
Abstract
The study aims to identify predictors for de novo stress urinary incontinence (SUI) following Elevate mesh surgery. A total of 164 women who underwent Elevate mesh surgeries between November 2011 and February 2014 in a single center were included. Seventy-three women were excluded due to preoperative incontinence or concomitant mid-urethral sling surgery. Fourteen others were excluded due to incomplete medical records. Fisher’s exact test and χ2 test were applied. The univariate logistic regression was used for odds ratios. Of the 77 continent women, 24 (31.2%) experienced de novo SUI after the operation. Significantly more women with de novo SUI were over the age of 64 years (75.0% vs. 47.2%, p = 0.023, OR 3.36, 95% CI 1.15–9.79). Preoperative occult urodynamic stress incontinence (29.2% vs. 3.8%, p = 0.003, OR 10.0, 95% CI 2.0–50.0) and previous SUI history (41.7% vs. 7.6%, p = 0.001, OR 9.1, 95% CI 2.38–33.3) were 2 other predictors of de novo SUI postoperatively. In conclusion, age over 64 years old, occult urodynamic stress incontinence, and previous history of SUI are 3 significant predictors for de novo SUI following the single-incision mesh surgeries.
Similar content being viewed by others


Introduction
The lifetime risk of surgery for pelvic organ prolapse (POP) in the general female population was 19%1. About 40–50% of women with POP report urinary incontinence before surgeries2. In previously continent women, de novo stress urinary incontinence (SUI) may occur in approximately a quarter of those who receive pelvic reconstruction surgeries2,3,4. The incontinence symptom may be so bothersome that those women would need secondary surgeries. Studies revealed evidence that prolapse surgery combined with anti-incontinence surgery reduces the risk of postoperative SUI5,6; whereas, others warn the risk of difficulty voiding, urinary urgency or urge incontinence, urinary tract injuries and more medical costs in combined surgery3,7,8,9.
If we can selectively perform concomitant anti-incontinence surgery only for women high risk of de novo SUI, we can provide a treatment strategy with high efficacy, high satisfaction, and reasonable cost. Although the mechanism of de novo SUI is not fully understood, urethral kinking or external urethral compression may be the underlying cause10. Different surgical methods have different predictors for de novo SUI11,12, resulting in different de novo SUI rate13.
Elevate mesh is the next generation of the Perigee system, using type I polypropylene Intepro Lite mesh and single vaginal incision procedure that reaches obturator fascia and sacrospinous ligament. Lo, and his colleagues conducted a study mainly focusing on the predictors of de novo SUI after POP surgeries, including trans-obturator 4-arm mesh and native tissue12. However, there is limited data to evaluate the preoperative parameters in predicting postoperative SUI after single-incision mesh (SIM) surgery. In this study, we attempt to identify the predictive factors for de novo SUI following Elevate mesh placement.
Results
Of the 77 continent women, 24 (31.2%) experienced de novo SUI after the operation. Demographic data were obtained in the 77 women including age, parity, body mass index (BMI), menopausal status, number of them under hormone replacement therapy (HRT), smokers, underlying diseases such as hypertension and diabetes mellitus, and previously received hysterectomy, pelvic reconstruction surgeries and anti-incontinence surgeries (Table 1). Surgical procedures performed are listed in Table 2. Of the 77 women, 24 (31.2%) experienced de novo SUI after the operation, and 53 women (68.8%) were continent postoperatively during follow-up. The Elevate mesh surgeries provided successfully anatomical correction of the POP of all women, as shown in Table 3.
Comparison between the postoperative continent and incontinent women
Compared to postoperative continent women, de novo SUI were reported more commonly in women over the age of 64 years (75.0% vs. 47.2%, p = 0.023) (Table 4). Besides, women with preoperative occult urodynamic stress incontinence (29.2% vs. 3.8%, p = 0.003, OR 10.0, 95% CI 2.0–50.0) and previous history of SUI (41.7% vs. 7.6%, p = 0.001, OR 9.1, 95% CI 2.38–33.3) reported higher rate of de novo SUI postoperatively (Table 5). There was no statistical difference between the two groups in parity, BMI, HRT use, smoking status, underlying disease, surgical history, preoperative POP stage, or operative procedures. Interestingly, there was also no statistical difference between the two groups in preoperative urodynamic parameters evaluation for BOO (37.5% vs. 43.4%, p = 0.7) and maximum urethral closure pressure (MUCP) drop after POP reduction with vaginal gauze roll (33.3% vs. 30.2%, p = 0.73).
