
Abstract
Household air pollution has adverse effects on cardiovascular health. One of the major sources of household air pollutants is the combustion of cooking oils during cooking. Trans, trans-2,4-decadienal (tt-DDE) is a type of dienaldehyde that is present in a wide range of food and food products. It is a byproduct of the peroxidation of linoleic acid following the heating of oil during cooking. The mechanisms of the associations between household air pollution and cardiac arrhythmias are currently unclear. The purpose of this study was to determine effects of tt-DDE on the ion currents in H9c2 cells. The IK and ICa,L in H9c2 cells treated with and without tt-DDE were measured using the whole-cell patch clamp method. Expressions of Kv2.1 and Cav1.2 in H9c2 cells treated with and without tt-DDE were measured by western blot analysis. After the H9c2 cells had been exposed to tt-DDE, the IK and ICa,L were significantly decreased. The expression of Kv2.1, unlike that of Cav1.2, was also significantly decreased in these cells. These changes in IK and ICa,L that were induced by tt-DDE may help to explain the association between cardiac arrhythmogenesis and cooking-oil fumes.
Similar content being viewed by others

Introduction
Epidemiological studies have revealed that exposure to air pollutants, especially particulate matter (PM), is associated with an increased incidence of respiratory diseases, as well as of cardiovascular morbidity and mortality1,2. Exposure to air pollution could increase the risks of ischemic heart disease, heart failure, cerebrovascular disease, and cardiac arrhythmias3,4. In the Air Pollution and Cardiac Risk and its Time Course (APACR) study, 60 minutes of exposure to PM2.5 (particles with a diameter of ≤2.5 μm) was associated with increased premature ventricular contractures5. Another study demonstrated that brief exposure to air pollution could trigger atrial fibrillation6. The mechanisms of the associations between air pollution and cardiovascular diseases are currently unclear. It has been proposed that increased systemic inflammatory responses, systemic oxidative stress, systemic and pulmonary artery blood pressure, and risks of atherosclerosis, as well as changes in autonomic function indicate increased cardiovascular morbidity and mortality caused by air pollution7,8,9.
As comprehensively demonstrated in previous studies, household air pollution also has adverse effects on cardiovascular health10. Indoor exposures to PM2.5 is associated with alternation of heart rate variability that could in turn increase vulnerability to cardiac arrhythmias11. One of the major sources of household air pollutants is the combustion of cooking oils during cooking. A longitudinal study conducted by Chinese military cooks showed that exposure to compounds derived from cooking-oil fumes could cause oxidative DNA damage and lipid peroxidation12. However, the effects of the contents of cooking-oil fumes on vulnerability to cardiac arrhythmias is unknown. Trans, trans-2,4-decadienal (tt-DDE) is a type of dienaldehyde that is present in a wide range of food and food products. It is a byproduct of the peroxidation of linoleic acid following the heating of oil during cooking13. The alteration of ions currents in cardiomyocytes is one of the mechanisms involved in arrhythmogenesis. The purpose of this study was to determine these effects of tt-DDE on the ions currents in cardiomyocytes.
Results
Cytotoxicity of tt-DDE
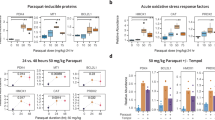
Figure 1 demonstrated viability of H9c2 cells after they had been co-cultured with different concentrations of tt-DDE for 24 hours. After the treatments of tt-DDE with concentrations of 0.1 µM and 1 µM, respectively, the H9c2 cellular viability was not significantly different (87.50 ± 5.44% v.s. 80.2 ± 3.85%; P = 0.14). The treatments with 1 µM and 2 µM of tt-DDE, respectively, for 24 hours resulted in a markable decrease in the viability of H9c2 cells, from 80.2 ± 3.85% to 56.07 ± 7.38% (P < 0.05) and tt-DDE at concentrations of ≥2 µM led to a significant reduction of cell viability compared with at a concentration of 1 µM (P < 0.05). To determine the effects of tt-DDE on delayed-rectifier potassium outward current (IK) and L-type calcium channel current (ICa,L), H9c2 cells were co-cultured with tt-DDE at a concentration of 1 µM.

