
Abstract
The interactions of antibodies with myeloid Fcγ receptors and the complement system are regulated by an Asn297-linked glycan in the Fc portion of IgG. Alterations of serum IgG-Fc glycosylation have been reported in various autoimmune diseases, and correlate with treatment response and disease activity. We hypothesized that IgG-Fc glycosylation is altered in immune thrombocytopenia (ITP) and associates with response to anti-CD20 monoclonal antibody treatment (rituximab). IgG-Fc glycosylation was analyzed by liquid chromatography-mass spectrometry. We found that IgG-Fc glycosylation was identical between refractory ITP patients (HOVON64 trial; N = 108) and healthy controls (N = 120). Two months after rituximab treatment, we observed a shift in Fc glycosylation, with a mean 1.7% reduction in galactosylation for IgG1 and IgG4 and a mean 1.5% increase for bisection in IgG1, IgG2/3 and IgG4 (adjusted p < 1.7 × 10−3 and p < 2 × 10−4, respectively). Neither baseline nor longitudinal changes in IgG-Fc glycosylation after rituximab were associated with clinical treatment response. We conclude that IgG-Fc glycosylation in refractory ITP is similar to healthy controls and does not predict treatment responses to rituximab. The observed changes two months after treatment suggest that rituximab may influence total serum IgG-Fc glycosylation. Overall, our study suggests that the pathophysiology of refractory ITP may differ from other autoimmune diseases.
Similar content being viewed by others


Introduction
Immune thrombocytopenia (ITP) is an autoimmune bleeding disease characterized by self-reactive cellular and humoral anti-platelet responses that result in platelet clearance. A hallmark of ITP in adults are IgG-anti-platelet autoantibodies1. The diagnosis of ITP is established clinically by exclusion of alternative causes of thrombocytopenia2, which is thought to result in diagnostic heterogeneity. Rituximab, an anti-CD20 antibody targeting B cells, represents an important second-line treatment, with about 60% of patients responding. The underlying working mechanisms remain incompletely understood3,4,5.
The Fc portion of each heavy chain of an IgG molecule has a single glycosylation site at Asn297. The exact composition of the attached N-glycan affects effector functions through modification of the Fc-tail affinity for Fcγ receptors and C1q-mediated complement activation6. The total serum IgG-Fc glycosylation is skewed in multiple autoimmune diseases, such as rheumatoid arthritis7,8, autoimmune hemolytic anemia9, systemic lupus erythematosus10, Guillain-Barre syndrome11, vasculitis12,13 and inflammatory bowel disease14. Across these studies, the strongest association with autoimmune diseases is a reduction in Asn-297 galactosylation, followed by sialylation, which are linked because galactosylated glycan structures are substrates for sialyltransferases6. Moreover, GWAS-identified loci that regulate Fc N-glycosylation are strongly associated with susceptibility to autoimmune diseases15.
In rheumatoid arthritis, extensive data indicate that a low total IgG-Fc galactosylation correlates with symptom onset and disease activity16,17,18,19,20. The low galactosylation reverts towards normal levels during treatment or spontaneous recovery, as observed during pregnancy21,22,23. In Guillain-Barrè syndrome and Kawasaki disease, IVIg-responses correlate with IgG-Fc glycosylation profiles before treatment as well as with treatment-induced changes of Fc glycosylation11,24.
Immunotherapy with immunomodulating biologicals can affect the IgG glycosylation, reflecting direct and indirect effects on the immune system. For instance, the reduced IgG galactosylation in rheumatoid arthritis, psoriatic arthritis and spondyloarthropathy were found to revert towards normal levels after anti-TNFα immunotherapy23,25,26, and this correlated with associated changes in CRP levels27. The effect of B cell depleting antibody therapy, such as rituximab, has however not been studied.
In the present study, we tested if serum IgG-Fc glycosylation is altered in ITP, similar to other autoimmune diseases. We further hypothesized that baseline or dynamic changes of IgG-Fc glycosylation may predict treatment response to rituximab.
