
Abstract
Coffee consumption is associated with cerebral hypoperfusion that may contribute to the development of cerebral white matter hyperintensities (WMH). We investigated the effect of lifetime coffee consumption on the volume of WMH (VWMH) in late life, and compared the effect between men and women since caffeine clearance may be different between sexes. We enrolled 492 community-dwelling cognitively normal elderly individuals (73.4 ± 6.7 years old on average) from the Korean Longitudinal Study on Cognitive Aging and Dementia. We evaluated their patterns and amounts of coffee consumption using a study-specific standardized interview and estimated cerebral VWMH by automatic segmentation of brain fluid-attenuated inversion recovery sequence magnetic resonance images. Higher cumulative lifetime coffee consumption was associated with higher logVWMH in both sexes (p = 0.030). The participants who consumed more than 2 cups of coffee per day on average in their lifetime showed higher logVWMH in late life than those who consumed less. When both sexes were analyzed separately, these coffee-logVWMH associations were found only in women, although the volumes of brain and white matter of women were smaller than those of men. Our findings suggest that prolonged high coffee consumption may be associated with the risk of WMH in late life.
Similar content being viewed by others


Introduction
Although numerous studies have linked coffee consumption with lower risk of stroke, diabetes mellitus (DM), cardiovascular disease (CVD), and reduced risk of developing cognitive impairment and/or dementia1,2,3,4,5, health impacts of coffee consumption on human brain has remained controversial. Coffee is a major dietary source of caffeine around the world6, and caffeine (1, 3, 7-trimethylxanthine) is associated with cerebral hypoperfusion in humans7. Regular caffeine consumption, of 2 to 4 cups of coffee a day, eliminates the protective effect of ischemic preconditioning8 and reduces global cerebral blood flow by approximately 22–30%9,10,11,12. Long-term caffeinated coffee increases blood pressure6,13,14, increases vascular resistance15, and causes arterial stiffness16 and cerebral vasoconstriction12.
White matter hyperintensities (WMH) are brain areas in the white matter (WM) that appear abnormally hyperintense on T2-weighted or fluid-attenuated inversion recovery (FLAIR) sequences of brain magnetic resonance imaging (MRI)17. Although the etiologies of WMH are not fully understood, increasing evidence suggests that a majority of WMH may be attributable to cerebral hypoperfusion and ischemic brain damages17,18,19,20,21. Hyperintense WM showed lower cerebral blood flow and cerebrovascular reactivity than normal-appearing WM22, and were associated with high blood pressure, DM, other CVD, stroke and cognitive impairments17,18,19,20,21.
Therefore prolonged coffee consumption may increase the risk of WMH in late life. Furthermore, the effects of coffee on the risk of WMH may be more pronounced in women than in men, since estradiol decreases caffeine clearance in humans23. Temple and Ziegler reported that women show greater blood pressure responses to caffeine than do men, possibly due to differences in the levels of circulating sex hormones24. Elderly women have greater WMH volume relative to their WM volume compared to men25, and have a greater progression of WMH than men26. This study aimed to investigate the association between the amount of lifetime coffee consumption and the volume of WMH (VWMH) in cognitively normal elderly individuals, and to examine whether this association is different between sexes.
Methods
Study participants
In this retrospective cohort study, we enrolled 492 community-dwelling cognitively normal elderly Koreans (204 men and 288 women) aged 60 years or above (73.4 ± 6.7 years old) at Seoul National University Bundang Hospital for the Korean Longitudinal Study on Cognitive Aging and Dementia (KLOSCAD)27. The KLOSCAD is a nationwide population-based prospective elderly cohort study that was launched in 2009. In the KLOSCAD, a total of 6,818 community-dwelling Koreans aged 60 years or older were randomly sampled from 30 villages and towns across South Korea using residential rosters. The baseline evaluation was conducted from November 2010 to October 2012, and follow-up evaluations were conducted every two years27.
All participants were fully informed regarding study participation, and written informed consent was obtained from the participants or their legal guardians. The Institutional Ethics Review Board of the Seoul National University Bundang Hospital approved the study protocol.
