviews
The seven SRs included in our overview are described in Supplementary, Table S3. The summary of qualitative results, strengths and limitations, research gaps, and recommendations are synthesized in Supplementary, Table S4. PA-related outcomes were found for all the 20 MENA countries. The physical inactivity and sedentary behaviour measures were the primary outcomes in three SRs54. The other SRs reported these outcomes only if included in the primary studies on PA. No SR restricted the primary study inclusion to one specific definition of PA. All the identified data was based on the general population. Of note, only Yammine et al.56 conducted a meta-analysis of prevalence measures of different levels of PA among UAE adolescents. All the included SRs excluded clinical populations and three SR53,57,58 excluded primary studies based on their methodological quality of sampling and measurement methodology.
Methodological quality assessment of the included systematic reviews and primary studies
No SR reported the list of excluded studies, assessed publication bias, or included the source of funding for the SR itself and of the included primary studies, as per the AMSTAR recommendations48 (Table 1). Two SRs56,58 searched for grey literature sources (Table 1).
The checklist used for the quality assessment of the included studies is presented in Supplementary, Table S5. The quality assessment scores of each reported PA related outcome are reported in Supplementary, Tables S8–S11. The methodological quality scores varied between 11 and 20 out of a maximum score of 21. Most of the reported outcomes had a quality score closer to the upper score limit. Most of the primary studies were cross-sectional clearly describing the population characteristics and study setting, used PA definition consistent with international recommendations, utilized validated measurement tools, used probability-based sampling method, had an equal male and female ratio, and country-level coverage.
Overview of studies with physical activity data
Forty-seven primary studies with 75 PA prevalence measures on adults and thirty-five primary studies with 50 PA prevalence measures on youth were included in the meta-analysis. The study characteristics and PA prevalence measures among the adult and youth population are summarized in Supplementary, Tables S8 and S9.
For both populations, limited data on PA was reported in MENA countries with the exception of the GCC countries (Bahrain, Kuwait, Oman, Qatar, Saudi Arabia and UAE). In most included studies pertaining to GCC countries, the distinction between the national and non-national population was unclear. A wide range of PA prevalence measures were reported for the MENA region. A higher PA prevalence measure among males than females was observed for all included MENA countries except among adults in Lebanon and Jordan. Considering all retrieved data (before and after 2000) among adult males, the highest pooled prevalence measures of sufficient PA participation was found in Jordan [94.2% (95% CI = 93.1–95.2%) and the lowest in Bahrain [23.1% (95% CI = 20.9–25.5%)]. Among adult females, the highest pooled prevalence measures of sufficient PA participation were found in Jordan [95.5% (95% CI = 94.4–96.4%)], and the lowest in Bahrain 1.3% (95% CI = 0.7–2.3%) (Table 2).
The highest pooled prevalence measures of sufficient PA participation among youth males was observed in Kuwait [70.4% (95% CI = 66.0–74.5%)] and the lowest in Egypt [14.0% (95% CI = 12.5–15.6%)]. The highest pooled prevalence measures of sufficient PA participation among youth females was observed in Kuwait 39.3% (95% CI = 34.7–44.0%) and the lowest in Egypt 4.0% (95% CI = 3.1–5.1. %) (Table 3).
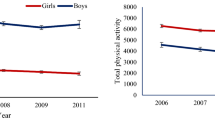
In most of the MENA countries among both adult and youth populations, more males engage in PA than females except for adults in Lebanon and Jordan (Tables 2, 3, Fig. 2). In MENA as a whole and within GCC countries, greater PA participation was observed among adults than in youth. However, caution must be practiced in interpreting these results given the limited number of included studies and the high heterogeneity between the included prevalence measures.

Map of the physical activity prevalence measures, using data collected after 2000: (A) In the adult MENA population, (B) in the youth MENA population, and (C) in the national GCC adult and youth populations. All PA data were collected after 2000. MENA countries with no PA prevalence measures among adults include Djibouti, Yemen, Bahrain, and Syria. MENA countries with no PA prevalence measures among youth include Algeria, Bahrain and Pakistan. Heterogeneity (I2) between the PA prevalence measures varied between 99.6–99.7% in adults and 99.2–99.4% in youth in MENA countries. Among GCC nationals, heterogeneity (I2) between the PA prevalence measures varied between 99.8–99.8% in adults and 99.0–99.5% in youth. N/A is used to indicate the non-availability of disaggregated prevalence data according to gender in (A,B) and age (adult/youth) in (C).
Only the SR of Yammine et al. 2016 pooled the PA prevalence measures among adolescents in the UAE56 for moderate and vigorous levels of PA [19.2% (95% CI = 18.5–19.9%, I2 = 98.6%) and 24.7% (95% CI = 23.2–26.3%, I2 = 97.8%)]. This pooled prevalence was higher among males than females for both moderate and vigorous levels of PA [ORpooled: 1.23% (95% CI = 1.13–1.35%, I2 = 89.5%) and ORpooled: 2.6% (95% CI = 2.14–3.14%, I2 = 84.5%), respectively]. Our pooled prevalence of both moderate and vigorous levels of PA in the UAE among youth was 36.0% (95% CI = 23.9–49.9%).
For adults, most studies used PA definitions consistent with international recommendations of i) at least 150 minutes of moderate-intensity activity per week or ii) at least 600 or more metabolic equivalent of task (MET)-minutes per week of vigorous or moderate activity6,59,60. For youth, most studies used a PA definition corresponding to 60 minutes of moderate intensity activity as per the Arab Teens Lifestyle Study (ATLS) questionnaire PA measurement and compilation (Supplementary, Table S12)61.
Only one study62 used a daily threshold of ≥13,000 steps using the pedometer to quantify sufficient PA participation (Supplementary, Table S12). Most studies pertaining to adults and youth utilized validated tools along with a validated version in Arabic or Urdu language, depending on the primary language of the country.
The results from univariate meta-regression analyses assessing the relationship between study-level covariates and the PA prevalence measures are summarized in Table 4. Factors associated with a higher prevalence of PA among adults were the use of the two validated questionnaires- IPAQ and GPAQ, and data collected after the year 2000. Factors associated with a higher prevalence of PA among youth were male gender and the use of IPAQ. The HBSC, PACE+ questionnaires and country level coverage of the study are associated with a lower PA prevalence among youth (Table 4).
Overview of studies with physical inactivity data
To define physical inactivity, we used physical activity levels below the recommended levels of PA. Hence, the validated measurement tools used to assess PA participation were also used to assess physical inactivity (Supplementary, Table S12).
Two studies used a daily threshold of <10,000 steps using the pedometer to quantify insufficient PA participation. Two studies used a daily threshold of a daily heart rate <159 bpm for at least 20 min and a daily heart rate <140 bpm for at least 30 min to quantify physical inactivity.
Among adults and youths, a total of 134 primary studies reported data on physical inactivity (Supplementary, Tables S10 and S11). Studies using a standard definition for physical inactivity and not overlapping with an already included data/study were included in the meta-analysis and are listed in Supplementary, Tables S6 and S7. Overall, higher prevalence measures of physical inactivity among female adults compared to male adults was noted.
A total of 58 primary studies reported factors positively correlated to physical inactivity and barriers to physical activity.
Among the included SRs, only the SR of Ranasinghe 201354 reported an OR comparing the prevalence of physical inactivity between males and females in Pakistan. This SR concluded that females were significantly more inactive than males [OR: 2.1 (95% CI = 1.5–3.1), p-value<0.001]. In UAE, Yammine et al.56 concluded that adolescent females had a significantly higher mild level of PA compared to males [ORpooled: 0.82 (95% CI = 0.698–0.961%); I2 = 98.0%; n = 2]56.
Overview of studies with sedentary behaviour
A total of 22 primary studies63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84 on sedentary behaviour among adults and youth were included (Supplementary, Tables S8 and S9). Adult sedentary behaviour data was reported for Kuwait, Oman, Qatar, and Saudi Arabia and youth sedentary behaviour measures were available for Bahrain, Djibouti, Jordan, Kuwait, Libya, Morocco, Oman, Saudi Arabia, and the UAE. However, the wide variability in sedentary behaviour measurement prevents measurable conclusions on age and sex-related differences.