Viability of H9c2 cells after they had been co-cultured with different concentrations of tt-DDE for 24 h. After 24 h, tt-DDE at concentrations of ≥2 µM led to a significant reduction of cell viability. Data are mean ± standard deviation. Each measurement was performed in triplicate *P < 0.05 compared with 1 µM.
IK in H9c2 cells treated with tt-DDE-free media
IK were evoked in the H9c2 cells treated with tt-DDE-free media for 18 hours (control group) with 300 ms of depolarizing step pulses from −70 to +50 mV in 10 mV increments at a holding potential of −60 mV. As described in a previous report14, IK first appeared significantly at the membrane potential of −20 mV and the currents amplitude increased with more positive membrane potentials until it reached the at membrane potentials of 50 mV (Fig. 2a). The IK was suppressed significantly by 4-amiopyridine (4-AP) (Fig. 2a).

(a) Representative current traces for the delayed rectifier K+ outward currents (IK) measured in H9c2 cells after treatment with tt-DDE-free media for 18 h (control group), tt-DDE-containing media for 18 h (1 µM; tt-DDE group) and 4-amiopyridine (5 mM; 4-AP).The IK were elicited by 300 ms of depolarizing step pulses from −70 to +50 mV at a holding potential of −60 mV. The IK were suppressed significantly by 4-AP. (b) The average relationship between the IK (pA/pF) and membrane potential in the control group (squares), the tt-DDE group (black circles) and 4-AP group (triangles) (n = 10). Compared with the control group, the IK were significantly decreased at membrane potentials from 0 to +50 mV in the tt-DDE group and 4-AP groups. Compared with 4-AP group, the IK were significantly decreased at membrane potentials from 40 to 50 mV in the tt-DDE group. *P < 0.05 compared with the control group. #P < 0.05 compared with the 4-AP group.
Effects of tt-DDE on IK
After treatment with tt-DDE-containing media for 18 hours (tt-DDE group), IK were evoked in the H9c2 cells with 300 ms of depolarizing step pulses from −70 to +50 mV in 10 mV increments at a holding potential of −60 mV. Compared with the activation pattern of the IK in the control group, the IK amplitudes in the cells of this group were significantly smaller (Fig. 2a). The average relationships between the IK (pA/pF) currents and membrane potentials in the control and tt-DDE groups are analyzed in Fig. 2b (n = 10), which shows that the IK in the tt-DDE group were significantly lower than those in the control group from 0 to 50 mV (all P < 0.05; Fig. 2b).
ICa,L in H9c2 cells treated with tt-DDE-free media
A depolarizing single pulse with 0 mV was applied for 300 ms at a holding potential of −80 mV to record the inward ICa,L current in the control group. The ICa,L current was recorded, and it was significantly suppressed by verapamil (Fig. 3a).

(a) Representative current traces for the L-type Ca2+ channel current (ICa,L) measured in H9c2 cells after treatment with tt-DDE-free media for 18 hours (control group), tt-DDE-containing media for 18 hours (1 µM; tt-DDE group) and verapamil (1 μM). The ICa,L were elicited by a depolarizing single pulse of 0 mV for 300 ms at a holding potential of −80 mV. The ICa,L were significantly suppressed by verapamil. (b) Comparison of the ICa,L density in the control, tt-DDE and verapamil groups. The ICa,L were significantly decreased in the tt-DDE and verapamil groups than in the control group (n = 6). Data are mean ± standard deviation; *P < 0.05 compared with the control; #P < 0.05 compared with the tt-DDE group.
Effects of tt-DDE on the ICa,L
ICa,L in the tt-DDE group were evoked by a depolarizing single pulse with 0 mV for 300 ms at a holding potential of −80 mV (Fig. 3a). The ICa,L current were significantly decreased in this group than in the control group (−0.55 ± 0.05 v.s. −0.81 ± 0.07 pA/pF, respectively, n = 6; P < 0.001; Fig. 3b).