The independent predictors of postoperative de novo SUI
Univariate logistic regression was used to determine independent predictors of postoperative de novo SUI. Women older than 64 years of age were 3.36 times (95% CI 1.15–9.79) at a greater risk than younger women; while women who had occult urodynamic stress incontinence and the previous history of SUI were 10.0 times (95% CI 2.0–50.0) and 9.1 times (95% CI 2.38–33.3) at greater risks than no history women, respectively.
Discussion
This is the first study for evaluating the predictors of de novo SUI following Elevate mesh surgeries. The strongest predictors are age over 64 years old, occult urodynamic stress incontinence and previous history of SUI. The de novo SUI rate after Elevate mesh placement is 31.2%.
Among the studied cohort, over half (87 of 164, 53%) were incontinent women. After exclusion, the prolapse reduction test with vaginal gauze roll during the urodynamic study revealed occult urodynamic stress incontinence in 9 of 77 (12%) of the preoperatively continent women, which is compatible to the rate reported previously14. A study compared the detection rates of occult urodynamic stress incontinence with 5 different prolapse reduction methods, and the detection rate ranged from 6% to 30%15. But the study did not mention vaginal gauze roll, which can also be applied easily as a prolapse reduction method in daily practice16.
It was reported that approximately a quarter of continent women with POP develop de novo SUI after prolapse repair with or without mesh2,4. In our study, 31.2% of women developed de novo SUI after Elevate mesh surgeries. Previous studies revealed 26.3% (15 of 57) and 28.1% (18 of 64) de novo SUI after anterior Elevate mesh surgeries, but those studies excluded occult urodynamic stress incontinence before analysis12,17. The incidence of de novo SUI after Elevate mesh surgeries is higher than expected according to our result.
Among the 9 women with occult urodynamic stress incontinence, 7 (77.8%) developed de novo SUI. In previous articles, only 65% women with stage III to IV POP and occult urodynamic stress incontinence18 and 12.5% women with stage II POP and occult urodynamic stress incontinence19 developed de novo SUI after pelvic reconstruction surgeries without concurrent anti-incontinence surgery. The reason that the anterior Elevate mesh surgery resulted in more de novo SUI may be the extensive dissection from paravesical space to sacrospinous ligament bilaterally, which might result in more tissue damage and denervation17. Interestingly, previous literature and our study revealed that not all women having positive reduction test for occult SUI develop de novo SUI after pelvic reconstruction surgeries. In our study, 2 remained continent after the Elevate mesh surgeries. The reason may be the reduction test itself that deteriorates the urethral closure mechanism20. Therefore, further study is needed to determine the real urethral closure mechanism and evaluate occult urodynamic stress incontinence.
POP surgery can result in an improvement of SUI; meanwhile, it may unmask SUI which had been obscured by POP preoperatively2. Kuribayashi and his colleagues had found that preoperative evaluation of urethral obstruction will contribute to the prediction of de novo SUI combined with a conventional diagnosis of occult urodynamic stress incontinence11. Besides, a reduction of MUCP was also reported after transvaginal mesh surgery21. Theoretically, more women with BOO and reduction of MUCP are supposed to be found in de novo SUI group. However, neither BOO nor reduction of MUCP was found statistically different between the 2 groups in our study, indicating that unmasked BOO and reduction of MUCP cannot explain the mechanism of de novo SUI in the Elevate mesh surgeries. We found that age and previous incontinence history, either self-reported or diagnosed on examinations, are the key predictors for de novo SUI after reconstruction surgery. Firstly, age is an irreversible factor which has a negative impact on urethral closure. Secondly, once incontinence happens, no matter in daily life or in diagnostic tests, it is very likely to occur again after anatomic correction of POP.