Sedentary behaviour definitions varied for adults (three definitions) and youth (17 definitions). Definition variations were related to the type of sedentary activities considered (screen time, sitting time, game time, reading time, standing time, talking time, or total sedentary time) and the measurement unit (minutes or hours per day or week). Sedentary behaviour was assessed using the mean time (minutes per day or week) or the proportion of the population exhibiting sedentary behaviour (prevalence measure, %). The threshold used for sedentary behaviour prevalence measures (6+ hours per day, 3+ hours per day, or 2+ hours per day) also varied among the studies. Within the 13 sedentary behaviour measures in adults, 54% were reported as a sedentary behaviour prevalence measure and 46% as the mean amount of time spent sitting (Supplementary, Table S10). Among the 79 sedentary behaviour measures in youth, 63% were reported as a sedentary behaviour prevalence measure and 37% as the mean amount of time spent sitting (Supplementary, Table S11). The validated tools utilized for sedentary behaviour measurement were the same tools used for PA assessment among adults and youth.
Discussion
Our overview included seven SRs, 229 primary studies and 203,617 participants spanning the 20 MENA countries. Our meta-analysis on PA participation after the year 2000 demonstrates that 49.2% of adults and 74.4% of the youth population were not sufficiently active. Insufficient evidence is available on sedentary behaviour due to the absence of clear measurement guidelines.
Our regional pooled PA prevalence of 50.8% among adults was similar to the recent estimate in the region of MENA and Central Asia (67.2%)26 but lower than the global estimates of 72.5–77%25,26. Minor differences in PA prevalence estimates can be explained by the differences in the number of countries considered for the calculation, the measurement of PA, and data management25. Evolving PA recommendations could also be an explanation; previously, sufficient PA was defined as undertaking at least 30 minutes per day of moderate intensity activity for at least five days per week or at least 20 minutes per day of vigorous intensity activity for at least three days per week or an equivalent combination achieving 600 METs-minutes per week85,86. This recommendation is likely more difficult to be achieved when compared to the updated recommendation of 150 minutes of moderate intensity activity or 75 minutes of vigorous intensity activity per week, or an equivalent combination regardless of the weekly frequency6,7, since this has more flexibility.
Our regional pooled PA prevalence of 25.6% among youth is consistent with the global estimate of about 20% of youth who are sufficiently active as per the international recommendation for PA9,25. The lack of awareness pertaining to the recommendation of 60 minutes of moderate- to vigorous-intensity PA daily for children and youth6,7,87 and its benefits can explain the very low PA participation in the region57,58and globally. Our findings in MENA confirm the lower PA participation of youth in comparison to adults which is observed globally9,25. This could partially be due to the higher recommended levels of PA for youth and in part due to the tools utilized to measure PA. Because PA habits developed during youth may persist in adulthood, young people should be encouraged to participate in a variety of physical activity that supports their natural development6. Implementation of locally informed, evidence-based interventions promoting PA participation at the standardized recommended levels and addressing barriers for PA would be a step in the right direction.
Our findings confirm the higher PA participation among males as compared to females which is observed globally9,22,88,89 and regionally52,53,56,57,58 among both adults and youth. Hence, the female youth should be a target population for future interventions to increase PA participation in the region. Understanding the barriers and determinants of PA in the MENA population is essential for developing culturally- and age-appropriate PA interventions (Table 5). The sex differences in adults may be attributable to the sociocultural role of men and women in the region54,58, however, barriers related to the lower participation of female youth in PA requires further investigation (Table 5). Physical activity interventions should be inspired from countries with the highest PA prevalence measures among girls, for example in China (75%)88, where walking and biking are a common form of commuting. Our analyses provide some indication of an increased PA participation among adults after 2000 in all MENA countries with available data in both periods. Although definitions used for sufficient PA participation were similar between the studies conducted before and after 2000, caution must be practiced while interpreting these results given the limited data collected before 2000. In addition, none of the studies conducted before 2000 assessed PA participation using a standard PA questionnaire (GPAQ, IPAQ) as these questionnaires were developed in 200290 and 200391 respectively.
Unlike other MENA countries, a substantial proportion of the population in the GCC countries is non-national37. Physical activity data differentiating nationals and non-nationals is scarce. The increase in PA in the GCC after 2000 may be explained by urbanization and socioeconomic improvement, see Table 5. Additional studies considering the demographic specificities in the GCC are needed to provide evidence on PA behaviour to develop, implement, and monitor public health programs.
We found a high proportion of heterogeneity between PA prevalence measures attributable to the type of questionnaire used. Prevalence estimates using the IPAQ were higher than those using the GPAQ. This is consistent with previous findings demonstrating PA over-reporting using the IPAQ compared to other similar questionnaires such as the GPAQ27, the Behavioural Risk Factor Surveillance System (BRFSS)92, or the accelerometer93,94. This results in an overestimation of the PA prevalence measures and consequently an underestimation of the physical inactivity prevalence measures95. Moreover, the GPAQ and IPAQ measure the total PA for a typical week making comparison difficult with the BRFSS (non-occupational PA for the past month)96 and the Active Australia Survey (leisure-time PA in the week preceding interview)97 used in Western countries.
The GPAQ is a valid measurement tool to assess moderate-to-vigorous PA endorsed by the World Health Organization90. However, this tool demonstrated a weak agreement with accelerometer use in young Saudi men98. Adapting the current GPAQ to build a regional PA questionnaire has been recommended98. Both measurement tool-based factors (question phrasing, time period coverage, and single or multipart questions)99 and individual-based factors (demographic and socioeconomic characteristics)98 should be considered in its development.
The international PA recommendations for youth require a mix of moderate and vigorous intensity activity (vigorous-intensity activity, including those that strengthen muscle and bone, at least three days per week)6,7,87. Physical activity participation among youth assessed using the ATLS questionnaire was based on the conversion of all moderate and vigorous activities during the week to a summary measure in MET-minutes with a cut-off of 1,680 METs-minutes per week corresponding to 60 minutes of moderate intensity activity every day of the week61. This methodology of quantifying PA participation is inclusive of participants engaging in solely moderate activities while the standard definition includes only those participants who engage in a combination of moderate activities most days of the week and vigorous activities three times per week6,7,87. The ATLS questionnaire could then overestimate the proportion of the population which is physically active. Nevertheless, the ATLS questionnaire was the only PA questionnaire validated among youth in MENA countries.
Objectively measured PA using accelerometer, pedometer or continuous heart rate monitor can avoid recall bias and is practical for use particularly among youth when compared to self-reported data100. However, the minimum number of steps measured by the pedometer required for health benefits is still debatable101,102,103,104 and no health-based criteria for steps per day have been developed for adults and youth88,100,102,104,105. Despite attempts to establish the steps per day threshold equivalent to the daily recommended PA level for youth106, validation studies are inconsistent on the standard threshold steps count62,102,103,105,107,108. Moreover, none of the international guidelines use the steps count to define sufficient PA6,7,49,86. Additionally, even if it was used as a gold standard in the ATLS validation study109, the pedometer is not designed to capture pattern, intensity, or type of PA and most are sensitive to ambulatory activities105.
The most basic dimensions of PA assessment are frequency, intensity, time (duration), and type of activities100. Currently, no single tool can adequately assess all these dimensions101. A combination of self-reported measures (to capture important domain- and behaviour-specific sedentary time information) and device-based measures (to measure both total sedentary time and patterns of sedentary time accumulation) is recommended99,110.
Sedentary behaviour is a different concept than physical inactivity and is expressed as a total number of minutes or hours spent in sedentary activities on a typical day60. The variability in the type of sedentary activities considered in the sedentary behaviour questionnaires prevent comparisons between countries in the region and globally. To date there is no well-accepted threshold to categorize sedentary behaviour data59.
The accelerometer is acknowledged as a valid and reliable instrument for objective measurement of sedentary behaviour in adults and youth111,112,113,114,115. However, it is a costly option for researchers. Moreover, it cannot provide information on the type and setting of sedentary behaviour and there is no consensus on the number of steps to identify individuals with sedentary behavior110,116. Sedentary behaviour has been recognized as a public health issue only in the past decade9 and therefore, only minimal standardized instruments exist for its assessment with no clear interpretation guidelines.
To our knowledge, this is the most comprehensive systematic overview and meta-analysis covering several dimensions of PA behaviour in the MENA region. Our overview is the first to bring together the available evidence on sedentary behaviour and PA. Moreover, most of the included primary studies have assessed PA prevalence using validated measurement tools in random national-level samples supporting the quality of the reported estimates. The country-, time-, age-, and sex-specific pooled PA prevalence measures are a major addition to the evidence on PA. This compilation will serve as a benchmark for epidemiologists and public health interventionists (Table 6). This overview identifies barriers (Table 5) and research gaps (Table 7) that could help direct future funding and investigation.