Results
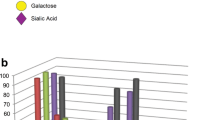
The N-linked Fc glycan composition at position Asn297 found in all IgG subclasses (Fig. 1A) was analyzed in 108 ITP patients and 120 age- and sex-matched healthy controls. Patients were randomized to one of three treatment schemes (detailed in methods; Fig. 1B)28. IgG2 and IgG3 results are analyzed together (IgG2/3) because of overlapping peptide moieties29.

IgG1-Fc glycosylation is similar between patients with immune thrombocytopenia and healthy controls. (A) An example of complex-type IgG-linked Fc glycan as found in our samples: a diantennary, digalactosylated, disialylated N-glycan carrying a core fucose and a bisecting N-acetylglucosamine (GlcNAc). (B) Patients with refractory ITP (N = 108) were randomized to three treatment schemes of rituximab (detailed in method section). (C–E) Overview of IgG1-, IgG2/3- and IgG4-Fc glycan traits in ITP (N = 108) and healthy controls (N = 120). Data are individual patient measurements (mean ± SEM). Indicated p-values are given for the effect of ITP in a linear model of the respective Fc glycan, adjusted for covariates age and sex, and corrected for multiple comparisons.
Unlike observations made for other autoimmune diseases, ITP patients showed a total IgG-Fc glycosylation similar to healthy controls (Fig. 1C–E). In particular, there was no reduction of IgG1 galactosylation in ITP. Importantly, we did observe the expected age-dependent differences in healthy controls as well as excellent reproducibility in technical controls (N = 25, coefficient of variation, 4.9%; data not shown). The only statistically significant finding was a minor absolute difference in the level of IgG1 hybrid-type Fc glycans (Fig. 1C), with higher levels in the patient group. As this hybrid glycan-type, containing a mannose on the α1,6 arm of the glycan, comprises only a very small fraction of the Fc glycan repertoire of total serum IgG (generally <1%), it is unlikely that this is of functional significance.
To evaluate the impact of rituximab on Fc glycosylation, we compared paired samples obtained before and 60 days after start of treatment (N = 41; Fig. 2), which is well beyond the IgG half-life of 21 days30. We observed statistically significant changes in the composition of Asn297-linked Fc glycans of most IgG subclasses, but not for IgG1 fucosylation, IgG2/3 fucosylation or IgG2/3 galactosylation (Fig. 2; IgG2/3 and IgG4 data not shown). There were no differences in the direction of change between the allocated treatment regimens. The observed changes on absolute glycan levels were minor: the largest effect after rituximab treatment was a mean 1.7% reduction in IgG1 and IgG4 galactosylation, followed by a mean 1.5% increase in Fc-bisection for all IgG subclasses (adjusted p < 1.7 × 10−3 and p < 2 × 10−4, respectively).

Rituximab treatment has complex effects on IgG1-Fc glycosylation. Paired samples of immune thrombocytopenia patients (N = 41) were assessed before and 60 days after rituximab treatment. Data are individual patient measurements (mean ± SEM). p-values are given for a paired t-test, corrected for multiple comparisons.
Baseline IgG glycosylation could be predictive of response to immunomodulatory therapy, as shown for Guillain-Barrè syndrome or Kawasaki disease11,24. Therefore, we assessed if IgG-Fc glycosylation were associated with a clinical response to rituximab. Of patients with available platelet response data two months after rituximab, 22 patients had a complete response (CR; platelet count ≥100 × 109 L−1), 37 a partial response (PR; platelet count ≥30 × 109 L−1), and 30 no response (NR)31. We observed no association between levels of IgG1-Fc glycosylation traits before rituximab administration and platelet responses (Fig. 3A).

IgG1-Fc glycosylation is not associated with response to rituximab. (A) Baseline levels of IgG1-Fc glycans and response to rituximab 60 days after treatment. (B) Dynamic changes (day 60 minus baseline levels) in IgG1-Fc glycans are not associated with response to rituximab in paired samples. Data are individual patient measurements (mean ± SEM). p-values are given for ANOVA (adjusted for age and sex for the baseline levels). This was a secondary, exploratory analysis and p-values were not corrected for multiple comparisons.
