
Abstract
Ethnic disparity of cerebral small vessel disease (CSVD) has been reported previously but understanding of its clinical-anatomical is sparse. Two cohorts of CSVD patients from Peking University First Hospital, China and University Hospital of Ulm, Germany were retrospectively collected between 2013 and 2017. Visual rating scales and semiautomatic computer-assisted quantitative analysis were used to describe the neuroimaging features of CSVD, including lacunes, enlarged perivascular spaces, white matter changes and microbleeds. After exclusion of confounding neurological disorders, 165 out of 220 Chinese and 86 out of 98 German patients’ data were analyzed. Mean age of patients was 64.0 ± 11.9 years in China and 73.9 ± 10.3 years in Germany. Cognitive deficits were more prominent in the German group, mainly in the cognitive domains of language and delayed recall. Neuroimaging comparison showed that lacunes were more common and white matter lesion load was more severe in German than Chinese patients. Spatial distribution analysis suggested that Chinese patients showed more deep and infratentorial lesions (microbleeds and lacunes), while lesions in German patients were more frequently located in the lobes or subcortical white matter. In conclusion, different age of onset and anatomical distribution of lesions exist between Chinese and German CSVD patients in the observed population.
Similar content being viewed by others
Introduction
Cerebral small vessel disease (CSVD) is a syndrome defined by clinical presentation and neuroimaging with a heterogeneous etiology. The age and hypertension-related small vessel disease is the most common form1. From a clinical point of view, CSVD is a major cause of stroke and vascular cognitive impairment. In addition, progressive dysfunction of gait, swallowing and sphincters lead to disability and loss of autonomy1,2, and the socioeconomic impact is tremendous3. As the small vessels can currently not be visualized in vivo, the typical parenchymal lesions in neuroimaging are thought to be directly related to impairment of small cerebral vessels. As markers of small vessel disease, recent small subcortical infarct, lacune of presumed vascular origin, white matter hyperintensity of presumed vascular origin, enlarged perivascular spaces, cerebral microbleed and brain trophy4 have been adopted1,3. The pathogenesis of these changes is not well understood, but is thought to be diffuse cerebrovascular endothelial failure as a result of a combination of traditional vascular risk factors, socioeconomic risk factors, genetic susceptibility and as yet undetermined environmental factors1,3.
Ethnic disparity of CSVD has been reported previously5,6,7,8,9,10. A hospital-based study from the Netherlands showed that white stroke patients had higher odds for carotid artery stenosis while Black and Asian stroke patients more often presented with lacunar infarcts10. In the South London Ethnicity and Stroke Study, small vessel disease associated stroke and white matter hyperintensities were markedly increased in Black Africans versus White stroke patients, while Black Caribbean appeared to have an intermediate risk5. In a multiethnic stroke population from Florida, a higher proportion of lacunar stroke was found in Caribbean Blacks, African Americans, and Caribbean Hispanics, compared with non-Hispanic Whites6. The population-based Auckland Regional Community Stroke Study found Maori/Pacific and Asian/other people at higher risk of primary intracerebral hemorrhage compared to New Zealand/Europeans9. In addition, emerging evidence exists that - compared with white populations of European origin, Chinese populations have a higher proportion of stroke attributable to intracerebral hemorrhage and lacunar ischemic stroke7,8. All these studies yield similar results, showing that Black and Yellow patients share a higher susceptibility to CSVD than White patients5,7,8,9. These differences are commonly explained by a different prevalence of vascular risk factors9, yet undetermined genetic or environmental risk factors may also account for it. However, these previous studies had their focus on the prevalence of CSVD and the distribution of risk factors, while only few studies11,12 reported on differences in clinical phenotype and anatomical distribution of CSVD on brain imaging between different ethnic groups. From a pathophysiological point of view, the clinical-anatomical correlation in particular might provide a deeper insight into the mechanisms of CSVD.
Owing the support from the joint project of Peking University Health Science Center (PUHSC) and University of Ulm, we were able to acquire patients’ data from both countries and to conduct a retrospective study to explore the clinical and neuroimaging disparities of CSVD between Chinese and German patients.