Limitations include the restriction of the search strategy to PubMed/MEDLINE. However, we searched additional sources indexing grey and non-grey literature relevant to the region. Moreover, the included SRs have searched in total 21 literature sources for primary studies including grey literature sources, which are potentially important data sources for MENA countries27,31. This minimizes the risk of publication bias in our overview. We also extracted the data from the primary studies to complete the missing information and provide a complete overview of the available data.
The data that we used on PA and sedentary behaviour was collected before 2018; new PA data from MENA countries may have been published since. The limited data on PA behaviour in the MENA countries could be explained by the targeted population and outcomes of the included SRs. To optimize the quantitative synthesis, we converted physical inactivity data, using a standard definition, to PA measures. Despite attempts to minimize the heterogeneity using several subgroup analyses, a high heterogeneity between the PA prevalence measures persisted. Although most of the primary studies used validated PA-measurement tools, differences in PA domains captured by these measurement tools contributes to the heterogeneity between estimates. Another limitation of our metanalysis could be the minor differences in the definitions of the ‘active’ category among youth (e.g. number of days per week or steps). However, since only a limited number of studies had these differences, we feel this may have a minimal impact on the results. Differences according to the area of residence (rural versus urban) and the study coverage (country versus local coverage) might have been additional sources of heterogeneity in the reported prevalence measures.
In comparison to the global average estimates, our regional PA prevalence estimates for MENA were lower among both adults and youth. The lower PA participation by females and youth observed globally was also found in several MENA countries. More recent data suggests an increased PA participation in the region as a whole. Some of the variability in the PA measures might be attributable to the type of questionnaires used for data collection. Trends and patterns need to be confirmed in future investigations. Whether sedentary behaviour is a public health issue in the MENA region remains unclear, due to the absence of guidelines to quantify and interpret it. Harmonizing definitions of sedentary behaviour would be useful to generate evidence for the region. Promoting PA and limiting sedentary behaviour should be health priorities for both adults and the youth to reduce the overall burden of obesity and other non-communicable diseases. Additionally, promoting PA surveillance and identifying and investigating sedentary behaviour trends utilizing validated and reliable measurement tools consistent at national and international levels is essential to allow meaningful comparisons and to implement effective evidence-based interventions.
Data availability
The datasets generated during and/or analysed during the current study are available from the corresponding author on reasonable request.
References
The World Health Organization (WHO). Noncommunicable diseases, https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (2018).
International Diabetes Federation (IDF). IDF Diabetes Atlas. (2017).
Hurt, R. T., Kulisek, C., Buchanan, L. A. & McClave, S. A. The Obesity Epidemic: Challenges, Health Initiatives, and Implications for Gastroenterologists. Gastroenterology & Hepatology 6, 780–792 (2010).
Nikoloski, Z. & Williams, G. In Metabolic Syndrome (ed R.S. Ahima) (Springer International Publishing Switzerland 2016, Philadelphia, PA, USA).
Warburton, D. E. R., Nicol, C. W. & Bredin, S. S. D. Health benefits of physical activity: the evidence. Canadian Medical Association Journal 174, 801–809, https://doi.org/10.1503/cmaj.051351 (2006).
World Health Organization (WHO). In Global Recommendations on Physical Activity for Health (World Health Organization 2010, Geneva, 2010).
Committee, U. S. D. O. H. A. H. S. P. A. G. A. 2018 Physical Activity Guidelines Advisory Committee Scientific Report.. (Washington, DC:).
González, K., Fuentes, J. & Márquez, J. L. Physical Inactivity, Sedentary Behavior and Chronic Diseases. Korean Journal of Family Medicine 38, 111–115, https://doi.org/10.4082/kjfm.2017.38.3.111 (2017).
Hallal, P. C. et al. Global physical activity levels: surveillance progress, pitfalls, and prospects. The Lancet 380, 247–257, https://doi.org/10.1016/S0140-6736(12)60646-1 (2012).
Kyu, H. H. et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ 354, i3857, https://doi.org/10.1136/bmj.i3857 (2016).
Lee, C. D., Folsom, A. R. & Blair, S. N. Physical activity and stroke risk: a meta-analysis. Stroke 34, 2475–2481, https://doi.org/10.1161/01.Str.0000091843.02517.9d (2003).
Lee, I. M. et al. Impact of Physical Inactivity on the World’s Major Non-Communicable Diseases. Lancet 380, 219–229, https://doi.org/10.1016/S0140-6736(12)61031-9 (2012).
Biswas A O. P. et al. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults a systematic review and meta-analysis of sedentary time and disease incidence, mortality, and hospitalization. 162(2):123–32 (2015).
Carson, V. et al. Systematic review of sedentary behaviour and health indicators in school-aged children and youth: an update. Applied Physiology, Nutrition, and Metabolism 41, S240–S265, https://doi.org/10.1139/apnm-2015-0630 (2016).
Patterson, R. et al. Sedentary behaviour and risk of all-cause, cardiovascular and cancer mortality, and incident type 2 diabetes: a systematic review and dose response meta-analysis. European Journal of Epidemiology, https://doi.org/10.1007/s10654-018-0380-1 (2018).
Berlin, J. A. & Colditz, G. A. A meta-analysis of physical activity in the prevention of coronary heart disease. American journal of epidemiology 132, 612–628 (1990).
Sofi, F., Capalbo, A., Cesari, F., Abbate, R. & Gensini, G. F. Physical activity during leisure time and primary prevention of coronary heart disease: an updated meta-analysis of cohort studies. European Journal of Cardiovascular Prevention & Rehabilitation 15, 247–257, https://doi.org/10.1097/HJR.0b013e3282f232ac (2008).
Thune, I. & Furberg, A.-S. Physical activity and cancer risk: dose-response and cancer, all sites and site-specific. Medicine & Science in Sports & Exercise 33, S530–S550 (2001).
Street, S. J., Wells, J. C. K. & Hills, A. P. Windows of opportunity for physical activity in the prevention of obesity. Obesity Reviews 16, 857–870, https://doi.org/10.1111/obr.12306 (2015).
Biddle, S. J. H. & Asare, M. Physical activity and mental health in children and adolescents: a review of reviews. British Journal of Sports Medicine 45, 886–895, https://doi.org/10.1136/bjsports-2011-090185 (2011).
Khan, N. A. & Hillman, C. H. The Relation of Childhood Physical Activity and Aerobic Fitness to Brain Function and Cognition: A Review. Pediatric Exercise Science 26, 138–146, https://doi.org/10.1123/pes.2013-0125 (2014).
World Health Organization (WHO). Global Strategy on Diet, Physical Activity and Health, http://www.who.int/dietphysicalactivity/factsheet_inactivity/en/ (2018).
Hallal, P. C., Martins, R. C. & Ramírez, A. The Lancet Physical Activity Observatory: promoting physical activity worldwide. The Lancet 384, 471–472, https://doi.org/10.1016/S0140-6736(14)61321-0 (2014).
Varela, A. R. et al. Mapping the historical development of physical activity and health research: A structured literature review and citation network analysis. Preventive Medicine 111, 466–472, https://doi.org/10.1016/j.ypmed.2017.10.020 (2018).
Sallis, J. F. et al. Progress in physical activity over the Olympic quadrennium. The Lancet 388, 1325–1336, https://doi.org/10.1016/S0140-6736(16)30581-5 (2016).
Guthold, R., Stevens, G. A., Riley, L. M. & Bull, F. C. Worldwide trends in insufficient physical activity from 2001 to 2016: a pooled analysis of 358 population-based surveys with 1·9 million participants. The Lancet Global Health, https://doi.org/10.1016/S2214-109X(18)30357-7 (2018).
Chaabna, K. et al. Gray literature in systematic reviews on population health in the Middle East and North Africa: protocol of an overview of systematic reviews and evidence mapping. Systematic Reviews 7, 94, https://doi.org/10.1186/s13643-018-0751-4 (2018).
Booth, A. et al. PROSPERO at one year: an evaluation of its utility. Systematic Reviews 2, 4, https://doi.org/10.1186/2046-4053-2-4 (2013).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. J Clin Epidemiol 62, 1006–1012, https://doi.org/10.1016/j.jclinepi.2009.06.005 (2009).
Higgins J & Green S. (The Cochrane Collaboration, 2011).
Quenby, M., Dwayne, V. E. & Emma, I. Searching for grey literature for systematic reviews: challenges and benefits. Research Synthesis Methods 5, 221–234, https://doi.org/10.1002/jrsm.1106 (2014).
Ouzzani, M., Hammady, H., Fedorowicz, Z. & Elmagarmid, A. Rayyan—a web and mobile app for systematic reviews. Systematic Reviews 5, 210, https://doi.org/10.1186/s13643-016-0384-4 (2016).