ITP is a heterogeneous disorder and a subgroup of ITP patients has no anti-platelet antibodies and responds differently to rituximab treatment5. However, total IgG-glycosylation levels between antibody positive and negative patients were similar, and there was no association between IgG-glycosylation with response for either of these subgroups (Supplementary Table). Moreover, in patients with paired samples before and 2 months after rituximab treatment (CR, N = 15; NR, N = 11; PR, N = 13), there was no relationship between baseline levels or change in IgG1-Fc glycans and platelet response (Fig. 3B).
Discussion
In contrast to our hypothesis, we unexpectedly found that refractory ITP patients showed no skewing of IgG-Fc glycosylation, which is observed - in particular with a low total serum IgG-galactosylation - in other autoimmune diseases9,10,11,13,16. Our findings may suggest that the pathophysiological mechanisms in ITP are different from other antibody-mediated autoimmune diseases, where IgG-glycosylation shows clear associations with disease onset and progression(in particular also autoimmune hemolytic anemia9).
The exact mechanism by which IgG Fc-galactosylation and sialylation is reduced in autoimmune diseases and inflammation is unknown. Lowered IL-6 has been associated with decreased IgG Fc-galactosylation32,33. As IL-6 is a primary cytokine of the acute-phase response and subsequent inflammation, the possibility exists that Fc-galactosylation is indirectly associated with inflammation. Ultimately, the increased serum levels and B cell expression of beta-galactosidase, an enzyme that cleaves terminal galactose residues, might be one of the involved pathways34. Moreover, IL-21 and IL-22 produced by Th17 cells may instruct B cells to reduce expression of St6Gal1, which leads to asialylated IgG species18. Why these pathways are apparently not affected in ITP is unclear. We speculate that heterogeneity in the clinical background of ITP may be one of the reasons that we could not detect any change in IgG Fc-glycosylation. First, it is known that a proportion of patients initially diagnosed as ITP may have other, non-immune causes of thrombocytopenia35. Previous work by our group and others has indicated that treatment-refractory patients may not have any detectable anti-platelet antibodies in the first place5,36, and CD8-T cell mediated platelet clearance could be an alternative mechanism that maintains thrombocytopenia37,38.
We report for the first time that rituximab treatment alters serum IgG glycosylation. The observed changes were minor, the most pronounced being an increase of bisecting GlcNAcs and a decrease in galactosylation after treatment. These changes in IgG-Fc glycosylation are perhaps not surprising as rituximab depletes circulating and lymph-node resident CD20+ B cells for >2–6 months39,40. Although the precise regulation of IgG-Fc glycosylation is still incompletely elucidated, it is clear that B cell glycosyltransferases regulate the glycosylation in an antigen-specific manner41,42,43,44. Importantly, rituximab does not affect IgG levels40,45,46, suggesting that these are maintained by CD20-negative plasma cells. Although there were effects of rituximab on IgG glycosylation, these changes did not associate with the clinical response to rituximab (Fig. 3).
Therefore, in ITP, it is likely that rituximab exerts its immunomodulatory effects through other mechanisms, e.g. IgM positive B cells, an influence on T cell balance47, the induction of regulatory B cells48, or simply through reduction of anti-platelet antibodies in ITP5. Whether glycosylation of those pathogenic antibodies is affected is still unknown and remains challenging to investigate due to the minute amount of these antibodies.
Our study focused on refractory ITP patients who all had long-standing and ongoing disease. This implied that they had already received first-line treatment with corticosteroids, which might have affected changes in IgG glycosylation. However, patients treated with high-dose corticosteroids within three weeks were not eligible for trial participation. One study found that corticosteroids reduced IgG1 Fc-galactosylation and -sialylation slightly in patients with inflammatory bowel disease14. Accordingly, if corticosteroid would have affected the present results, it would have been expected to result in lowered IgG1 Fc-galactosylation and -sialylation, which we did not observe. A further limitation of our study was that we did not have an untreated control group, and the changes 60 days after rituximab administration may theoretically represent the natural course of disease and not rituximab treatment per se.