Assessments of clinical characteristics and diagnosis
Geriatric psychiatrists with expertise in dementia research administered in person standardized diagnostic interviews including detailed medical histories, physical and neurological examinations, laboratory tests, echocardiography and chest X-ray according to the Korean version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment Packet (CERAD-K) Clinical Assessment Battery (CERAD-K-C)28 and the Korean version of the Mini International Neuropsychiatric Interview29. A research neuropsychologist or trained research nurse administered the CERAD-K Neuropsychological Assessment Battery (CERAD-K-N)28,30, Digit Span Test31, and Frontal Assessment Battery32 to each participant. Trained research nurses collected data on body mass index (BMI), history of hypertension, diabetes mellitus (DM), and cardiovascular disease (CVD), amount of lifetime alcohol consumption (ALAC, standard unit-years), amount of lifetime smoking (ALS, pack-years), Geriatric Depression Scale (GDS)33, Pittsburgh Sleep Quality Index (PSQI)34, Cumulative Illness Rating Scale (CIRS)35, and obstructive sleep apnea as a STOP questionnaire36. We diagnosed dementia and other Axis I mental disorders. We defined normal cognition as 0 in Clinical Dementia Rating37 without any of following conditions; dementia and major psychiatric disorders according to the Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision (DSM-IV-TR) criteria38, mild cognitive impairment according to the consensus criteria from the International Working Group39, a history of stroke or transient ischemic attack, neurologic diseases, substance abuse or dependence, and any history of brain tumors.
Assessment of coffee consumption
We evaluated the pattern and amount of coffee consumption using a study-specific interview that examined the average amount of daily coffee consumption over the past year (current ADCC, cups/d), the average amount of daily coffee consumption during their lifetime (ADCC, cups/d), and their ages at the start and end of coffee drinking (years). We calculated the duration of lifetime coffee consumption (DLCC, years) by subtracting the age at which coffee drinking started from the age at which coffee drinking ended. We estimated the amount of lifetime coffee consumption (ALCC, cup-years) by multiplying the ADCC by the DLCC (see Supplementary Table). Based on the previous literatures showing the effects of 200–250 mg caffeine (equivalent to 2 cups of coffee) on the cerebrovascular health7,8,9,10,11,12,14, we classified the participants into three groups according to their ADCC: never consumed (n = 101, 20.5%), consumed two cups per day or less (n = 306, 62.2%), and consumed over 2 cups per day (n = 85, 17.3%). We assumed that the participants did not change their coffee consumption habits during their lifetime.
Assessment of VWMH
We performed brain MRI using a 3.0 Tesla GE SIGNA Scanner (GE Healthcare; Milwaukee, WI) within three months of the clinical assessments. We obtained three-dimensional structural T1 weighted spoiled gradient echo sequences (acquisition voxel size = 1.0 × 0.5 × 0.5 mm; 1.0-mm sagittal slices thickness with no inter-slice gap; repetition time = 25.0 ms; echo time = 3.68 ms; number of excitations = 1; flip angle = 90°; field of view = 240 × 240 mm; and acquisition matrix size = 175 × 256 × 256 mm) and FLAIR sequences (acquisition voxel size = 0.5 × 0.5 × 3.0 mm; 3.0-mm axial slices thickness with no inter-slice gap; repetition time = 9,900 ms; echo time = 160 ms; inversion time = 2,500 ms; number of excitations = 1; flip angle = 90°; field of view = 240 × 240 mm; and acquisition axial plane matrix size = 256 × 256 mm). We quantified the absolute whole brain VWMH using a fully automated monospectral and intensity-based segmentation method from the FLAIR sequence, as described in a previous report40. We obtained the total intracranial volume (ICV) by summing the volumes of total grey matter, WM, and cerebrospinal fluid using the Freesurfer software (version 5.3.0; http://surfer.nmr.mgh.harvard.eu). We implemented all study procedures using custom written codes running in MATLAB R2014a (The Math Works, Inc., Natick, MA, USA) as well as functions from the Statistical Parametric Mapping software (version 8, SPM8; Wellcome Trust Centre for Neuroimaging, London; http://www.fil.ion.ucl.ac.uk/spm). All analyses were performed blind to participant details, including demographics, clinical characteristics, and coffee consumption data.