Troiano, R. P., Gabriel, K. K. P., Welk, G. J., Owen, N. & Sternfeld, B. Reported Physical Activity and Sedentary Behavior: Why Do You Ask? Journal of Physical Activity and Health 9, S68–S75, https://doi.org/10.1123/jpah.9.s1.s68 (2012).
Mehairi, A. E. et al. Metabolic syndrome among Emirati adolescents: a school-based study. PLoS One 8, e56159, https://doi.org/10.1371/journal.pone.0056159 (2013).
Muhairi, S. J. et al. Vitamin D deficiency among healthy adolescents in Al Ain, United Arab Emirates. BMC Public Health 13, 33, https://doi.org/10.1186/1471-2458-13-33 (2013).
Wasfi, A. S., El-Sherbiny, A. A., Gurashi, E. & Al Sayegh, F. U. Sport practice among private secondary-school students in Dubai in 2004. East Mediterr Health J 14, 704–714 (2008).
Chaabna, K., Cheema, S. & Mamtani, R. Migrants, healthy worker effect, and mortality trends in the Gulf Cooperation Council countries. PLOS ONE 12, e0179711, https://doi.org/10.1371/journal.pone.0179711 (2017).
Jakovljevic, M. M. et al. Population aging and migration - history and UN forecasts in the EU-28 and its east and south near neighborhood - one century perspective 1950-2050. Globalization and health 14, 30, https://doi.org/10.1186/s12992-018-0348-7 (2018).
Farrag, N. S., Cheskin, L. J. & Farag, M. K. A systematic review of childhood obesity in the Middle East and North Africa (MENA) region: Prevalence and risk factors meta-analysis. Advances in pediatric research 4, 8, https://doi.org/10.12715/apr.2017.4.8 (2017).
UN news. Malnutrition among children in Yemen at ‘all-time high,’ warns UNICEF, https://news.un.org/en/story/2016/12/547632-malnutrition-among-children-yemen-all-time-high-warns-unicef#.WI_-ifl97IU (2016).
World Bank. Middle East and North Africa., http://www.worldbank.org/en/region/mena/overview (2018).
Khan, H. T. A., Hussein, S. & Deane, J. Nexus Between Demographic Change and Elderly Care Need in the Gulf Cooperation Council (GCC) Countries: Some Policy Implications. Ageing International 42, 466–487, https://doi.org/10.1007/s12126-017-9303-9 (2017).
Higgins, J. P. T., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ 327, 557–560, https://doi.org/10.1136/bmj.327.7414.557 (2003).
Michael Borenstein, Larry V. Hedges, Julian P.T. Higgins & Rothstein, H. R. Borenstein, M. Introduction to meta-analysis.. (John Wiley & Son, 2009).
Schwarzer, G. (CRAN, 2018).
National Institutes of Health: Division of Cancer Control and Population Sciences. List of physical activity standard questionnaires validations studies, https://epi.grants.cancer.gov/paq/validation.html(
Shea, B. J. et al. Development of AMSTAR: a measurement tool to assess the methodological quality of systematic reviews. BMC Medical Research Methodology 7, 10, https://doi.org/10.1186/1471-2288-7-10 (2007).
Shea, B. J. et al. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. Journal of Clinical Epidemiology 62, 1013–1020, https://doi.org/10.1016/j.jclinepi.2008.10.009 (2009).
Institute of Medicine of the National Academies. Finding What Works in Health Care: Standards for Systematic Reviews. (Washington, DC: THE NATIONAL ACADEMIES PRESS 2011).
National Heart, L., and Blood Institute (NHLBI)/National Institutes of Health (NIH),. In Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies (2018).
Davids, E. & Roman, N. A systematic review of the relationship between parenting styles and children’s physical activity. Vol. 20 (2014).
Mabry, R., Koohsari, M. J., Bull, F. & Owen, N. A systematic review of physical activity and sedentary behaviour research in the oil-producing countries of the Arabian Peninsula. BMC Public Health 16, 1003, https://doi.org/10.1186/s12889-016-3642-4 (2016).
Mabry, R. M., Reeves, M. M., Eakin, E. G. & Owen, N. Evidence of physical activity participation among men and women in the countries of the Gulf cooperation council: a review. Obesity reviews: an official journal of the International Association for the Study of Obesity 11, 457–464, https://doi.org/10.1111/j.1467-789X.2009.00655.x (2010).
Ranasinghe, C. D., Ranasinghe, P., Jayawardena, R. & Misra, A. Physical activity patterns among South-Asian adults: a systematic review. International Journal of Behavioral Nutrition and Physical Activity 10, 116, https://doi.org/10.1186/1479-5868-10-116 (2013).
Boyle, M. H. Guidelines for evaluating prevalence studies. Evidence Based Mental Health 1, 37–39, https://doi.org/10.1136/ebmh.1.2.37 (1998).
Yammine, K. The prevalence of physical activity among the young population of UAE: a meta-analysis. Perspectives in Public Health 137, 275–280, https://doi.org/10.1177/1757913916675388 (2016).
Al-Hazzaa, H. M. Physical inactivity in Saudi Arabia revisited: A systematic review of inactivity prevalence and perceived barriers to active living. Int J Health Sci (Qassim) 12, 50–64 (2018).
Sharara, E., Akik, C., Ghattas, H. & Makhlouf Obermeyer, C. Physical inactivity, gender and culture in Arab countries: a systematic assessment of the literature. BMC Public Health 18, 639, https://doi.org/10.1186/s12889-018-5472-z (2018).
International Physical Activity Questionnaire, https://docs.google.com/viewer?a=v&pid=sites&srcid=ZGVmYXVsdGRvbWFpbnx0aGVpcGFxfGd4OjE0NDgxMDk3NDU1YWRlZTM (2005).
World Health Organization (WHO). In Working version 5 (Geneva 2014).
Al-Hazzaa, H. M., Musaiger, A. O. & Group, A. R. Arab Teens Lifestyle Study (ATLS): objectives, design, methodology and implications. Diabetes Metab Syndr Obes 4, 417–426, https://doi.org/10.2147/DMSO.S26676 (2011).
Al-Hazzaa, H. M. Pedometer-determined physical activity among obese and non-obese 8- to 12-year-old Saudi schoolboys. J Physiol Anthropol 26, 459–465 (2007).
Al-Thani, M. et al. Lifestyle Patterns Are Associated with Elevated Blood Pressure among Qatari Women of Reproductive Age: A Cross-Sectional National Study. Nutrients 7, 7593–7615, https://doi.org/10.3390/nu7095355 (2015).
El-Aty, M. A. et al. Metabolic Syndrome and Its Components: Secondary analysis of the World Health Survey, Oman. Sultan Qaboos Univ Med J 14, e460–467 (2014).
Mabry, R. M., Winkler, E. A., Reeves, M. M., Eakin, E. G. & Owen, N. Correlates of Omani adults’ physical inactivity and sitting time. Public Health Nutr 16, 65–72, https://doi.org/10.1017/s1368980012002844 (2013).
WHO-STEPS Survey Kuwait. World Health Organization (WHO) Stepwise Approach to NCD Surveillance, Kuwait. (MOH & WHO, Kuwait City, Kuwait, 2008).
WHO-STEPS Survey Saudi Arabia. World Heath Organization (WHO) Stepwise Approach to NCD Surveillance - Country-Specific Standard Report. (MOH, WHO & EMRO, Riyadh, Saudi Arabia, 2005).
Al-Hazzaa, H. M., Abahussain, N. A., Al-Sobayel, H. I., Qahwaji, D. M. & Musaiger, A. O. Physical activity, sedentary behaviors and dietary habits among Saudi adolescents relative to age, gender and region. International Journal of Behavioral Nutrition and Physical Activity 8, 140 (2011).
Al-Hazzaa, H. M. et al. A cross-cultural comparison of health behaviors between Saudi and British adolescents living in urban areas: gender by country analyses. Int J Environ Res Public Health 10, 6701–6720, https://doi.org/10.3390/ijerph10126701 (2013).
Al-Hazzaa, H. M. & Al-Rasheedi, A. A. Adiposity and physical activity levels among preschool children in Jeddah, Saudi Arabia. Saudi medical journal 28, 766–773 (2007).
Al-Hazzaa, H. M. et al. Association of dietary habits with levels of physical activity and screen time among adolescents living in Saudi Arabia. J Hum Nutr Diet 27(Suppl 2), 204–213, https://doi.org/10.1111/jhn.12147 (2013).