Methods
Study population
Two cohorts of CSVD patients from Peking University First Hospital and University Hospital of Ulm (University and Rehabilitation Clinics Ulm, RKU), were recruited for the study. Inclusion criteria for both groups were recent lacunar stoke, transient ischemic attack (TIA), intracerebral hemorrhage (ICH) or other symptoms such as progressive gait disorder and cognitive decline due to vascular factors, with one or more characteristic imaging changes of CSVD in magnetic resonance imaging (MRI) according to current standards, including recent small subcortical infarct, lacune of presumed vascular origin, white matter hyperintensity of presumed vascular origin, enlarged perivascular space or cerebral microbleed4. The Chinese patients were recruited between 2013 and 2017 from the Dept. of Neurology wards and outpatient clinic of the Peking University First Hospital. German patients were recruited between 2015 and 2017 from the stroke unit and outpatient clinic of the university hospital of Ulm. Informed consents were obtained from all participants. This research was approved by the Ethics Committee of Peking University (IRB00001052-17018) and Ulm University (#295/17), and performed in accordance with the declaration of Helsinki. Patients with large vessel stenosis, which was defined as a stenosis more than 50% detected by carotid ultrasound/transcranial doppler sonography (TCD) or magnetic resonance angiography (MRA) in any large or medium artery supplying brain tissue, or suspicion of cerebral amyloid angiopathy (CAA) or Alzheimer disease (AD) from clinical course or imaging changes were excluded from the final analysis.
Clinical data collection
Demographic information of the patients such as age, sex, education, and body mass index (BMI) were collected. Common vascular risk factors including hypertension, diabetes mellitus, dyslipidemia, coronary heart disease, atrial fibrillation, chronic kidney disease, level of serum homocysteine (China: HLPC, Germany: Enzyme-Cycling-Assay), smoking, and family stroke history were documented on the first visit of the patient. Color Doppler carotid ultrasound, TCD and MRA were used to reveal the extra- and intracranial artery changes. 143 of the patients accepted neuropsychological assessment using the Mini-mental State Examination (MMSE). In a subgroup of patients (N = 96), the Montreal Cognitive Assessment (MoCA) was conducted additionally. These scales were assessed during the follow-up at least 2 weeks after stroke, in order to rule out the effect of acute stroke on cognitive function.
MR scanning and measuring
Each patient had undergone head MR scan, with sequences including T1-weighted, T2-weighted, fluid attenuated inversion recovery (FLAIR), diffusion weighted imaging (DWI) and T2*-weighted gradient-recalled echo (GRE). The MRI data of Beijing were acquired on two MR scanners (General Electric Medical Systems 1.5 T, Philips Medical Systems 3.0 T), with axial slices and slice thickness of 6.0 mm. The MRI data of Ulm were acquired on a 1.5 T MR scanner (Symphony, Siemens Medical), with coronal slices for FLAIR image, axial slices for others, and thickness of 5.0 mm.
Two independent specifically trained raters analyzed the MRI data. The intraclass correlation coefficient (ICC) of intrarater reliability was 0.98 [95% CI 0.95–1.00] and interrater reliability was 0.92 [95% CI 0.86–0.95]. Key neuroimaging markers including lacunes, enlarged perivascular spaces, white matter changes and microbleeds were evaluated, followed the definition of STandards for ReportIng Vascular changes on nEuroimaging (STRIVE)4. The presence, number and location of the lacunes were recorded. For lacune counting, different areas were documented in the right and left hemispheres separately, i.e., frontal, parietooccipital, temporal, corpus callosum, internal capsule, external capsule, basal ganglia, thalamus, brainstem and cerebellum. Enlarged perivascular spaces were assessed on T2-weighted image at the basal ganglia and corona radiate level. According to severity, we classified it into three types: A. none, B. visible (round/ovoid, <3 mm cavity at basal ganglia level or few linear changes at corona radiate level), and C. diffuse (honeycomb-like change at basal ganglia level or cloth-like change at corona radiate level). White matter changes (WMC) were assessed qualitatively and quantitatively. The age-related white matter changes (ARWMC) scale13 was adopted to rate the severity and distribution of the lesions. A semiautomatic analysis software14 was applied to extract and calculate the volume of white matter change. For microbleeds, we used the Microbleed Anatomical Rating Scale (MARS)15 to record information of its presence, number and distribution.