Statistical analysis
We compared continuous variables using one-way analyses of variance and categorical variables using chi-square tests between groups. Given the skewed distribution of the VWMH, we normalized the VWMH by dividing the corresponding ICV and log-transformed the values for better approximation of normality (logVWMH). In each group (all, men, and women), we performed two models (ALCC with covariates in the MODEL A, and ADCC and DLCC with covariates in the MODEL B) because ALCC is the value multiplied by ADCC and DLCC. We examined the effect of ALCC on logVWMH using multiple linear regression models adjusted for the following potential confounding factors: age, sex, years of education, BMI, hypertension, DM, CVD, ALAC, ALS, GDS score, PSQI score, and CIRS score (MODEL A). In examining the effects of ADCC and DLCC on logVWMH, we also conducted multiple linear regression analysis that computed ADCC and DLCC as independent variables, to determine which variable more strongly predicted logVWMH (MODEL B). In these analyses, we adjusted for the covariates of age, sex, years of education, BMI, hypertension, DM, CVD, ALAC, ALS, GDS score, PSQI score, and CIRS score. In the regression analyses, the ALCC, ADCC, and DLCC values were entered as continuous variables. We assessed multicollinearity using collinearity statistical tests (tolerance and variance inflation factor). We then compared logVWMH among the three groups of ADCC (never, ≤2.0 cups/d, and >2.0 cups/d) using analyses of covariance with Bonferroni post hoc comparisons. In these analyses, we adjusted for the covariates of age, sex, years of education, BMI, hypertension, DM, CVD, ALAC, ALS, GDS score, PSQI score, CIRS score, and DLCC. For all analyses, a two-sided p value less than 0.05 was considered to be statistically significant, and Bonferroni corrections were employed in multiple comparisons. We performed all statistical analyses using the Statistical Package for the Social Sciences (SPSS) for Windows (version 20.0; IBM Corporation; Armonk, NY).
Results
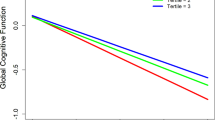
The participant characteristics are summarized in Table 1. ALCC was associated with logVWMH (adjusted R2 = 0.181, standardized β = 0.094, p = 0.030; Table 2; MODEL A). VWMH increased by 0.044 cm3 as the coffee consumption increased by one cup-year. The association between logVWMH and ADCC was significant (adjusted R2 = 0.186, standardized β = 0.126, p = 0.008) while the association between logVWMH and DLCC was not statistically significant (adjusted R2 = 0.201, standardized β = −0.003, p = 0.958 for DLCC; Table 2; MODEL B). VWMH increased by 1.251 cm3 as the average daily coffee consumption increased by one cup. When we divided the participants into three groups according to ADCC, the participants who consumed an average of more than 2 cups of coffee per day had a greater logVWMH than those who consumed an average of 2 cups of coffee per day or less as well as those who never consumed coffee (Fig. 1).

Comparisons of logVWMH between the participants grouped by ADCC for (A) All (n = 492), (B) men (n = 204), and (C) women (n = 288)*. *Analyses of covariance adjusted for age, years of education, body mass index (BMI), hypertension, diabetes mellitus (DM), cardiovascular disease (CVD), amount of lifetime alcohol consumption (ALAC), amount of lifetime smoking (ALS), Geriatric Depression Scale (GDS), Pittsburgh Sleep Quality Index (PSQI), Cumulative Illness Rating Scale (CIRS) and duration of lifetime coffee consumption (DLCC). Notes: logVWMH = log-transformed white matter hyperintensities volume/intracranial volume; ADCC = average amount of daily coffee consumption during lifetime; Low = 2 cups of coffee or less per day; High = more than 2 cups of coffee per day.
Compared to men, women showed smaller ICV (men = 1680.2 ± 128.8 cm3, women = 1472.4 ± 107.6 cm3, p < 0.001) and WM volume (men = 477.1 ± 128.6 cm3, women = 453.5 ± 185.3 cm3, p = 0.097). Compared to men, women started to consume coffee later (p = 0.001) and showed lower ALCC, ADCC and DLCC (p = 0.001). As summarized in Table 2, ALCC was associated with logVWMH in women (adjusted R2 = 0.207, standardized β = 0.112, p = 0.040; MODEL A). VWMH increased by 0.071 cm3 as the coffee consumption increased by one cup-year. Among the two determinants of ALCC, ADCC was associated with logVWMH (adjusted R2 = 0.225, standardized β = 0.209, p = 0.001) but DLCC was not (adjusted R2 = 0.225, standardized β = −0.073, p = 0.233; MODEL B). VWMH increased by 2.00 cm3 as the average daily coffee consumption increased by one cup. The women who consumed more than 2 cups of coffee per day on average showed greater logVWMH than those who consumed 2 cups of coffee per day or less as well as those who never consumed coffee (Fig. 1). ALCC was not associated with logVWMH in men (adjusted R2 = 0.224, standardized β = 0.099, p = 0.129; Table 2; MODEL A). VWMH increased by 0.032 cm3 as the coffee consumption increased by once cup-year. The associations of logVWMH with ADCC (adjusted R2 = 0.226, standardized β = 0.067, p = 0.336) and DLCC (adjusted R2 = 0.226, standardized β = 0.080, p = 0.259) were not significant (Table 2; MODEL B). The results were not changed when we analyzed the subjects who did not have a history of hypertension separately (106 men and 127 women).