Effects of tt-DDE on the expression of Kv2.1 and Cav1.2
The IK and ICa,L recorded in the H9c2 cells were generated by the activation of potassium (K+) channels and L-type calcium (Ca2+) channels composed mainly of Kv2.1 α-subunits and Cav1.2 subunits, respectively14,15. Compared with the control group, the expressions of Kv2.1 in the tt-DDE group was significantly decreased (0.36 ± 0.06 v.s. 0.25 ± 0.05; P = 0.003) (Fig. 4a). The expression of Cav1.2 in the control and tt-DDE groups was 0.5 ± 0.02 and 0.44 ± 0.07, respectively, which was not a statistically significant difference (P = 0.35) (Fig. 4b).

Expression of Kv2.1 (a) and Cav1.2 (b) measured by western blotting in the H9c2 cells after treatment with tt-DDE-free media for 18 hours (control group), tt-DDE-containing media for 18 hours (1 µM; tt-DDE group). Compared with the control group, the expression of Kv2.1 was significantly decreased in the tt-DDE group. In contrast, expression of Cav1.2 did not significantly differ between the two groups. Data are mean ± standard deviation; *P < 0.05 compared with the control.
Discussions
After the H9c2 cells had been exposed to tt-DDE, the IK and ICa,L were significantly decreased. The expression of Kv2.1, a component of the K+ channel, unlike that of Cav1.2, a component of the Ca2+ channel, was also significantly decreased in these cells. These changes in IK and ICa,L that were induced by tt-DDE may help to explain the association between cardiac arrhythmogenesis and cooking-oil fumes.
Many studies have demonstrated an association between air pollution and cardiac arrhythmias4,5,6,7. Gold et al. investigated the association between the level of ambient pollution and cardiovascular function3. They found that exposure to PM2.5 and ozone could decrease vagal tone, resulting in reduced heart rate variability. As previous studies, air pollution is associated with changes in cardiac ventricular repolarization, regardless of the duration of exposure7,16. The APACR study showed that increases of 10 µg/m3 in the average PM2.5 concentration were associated with 8% and 3% increases in the average premature ventricular contraction count in the same and subsequent 30 min periods, respectively5. Link et al. studied the association between air pollution and cardiac arrhythmias in patients with implantable cardioverter defibrillators. They found that PM2.5 exposure was associated with an increased risk of atrial fibrillation within the subsequent hours in patients with known cardiac disease6. Indoor air pollution has also contributed to changes in heart rate variability and electrocardiography. A study of housewives in Taiwan showed that indoor exposure to PM2.5, especially during stir-frying, cleaning with detergents, and burning incense, was associated with changes in the heart rate variability index11. Collectively, these results suggest that indoor air pollution, especially in the kitchen, may contribute to cardiac arrhythmogenesis. However, the mechanisms by which arrhythmogenesis is caused by air pollution have not been well studied.
Cooking-oil fumes are major air pollutants in the kitchen. There is abundant tt-DDE in cooking-oil fumes, and exposure to cooking-oil fumes containing tt-DDE could induce oxidative stress and genotoxicity in human lung cells13. Also, tt-DDE could induce the generation of reactive oxygen species and cell death in lung cells17. However, the cytotoxicity of tt-DDE to cardiomyocytes is seldom discussed.
Triggered activity, abnormal automaticity, and re-entry are major mechanisms of cardiac arrhythmogenesis. Alterations of function in ion channels and ion currents in cardiomyocytes could result in triggered activity and cardiac arrhythmias. In the current study, we found that after 18 hours of exposure to tt-DDE, the IK and ICa,L in H9c2 cells were significantly decreased. This effect may prolong the duration of the action potential of cardiomyocytes, which could increase vulnerability to cardiac arrhythmogenesis.
This study also showed that the expression of Kv2.1 was significantly decreased in H9c2 cells treated with tt-DDE. This decrease in the expression of Kv2.1 in H9c2 cells could be one of the mechanisms of decreasing the IK in H9c2 cells treated with tt-DDE. In contrast, the expression of Cav1.2 in the H9c2 cells was not significantly affected by treatment with tt-DDE. This suggests that the toxic effect of tt-DDE on the ICa,L in cardiomyocytes may not directly affect the L-type Ca2+ channel. The effects of tt-DDE on the IK and ICa,L in cardiomyocytes should be further investigated.