Statistical analysis
Statistical analyses were performed using the Statistical Package for Social Sciences version 24.0 (IBM SPSS Statistics, Armonk, N.Y., USA). The Shapiro-Wilk test was used to examine the distribution of data. Quantitative data are expressed as means and standard deviations (SD) or median depending on the distribution of the values. Categorical data are described as frequencies and ratios. The t-test was used for the comparison of age, and Mann-Whitney U test was used for other non-normal distribution data. We used Pearson’s chi-squared test to analyze the difference of categorical data. Regression analysis was conducted for evaluating whether there is a significant difference after correcting the effects of confounding factors such as age. P < 0.05 was considered significant.
Results
Demographic and risk factors
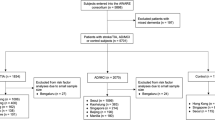
Out of a total of 318 CSVD patients, 220 patients were Chinese and 98 cases were German. Fifty-five patients from China and 3 patients from Germany were excluded for large vessel stenosis, and 9 patients from Germany were excluded for suspicion of CAA or AD. The data of 165 Chinese patients and 86 German patients were included in the final analysis. In the Chinese group, 121(73%) patients manifested with lacunar stroke or TIA, 35(21%) with ICH, and 9(6%) presented with other symptoms of CSVD. In the German group, there were 58(67%) lacunar strokes or TIAs, 11(13%) ICHs, and 17(20%) presented with other symptoms of CSVD. The average age of Chinese patients was 64.0 ± 11.9 years, while the German patients were about 10 years older at onset (73.9 ± 10.3 years), with a similar male proportion (68.5% versus 59.3%, P = 0.15).
With respect to risk factors, more Chinese patients were diagnosed with hyperlipidemia (54.8% vs. 35.9%, P = 0.007) and smoking (42.5% vs. 7.3%, P < 0.01). Defined as serum homocysteine levels above 15 umol/L, German group had a significantly higher proportion of hyperhomocysteinemia (79.7%), in contrast to the Chinese group (31.5%). In addition, the proportion of obesity (BMI ≥ 30 kg/m2) was 20.5% in German group, while the proportion in China group was only 9.8%, which also presented statistical difference (P = 0.03). The baseline characteristics and risk factors of the both groups are shown in Table 1.
Cognitive function
Sixty Chinese and 83 German patients were assessed by use of the MMSE scale, and among them, 59 Chinese and 37 German patients were also assessed with MoCA scale on the same day. The comparison showed that German patients had lower scores than Chinese patients both in MMSE [27(23, 28) vs. 28(26, 29), P < 0.01] and MoCA [21(16, 25) vs. 25(22, 27), P < 0.01]. However, these differences were not significant after adjusting for the confounding effect of age. Cognitive subdomain analysis of MoCA showed that German patients performed worse in language, delayed recall, and spatial orientation (Table 2).
Neuroimaging markers and spatial distribution of CSVD
All the patients had MR scanning, but 12 cases were excluded when evaluating the white matter changes and microbleeds due to poor image quality or lack of necessary sequence (Table 3). The German group presented more lacunes than the Chinese group in both occurrence (76.7% vs. 63.6%, P = 0.03) and number [2(1, 5) vs. 1(0, 3), P < 0.01]. There were, furthermore, significant differences in the severity of white matter changes between the two groups. The median volume of WMC in the German group was 28 ml (14.1, 47.2), nearly twice of the median volume in the Chinese group [14.1 ml (5.1, 35.9)]. Significant differences in the ARWMC scores of both groups confirmed this difference [10(6, 14) vs. 6(3, 11), P < 0.01]. These differences were still significant after adjusting for confounding effect of age. There was no difference found in the enlarged perivascular spaces and presence of microbleeds or MARS scores between the two groups.
Taking each lacune and microbleed into account, we analyzed its spatial distribution among different regions, and median ARWMC scores of different regions were calculated. It showed that most of the lacunes located in the subcortical regions (frontal area, parietooccipital area, temporal area, and corpus callosum) (47.0% in Chinese group, 62.3% in German group), but Chinese patients seemed more likely to have lacune in regions of thalamus, brainstem or cerebellum than German patients (16.1% vs. 7.0% P < 0.01) which are close to posterior circulation area. With respect to microbleeds, a similar distribution could be detected: in the Chinese group, most of the microbleeds (44.6%) were located in deep regions, while microbleeds were more often located in lobar areas in the German group (62.4%). Furthermore, the comparison of the white matter changes in all regions demonstrated that the German group had a higher mean ARWMC score than the Chinese group in the subcortical region [8(6, 10) vs. 5(3, 8.5) P < 0.01], with no differences between the two samples in the basal ganglia and infratentorial regions.