Discussion
This study found that higher ALCC was associated with higher logVWMH in cognitively normal elderly individuals in both sexes. Although 3 to 4 cups of coffee per day (providing 300–400 mg/d of caffeine) are generally regarded as safe for most healthy adults6, the participants who consumed an average of more than 2 cups of coffee per day had greater logVWMH in late life than those who consumed less.
To our knowledge, this study is the first to show a positive association between ALCC and late life VWMH in cognitively normal elderly individuals. To date, there have been few studies on the effects of lifetime coffee consumption on WMH in humans, with conflicting results. Araújo et al. found no association between coffee consumption and VWMH in middle-aged adults41. Ritchie et al. reported that coffee consumption was associated with lower VWMH among women42. However, neither study considered the duration of coffee consumption or lifetime cumulative coffee consumption, and instead quantified coffee consumption through ADCC alone. Furthermore Ritchie et al. did not adjust for other potential confounding factors, such as hypertension, DM, and CVD42.
Coffee consumption may increase the risk of WMH via several mechanisms. First, caffeine, at a dose that is equivalent to 2 cups of coffee, reduces cerebral blood flow7,9,10,11,12 and abolishes the protective effect of ischemic preconditioning in humans8. Endogenous adenosine dilates cerebral vessels by activating adenosine A2A and A2B receptors of cerebrovascular smooth muscle15,43. At a normal dietary level, caffeine competitively antagonizes these adenosine receptors15, reduces adenosine-induced vasodilation up to 70%44. The majority of previous human studies have consistently found that chronic consumption of caffeinated coffee causes increased vascular resistance15, arterial stiffness16 and cerebral vasoconstriction12, which result in a decrease in cerebral blood flow due to blocking of the adenosine receptors. A study of middle-aged adults reported that increased aortic stiffness was independently associated with a greater VWMH45. Therefore, prolonged heavy consumption of caffeinated coffee may result in chronic cerebral hypoperfusion, which, in turn, may contribute to an increased VWMH in late life. Moreover, variations in the expression and/or distribution of adenosine receptor subtypes within the cerebrovascular system and other components of the neurovascular unit, such as astrocytes, which regulate the tone of cerebral arterioles46, might influence VWMH, directly or indirectly. Second, the pressor response to caffeine could partly explain the association between coffee consumption and VWMH. High blood pressure is a major independent risk factor for increased VWMH17,18,19,20,21, and population-based MRI studies have shown a linear association between systolic and diastolic blood pressure levels and severity of VWMH18,19. In considering the long-term effects of caffeinated coffee consumption on normotensive adult populations, two meta-analyses of randomized controlled trials have shown increased blood pressure: 2.4 mm Hg in systolic pressure and 1.2 mm Hg in diastolic pressure14 and 2.0 mm Hg in systolic pressure and 0.7 mm Hg in diastolic pressure13. In hypertensive individuals, those who habitually drinking ≥3 cups of coffee per day showed higher 24-h systolic and (beta: 3.25 mm Hg) diastolic pressure (beta: 2.24 mm Hg) than non-coffee drinkers47. Paraxanthine, a major metabolite of caffeine, also increases the blood pressure in humans48. A previous observational study49 and a randomized controlled trial50 both reported that improved blood pressure control delayed the progression of WMH in elderly participants. It is therefore plausible that the effect of long-term coffee consumption on blood pressure may have contributed to the observed VWMH increases, at least in part, during chronic daily lifetime exposure. However, the association of coffee drinking with the risk of hypertension was conflicting even between the previous meta-analyses; an inverted J-shape increase in one study51 while a dose-dependent decrease in other studies52,53. Furthermore, a recent study reported that several caffeine metabolites, such as methyluric acid and methylxanthine, reduced the odds for hypertension in adult individuals54. These ingredients may counterbalance caffeine’s pressor effect above a certain level of consumption13,54. Thus, further experimental studies are warranted to elucidate the mechanisms that underlie the effect of coffee consumption on the risk of WMH. Although the participants who regularly consume coffee may develop a degree of tolerance to the pressor effect of coffee, several experimental trials have confirmed that the tolerance may be partial. Caffeine can still to increase systolic and diastolic blood pressure even following regular consumption55. Furthermore, the pressor response to caffeine is regained after a relatively short period of abstinence56. Lastly, large individual variations in the sensitivity to the effects of coffee and the genetic polymorphisms associated with the enzymatic breakdown of caffeine or adenosine receptor function57 may also partly mediate the effect of coffee consumption on the VWMH increase. Although sleep apnea may also increase the risk of cerebral WMH58, neither the PSQI score nor the STOP questionnaire score was different by coffee intake in the current study. Therefore, the association between coffee and VWMH in our sample may not be confounded by comorbid sleep apnea.