Study limitations
There are some study limitations in this study. First, the effects of tt-DDE on the IK and ICa,L of H9c2 cells were determined using only one concentration of tt-DDE (1 µM). We did not analyze effects of tt-DDE on IK and ICa,L with different concentrations of tt-DDE. Results of this study can not conclude the concentration-related effects of tt-DDE on the Ik and ICa,L of H9c2 cells. However, results of this study suggested that tt-DDE could affect the Ik and ICa,L of H9c2 cells. Second, although decrease of the IK and ICa,,L of H9c2 cells by exposure to 1 µM tt-DDE demonstrated in vitro in this study, how much and how long exposure to cooking-oil fume could achieve similar effects by exposure of 1 µM tt-DDE in vivo were unknown. Further studies in vivo are needed.
Conclusion
Exposure to tt-DDE has adverse effects leading to decrease in the IK and ICa,L of cardiomyocytes. This decrease in the IK may be related to decreased expression of the Kv2.1. Decreases in both IK and ICa,L of cardiomyocytes could prolong the action potential of cardiomyocytes and contribute toward vulnerability to arrhythmogenesis. These may be the mechanisms involved in the development of cardiac arrhythmias associated with exposure to cooking-oil fumes.
Methods
Cell culture
We used H9c2 cells (ATCC CLR-1446; Rockville, MD, USA) derived from rat embryonic myoblasts as an in vitro model of cardiomyocytes biology, since they show similar ions currents responses to primary adult and neonatal cardiomyocytes. The cells were plated onto collagen-coated culture dishes and cultured in Dulbecco’s Modified Eagle’s Medium supplemented with 10% fetal bovine serum in a humidified atmosphere of 5% CO2 and 95% air at 37 °C14,18. Cells were used under the 20th passage.
Cytotoxicity assay
The viability of H9c2 cells in tt-DDE-containing media was determined in an assay using the Cell Counting Kit-8 (CCK-8; Dojinodo Molecular Technologies, Gaithersburg, MD, USA). The CCK-8 assay was based on the conversion of a water-soluble tetrazolium salt, 2-(2-methoxy-4-nitrophenyl)-3-(4-nitrophenyl)-5-(2,4-disulfophenyl)-2H-tetrazolium, monosodium salt, to a water-soluble formazan dye upon reduction by dehydrogenases in the presence of an electron carrier19. The CCK-8 assay was performed according to the kit’s manual protocol. Briefly, the H9c2 cells were seeded in 96-well plates and incubated either with 0.1% DMSO or one of several concentrations (0.1 µM, 1 µM, 2 µM, 2.5 µM, 3 µM, 4 µM, and 5 µM) of tt-DDE for 24 hours. The CCK-8 solution was added before the cells were incubated for 3 hours at 37 °C. The absorbance of each well was measured at 450 nm using a Microplate Reader (Bio-Rad, Hercules, CA, USA). Each measurement was performed in triplicate.
Determination of IK and ICa,L in H9c2 cells
The IK were measured using the whole-cell patch clamp method previously described in detail14,20. In brief, H9c2 cells treated with (tt-DDE group) or without (control group) tt-DDE-containing media for 18 hours were detached with 0.25% trypsin-0.02% EDTA solution, the supernatant was removed by centrifugation, and the pellets were resuspended in 1 ml of bath solution containing (in mM): 60 NaCl, 80 Na-gluconate, 0.1 CaCl2, 1 MgCl2, 5 KCl, 10 HEPES, and 10 glucose (pH 7.4, NaOH). A recording electrode was pulled from borosilicate glass (resistance: 4–7 MΩ), and the pipette was coated with sticky wax close to the tip to reduce capacitance, backfilled with pipette solution containing (in mM): 0.5 MgCl2, 30 KCl, 110 K-gluconate, 10 EGTA, 5 HEPES, 5 Na2ATP, and 1 GTP-tris (pH 7.2, KOH). and gently lowered onto an H9c2 cell. Negative pressure was briefly applied to rupture the membrane, and a gigaohm seal was obtained. Cells were subsequently voltage clamped. The IK were recorded using an Axopatch 700 A amplifier (Axon Instruments, Union City, CA, USA), filtered at 1 kHz using a low-pass Bessel filter, digitized at 5 kHz, and stored on a computer for subsequent analysis with Clampfit 10.2(Molecular Devices, San Jose, CA, USA). A 1 M NaCl-agar salt bridge between the bath and the Ag-AgCl reference electrode was used to minimize offset potentials. All electrical recordings were performed at room temperature.