Al-Nakeeb, Y. et al. Obesity, physical activity and sedentary behavior amongst British and Saudi youth: a cross-cultural study. Int J Environ Res Public Health 9, 1490–1506, https://doi.org/10.3390/ijerph9041490 (2012).
Al-Nuaim, A. A. et al. The Prevalence of Physical Activity and Sedentary Behaviours Relative to Obesity among Adolescents from Al-Ahsa, Saudi Arabia: Rural versus Urban Variations. J Nutr Metab 2012, 417589, https://doi.org/10.1155/2012/417589 (2012).
Allafi, A. et al. Physical activity, sedentary behaviours and dietary habits among Kuwaiti adolescents: gender differences. Public Health Nutr 17, 2045–2052, https://doi.org/10.1017/S1368980013002218 (2013).
Farghaly, N. F., Ghazali, B. M., Al-Wabel, H. M., Sadek, A. A. & Abbag, F. I. Life style and nutrition and their impact on health of Saudi school students in Abha, Southwestern region of Saudi Arabia. Saudi medical journal 28, 415–421 (2007).
Gharib, N. M. & Rasheed, P. Obesity Among Bahraini Children and Adolescents: Prevalence And Associated Factors. Journal of the Bahrain Medical Society 20 (2008).
Guthold, R., Cowan, M. J., Autenrieth, C. S., Kann, L. & Riley, L. M. Physical activity and sedentary behavior among schoolchildren: a 34-country comparison. J Pediatr 157(43-49), e41, https://doi.org/10.1016/j.jpeds.2010.01.019 (2010).
Guthold, R., Ono, T., Strong, K. L., Chatterji, S. & Morabia, A. Worldwide variability in physical inactivity a 51-country survey. American journal of preventive medicine 34, 486–494, https://doi.org/10.1016/j.amepre.2008.02.013 (2008).
Kilani, H., Al-Hazzaa, H., Waly, M. I. & Musaiger, A. Lifestyle Habits: Diet, physical activity and sleep duration among Omani adolescents. Sultan Qaboos Univ Med J 13, 510–519 (2013).
Mahfouz, A. A. et al. Obesity and related behaviors among adolescent school boys in Abha City, Southwestern Saudi Arabia. J Trop Pediatr 54, 120–124, https://doi.org/10.1093/tropej/fmm089 (2008).
Mahfouz, A. A. et al. Nutrition, physical activity, and gender risks for adolescent obesity in Southwestern Saudi Arabia. Saudi J Gastroenterol 17, 318–322, https://doi.org/10.4103/1319-3767.84486 (2011).
Musaiger, A. O. & Zagzoog, N. Dietary and lifestyle habits among adolescent girls in Saudi Arabia. Nutrition & Food Science 43, 605–610 (2013).
Yousef, S., Eapen, V., Zoubeidi, T. & Mabrouk, A. Behavioral correlation with television watching and videogame playing among children in the United Arab Emirates. Int J Psychiatry Clin Pract 18, 203–207, https://doi.org/10.3109/13651501.2013.874442 (2013).
Youssef, R. M., Al Shafie, K., Al-Mukhaini, M. & Al-Balushi, H. Physical activity and perceived barriers among high-school students in Muscat, Oman. East Mediterr Health J 19, 759–768 (2013).
Pate, R. R., Pratt, M. & Blair, S. N. et al. Physical activity and public health: A recommendation from the centers for disease control and prevention and the american college of sports medicine. JAMA 273, 402–407, https://doi.org/10.1001/jama.1995.03520290054029 (1995).
Human energy requirements. Scientific background papers from the Joint FAO/WHO/UNU Expert Consultation. October 17-24, 2001.. Report No. 1368-9800 (Print) 1368-9800, 929-1228 (Rome, Italy, 2005).
Tremblay, M. S. et al. New Canadian physical activity guidelines. Appl Physiol Nutr Metab 36(36-46), 47–58, https://doi.org/10.1139/h11-009 (2011).
Sisson, S. B. & Katzmarzyk, P. T. International prevalence of physical activity in youth and adults. Obesity reviews: an official journal of the International Association for the Study of Obesity 9, 606–614, https://doi.org/10.1111/j.1467-789X.2008.00506.x (2008).
Khuwaja, A. K. & Kadir, M. M. Gender differences and clustering pattern of behavioural risk factors for chronic non-communicable diseases: community-based study from a developing country. Chronic Illn 6, 163–170, https://doi.org/10.1177/1742395309352255 (2010).
Cleland, C. L. et al. Validity of the Global Physical Activity Questionnaire (GPAQ) in assessing levels and change in moderate-vigorous physical activity and sedentary behaviour. BMC Public Health 14, 1255, https://doi.org/10.1186/1471-2458-14-1255 (2014).
Craig, C. L. et al. International physical activity questionnaire: 12-country reliability and validity. Med Sci Sports Exerc 35, 1381–1395, https://doi.org/10.1249/01.Mss.0000078924.61453.Fb (2003).
Ainsworth, B. E. et al. Comparison of the 2001 BRFSS and the IPAQ Physical Activity Questionnaires. Medicine & Science in Sports & Exercise 38, 1584–1592, https://doi.org/10.1249/01.mss.0000229457.73333.9a (2006).
Ekelund, U. et al. Criterion-related validity of the last 7-day, short form of the International Physical Activity Questionnaire in Swedish adults. Public Health Nutrition 9, 258–265, https://doi.org/10.1079/PHN2005840 (2006).
Lee, P. H., Macfarlane, D. J., Lam, T. H. & Stewart, S. M. Validity of the international physical activity questionnaire short form (IPAQ-SF): A systematic review. The International Journal of Behavioral Nutrition and Physical Activity 8, 115–115, https://doi.org/10.1186/1479-5868-8-115 (2011).
Rzewnicki, R., Auweele, Y. V. & Bourdeaudhuij, I. D. Addressing overreporting on the International Physical Activity Questionnaire (IPAQ) telephone survey with a population sample. Public Health Nutrition 6, 299–305, https://doi.org/10.1079/PHN2002427 (2003).
Centers for Disease Control and Prevention: National Center for Cahronic Disease Prevention and Health Promotion. The Behavioral Risk Factor Surveillance System (BRFSS) questionnaire. (U.S 2018).
Australian Institute of Health and Welfare (AIHW). The Active Australia Survey: a guide and manual for implementation, analysis and reporting. (Canberra, Australia 2003).
Alkahtani, S. A. Convergent validity: agreement between accelerometry and the Global Physical Activity Questionnaire in college-age Saudi men. BMC Research Notes 9, 436, https://doi.org/10.1186/s13104-016-2242-9 (2016).
Healy, G. N. et al. Measurement of Adults’ Sedentary Time in Population-Based Studies. American journal of preventive medicine 41, 216–227, https://doi.org/10.1016/j.amepre.2011.05.005 (2011).
Sallis, J. F. Measuring Physical Activity: Practical Approaches for Program Evaluation in Native American Communities. Journal of public health management and practice: JPHMP 16, 404–410, https://doi.org/10.1097/PHH.0b013e3181d52804 (2010).
Graf, C. et al. Feasibility and acceptance of exercise recommendations (10,000 steps a day) within routine German health check (Check-Up 35/GOÄ29)—study protocol. Pilot and Feasibility Studies 2, 52, https://doi.org/10.1186/s40814-016-0092-9 (2016).
Tudor-Locke, C. et al. BMI-referenced standards for recommended pedometer-determined steps/day in children. Preventive Medicine 38, 857–864, https://doi.org/10.1016/j.ypmed.2003.12.018 (2004).
Beets, M., Beighle, A., Bottai, M., Rooney, L. & Tilley, F. Pedometer-Determined Step-Count Guidelines for Afterschool Programs. Vol. 9 (2012).
Harrington, D. M. et al. Step-based translation of physical activity guidelines in the Lower Mississippi Delta. Applied Physiology, Nutrition, and Metabolism 36, 583–585, https://doi.org/10.1139/h11-053 (2011).
Tudor-Locke, C., Williams, J. E., Reis, J. P. & Pluto, D. Utility of pedometers for assessing physical activity: convergent validity. Sports Med 32, 795–808, https://doi.org/10.2165/00007256-200232120-00004 (2002).
Rowlands, A. V. & Eston, R. G. Comparison of accelerometer and pedometer measures of physical activity in boys and girls, ages 8-10 years. Research quarterly for exercise and sport 76, 251–257, https://doi.org/10.1080/02701367.2005.10599296 (2005).
Beets, M. et al. Convergent Validity of Pedometer and Accelerometer Estimates of Moderate-to-Vigorous Physical Activity of Youth. Vol. 8 Suppl 2 (2011).