When the both sexes were analyzed separately, lifetime consumption of coffee was associated with cerebral WMH in late life, in women but not in men, although the total brain and WM volumes of women are smaller than those of men. This difference may be, at least in part, attributable to the differences in hormones and/or the sensitivity to caffeine between the sexes. Sex differences in response to caffeine emerge after pubertal development, and these responses differ across the menstrual cycle in postpubertal women59. Women show more toxic reactions to caffeine than do men, suggesting that men and women metabolize caffeine differently60. In women, the increases in blood pressure after caffeine administration was greater when estradiol levels were higher, indicating that the sex differences in the caffeine response between men and women may be mediated by differences in sex hormone levels24. Estradiol decreases the rate of caffeine clearance in old women by inhibiting cytochrome P450 1A2 (CYP1A2) activity23.
Although higher cumulative coffee consumption may have a detrimental effect on late life cerebral VWMH as described above, previous cross-sectional and longitudinal studies have reported that regular coffee consumption is associated with lower risk of stroke, DM, and CVD, better cognitive performance and a reduced risk of late life cognitive impairment/decline and dementia1,2,3,4,5, although the association was not found in all cognitive domains investigated and there was a lack of distinct dose-response associations. Therefore, given the overall benefits of coffee consumption on brain health, it is recommended to have an adequate amount of coffee depending on age, sex, and health status.
This study has some limitations. First, we could not account for the other sources of caffeine, such as tea, soft drinks, energy drinks, and chocolate products. We did not examine the type and preparation method of coffee (e.g. boiled, filtered, etc.), and did not differentiate between decaffeinated and caffeinated coffee, which directly influence the amount of consumed caffeine. However, coffee has been identified as a major dietary source of caffeine6, and decaffeinated coffee is not commonly consumed in Korea61. Second, because the patterns and amounts of coffee consumption were evaluated using retrospective self-reports and were subject to measurement error, we cannot rule out the possibility of misclassification bias, which could lead to the over- or underestimation of the real amount of coffee consumed. Nevertheless, results from validation studies suggest that self-reported habitual coffee consumption can be assessed with high reproducibility and validity62. Third, although habitual patterns of drinking coffee remain relatively stable over time63, some hypertensive patients with uncontrolled blood pressure and women who are pregnant or breastfeeding are more likely to refrain from consuming coffee3,64. However, we did not obtain information regarding the changes in participants’ coffee-drinking habits in the current study. Finally, causal inferences from our results is limited due to relatively small sample size and retrospective cohort design of this study.
In conclusions, we found that an increased lifetime cumulative coffee consumption was associated with an increased VWMH in late life. People who consumed an average of more than 2 cups of coffee per day had greater VWMH than those who consume less. The coffee-associated increase in VWMH was larger in women than in men. Given that coffee is consumed worldwide and WMH are common in community-dwelling old people17,18, we should be concerned with the potential adverse effects of lifetime coffee consumption on brain health in late life.
Data availability
The datasets generated during and/or analyzed during the current study are available from the corresponding author on reasonable request. All methods were performed in accordance with the relevant guidelines and regulations.
References
Larsson, S. C., Virtamo, J. & Wolk, A. Coffee consumption and risk of stroke in women. Stroke 42, 908–912 (2011).
Van Dam, R. M. & Hu, F. B. Coffee consumption and risk of type 2 diabetes: a systematic review. JAMA 294, 97–104 (2005).
Rodríguez-Artalejo, F. & López-García, E. Coffee consumption and cardiovascular disease: A condensed review of epidemiological evidence and mechanisms. J. Agric. Food Chem. 66, 5257–5263 (2017).