Discussion
A growing body of literature reports on ethnic disparities in stroke patients and CSVD between Western and Chinese populations7,8,16. Throughout the literature, Chinese patients are reported to have a younger age-onset of stroke and a high prevalence of CSVD. In this comparative study of CSVD between a Chinese and a German cohort, we found a younger age at onset of CSVD in Chinese patients and a different anatomical distribution of CSVD-associated lesions, including lacunes, white matter changes, and microbleeds. The observation that the German group presented with more lacunes (in deep and infratentorial regions) is not at odds with previous reports of a higher susceptibility to CSVD in Asian patients5,7,8,9, given that the current study compared CSVD patients and did not address the different etiologies in general stroke populations from the two countries. With respect to the different types of CSVD1, our study has focused on type 1 (arteriolosclerosis) and excluded other types of CSVD as far as possible in the final analysis. Further, patient groups between countries presented with significantly different cognitive profile which was attributed to differences in age.
To date, age and hypertension are the most commonly recognized risk factors of arteriosclerotic CSVD, while others such as diabetes, dyslipidemia, and smoking are still controversially discussed, possibly reflecting different underlying subtypes or pathogenesis1,17. The results of our comparison showed that there was no significant difference in the proportion of hypertension between the two groups, but a striking difference in age. According to statistics of the World Health Organization, in 2016, life expectancy in Germany was 81.0 years and 76.4 years in China18. The difference in life expectancy of about 4.6 years is less than the observed 10 years difference between the two groups in the current study, which points to an early onset of CSVD in Chinese patients. A similar age difference between other different ethnicities were observed in the Secondary Prevention of Small Subcortical Strokes (SPS3) Trial with 3,020 participants from 81 clinical sites in 8 countries which suggested a 6 year difference in the ages of CSVD onset with an average age of 58 years (SD = 9.5) for Black participants compared with 64 years for White (SD = 10.8) and Hispanics (SD = 10.7)19.
Beyond age, a marked difference between Chinese and German patients was the different spatial distribution of CSVD-associated findings. Although Chinese patients had fewer lacunes and microbleeds than German patients, Chinese patients presented with significantly more lacunes and microbleeds in deep and infratentorial regions. German patients had significantly more severe white matter changes in subcortical areas, but lacunes and microbleeds were centered preferentially in subcortical areas and lobes. The supratentorial and lobar distribution of lesions might explain poorer cognitive performance in neuropsychological tests. This result corresponds with the findings by Yakushiji and colleagues that the Eastern populations had higher odds of deep and/or infratentorial microbleeds than Western populations12. A different distribution of CSVD lesions between different ethnicities was also found in the SPS3 study11 which showed Blacks and Hispanics having more recent lacunar infarcts in the brainstem/cerebellum than non-Hispanic Whites (p < 0.001). Different risk factor profiles might be one reason for this finding. The Rotterdam Scan Study showed that total homocysteine levels were associated with silent brain infarcts and periventricular and subcortical white matter lesions20, while smoking and systolic hypertension was found to be associated with deep or infratentorial but not lobar microbleeds21. Hyperlipidemia was hypothesized as a relatively protective role in CSVD and was found to be associated with less severe WMC22. Obesity is recognized as an potential risk factor for CSVD and to be associated with incident lacunes23 and deep or infratentorial microbleeds24. In the current study, there were higher proportions of hyperlipidemia and smoking in Chinese patients but a higher rate of hyperhomocysteinemia and obesity in German patients which might correlate with the respective imaging changes at least to some extent.