On April 16, 2019, the FDA ordered all manufacturers to stop selling synthetic mesh intended for transvaginal repair of anterior compartment prolapse, because the manufacturers have not demonstrated a reasonable assurance of safety and effectiveness for these devices22. Although there is going to have a great change in operative methods in POP correction, we still have to look into the advantage and disadvantage of transvaginal mesh from the experience and studies before the announcement of FDA. In POP correction, Elevate mesh provides effective surgical outcome with low mesh extrusion rate23 despite a higher incidence of de novo SUI17. However, this does not mean that other single-incision meshes will result in a similar surgical outcome. Each commercial kit varies in approach methods, interaction with surrounding tissue, efficacy and adverse effect so that more studies are needed to find out.
Many studies tried to identify predictors of de novo SUI to evaluating the indications of concomitant anti-incontinence surgery. In women with POP and SUI (symptomatic or occult), concurrent MUS may reduce postoperative SUI6. Although de novo SUI is not uncommon, the symptoms might not bother some patients too much17. It might be feasible to postpone the MUS and perform a two-staged procedure if required6. Therefore, the value of de novo SUI prediction is for preoperative counseling of the indications of concomitant anti-incontinence surgery and postoperative education of the symptoms. Concurrent MUS should only be provided to high-risk women who can best benefit from reduced postoperative SUI. Therefore, whether concurrent MUS is needed should be discussed during the preoperative consultation, especially for women over 64-year-old, with a history of SUI or occult urodynamic stress incontinence, when scheduled to receive the Elevate mesh surgeries.
There is no doubt that the retrospective design of this study is a major limitation. Although the analysis was retrospective, all data were collected prospectively in a standard survey for patient care visits. The strength of our study is the simplicity and effectiveness of surgical procedures that all participants underwent the same mesh surgeries. We believe this can minimize the limitation of the study design.
Patients and Methods
Between November 2011 and February 2014, medical records of all women who received Elevate mesh procedures for their stage II to IV POP without concomitant urinary incontinence at a tertiary referral center at Taiwan were reviewed.
Approval
This study received approval from the Institutional Review Board of Kaohsiung Medical University Hospital. All basic and experimental data collection was performed in accordance with the International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction24. All procedures were performed in accordance with original advice of the Elevate Device (American Medical Systems, Minnetonka, MN).
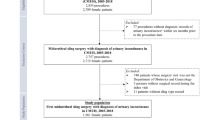
A total of 164 women were included. Fifty-five women were excluded due to concomitant MUS for preoperatively diagnosed overt or occult SUI. Eighteen women were excluded due to preoperative incontinence without MUS. Another 14 were excluded due to incomplete medical records. Thus, our study examined the de novo SUI rate based on 77 available subject files.
The review of the chart records consisted of a detailed history before and 6 months after the surgery, including urinary analysis, pelvic examination using POP-Q system24, urodynamic studies (UDS) and 1-hour pad test, and personal interview to identify urinary symptoms with the Overactive Bladder Symptom Score (OABSS)25. Urinary symptoms with the standardized questionnaire taking into account the 2002 ICS definitions26. Women were asked to fill out the VAS (visual analog scale) scores during the postoperative day 1 round. Urodynamic studies were performed according to the recommendations by the International Continence Society27 with a 6-channel urodynamic monitor (MMS; UD2000, Enschede, Netherlands). The diagnosis of occult urodynamic stress incontinence was made by the occurrence of urinary leakage in the stress test after prolapse reduction with vaginal gauze roll with the strong-desire amount of urine in the bladder. Any uninhibited detrusor contraction during filling cystometry was deemed positive for detrusor overactivity (DO). Bladder outlet obstruction (BOO) was diagnosed by pressure-flow study if the maximum flow (Qmax) was equal or less than 12 mL/s, and peak detrusor pressure at peak flow (PdetQmax) was equal or more than 20 cmH2O10,28.
Operative technique: Elevate device – anterior/apical mesh
The selection of operative methods depended on the preoperative diagnosis. All surgical procedures were performed under general anesthesia. Every patient received a single dose of intravenous prophylactic antibiotic. The patients were placed in a lithotomy position. After hydro-dissection and separation of the paravesical fascia and vaginal mucosa, the Elevate anterior mesh with bilateral upper and lower arms were pushed to the obturator fascia and sacrospinous ligaments, respectively. Graft anchorage was performed via self-fixating tips. Then, we performed a cystoscopy to check if there is any bladder or ureter injury. The synthetic mesh was put under the bladder base and anchored with 2–0 polydioxanone (PDS) sutures proximally and distally. The vaginal wound was closed with 2–0 Vicryl sutures. The skin wounds were closed using Dermabond, and vaginal packing was placed for 48 hours.