In conclusion, IgG-Fc glycosylation in ITP patients was similar to healthy controls, and no association was found with treatment outcomes after rituximab. Rituximab treatment may have an effect on total serum IgG Fc-glycosylation, as observed two months after treatment. Our data suggest that the pathophysiology of refractory ITP may differ from other autoimmune diseases.
Methods
Study subjects
Adult refractory ITP samples were included from the Dutch Hemato-Oncology Cooperative Group (HOVON) HOVON64 study28, a randomized controlled multicenter trial in the Netherlands. In brief, patients with relapsed or refractory ITP above 18 years who completed first-line treatment with corticosteroids and had at least 2 platelets counts ≤30 × 109 L−1 and a WHO performance status of 0–2 were eligible for inclusion. Patients were not eligible for study entry if they received treatment with pulsed or high dose corticosteroids, IVIG or splenectomy less than 3 weeks before randomization. Further exclusion criteria included prior treatment with rituximab, active grade 3 or 4 bleeding (by NCI CTCAE v3.0 criteria), the presence of malignancies, systemic infections or systemic autoimmune disorders. Patients were randomized into three arms to receive (A) 4 weekly doses of 375 mg/m2 body surface area rituximab, (B) 2 weekly doses of 375 mg/m2 rituximab, with potential extension to receive 2 additional doses in case of no response, or (C) 2 weekly doses of 750 mg/m2 rituximab. The study was approved by the medical ethical committee of Academic Medical Center Amsterdam and all participants gave written informed consent. Splenectomized patients were excluded for the present study. The median age of the patients was 52 years (interquartile range [IQR], 35–64) and 58% were female. The median time between ITP diagnosis and start of rituximab was 1.06 years (IQR 0.34–3.14). Control samples were obtained from age- and sex-matched healthy Dutch blood donors by antecubital venipuncture before a blood donation (Sanquin, Amsterdam; The Netherlands). The study was performed under Dutch national guidelines (Human Tissue and Medical Research: Code of conduct for responsible use; https://www.federa.org/codes-conduct) and conducted in accordance with the Declaration of Helsinki. All analyses were performed on coded, de-identified data. Stored serum or plasma samples (−20 °C) were used for analyses of IgG-Fc glycosylation by LC-MS.
IgG-Fc glycosylation
IgG was isolated using protein G affinity beads (GE Healthcare, Uppsala, Sweden), as previously described9. After washing the beads, IgG was eluted with formic acid, dried in a vacuum concentrator, trypsin digested and stored at −20 °C. Analysis of the tryptic IgG-Fc glycopeptides was performed with nanoLC-reversed phase-electrospray-quadrupole time-of-flight (QTOF)-mass spectrophotometry (MS) on an Ultimate 3000 RSLCnano system (Dionex Corporation, Sunnyvale, CA) coupled to an Impact QTOF-MS (Bruker Daltonics, Bremen, Germany)49,50. The nanoLC-MS data was processed using LaCyTools51, as previously described9.
Statistical analysis
Statistical analyses were performed in R version 3.4.1. A sample size calculation was performed assuming similar differences in IgG1 galactosylation as observed before in autoimmune hemolytic anemia9, with a mean difference of 10% and standard deviation of 8%. For a power of 0.9 and a significance level of 0.001, 30 individuals were required in each group. Additional samples were included based on availability. Due to the age and sex dependency of IgG glycans52, groups were compared by constructing a linear model for each glycan, adjusted for age and sex as covariate. Paired samples were evaluated by a paired t-test. Reported p-values for the primary analysis (Figs. 1 and 2) were adjusted for multiple testing by false discovery rate (FDR). P-values in the secondary analysis (Fig. 3), using ANOVA, were not adjusted. A two-tailed p-value < 0.05 was considered statistically significant.
References
Porcelijn, L. et al. Detection of platelet autoantibodies to identify immune thrombocytopenia: state of the art. British Journal of Haematology. 39(Suppl. 1), 195 (2018 May 29).
Neunert, C. et al. The American Society of Hematology 2011 evidence-based practice guideline for immune thrombocytopenia. Blood. 117, 4190–207 (2011).