Another important issue of consideration was the control of hypertension. Although the available data showed no differences in the proportion of hypertension between the two groups, literature reports suggest that there is a significant difference in hypertension control between the two countries. A population-based screening project that enrolled about 1.7 million adults in China from 2014 to 2017 showed that the age and sex standardized rates of hypertension awareness, treatment and control were 36·0% (35·8–36·2), 22·9% (22·7–23·0), and 5·7% (5·6–5·7)25, while the reported rates were 82%, 72%, and 51% in Germany 200826. Meanwhile, the level of health care varies considerably between regions in China. The reported rates of hypertension control in Beijing were 21.5% in 200727 and 31.6% in 2013–201428, respectively, which were higher than China’s average, but still significantly lower than Germany’s average. As a result, the small cerebral vessels may suffer more and earlier impairment from hypertension. In the same way, differences in the control of hypertension could in part explain differences in neuroimaging. Chinese patients had a poor hypertension control, leading to a hypertension-related brain change, which brought more ischemic or hemorrhagic damage on basal ganglia, thalamus, brainstem, or cerebellum. In contrast, German patients can be expected to have received a good hypertension control according to literature, presenting with less hypertensive-related but possible age-related brain changes, i.e., more subcortical white matter damage and cognitive impairment. In addition, it may also explain why significantly more Chinese patients had to be excluded from the final analysis due to the diagnosis of large vessel stenosis, since uncontrolled hypertension is the core risk factor of atherosclerosis in large vessels. Unfortunately, the available data did not include information on the first diagnosis and control of hypertension in our patients which prompts further research for confirming this point.
In addition, genetic differences may play an important role regarding severity and distribution of CSVD in Chinese and German patients. The APOE ε4 phenotype was reported to relate to microbleeds in a strictly lobar location21, which may be found not only in patients of Alzheimer disease29, but also patients of arteriolosclerosis CSVD simultaneously. There are numerous genes which may have an impact on CSVD by impairing the blood brain barrier. The latter was confirmed to play a major role in the formation of several CSVD-related lesions (lacunar infarction, white matter hypertension)3. Rannikmae and colleagues observed an association between common variations in the COL4A2 gene and symptomatic small vessel disease, particularly deep intracerebral hemorrhage, in the ethnic group of individuals of European ancestry30,31. In addition, dysfunction of connexins (Cx), an important component of gap junctions, can affect the permeability of blood-brain barrier in various ways32,33,34,35, resulting in WMC or microbleeds different anatomical regions. Therefore, does ethnic differences in these genotypes contribute to imaging difference of CSVD between our two countries? There is no answer yet, which requires further exploration and demonstration in future genetic and autopsy studies.
The strength of the study is that we conducted a detailed comparison of the important neuroimaging features in a well characterized clinical sample of patients with CSVD from China and Germany. As an exploratory research, it reflects the ‘real life‘ data of CSVD in the two countries to a certain extent and provides a direction of future research. The study, however, was not without limitations. First, it was a hospital-based retrospective study. Inevitably, selection bias may affect the interpretation of the results. Furthermore, data acquisition did not follow a standard operating procedure, although we applied some unified definition to ensure consistency in the processes of analysis and comparison. Finally, lack of information on social factors like income and status of health insurance might impact on health and CSVD and confound our results. A prospective study is being planned for confirming our results and assumptions.
Conclusion
In conclusion, clinical and imaging differences exist between Chinese and German CSVD patients in the observed population. Chinese patients tend to be younger and to have more lesions in deep and infratentorial structures, while German patients have more lesions in the subcortical white matter and are susceptible to cognition decline. These observed differences need to be confirmed and clarified by further prospective studies.
References
Pantoni, L. Cerebral small vessel disease: from pathogenesis and clinical characteristics to therapeutic challenges. Lancet neurology 9, 689–701, https://doi.org/10.1016/S1474-4422(10)70104-6 (2010).
The, L. S. G. et al. 2001–2011: A Decade of the LADIS (Leukoaraiosis And DISability) Study: What Have We Learned about White Matter Changes and Small-Vessel Disease? Cerebrovascular diseases 32, 577–588, https://doi.org/10.1159/000334498 (2011).
Wardlaw, J. M., Smith, C. & Dichgans, M. Mechanisms of sporadic cerebral small vessel disease: insights from neuroimaging. Lancet neurology 12, 483–497, https://doi.org/10.1016/S1474-4422(13)70060-7 (2013).
Wardlaw, J. M. et al. Neuroimaging standards for research into small vessel disease and its contribution to ageing and neurodegeneration. The Lancet Neurology 12, 822–838, https://doi.org/10.1016/s1474-4422(13)70124-8 (2013).
Gulli, G. et al. Differences in the distribution of stroke subtypes in a UK black stroke population - final results from the South London Ethnicity and Stroke Study. BMC Med 14, 77, https://doi.org/10.1186/s12916-016-0618-2 (2016).