Operative technique: Elevate device – posterior mesh
After hydro-dissection, a posterior longitudinal incision was created and bilateral sacrospinous ligaments were identified. The posterior mesh implant arms with hooks were anchored in the sacrospinous ligament. Then another 2-arm synthetic mesh was pushed inside as deep as possible. Graft anchorage was performed via self-fixating tips. PDS 2–0 was sutured over cervical stroma or vaginal vault with mesh. The vaginal wound was closed with 2–0 Vicryl sutures, and vaginal packing was placed for 48 hours.
Informed consent
Informed consent was obtained from all participants before the surgeries.
Statistics
IBM SPSS Statistical Software version 20.0 ed. was used for statistical analyses. The Wilcoxon signed-rank test was performed for comparison between pre-operative and post-operative POP-Q parameters. Fisher’s exact test and χ2 test were performed for categorical variables. The Univariate logistic regression was applied for odds ratios and 95% confidence intervals. A p-value of less than 0.05 was considered statistically significant.
Conclusions
Age over 64 years old, occult urodynamic stress incontinence and previous history of SUI are 3 significant predictors for de novo SUI following the single-incision mesh surgeries. For high-risk women, whether a concurrent MUS is needed should be discussed during the preoperative consultation.
Data availability
The datasets generated during and analyzed during the current study are available from the corresponding author on reasonable request.
References
Smith, F. J., Holman, C. D., Moorin, R. E. & Tsokos, N. Lifetime risk of undergoing surgery for pelvic organ prolapse. Obstet Gynecol. 116, 1096–100 (2010).
Lensen, E. J., Withagen, M. I., Kluivers, K. B., Milani, A. L. & Vierhout, M. E. Urinary incontinence after surgery for pelvic organ prolapse. Neurourol Urodyn. 32, 455–9 (2013).
Brubaker, L. et al. Abdominal sacrocolpopexy with Burch colposuspension to reduce urinary stress incontinence. N Engl J Med. 354, 1557–66 (2006).
Wei, J. T. et al. A midurethral sling to reduce incontinence after vaginal prolapse repair. N Engl J Med. 366, 2358–67 (2012).
van der Ploeg, J. M., van der Steen, A., Zwolsman, S., van der Vaart, C. H. & Roovers, J. Prolapse surgery with or without incontinence procedure: a systematic review and meta-analysis. BJOG. 125, 289–97 (2018).
Baessler, K. et al. Surgery for women with pelvic organ prolapse with or without stress urinary incontinence. Cochrane Database Syst Rev. 8, Cd013108 (2018).
Cortesse, A., Cardot, V., Basset, V., Le Normand, L. & Donon, L. Treatment of Urinary incontinence associated with genital prolapse: Clinical practice guidelines. Prog Urol. 26(Suppl 1), S89–97 (2016).
Drain, A. et al. Use of Concomitant Stress Incontinence Surgery at Time of Pelvic Organ Prolapse Surgery Since Release of the 2011 Notification on Serious Complications Associated with Transvaginal Mesh. J Urol. 197, 1092–8 (2017).
Chermansky, C. J., Krlin, R. M. & Winters, J. C. Selective management of the urethra at time of pelvic organ prolapse repair: an assessment of postoperative incontinence and patient satisfaction. J Urol. 187, 2144–8 (2012).
Long, C. Y. et al. Urodynamic comparison of continent and incontinent women with severe uterovaginal prolapse. J Reprod Med. 49, 33–7 (2004).
Kuribayashi, M. et al. Predictor of de novo stress urinary incontinence following TVM procedure: a further analysis of preoperative voiding function. Int Urogynecol J. 24, 407–11 (2013).
Lo, T. S., Bt Karim, N., Nawawi, E. A., Wu, P. Y. & Nusee, Z. Predictors for de novo stress urinary incontinence following extensive pelvic reconstructive surgery. Int Urogynecol J. 26, 1313–9 (2015).
Maher, C. et al. Surgery for women with anterior compartment prolapse. Cochrane Database Syst Rev. 11, Cd004014 (2016).