To measure the ICa,L through L-type Ca2+ channels, perforated whole-cell patch clamp electrophysiology was used in H9c2 cells treated with (tt-DDE group) or without (control group) tt-DDE-containing media (1 µM) for 18 hours. This technique was previously described in detail18. In brief, H9c2 cells were placed in a recording dish and perfused with a bath solution containing (in mM): 135 tetraethylammonium (TEA)-Cl, 1.8 CaCl2, 2 MgCl2, 10 glucose, and 10 HEPES (pH 7.4, Tris) using a fire polished glass pipette. To minimize outward potassium currents, Cs+ rather than K+ was used in the pipette solution. A recording electrode was pulled from borosilicate glass (resistance: 3–5 MΩ), and the pipette was coated with sticky wax close to the tip to reduce capacitance and backfilled with pipette solution containing (in mM): 140 CsCl, 1 EGTA, 1 MgCl2, 5 Na2ATP, and 5 HEPES (pH 7.2, Tris). Membrane currents were recorded using the MultiClamp 700 A amplifier, filtered at 1 kHz using a low-pass Bessel filter, digitized at 5 kHz and stored on a computer for subsequent analysis with Clampfit 10.2. A 1 M NaCl-agar salt bridge between the bath and the Ag-AgCl reference electrode was used to minimize offset potentials. All electrical recordings were performed at room temperature.
Western blot analysis
The protein levels of Kv2.1 and Cav1.2 in the H9c2 cells were analyzed using western blotting. The methods used in western blotting have previously been described in detail14,18. In brief, total protein content was extracted using a Bio-Rad Protein Assay (Bio-Rad Laboratories, Hercules, USA) and subsequently separated using a 10% denaturing acrylamide gel. The proteins were transferred to Immobilon PVDF membranes (Merck Millipore, Darmstadt, Germany) and incubated with rabbit polyclonal antibodies for Kv2.1 (Merck Millipore, Darmstadt, Germany) and Cav1.2 (Sigma-Aldrich, Darmstadt, Germany) for 1 hour at room temperature. Antibodies were diluted in TBS-Tween 1:500 for anti-Kv2.1 and anti-Cav1.2. Membranes were incubated with a secondary antibody (Merck Millipore, Darmstadt, Germany) conjugated with horseradish peroxidase. Antigen-antibody complexes were detected using enhanced chemiluminescence (Thermo Fisher Scientific Inc., Rockford, USA). Densitometric analysis was conducted using LabWorks 4.5 ImageAcquisition and Analysis software (Ultra-Violet Products Ltd., Cambridge, UK). Each measurement was performed in triplicate.
Statistical analysis
All data were expressed as mean ± standard deviation, with n indicating the number of cells. Continuous variables in the two groups (control and tt-DDE groups) were compared using non-parametric tests for two independent samples (Mann-Whitney U test). The P value less than 0.05 was considered significant. All statistical analyses were performed using SPSS software (version 11.0, SPSS, Chicago, IL, USA).
References
Samet, J. M. et al. Concentrated ambient ultrafine particle exposure induces cardiac changes in young healthy volunteers. Am. J. Respir. Crit. Care Med. 179, 1034–1042 (2009).
Brook, R. D. et al. Air pollution and cardiovascular disease: a statement for healthcare professionals from the Expert Panel on Population and Prevention Science of the American Heart Association. Circulation 109, 2655–2671 (2004).
Gold, D. R. et al. Ambient pollution and heart rate variability. Circulation 101, 1267–1273 (2000).
Brook, R. D. et al. Particulate matter air pollution and cardiovascular disease: An update to the scientific statement from the American Heart Association. Circulation 121, 2331–2378 (2010).
Liao, D. et al. Fine particulate air pollution is associated with higher vulnerability to atrial fibrillation–the APACR study. J. Toxicol. Env. Health A 74, 693–705 (2011).