Koch, S., Gupta, R., McClendon, M. S. & Romano, J. G. Racial-ethnic differences in lacunar infarction in a multiethnic stroke population. J Stroke Cerebrovasc Dis 22, 107–112, https://doi.org/10.1016/j.jstrokecerebrovasdis.2011.06.019 (2013).
Tsai, C. F., Anderson, N., Thomas, B. & Sudlow, C. L. Risk factors for ischemic stroke and its subtypes in Chinese vs. Caucasians: Systematic review and meta-analysis. Int J Stroke 10, 485–493, https://doi.org/10.1111/ijs.12508 (2015).
Tsai, C. F., Thomas, B. & Sudlow, C. L. Epidemiology of stroke and its subtypes in Chinese vs white populations: a systematic review. Neurology 81, 264–272, https://doi.org/10.1212/WNL.0b013e31829bfde3 (2013).
Feigin, V. et al. Ethnic disparities in incidence of stroke subtypes: Auckland Regional Community Stroke Study, 2002-2003. Lancet neurology 5, 130–139, https://doi.org/10.1016/s1474-4422(05)70325-2 (2006).
Wolma, J. et al. Ethnicity a risk factor? The relation between ethnicity and large- and small-vessel disease in White people, Black people, and Asians within a hospital-based population. European journal of neurology 16, 522–527, https://doi.org/10.1111/j.1468-1331.2009.02530.x (2009).
Benavente, O. R. et al. Clinical-MRI correlations in a multiethnic cohort with recent lacunar stroke: the SPS3 trial. Int J Stroke 9, 1057–1064, https://doi.org/10.1111/ijs.12282 (2014).
Yakushiji, Y. et al. Distribution of cerebral microbleeds in the East and West: Individual participant meta-analysis. Neurology 92, e1086–e1097, https://doi.org/10.1212/WNL.0000000000007039 (2019).
Wahlund, L. O. et al. A New Rating Scale for Age-Related White Matter Changes Applicable to MRI and CT. Stroke 32, 1318–1322, https://doi.org/10.1161/01.str.32.6.1318 (2001).
Muller, H. P., Unrath, A., Ludolph, A. C. & Kassubek, J. Preservation of diffusion tensor properties during spatial normalization by use of tensor imaging and fibre tracking on a normal brain database. Physics in medicine and biology 52, N99–109, https://doi.org/10.1088/0031-9155/52/6/n01 (2007).
Gregoire, S. M. et al. The Microbleed Anatomical Rating Scale (MARS): reliability of a tool to map brain microbleeds. Neurology 73, 1759–1766, https://doi.org/10.1212/WNL.0b013e3181c34a7d (2009).
Mok, V. et al. Race-ethnicity and cerebral small vessel disease–comparison between Chinese and White populations. Int J Stroke 9(Suppl A100), 36–42, https://doi.org/10.1111/ijs.12270 (2014).
Khan, U., Porteous, L., Hassan, A. & Markus, H. S. Risk factor profile of cerebral small vessel disease and its subtypes. J Neurol Neurosurg Psychiatry 78, 702–706, https://doi.org/10.1136/jnnp.2006.103549 (2007).
World health statistics 2018: monitoring health for the SDGs, sustainable development goals., (World Health Organization, 2018).
White, C. L. et al. Clinical features and racial/ethnic differences among the 3020 participants in the Secondary Prevention of Small Subcortical Strokes (SPS3) trial. J Stroke Cerebrovasc Dis 22, 764–774, https://doi.org/10.1016/j.jstrokecerebrovasdis.2012.03.002 (2013).
Vermeer, S. E. et al. Homocysteine, silent brain infarcts, and white matter lesions: The Rotterdam Scan Study. Annals of neurology 51, 285–289 (2002).
Poels, M. M. et al. Prevalence and risk factors of cerebral microbleeds: an update of the Rotterdam scan study. Stroke 41, S103–106, https://doi.org/10.1161/STROKEAHA.110.595181 (2010).
Jimenez-Conde, J. et al. Hyperlipidemia and reduced white matter hyperintensity volume in patients with ischemic stroke. Stroke 41, 437–442, https://doi.org/10.1161/STROKEAHA.109.563502 (2010).
Dearborn, J. L. et al. Obesity, Insulin Resistance, and Incident Small Vessel Disease on Magnetic Resonance Imaging: Atherosclerosis Risk in Communities Study. Stroke 46, 3131–3136, https://doi.org/10.1161/STROKEAHA.115.010060 (2015).