Haller, S., Montandon, M.-L., Rodriguez, C., Herrmann, F. & Giannakopoulos, P. Impact of Coffee, Wine, and Chocolate Consumption on Cognitive Outcome and MRI Parameters in Old Age. Nutrients 10, 1391 (2018).
Panza, F. et al. Coffee, tea, and caffeine consumption and prevention of late-life cognitive decline and dementia: a systematic review. J. Nutr. Health Aging 19, 313–328 (2015).
Higdon, J. V. & Frei, B. Coffee and health: a review of recent human research. Crit. Rev. Food Sci. Nutr. 46, 101–123 (2006).
Nehlig, A., Daval, J.-L. & Debry, G. Caffeine and the central nervous system: mechanisms of action, biochemical, metabolic and psychostimulant effects. Brain Res. Rev. 17, 139–170 (1992).
Riksen, N. P. et al. Caffeine prevents protection in two human models of ischemic preconditioning. J. Am. Coll. Cardiol. 48, 700–707 (2006).
Cameron, O. G., Modell, J. G. & Hariharan, M. Caffeine and human cerebral blood flow: a positron emission tomography study. Life Sci. 47, 1141–1146 (1990).
Field, A. S., Laurienti, P. J., Yen, Y.-F., Burdette, J. H. & Moody, D. M. Dietary caffeine consumption and withdrawal: confounding variables in quantitative cerebral perfusion studies? Radiology 227, 129–135 (2003).
Lunt, M., Ragab, S., Birch, A., Schley, D. & Jenkinson, D. Comparison of caffeine-induced changes in cerebral blood flow and middle cerebral artery blood velocity shows that caffeine reduces middle cerebral artery diameter. Physiol. Meas. 25, 467 (2004).
Addicott, M. A. et al. The effect of daily caffeine use on cerebral blood flow: how much caffeine can we tolerate? Hum. Brain Mapp. 30, 3102–3114 (2009).
Noordzij, M. et al. Blood pressure response to chronic intake of coffee and caffeine: a meta-analysis of randomized controlled trials. J. Hypertens. 23, 921–928 (2005).
Jee, S. H., He, J., Whelton, P. K., Suh, I. & Klag, M. J. The effect of chronic coffee drinking on blood pressure: a meta-analysis of controlled clinical trials. Hypertension 33, 647–652 (1999).
Ngai, A. C., Coyne, E. F., Meno, J. R., West, G. A. & Winn, H. R. Receptor subtypes mediating adenosine-induced dilation of cerebral arterioles. Am. J. Physiol. Heart Circ. Physiol. 280, H2329–H2335 (2001).
Vlachopoulos, C., Panagiotakos, D., Ioakeimidis, N., Dima, I. & Stefanadis, C. Chronic coffee consumption has a detrimental effect on aortic stiffness and wave reflections. Am. J. Clin. Nutr. 81, 1307–1312 (2005).
Kim, K. W., MacFall, J. R. & Payne, M. E. Classification of white matter lesions on magnetic resonance imaging in elderly persons. Biol. Psychiatry 64, 273–280 (2008).
Longstreth, W. et al. Clinical correlates of white matter findings on cranial magnetic resonance imaging of 3301 elderly people: the Cardiovascular Health Study. Stroke 27, 1274–1282 (1996).
Breteler, M. et al. Cerebral white matter lesions, vascular risk factors, and cognitive function in a population‐based study The Rotterdam Study. Neurology 44, 1246–1246 (1994).
Pantoni, L. & Garcia, J. H. Pathogenesis of leukoaraiosis: a review. Stroke 28, 652–659 (1997).
de Leeuw, F. E. et al. Hypertension and cerebral white matter lesions in a prospective cohort study. Brain 125, 765–772 (2002).
Marstrand, J. et al. Cerebral perfusion and cerebrovascular reactivity are reduced in white matter hyperintensities. Stroke 33, 972–976 (2002).
Pollock, B. G. et al. Inhibition of caffeine metabolism by estrogen replacement therapy in postmenopausal women. J. Clin. Pharmacol. 39, 936–940 (1999).
Temple, J. L. & Ziegler, A. M. Gender differences in subjective and physiological responses to caffeine and the role of steroid hormones. J. Caffeine Res. 1, 41–48 (2011).