Link, M. S. et al. Acute exposure to air pollution triggers atrial fibrillation. J. Am. Coll. Cardiol. 62, 816–825 (2013).
Sivagangabalan, G. et al. The effect of air pollution on spatial dispersion of myocardial repolarization in healthy human volunteers. J. Am. Coll. Cardiol. 57, 198–206 (2011).
Creason, J. et al. Particulate matter and heart rate variability among elderly retirees: the Baltimore 1998 PM study. J. Expo. Anal. Env. Epidemiol. 11, 116–122 (2001).
An, Z., Jin, Y., Li, J., Li, W. & Wu, W. Impact of Particulate Air Pollution on Cardiovascular Health. Curr. Allergy Asthma Rep. 18, 15 (2018).
Young, B. N. et al. Exposure to household air pollution from biomass cookstoves and blood pressure among women in rural Honduras: A cross-sectional study. Indoor Air 29 (2019).
Huang, Y. L. et al. Personal exposure to household particulate matter, household activities and heart rate variability among housewives. PLoS One 9 (2014).
Lai, C. H. et al. Exposure to cooking oil fumes and oxidative damages: a longitudinal study in Chinese military cooks. J. Expo. Sci. Env. Epidemiol. 23, 94–100 (2013).
Young, S. C. et al. DNA damages induced by trans, trans-2,4-decadienal (tt-DDE), a component of cooking oil fume, in human bronchial epithelial cells. Environ Mol Mutagen 51 (2010).
Lee, K. T. et al. Differential effects of central and peripheral fat tissues on the delayed rectifier K(+) outward currents in cardiac myocytes. Cardiology 125, 118–124 (2013).
Tang, Z. Z. et al. Differential splicing patterns of L-type calcium channel Cav1.2 subunit in hearts of Spontaneously Hypertensive Rats and Wistar Kyoto Rats. Biochim Biophys Acta 1783 (2008).
Van Hee, V. C. et al. Association of long-term air pollution with ventricular conduction and repolarization abnormalities. Epidemiology 22, 773–780 (2011).
Lin, P. P. et al. Proteomic analysis of proteins associated with tt-DDE induced toxicity in BEAS-2B cells. Biochem Biophys Res Commun 376 (2008).
Kuo, H. F. et al. A xanthine-derivative K(+)-channel opener protects against serotonin-induced cardiomyocyte hypertrophy via the modulation of protein kinases. Int. J. Biol. Sci. 10, 64–72 (2013).
Han, S. B., Shin, Y. J., Hyon, J. Y. & Wee, W. R. Cytotoxicity of voriconazole on cultured human corneal endothelial cells. Antimicrob. Agents Chemother. 55, 4519–4523 (2011).
Wu, B.-N., Tu, H.-F., Welsh, D. G. & Chen, I.-J. KMUP-1 activates BKCa channels in basilar artery myocytes via cyclic nucleotide-dependent protein kinases. Br. J. Pharmacol. 146, 862–871 (2005).
Acknowledgements
The study was supported by Kaohsiung Medical University Hospital Research Project (Grant number: KMUH105-5R10). The study was funded by Kaohsiung Medical University Hospital (Grant number: KMUH105-5R10). The article does not contain any studies with human participants or animals performed by any of the authors.
Author information
Authors and Affiliations
Contributions
Shih-Jie Jhuo, and I-Hsin Liu drafted the manuscript. Shih-Jie Jhuo performed cell culture. I-Hsin Liu and Bin-Nan Wu performed the whole-cell patch clamp to measure IK and ICa,L and Western blot analysis. Wei-Chung Tsai, and Kun-Tai Lee prepared figures and helped statistical analysis. Bin-Nan Wu, Kun-Tai Lee and Wen-Ter Lai conceived of the study, participated in its design, revise the manuscript and coordination. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jhuo, SJ., Liu, IH., Tsai, WC. et al. Effects of Trans, Trans-2,4-decadienal on the Ions Currents of Cardiomyocytes: Possible Mechanisms of Arrhythmogenesis Induced by Cooking-oil Fumes. Sci Rep 10, 5771 (2020). https://doi.org/10.1038/s41598-020-62733-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-62733-1
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