Patel, V.L. et al. Outcomes 5 years after response to rituximab therapy in children and adults with immune thrombocytopenia. Blood. American Society of Hematology; 119(25), 5989–95 (2012 Jun 21).
Godeau, B. & Stasi R. Is B-cell depletion still a good strategy for treating immune thrombocytopenia? La Presse Medicale. Elsevier Masson SAS; 43(4), e79–e85 (2014 Apr 1).
Porcelijn, L. et al. Lack of detectable platelet autoantibodies is correlated with non-responsiveness to rituximab treatment in ITP patients. Blood. blood–2016–11–751719–9 (2017 May 3).
Dekkers, G. et al. Decoding the Human Immunoglobulin G-Glycan Repertoire Reveals a Spectrum of Fc-Receptor- and Complement-Mediated-Effector Activities. Front Immunol. 8, 877 (2017).
Parekh, R. B. et al. Association of rheumatoid arthritis and primary osteoarthritis with changes in the glycosylation pattern of total serum IgG. Nature. 316(6027), 452–7 (1985 Aug).
Tomana, M., Schrohenloher, R. E., Koopman, W. J., Alarcón, G. S. & Paul, W. A. Abnormal glycosylation of serum IgG from patients with chronic inflammatory diseases. Arthritis Rheum. 31(3), 333–8 (1988 Mar).
Sonneveld, M. E. et al. Patients with IgG1-anti-red blood cell autoantibodies show aberrant Fc-glycosylation. Sci Rep. 7(1), 8187 (2017 Aug 15).
Vučković, F. et al. Association of systemic lupus erythematosus with decreased immunosuppressive potential of the IgG glycome. Arthritis Rheumatol. Wiley-Blackwell; 67(11), 2978–89 (2015 Nov).
Fokkink, W.-J. R. et al. IgG Fc N-glycosylation in Guillain-Barré syndrome treated with immunoglobulins. J. Proteome. Res. American Chemical Society; 13(3), 1722–30 (2014 Mar 7).
Holland, M. et al. Differential glycosylation of polyclonal IgG, IgG-Fc and IgG-Fab isolated from the sera of patients with ANCA-associated systemic vasculitis. Biochim Biophys Acta. 1760(4), 669–77 (2006 Apr).
Wuhrer, M. et al. Skewed Fc glycosylation profiles of anti-proteinase 3 immunoglobulin G1 autoantibodies from granulomatosis with polyangiitis patients show low levels of bisection, galactosylation, and sialylation. J. Proteome. Res. 14(4), 1657–65 (2015 Apr 3).
Šimurina, M. et al. Glycosylation of Immunoglobulin G Associates With Clinical Features of Inflammatory Bowel Diseases. Gastroenterology. 154(5), 1320–1333.e10 (2018 Apr).
Lauc, G. et al. Loci Associated with N-Glycosylation of Human Immunoglobulin G Show Pleiotropy with Autoimmune Diseases and Haematological Cancers. Gibson G, editor. PLoS Genet. 9(1), e1003225–17 (2013 Jan 31).
Bondt, A. et al. ACPA IgG galactosylation associates with disease activity in pregnant patients with rheumatoid arthritis. Ann. Rheum. Dis; annrheumdis–2018–212946 (2018 Apr 3).
Parekh, R. B. et al. Galactosylation of IgG associated oligosaccharides: reduction in patients with adult and juvenile onset rheumatoid arthritis and relation to disease activity. Lancet. 1(8592), 966–9 (1988 Apr 30).
Pfeifle, R. et al. Regulation of autoantibody activity by the IL-23-TH17 axis determines the onset of autoimmune disease. Nat. Immunol. Nature Publishing Group, 18(1), 104–13; (2017 Jan).
Rook, G. A. et al. Changes in IgG glycoform levels are associated with remission of arthritis during pregnancy. J. Autoimmun. 4(5), 779–94 (1991 Oct).
van de Geijn, F. E. et al. Immunoglobulin G galactosylation and sialylation are associated with pregnancy-induced improvement of rheumatoid arthritis and the postpartum flare: results from a large prospective cohort study. Arthritis Research & Therapy. Bio. Med. Central. 11(6), R193 (2009).