Fatemi, F. et al. Sex differences in cerebrovascular pathologies on FLAIR in cognitively unimpaired elderly. Neurology 90, e466–e473 (2018).
van Dijk, E. J. et al. Progression of cerebral small vessel disease in relation to risk factors and cognitive consequences: Rotterdam Scan study. Stroke 39, 2712–2719 (2008).
Han, J. W. et al. Overview of the Korean Longitudinal Study on Cognitive Aging and Dementia. Psychiatry Investig. 15, 767 (2018).
Lee, J. H. et al. Development of the Korean Version of the Consortium to Establish a Registry for Alzheimer’s Disease Assessment Packet (CERAD-K) clinical and neuropsychological assessment batteries. J. Gerontol. Ser. B Psychol. Sci. Soc. Sci. 57, 47–53 (2002).
Yoo, S.-W. et al. Validity of Korean version of the mini-international neuropsychiatric interview. Anxiety. Mood. 2, 50–55 (2006).
Lee, D. Y. et al. A normative study of the CERAD neuropsychological assessment battery in the Korean elderly. J. Int. Neuropsychol. Soc. 10, 72–81 (2004).
Wechsler, D. Instruction Manual for the Wechsler Memory Scale Revised. New York, NY: Psychological Corporation (1987).
Kim, T. H. et al. Korean version of frontal assessment battery: psychometric properties and normative data. Dement Geriatr. Cogn. Disord. 29, 363–370 (2010).
Kim, J. Y. et al. Standardization of the Korean version of the geriatric depression scale: reliability, validity, and factor structure. Psychiatry Investig. 5, 232–238 (2008).
Buysse, D. J., Reynolds, C. F. III, Monk, T. H., Berman, S. R. & Kupfer, D. J. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 28, 193–213 (1989).
Miller, M. D. et al. Rating chronic medical illness burden in geropsychiatric practice and research: application of the Cumulative Illness Rating Scale. Psychiatry Res. 41, 237–248 (1992).
Chung, F. et al. Stop questionnairea tool to screen patients for obstructive sleep apnea. Anesthesiology 108, 812–821 (2008).
Hughes, C. P., Berg, L., Danziger, W., Coben, L. A. & Martin, R. L. A new clinical scale for the staging of dementia. Brit. J. Psychiat. 140, 566–572 (1982).
Association, A. P. DSM-IV-TR: Diagnostic and Statistical Manual of Mental Disorders, 4th Edition, Text Revision. Vol. 75 (Washington, DC: American Psychiatric Association Press, 2000).
Winblad, B. et al. Mild cognitive impairment–beyond controversies, towards a consensus: report of the International Working Group on Mild Cognitive Impairment. J. Intern. Med. 256, 240–246 (2004).
Yoo, B. I. et al. Application of variable threshold intensity to segmentation for white matter hyperintensities in fluid attenuated inversion recovery magnetic resonance images. Neuroradiology 56, 265–281 (2014).
Araújo, L. F. et al. Association of coffee consumption with MRI markers and cognitive function: A population-based study. J. Alzheimers Dis. 53, 451–461 (2016).
Ritchie, K. et al. Caffeine, cognitive functioning, and white matter lesions in the elderly: establishing causality from epidemiological evidence. J. Alzheimers Dis. 20, S161–S166 (2010).
Phillis, J. Adenosine in the control of the cerebral circulation. Cerebrovasc. Brain Metab. Rev. 1, 26–54 (1989).
Meno, J. R. et al. Effect of caffeine on cerebral blood flow response to somatosensory stimulation. J. Cereb. Blood Flow Metab. 25, 775–784 (2005).
Poels, M. M. et al. Arterial stiffness and cerebral small vessel disease: the Rotterdam Scan Study. Stroke 43, 2637–2642 (2012).
Pelligrino, D. A., Xu, H.-L. & Vetri, F. Caffeine and the control of cerebral hemodynamics. J. Alzheimers Dis. 20, S51–S62 (2010).
Lopez-Garcia, E. et al. Habitual coffee consumption and 24-h blood pressure control in older adults with hypertension. Clin. Nutr. 35, 1457–1463 (2016).
Benowitz, N. L., Jacob, P., Mayan, H. & Denaro, C. Sympathomimetic effects of paraxanthine and caffeine in humans. Clin. Pharmacol. Ther. 58, 684–691 (1995).