McNamara, E., Hudson, Z. & Taylor, S. J. C. Measuring activity levels of young people: the validity of pedometers. British Medical Bulletin 95, 121–137, https://doi.org/10.1093/bmb/ldq016 (2010).
Al-Hazzaa, H. M., Al-Sobayel, H. I. & Musaiger, A. O. Convergent Validity of the Arab Teens Lifestyle Study (ATLS) Physical Activity Questionnaire. International Journal of Environmental Research and Public Health 8, 3810 (2011).
Hidding, L. M., Altenburg, T. M., Mokkink, L. B., Terwee, C. B. & Chinapaw, M. J. M. Systematic review of childhood sedentary behavior questionnaires: What do we know and what is next? Sports Med 47, https://doi.org/10.1007/s40279-016-0610-1 (2017).
Kim, Y., Welk, G. J., Braun, S. I. & Kang, M. Extracting objective estimates of sedentary behavior from accelerometer data: measurement considerations for surveillance and research applications. PLoS One 10, https://doi.org/10.1371/journal.pone.0118078 (2015).
Klaren, R. E., Hubbard, E. A., Zhu, W. & Motl, R. W. Reliability of accelerometer scores for measuring sedentary and physical activity behaviors in persons with multiple sclerosis. Adapt Phys Act Quart 33, https://doi.org/10.1123/apaq.2015-0007 (2016).
Manns, P., Ezeugwu, V., Armijo-Olivo, S., Vallance, J. & Healy, G. N. Accelerometer-Derived Pattern of Sedentary and Physical Activity Time in Persons with Mobility Disability: National Health and Nutrition Examination Survey 2003 to 2006. J Am Geriatr Soc 63, https://doi.org/10.1111/jgs.13490 (2015).
Peterson, N. E., Sirard, J. R., Kulbok, P. A., DeBoer, M. D. & Erickson, J. M. Validation of accelerometer thresholds and inclinometry for measurement of sedentary behavior in young adult University students. Res Nurs Health 38, https://doi.org/10.1002/nur.21694 (2015).
Trost, S. G., McIver, K. L. & Pate, R. R. Conducting accelerometer-based activity assessments in field-based research. Med Sci Sports Exerc 37, S531–543 (2005).
Tudor-Locke, C., Craig, C. L., Thyfault, J. P. & Spence, J. C. A step-defined sedentary lifestyle index: <5000 steps/day. Applied Physiology, Nutrition, and Metabolism 38, 100–114, https://doi.org/10.1139/apnm-2012-0235 (2012).
Al-Hazzaa Physical activity profile of college male students. King Saud University Journal (Educational Sciences) 2, 383–396 (1990).
Gawwad, E. S. A. Stages of change in physical activity, self efficacy and decisional balance among saudi university students. Journal of family & community medicine 15, 107–115 (2008).
Khalaf, A. et al. Female university students’ physical activity levels and associated factors–a cross-sectional study in southwestern Saudi Arabia. Int J Environ Res Public Health 10, 3502–3517, https://doi.org/10.3390/ijerph10083502 (2013).
Awadalla, N. J. et al. Assessment of physical inactivity and perceived barriers to physical activity among health college students, south-western Saudi Arabia. East Mediterr Health J 20, 596–604 (2014).
Amin, T. T., Suleman, W., Ali, A., Gamal, A. & Al Wehedy, A. Pattern, prevalence, and perceived personal barriers toward physical activity among adult Saudis in Al-Hassa, KSA. J Phys Act Health 8, 775–784, https://doi.org/10.1123/jpah.8.6.775 (2011).
Majeed, F. Association of BMI with diet and physical activity of female medical students at the University of Dammam, Kingdom of Saudi Arabia. Journal of Taibah University Medical Sciences 10, 188–196, https://doi.org/10.1016/j.jtumed.2014.11.004 (2015).
Al-Otaibi, H. H. Measuring stages of change, perceived barriers and self efficacy for physical activity in Saudi Arabia. Asian Pac J Cancer Prev 14, 1009–1016, https://doi.org/10.7314/apjcp.2013.14.2.1009 (2013).
Mandil, A. M., Alfurayh, N. A., Aljebreen, M. A. & Aldukhi, S. A. Physical activity and major non-communicable diseases among physicians in Central Saudi Arabia. Saudi medical journal 37, 1243–1250, https://doi.org/10.15537/smj.2016.11.16268 (2016).
Bajamal, E. et al. Physical Activity Among Female Adolescents in Jeddah, Saudi Arabia: A Health Promotion Model-Based Path Analysis. Nurs Res 66, 473–482, https://doi.org/10.1097/nnr.0000000000000244 (2017).
Al-Nozha, M. M. et al. Prevalence of physical activity and inactivity among Saudis aged 30-70 years. A population-based cross-sectional study. Saudi medical journal 28, 559–568 (2007).
Alam, A. A. Obesity among female school children in North West Riyadh in relation to affluent lifestyle. Saudi medical journal 29, 1139–1144 (2008).
Alsubaie, A. S. R. & Omer, E. O. M. Physical Activity Behavior Predictors, Reasons and Barriers among Male Adolescents in Riyadh, Saudi Arabia: Evidence for Obesogenic Environment. Int. J Health Sci (Qassim) 9, 400–408 (2015).
AlQuaiz, A. M. & Tayel, S. A. Barriers to a healthy lifestyle among patients attending primary care clinics at a university hospital in Riyadh. Annals of Saudi medicine 29, 30–35, https://doi.org/10.4103/0256-4947.51818 (2009).
Samara, A., Nistrup, A., Al-Rammah, T. Y. & Aro, A. R. Lack of facilities rather than sociocultural factors as the primary barrier to physical activity among female Saudi university students. Int. J Womens Health 7, 279–286, https://doi.org/10.2147/ijwh.S80680 (2015).
Al-Hazzaa, H. M. et al. Patterns and determinants of physical activity among Saudi adolescents. J Phys Act Health 11, 1202–1211, https://doi.org/10.1123/jpah.2012-0427 (2014).
Berger, G. & Peerson, A. Giving young Emirati women a voice: participatory action research on physical activity. Health Place 15, 117–124, https://doi.org/10.1016/j.healthplace.2008.03.003 (2009).
Kim, H. J., Choi-Kwon, S., Kim, H., Park, Y. H. & Koh, C. K. Health-promoting lifestyle behaviors and psychological status among Arabs and Koreans in the United Arab Emirates. Res Nurs Health 38, 133–141, https://doi.org/10.1002/nur.21644 (2015).
Mabry, R. M., Al-Busaidi, Z. Q., Reeves, M. M., Owen, N. & Eakin, E. G. Addressing physical inactivity in Omani adults: perceptions of public health managers. Public Health Nutr 17, 674–681, https://doi.org/10.1017/s1368980012005678 (2014).
Huang, N.-C., Kung, S.-F. & Hu, S. The Relationship between Urbanization, the Built Environment, and Physical Activity among Older Adults in Taiwan. International Journal of Environmental Research and Public Health 15, 836 (2018).
Kabisch, N., van den Bosch, M. & Lafortezza, R. The health benefits of nature-based solutions to urbanization challenges for children and the elderly - A systematic review. Environmental research 159, 362–373, https://doi.org/10.1016/j.envres.2017.08.004 (2017).
McCloskey, M. L. et al. Disparities in dietary intake and physical activity patterns across the urbanization divide in the Peruvian Andes. International Journal of Behavioral Nutrition and Physical Activity 14, 90, https://doi.org/10.1186/s12966-017-0545-4 (2017).
Eime, R. M. et al. The relationship of sport participation to provision of sports facilities and socioeconomic status: a geographical analysis. Australian and New Zealand Journal of Public Health 41, 248–255, https://doi.org/10.1111/1753-6405.12647 (2017).
O’Donoghue, G. et al. Socio-economic determinants of physical activity across the life course: A “Determinants of DIet and Physical ACtivity” (DEDIPAC) umbrella literature review. PLOS ONE 13, e0190737, https://doi.org/10.1371/journal.pone.0190737 (2018).
Al-Rukban, M. O. Obesity among Saudi male adolescents in Riyadh, Saudi Arabia. Saudi medical journal 24, 27–33 (2003).
Alquaiz, A. M. et al. Correlates of cardiovascular disease risk scores in women in Riyadh, Kingdom of Saudi Arabia. Women Health 55, 103–117, https://doi.org/10.1080/03630242.2014.972020 (2015).
Al-Gelban, K. S. Dietary habits and exercise practices among the students of a Saudi Teachers’ Training College. Saudi medical journal 29, 754–759 (2008).