Kim, C. K. et al. Association of obesity with cerebral microbleeds in neurologically asymptomatic elderly subjects. J Neurol 259, 2599–2604, https://doi.org/10.1007/s00415-012-6546-y (2012).
Lu, J. et al. Prevalence, awareness, treatment, and control of hypertension in China: data from 1.7 million adults in a population-based screening study (China PEACE Million Persons Project). Lancet (London, England) 390, 2549–2558, https://doi.org/10.1016/s0140-6736(17)32478-9 (2017).
Neuhauser, H. K., Adler, C., Rosario, A. S., Diederichs, C. & Ellert, U. Hypertension prevalence, awareness, treatment and control in Germany 1998 and 2008–11. Journal of human hypertension 29, 247–253, https://doi.org/10.1038/jhh.2014.82 (2015).
Ma, L. et al. Epidemiological Characteristics of Hypertension in the Elderly in Beijing, China. PloS one 10, e0135480, https://doi.org/10.1371/journal.pone.0135480 (2015).
Wang, C. X. et al. Prevalence, awareness, treatment and control of hypertension in population older than 15 years of age in Beijing, 2013–2014. Zhonghua liu xing bing xue za zhi = Zhonghua liuxingbingxue zazhi 39, 179–183, https://doi.org/10.3760/cma.j.issn.0254-6450.2018.02.008 (2018).
Sadigh-Eteghad, S., Talebi, M. & Farhoudi, M. Association of apolipoprotein E epsilon 4 allele with sporadic late onset Alzheimer’s disease. A meta-analysis. Neurosciences (Riyadh, Saudi Arabia) 17, 321–326 (2012).
Rannikmae, K. et al. Common variation in COL4A1/COL4A2 is associated with sporadic cerebral small vessel disease. Neurology 84, 918–926, https://doi.org/10.1212/WNL.0000000000001309 (2015).
Rannikmäe, K. et al. COL4A2 is associated with lacunar ischemic stroke and deep ICH. Neurology 89, 1829, https://doi.org/10.1212/WNL.0000000000004560 (2017).
De Bock, M. et al. Endothelial calcium dynamics, connexin channels and blood-brain barrier function. Progress in neurobiology 108, 1–20, https://doi.org/10.1016/j.pneurobio.2013.06.001 (2013).
Nagasawa, K. et al. Possible involvement of gap junctions in the barrier function of tight junctions of brain and lung endothelial cells. Journal of cellular physiology 208, 123–132, https://doi.org/10.1002/jcp.20647 (2006).
De Bock, M. et al. A new angle on blood-CNS interfaces: a role for connexins? FEBS letters 588, 1259–1270, https://doi.org/10.1016/j.febslet.2014.02.060 (2014).
Johnson, A. M. et al. Connexin 43 gap junctions contribute to brain endothelial barrier hyperpermeability in familial cerebral cavernous malformations type III by modulating tight junction structure. FASEB journal: official publication of the Federation of American Societies for Experimental Biology 32, 2615–2629, https://doi.org/10.1096/fj.201700699R (2018).
Acknowledgements
The project was supported by ULM-PUHSC joint institute for translational and Clinical research (Grant No: PKU2017ZC001-5).
Author information
Authors and Affiliations
Contributions
J. Shu and H. Neugebaue contributed equally (shared first authors). J. Shu was involved in the data collection in Beijing, performed the imaging evaluation, statistical analysis, interpreted the results, and drafted the manuscript. H. Neugebauer was responsible for data collection in Ulm, and was involved in the imaging evaluation, results interpretation and important intellectual content. F. Li and J. Zhang participated in the data collection in Beijing. D. Lulé contributed to statistical analysis. Hans-Peter Müller contributed for guidance and advice for semiautomatic quantitative analysis of WMC. AC. Ludolph, Y. Huang, J. Kassubek and W. Zhang were involved in design of the study, supervised the data collection process, the analysis and interpretation of the data, and revised the manuscript for intellectual content. J. Kassubek and W. Zhang contributed equally to this work (shared senior authors).
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Shu, J., Neugebauer, H., Li, F. et al. Clinical and neuroimaging disparity between Chinese and German patients with cerebral small vessel disease: a comparative study. Sci Rep 9, 20015 (2019). https://doi.org/10.1038/s41598-019-55899-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-55899-w
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