Bondt A. et al. Association between galactosylation of immunoglobulin G and improvement of rheumatoid arthritis during pregnancy is independent of sialylation. J. Proteome Res. 12(10), 4522–31 (2013 Oct 4).
Gińdzieńska-Sieśkiewicz, E. et al. Changes of glycosylation of IgG in rheumatoid arthritis patients treated with methotrexate. Adv. Med. Sci. 61(2), 193–7 (2016 Sep).
Pasek, M. et al. Galactosylation of IgG from rheumatoid arthritis (RA) patients – changes during therapy. Glycoconjugate Journal. 23(7–8), 463–71 (2006 Nov).
Ogata, S. et al. Treatment response in Kawasaki disease is associated with sialylation levels of endogenous but not therapeutic intravenous immunoglobulin G. Stover CM, editor. PLoS ONE. Public Library of Science 8(12), e81448 (2013).
Croce, A. et al. Effect of infliximab on the glycosylation of IgG of patients with rheumatoid arthritis. Journal of clinical laboratory analysis. 21(5), 303–14 (2007).
Van Beneden, K. et al. Reversible changes in serum immunoglobulin galactosylation during the immune response and treatment of inflammatory autoimmune arthritis. Ann. Rheum. Dis. BMJ Publishing Group Ltd; 68(8), 1360–5, (2009 Aug).
Collins, E. S. et al. Glycosylation status of serum in inflammatory arthritis in response to anti-TNF treatment. Rheumatology (Oxford). 52(9), 1572–82 (2013 Sep).
Zwaginga, J. J. et al. Multi-center randomized open label phase II trial on three rituximab dosing schemes in immune thrombocytopenia patients. Haematologica. Haematologica; 100(3), e90–2 (2015 Mar).
Wuhrer, M. et al. Glycosylation profiling of immunoglobulin G (IgG) subclasses from human serum. Proteomics. 7(22), 4070–81 (2007 Nov).
Vidarsson, G., Dekkers, G. & Rispens, T. IgG subclasses and allotypes: from structure to effector functions. Front Immunol. Frontiers 5(16), 520 (2014).
Rodeghiero, F. et al. Standardization of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. American Society of Hematology; 113(11), 2386–93 (2009 Mar 12).
Nakao, H. et al. Hypogalactosylation of immunoglobulin G sugar chains and elevated serum interleukin 6 in Castleman’s disease. Clin. Chim. Acta. 197(3), 221–8 (1991 Mar 29).
Cobb, B. A. The history of IgG glycosylation and where we are now. Glycobiology. 13(433–443), 315–12 (2019 Aug 27).
Zhipeng, S., Jingjing, G., Qing, X., Yanping, W. & Yunsen, L. Possible role of β-galactosidase in rheumatoid arthritis. Modern Rheumatology. Taylor & Francis, 0(0), 1–10, (2019).
Arnold, D. M. et al. Misdiagnosis of primary immune thrombocytopenia and frequency of bleeding: lessons from the McMaster ITP Registry. Blood Adv. 3rd ed. 1(25), 2414–20 (2017 Nov 28).
Cooper, N. et al. Platelet-associated antibodies, cellular immunity and FCGR3a genotype influence the response to rituximab in immune thrombocytopenia. British Journal of Haematology. 158(4), 539–47 (2012 Aug).
Olsson, B. et al. T-cell-mediated cytotoxicity toward platelets in chronic idiopathic thrombocytopenic purpura. Nat Med. 9(9), 1123–4 (2003 Sep).
Qiu, J. et al. CD8(+) T cells induce platelet clearance in the liver via platelet desialylation in immune thrombocytopenia. Sci Rep. Nature Publishing Group;6, 27445–12 (2016 Jun 20).
Maloney, D. G. et al. IDEC-C2B8 (Rituximab) anti-CD20 monoclonal antibody therapy in patients with relapsed low-grade non-Hodgkin’s lymphoma. Blood. 90(6), 2188–95 (1997 Sep 15).
Maloney, D. G. et al. Phase I clinical trial using escalating single-dose infusion of chimeric anti-CD20 monoclonal antibody (IDEC-C2B8) in patients with recurrent B-cell lymphoma. Blood. 84(8), 2457–66 (1994 Oct 15).