Memish, Z. A. et al. Burden of disease, injuries, and risk factors in the Kingdom of Saudi Arabia, 1990-2010. Prev Chronic Dis 11, E169, https://doi.org/10.5888/pcd11.140176 (2014).
Al-Baghli, N. A. et al. Overweight and obesity in the eastern province of Saudi Arabia. Saudi medical journal 29, 1319–1325 (2008).
Al-Mutairi, R. L., Bawazir, A. A., Ahmed, A. E. & Jradi, H. Health beliefs related to diabetes mellitus prevention among adolescents in Saudi Arabia. Sultan Qaboos University Medical Journal 15, e398 (2015).
Musaiger, A. O. et al. Perceived barriers to weight maintenance among university students in Kuwait: the role of gender and obesity. Environ Health Prev Med 19, 207–214, https://doi.org/10.1007/s12199-013-0377-z (2014).
Rahim, H. F. et al. Non-communicable diseases in the Arab world. Lancet 383, 356–367, https://doi.org/10.1016/s0140-6736(13)62383-1 (2014).
Baglar, R. “Oh God, save us from sugar”: an ethnographic exploration of diabetes mellitus in the United Arab Emirates. Med Anthropol 32, 109–125, https://doi.org/10.1080/01459740.2012.671399 (2013).
Al-Rafaee, S. A. & Al-Hazzaa, H. M. Physical activity profile of adult males in Riyadh City. Saudi medical journal 22, 784–789 (2001).
Al-Kandari, F. & Vidal, V. L. Correlation of the health-promoting lifestyle, enrollment level, and academic performance of College of Nursing students in Kuwait. Nurs Health Sci 9, 112–119, https://doi.org/10.1111/j.1442-2018.2007.00311.x (2007).
Ali, H. I., Baynouna, L. M. & Bernsen, R. M. Barriers and facilitators of weight management: perspectives of Arab women at risk for type 2 diabetes. Health Soc Care Community 18, 219–228, https://doi.org/10.1111/j.1365-2524.2009.00896.x (2010).
Al Junaibi, A., Abdulle, A., Sabri, S., Hag-Ali, M. & Nagelkerke, N. The prevalence and potential determinants of obesity among school children and adolescents in Abu Dhabi, United Arab Emirates. Int J Obes (Lond) 37, 68–74, https://doi.org/10.1038/ijo.2012.131 (2013).
Ng, S. W. et al. Nutrition transition in the United Arab Emirates. Eur J Clin Nutr 65, 1328–1337, https://doi.org/10.1038/ejcn.2011.135 (2011).
Albawardi, N. M., Jradi, H. & Al-Hazzaa, H. M. Levels and correlates of physical activity, inactivity and body mass index among Saudi women working in office jobs in Riyadh city. BMC Womens Health 16, 33, https://doi.org/10.1186/s12905-016-0312-8 (2016).
Amin, T. T., Al Khoudair, A. S., Al Harbi, M. A. & Al Ali, A. R. Leisure time physical activity in Saudi Arabia: prevalence, pattern and determining factors. Asian Pac J Cancer Prev 13, 351–360, https://doi.org/10.7314/apjcp.2012.13.1.351 (2012).
Al-Hazzaa, H. M. Health-enhancing physical activity among Saudi adults using the International Physical Activity Questionnaire (IPAQ). Public Health Nutr 10, 59–64, https://doi.org/10.1017/S1368980007184299 (2007).
Taha, A. Z. Self-reported knowledge and pattern of physical activity among school students in Al Khobar, Saudi Arabia. East Mediterr Health J 14, 344–355 (2008).
Al-Sobayel, H., Al-Hazzaa, H. M., Abahussain, N. A., Qahwaji, D. M. & Musaiger, A. O. Gender differences in leisure-time versus non-leisure-time physical activity among Saudi adolescents. Ann Agric Environ Med 22, 344–348, https://doi.org/10.5604/12321966.1152091 (2015).
Collison, K. S. et al. Sugar-sweetened carbonated beverage consumption correlates with BMI, waist circumference, and poor dietary choices in school children. BMC Public Health 10, 234, https://doi.org/10.1186/1471-2458-10-234 (2010).
Al-Kandari, Y. Y. Prevalence of obesity in Kuwait and its relation to sociocultural variables. Obesity reviews: an official journal of the International Association for the Study of Obesity 7, 147–154, https://doi.org/10.1111/j.1467-789X.2006.00231.x (2006).
Carter, A. O., Saadi, H. F., Reed, R. L. & Dunn, E. V. Assessment of obesity, lifestyle, and reproductive health needs of female citizens of Al Ain, United Arab Emirates. J Health Popul Nutr 22, 75–83 (2004).
Garawi, F., Ploubidis, G. B., Devries, K., Al-Hamdan, N. & Uauy, R. Do routinely measured risk factors for obesity explain the sex gap in its prevalence? Observations from Saudi Arabia. BMC public health 15, 254–254, https://doi.org/10.1186/s12889-015-1608-6 (2015).
Amin, T. T. et al. Physical activity and cancer prevention: awareness and meeting the recommendations among adult Saudis. Asian Pac J Cancer Prev 15, 2597–2606, https://doi.org/10.7314/apjcp.2014.15.6.2597 (2014).
Al-Isa, A. N., Campbell, J., Desapriya, E. & Wijesinghe, N. Social and Health Factors Associated with Physical Activity among Kuwaiti College Students. J Obes 2011, 512363, https://doi.org/10.1155/2011/512363 (2011).
Sabri, S. et al. Some risk factors for hypertension in the United Arab Emirates. East Mediterr Health J 10, 610–619 (2004).
Al-Nakeeb, Y., Lyons, M., Dodd, L. J. & Al-Nuaim, A. An investigation into the lifestyle, health habits and risk factors of young adults. Int J Environ Res Public Health 12, 4380–4394, https://doi.org/10.3390/ijerph120404380 (2015).
Khalid, M. E. M. The association between strenuous physical activity and obesity in high and low altitude populations in southern Saudi Arabia. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity 19, 776–780 (1995).
Assah, F. K., Ekelund, U., Brage, S., Mbanya, J. C. & Wareham, N. J. Urbanization, physical activity, and metabolic health in sub-Saharan Africa. Diabetes Care 34, 491–496, https://doi.org/10.2337/dc10-0990 (2011).
Sullivan, R. et al. Socio-demographic patterning of physical activity across migrant groups in India: results from the Indian Migration Study. PLoS One 6, e24898, https://doi.org/10.1371/journal.pone.0024898 (2011).
Monda, K. L., Gordon-Larsen, P., Stevens, J. & Popkin, B. M. China’s transition: The effect of rapid urbanization on adult occupational physical activity. Social Science & Medicine 64, 858–870, https://doi.org/10.1016/j.socscimed.2006.10.019 (2007).
Shediac-Rizkallah, M. C., Soweid, R. A. A., Farhat, T. M. & Yeretzian, J. Adolescent health-related behaviors in postwar Lebanon: findings among students at the American University of Beirut. International quarterly of community health education 20, 115–131 (2000).
Fazah, A. et al. Activity, inactivity and quality of life among Lebanese adolescents. Pediatr Int 52, 573–578, https://doi.org/10.1111/j.1442-200X.2009.03021.x (2010).
Jabre, P., Sikias, P., Khater-Menassa, B., Baddoura, R. & Awada, H. Overweight children in Beirut: prevalence estimates and characteristics. Child Care Health Dev 31, 159–165, https://doi.org/10.1111/j.1365-2214.2004.00458.x (2005).
Rguibi, M. & Belahsen, R. High blood pressure in urban Moroccan Sahraoui women. J Hypertens 25, 1363–1368, https://doi.org/10.1097/HJH.0b013e3280f31b83 (2007).
Rguibi, M. & Belahsen, R. Overweight and obesity among urban Sahraoui women of South Morocco. Ethn Dis 14, 542–547 (2004).
El-Gilany, A. H., Badawi, K., El-Khawaga, G. & Awadalla, N. Physical activity profile of students in Mansoura University, Egypt. East Mediterr Health J 17, 694–702 (2011).
Abolfotouh, M. A., Bassiouni, F. A., Mounir, G. M. & Fayyad, R. Health-related lifestyles and risk behaviours among students living in Alexandria University Hostels. East Mediterr Health J 13, 376–391 (2007).
Nsour, M., Mahfoud, Z., Kanaan, M. N. & Balbeissi, A. Prevalence and predictors of nonfatal myocardial infarction in Jordan. East Mediterr Health J 14, 818–830 (2008).