Ker, C. R., Lin, K. L., Loo, Z. X., Juan, Y. S. & Long, C. Y. Comparison of Uphold(TM) Vaginal Mesh Procedure with Hysterectomy or Uterine Preservation for the Treatment of Pelvic Organ Prolapse. Sci Rep. 8, 9438 (2018).
Visco, A. G. et al. The role of preoperative urodynamic testing in stress-continent women undergoing sacrocolpopexy: the Colpopexy and Urinary Reduction Efforts (CARE) randomized surgical trial. Int Urogynecol J Pelvic Floor Dysfunct. 19, 607–14 (2008).
Chang, T. C., Hsiao, S. M., Chen, C. H., Wu, W. Y. & Lin, H. H. Utilizing preoperative 20-minute pad testing with vaginal gauze packing for indicating concomitant midurethral sling during cystocele repair. Eur J Obstet Gynecol Reprod Biol. 172, 127–30 (2014).
Lo, T. S. et al. Comparison between Elevate anterior/apical system and Perigee system in pelvic organ prolapse surgery: clinical and sonographic outcomes. Int Urogynecol J. 26, 391–400 (2015).
Liang, C. C., Chang, Y. L., Chang, S. D., Lo, T. S. & Soong, Y. K. Pessary test to predict postoperative urinary incontinence in women undergoing hysterectomy for prolapse. Obstet Gynecol. 104, 795–800 (2004).
de Tayrac, R., Gervaise, A., Chauveaud-Lambling, A. & Fernandez, H. Combined genital prolapse repair reinforced with a polypropylene mesh and tension-free vaginal tape in women with genital prolapse and stress urinary incontinence: a retrospective case-control study with short-term follow-up. Acta Obstet Gynecol Scand. 83, 950–4 (2004).
Khayyami, Y., Lose, G. & Klarskov, N. Prolapse reduction deteriorates the urethral closure mechanism. Int Urogynecol J. 30, 489–93 (2019).
Lo, T. S. One-year outcome of concurrent anterior and posterior transvaginal mesh surgery for treatment of advanced urogenital prolapse: case series. J Minim Invasive Gynecol. 17, 473–9 (2010).
U.S. Food and Drug Administration. Urogynecologic surgical mesh implants. Available at, https://www.fda.gov/medical-devices/implants-and-prosthetics/urogynecologic-surgical-mesh-implants (2019).
Long. C. Y. et al. Comparison of clinical outcomes using “elevate anterior” versus “Perigee” system devices for the treatment of pelvic organ prolapse. Biomed Res Int. 479610 (2015).
Haylen, B. T. et al. An International Urogynecological Association (IUGA)/International Continence Society (ICS) joint report on the terminology for female pelvic floor dysfunction. Int Urogynecol J. 21, 5–26 (2010).
Homma, Y. et al. Symptom assessment tool for overactive bladder syndrome–overactive bladder symptom score. Urology. 68, 318–23 (2006).
Abrams, P. et al. The standardisation of terminology of lower urinary tract function: report from the Standardisation Sub-committee of the International Continence Society. Neurourol Urodyn. 21, 167–78 (2002).
Abrams, P., Blaivas, J. G., Stanton, S. L. & Andersen, J. T. The standardisation of terminology of lower urinary tract function. The International Continence Society Committee on Standardisation of Terminology. Scand J Urol Nephrol Suppl. 114, 5–19 (1988).
Groutz, A., Blaivas, J. G. & Chaikin, D. C. Bladder outlet obstruction in women: definition and characteristics. Neurourol Urodyn. 19, 213–20 (2001).
Acknowledgements
We would like to thank Ministry of Health and Welfare (MOHW106-TDU-B-212-113006 and MOHW107-TDU-B-212-123006) for financially supporting the work.
Author information
Authors and Affiliations
Contributions
P.C. Wu wrote the main manuscript text. C.H. Wu, K.L. Lin, Y. Liu and Z. Loo were in charge of data collection and analysis. Lee Y.C. and C.Y. Long developed the protocol and had work in manuscript editing. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wu, PC., Wu, CH., Lin, KL. et al. Predictors for de novo stress urinary incontinence following pelvic reconstruction surgery with transvaginal single-incisional mesh. Sci Rep 9, 19166 (2019). https://doi.org/10.1038/s41598-019-55512-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-55512-0
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