Kapur, R. et al. A prominent lack of IgG1-Fc fucosylation of platelet alloantibodies in pregnancy. Blood. 123(4), 471–80 (2014 Jan 23).
Kapur, R. et al. Prophylactic anti-D preparations display variable decreases in Fc-fucosylation of anti-D. Transfusion. Wiley/Blackwell (10.1111); 55(3), 553–62 (2014 Sep 19).
Sonneveld, M. E. et al. Glycosylation pattern of anti-platelet IgG is stable during pregnancy and predicts clinical outcome in alloimmune thrombocytopenia. British Journal of Haematology. 174(2), 310–20 (2016 Jul).
Kapur, R. et al. Low anti-RhD IgG-Fc-fucosylation in pregnancy: a new variable predicting severity in haemolytic disease of the fetus and newborn. British Journal of Haematology. 166(6), 936–45 (2014 Sep).
Khellaf, M. et al. Safety and efficacy of rituximab in adult immune thrombocytopenia: results from a prospective registry including 248 patients. Blood. 124(22), 3228–36 (2014 Nov 20).
Marco, H. et al. The effect of rituximab therapy on immunoglobulin levels in patients with multisystem autoimmune disease. BMC Musculoskelet Disord. Bio. Med. Central. 15(1), 178 (2014 May 25).
Stasi R. et al. Response to B-cell depleting therapy with rituximab reverts the abnormalities of T-cell subsets in patients with idiopathic thrombocytopenic purpura. Blood. 110(8), 2924–30 (2007 Oct 15).
Gudbrandsdottir, S., Brimnes, M., Køllgaard, T., Hasselbalch, H. C. & Nielsen, C. H. Effects of rituximab and dexamethasone on regulatory and proinflammatory B-cell subsets in patients with primary immune thrombocytopenia. Eur J Haematol. 100(1), 45–52 (2018 Jan).
Falck, D, Jansen, B. C., de Haan, N. & Wuhrer, M. High-Throughput Analysis of IgG Fc Glycopeptides by LC-MS. Methods Mol Biol. New York, NY: Springer New York; 1503(Suppl 1), 31–47 (2017).
Selman, M. H. J. et al. Fc specific IgG glycosylation profiling by robust nano-reverse phase HPLC-MS using a sheath-flow ESI sprayer interface. Journal of Proteomics. 75(4), 1318–29 (2012 Feb 2).
Jansen, B. C. et al. LaCyTools: A Targeted Liquid Chromatography-Mass Spectrometry Data Processing Package for Relative Quantitation of Glycopeptides. J. Proteome Res. 15(7), 2198–210 (2016 Jul 1).
Baković, M. P. et al. High-throughput IgG Fc N-glycosylation profiling by mass spectrometry of glycopeptides. J. Proteome Res. 12(2), 821–31 (2013 Feb 1).
Acknowledgements
This work was supported by a research grant from the Landsteiner Foundation for Blood Transfusion Research (LSBR) and a doctoral stipend to D.E.S. by the Studienstiftung des Deutschen Volkes.
Author information
Authors and Affiliations
Contributions
D.E.S. and N.d.H. co-designed the study, performed laboratory experiments, analyzed and interpreted data. M.E.S. co-designed the study and performed laboratory experiments. L.P. supervised diagnostic laboratory analyses. L.P., C.E.v.d.S., M.d.H. and J.-J.Z. interpreted and discussed data. J.-J.Z. supervised clinical analyses. M.W. and G.V. co-designed and supervised the study, interpreted and discussed data. D.E.S. and G.V. wrote the manuscript. All co-authors reviewed, revised and approved the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schmidt, D.E., de Haan, N., Sonneveld, M.E. et al. IgG-Fc glycosylation before and after rituximab treatment in immune thrombocytopenia. Sci Rep 10, 3051 (2020). https://doi.org/10.1038/s41598-020-59651-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-020-59651-7
This article is cited by
-
A functional spleen contributes to afucosylated IgG in humans
Scientific Reports (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