Madanat, H. & Merrill, R. M. Motivational factors and stages of change for physical activity among college students in Amman, Jordan. Promotion & education 13, 185–190 (2006).
Musaiger, A. O. et al. Perceived barriers to healthy eating and physical activity among adolescents in seven Arab countries: a cross-cultural study. ScientificWorldJournal 2013, 232164, https://doi.org/10.1155/2013/232164 (2013).
Musharrafieh, U. et al. Determinants of university students physical exercise: a study from Lebanon. Int J Public Health 53, 208–213, https://doi.org/10.1007/s00038-008-7037-x (2008).
Hallaj, F. A., El Geneidy, M. M., Mitwally, H. H. & Ibrahim, H. S. Activity patterns of residents in homes for the elderly in Alexandria, Egypt. East Mediterr Health J 16, 1183–1188 (2010).
Aounallah-Skhiri, H. et al. Health and behaviours of Tunisian school youth in an era of rapid epidemiological transition. East Mediterr Health J 15, 1201–1214 (2009).
Lachheb, M. Religion in practice. The veil in the sporting space in Tunisia. Social Compass 59, 120–135 (2012).
Rguibi, M. & Belahsen, R. Fattening practices among Moroccan Saharawi women. East Mediterr Health J 12, 619–624 (2006).
El Rhazi, K. et al. Prevalence of obesity and associated sociodemographic and lifestyle factors in Morocco. Public Health Nutr 14, 160–167, https://doi.org/10.1017/s1368980010001825 (2011).
Abdul-Rahim, H. F. et al. Obesity in a rural and an urban Palestinian West Bank population. International journal of obesity and related metabolic disorders: journal of the International Association for the Study of Obesity 27, 140–146, https://doi.org/10.1038/sj.ijo.0802160 (2003).
Sirdah, M. M., Al Laham, N. A. & Abu Ghali, A. S. Prevalence of metabolic syndrome and associated socioeconomic and demographic factors among Palestinian adults (20-65 years) at the Gaza Strip. Diabetes Metab Syndr 5, 93–97, https://doi.org/10.1016/j.dsx.2012.02.024 (2011).
Gharaibeh, M., Al-Ma’aitah, R. & Al Jada, N. Lifestyle practices of Jordanian pregnant women. Int Nurs Rev 52, 92–100, https://doi.org/10.1111/j.1466-7657.2005.00257.x (2005).
Haddad, L. G., Owies, A. & Mansour, A. Wellness appraisal among adolescents in Jordan: a model from a developing country: a cross-sectional questionnaire survey. Health Promot Int 24, 130–139, https://doi.org/10.1093/heapro/dap013 (2009).
Sibai, A. M., Costanian, C., Tohme, R., Assaad, S. & Hwalla, N. Physical activity in adults with and without diabetes: from the ‘high-risk’ approach to the ‘population-based’ approach of prevention. BMC Public Health 13, 1002, https://doi.org/10.1186/1471-2458-13-1002 (2013).
Al-Tannir, M., Kobrosly, S., Itani, T., El-Rajab, M. & Tannir, S. Prevalence of physical activity among Lebanese adults: a cross-sectional study. Journal of Physical Activity and Health 6, 315–320 (2009).
Najdi, A. et al. Correlates of physical activity in Morocco. Preventive medicine 52, 355–357 (2011).
Fouad, M., Rastam, S., Ward, K. & Maziak, W. Prevalence of obesity and its associated factors in Aleppo, Syria. Prev Control 2, 85–94, https://doi.org/10.1016/j.precon.2006.09.001 (2006).
Al Ali, R., Rastam, S., Fouad, F. M., Mzayek, F. & Maziak, W. Modifiable cardiovascular risk factors among adults in Aleppo, Syria. International journal of public health 56, 653–662 (2011).
Al Sabbah, H., Vereecken, C., Kolsteren, P., Abdeen, Z. & Maes, L. Food habits and physical activity patterns among Palestinian adolescents: findings from the national study of Palestinian schoolchildren (HBSC-WBG2004). Public health nutrition 10, 739–746 (2007).
Al-Tawil, N. G., Abdulla, M. M. & Abdul Ameer, A. J. Prevalence of and factors associated with overweight and obesity among a group of Iraqi women. East Mediterr Health J 13, 420–429 (2007).
Centers for Disease Control and Prevention. Prevalence of selected risk factors for chronic disease–Jordan, 2002. MMWR. Morbidity and mortality weekly report 52, 1042 (2003).
Moukhyer, M., Van Eijk, J., De Vries, N. & Bosma, H. Health-related behaviors of Sudanese adolescents. Education for health 21, 184 (2008).
Chamieh, M. C. et al. Diet, physical activity and socio-economic disparities of obesity in Lebanese adults: findings from a national study. BMC Public Health 15, 279, https://doi.org/10.1186/s12889-015-1605-9 (2015).
Batnitzky, A. Obesity and household roles: gender and social class in Morocco. Sociol Health Illn 30, 445–462, https://doi.org/10.1111/j.1467-9566.2007.01067.x (2008).
Aounallah-Skhiri, H. et al. Nutritional status of Tunisian adolescents: associated gender, environmental and socio-economic factors. Public Health Nutr 11, 1306–1317, https://doi.org/10.1017/s1368980008002693 (2008).
Maatoug, J. et al. Clustering of risk factors with smoking habits among adults, Sousse, Tunisia. Preventing chronic disease 10, E211–E211, https://doi.org/10.5888/pcd10.130075 (2013).
Chacar, H. R. & Salameh, P. Public schools adolescents’ obesity and growth curves in Lebanon. J Med Liban 59, 80–88 (2011).
Salazar-Martinez, E. et al. Overweight and obesity status among adolescents from Mexico and Egypt. Arch Med Res 37, 535–542, https://doi.org/10.1016/j.arcmed.2005.10.014 (2006).
Ammouri, A. A., Neuberger, G., Nashwan, A. J. & Al‐Haj, A. M. Determinants of self‐reported physical activity among Jordanian adults. Journal of Nursing Scholarship 39, 342–348 (2007).
Mahasneh, S. M. Health perceptions and health behaviours of poor urban Jordanian women. J Adv Nurs 36, 58–68, https://doi.org/10.1046/j.1365-2648.2001.01943.x (2001).
Acknowledgements
We would like to thank Sinéad O’Rourke, Content Development Specialist, Weill Cornell Medicine-Qatar for editing the manuscript, Aida Tariq Nasir, Project Coordinator for formatting and checking the tables and Hekmat Alrouh, Project Specialist for his help in the literature search and the screening step (both previously employed at the Institute for Population Health, Weill Cornell Medicine - Qatar). We would also like to thank Sapna Bhagat, Temporary Research Assistant and Anupama Jithesh, Research Coordinator for helping with the data extraction, formatting, and checking the tables and Sathyanarayanan Doraiswamy, Assistant Director for reviewing the revised manuscript (all are employed at the Institute for Population Health, Weill Cornell Medicine-Qatar). The work was funded by the Institute for Population Health, Weill Cornell Medicine - Qatar and Qatar Foundation through the Weill Cornell Medicine - Qatar Biomedical Research Program.
Author information
Authors and Affiliations
Contributions
Sonia Chaabane (S.C.1), Karima Chaabna (K.C.), Amit Abraham (A.A.), Ravinder Mamtani (R.M.) and Sohaila Cheema (S.C.2) collectively contributed to the conception of the study. S.C.1, K.C., A.A., and S.C.2 were involved in the literature search, screening, and extraction steps. Analysis and manuscript drafting were implemented by S.C.1 with support from K.C., A.A., S.C.2, and R.M. All authors read, edited, and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chaabane, S., Chaabna, K., Abraham, A. et al. Physical activity and sedentary behaviour in the Middle East and North Africa: An overview of systematic reviews and meta-analysis. Sci Rep 10, 9363 (2020). https://doi.org/10.1038/s41598-020-66163-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-66163-x
This article is cited by
-
Modifiable risk factors for cancer in the middle East and North Africa: a scoping review
BMC Public Health (2024)
-
Sleep disorders and associated factors among medical students in the Middle East and North Africa: a systematic review and meta-analysis
Scientific Reports (2024)
-
A cross-sectional study on the perceived barriers to physical exercise among women in Iraqi Kurdistan Region
BMC Women's Health (2023)
-
Daily step counts before, during, and after COVID-19 pandemic: a smartphone-tracking study of university students in Egypt and Saudi Arabia
BMC Public Health (2023)
-
The Pandemic of Coronary Heart Disease in the Middle East and North Africa: What Clinicians Need to Know
Current Atherosclerosis Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