Godin, O., Tzourio, C., Maillard, P., Mazoyer, B. & Dufouil, C. Antihypertensive treatment and change in blood pressure are associated with the progression of white matter lesion volumes: the Three-City (3C)–Dijon Magnetic Resonance Imaging Study. Circulation 123, 266–273 (2011).
Dufouil, C. et al. Effects of blood pressure lowering on cerebral white matter hyperintensities in patients with stroke: the PROGRESS (Perindopril Protection Against Recurrent Stroke Study) Magnetic Resonance Imaging Substudy. Circulation 112, 1644–1650 (2005).
Zhang, Z., Hu, G., Caballero, B., Appel, L. & Chen, L. Habitual coffee consumption and risk of hypertension: a systematic review and meta-analysis of prospective observational studies. Am. J. Clin. Nutr. 93, 1212–1219 (2011).
Xie, C. et al. Coffee consumption and risk of hypertension: A systematic review and dose–response meta-analysis of cohort studies. J. Hum. Hypertens. 32, 83–93 (2018).
D’Elia, L., La Fata, E., Galletti, F., Scalfi, L. & Strazzullo, P. Coffee consumption and risk of hypertension: a dose–response meta-analysis of prospective studies. Eur. J. Nutr. 58, 271–280 (2019).
Ngueta, G. Caffeine and caffeine metabolites in relation to hypertension in US adults. Eur. J. Clin. Nutr., 1 (2019).
James, J. E. Chronic effects of habitual caffeine consumption on laboratory and ambulatory blood pressure levels. J. Cardiovasc. Risk 1, 159–164 (1994).
Shi, J., Benowitz, N. L., Denaro, C. P. & Sheiner, L. B. Pharmacokinetic‐pharmacodynamic modeling of caffeine: tolerance to pressor effects. Clin. Pharmacol. Ther. 53, 6–14 (1993).
Yang, A., Palmer, A. A. & de Wit, H. Genetics of caffeine consumption and responses to caffeine. Psychopharmacology (Berl.) 211, 245–257 (2010).
Del Brutto, O. H., Mera, R. M., Zambrano, M. & Castillo, P. R. Relationship between obstructive sleep apnea and neuroimaging signatures of cerebral small vessel disease in community-dwelling older adults. The Atahualpa Project. Sleep Med. 37, 10–12 (2017).
Temple, J. L. et al. Cardiovascular responses to caffeine by gender and pubertal stage. Pediatrics 134, 112–119 (2014).
Carrillo, J. A. & Benitez, J. CYP1A2 activity, gender and smoking, as variables influencing the toxicity of caffeine. Br. J. Clin. Pharmacol. 41, 605–608 (1996).
USDA. United States Department of Agriculture (2015) USDA Foreign Agricultural Service. U.S. Embassy, Republic of Korea. Coffee market brief update. Available at: https://www.fas.usda.gov/data/south-korea-coffee-market-brief-update (accessed 11 January 2016).
Ferraroni, M. et al. Reproducibility and validity of coffee and tea consumption in Italy. Eur. J. Clin. Nutr. 58, 674 (2004).
Vercambre, M.-N., Berr, C., Ritchie, K. & Kang, J. H. Caffeine and cognitive decline in elderly women at high vascular risk. J. Alzheimers Dis. 35, 413–421 (2013).
Group, C. S. Maternal caffeine intake during pregnancy and risk of fetal growth restriction: a large prospective observational study. BMJ 337, a2332 (2008).
Acknowledgements
This study was supported by a grant from the Korean Health Technology R&D Project, Ministry of Health, Welfare, Republic of Korea (grant no. HI09C1379 [A092077]), the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2015R1D1A1A01059251), and Institute for Information & communications Technology Promotion (IITP) grant funded by the Korea government (MSIT) (2018-2-00861, Intelligent SW Technology Development for Medical Data Analysis).
Author information
Authors and Affiliations
Contributions
J.P. and K.W.K. conceived and designed the study. J.W.H., J.R.L., S.B., S.W.S., J.H.K. and K.W.K. acquired the data. J.P. and K.W.K. performed the analysis. J.P. and K.W.K. wrote the manuscript. J.W.H., J.R.L., S.B., S.W.S. and J.H.K. provided valuable advice during analysis and contributed writing the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Park, J., Han, J.W., Lee, J.R. et al. Association between lifetime coffee consumption and late life cerebral white matter hyperintensities in cognitively normal elderly individuals. Sci Rep 10, 421 (2020). https://doi.org/10.1038/s41598-019-57381-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-57381-z
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
