
Abstract
Epilepsy is a chronic neurological disease with a variable therapeutic response. To design effective treatment strategies for epilepsy, it is important to understand treatment responses and predictive factors. However, limited data are available in Africa, including Ethiopia. The aim of this study was therefore to assess treatment response and identify prognostic predictors among patients with epilepsy at Jimma university medical center, Ethiopia. We conducted a retrospective cohort study of 404 newly diagnosed adult epilepsy patients receiving antiepileptic treatment between May 2010 and May 2015. Demographic, clinical, and outcome data were collected for all patients with a minimum follow-up of two years. Cox proportional hazards model was used to identify predictors of poor seizure remission. Overall, 261 (64.6%) of the patients achieved seizure remission for at least one year. High number of pre-treatment seizures (adjusted hazard ratios (AHR) = 0.64, 95% CI: 0.49–0.83) and poor adherence (AHR = 0.57, 95% CI: 0.44–0.75) were significant predictors of poor seizure remission. In conclusion, our study showed that only about two-thirds of patients had achieved seizure remission. The high number of pre-treatment seizures and non-adherence to antiepileptic medications were predictors of poor seizure remission. Patients with these characteristics should be given special attention.
Similar content being viewed by others
Introduction
Epilepsy is one of the common neurological disorders of the brain. It affects more than 69 million people worldwide and about 80% of people with epilepsy are from low- and middle-income countries1,2. Epilepsy poses a substantial physical, social, and economic burden for health systems and individuals3,4. The risk of premature death due to epilepsy increases two to three times compared to the general population5. Mortality could even increase 4–7 times more in people with uncontrolled seizures and its effect is worse in developing countries6,7.
Antiepileptic drugs (AEDs) are the mainstay of epilepsy treatment and approximately 70% of patients with newly diagnosed epilepsy achieve seizure remission8,9. Although different definitions are given according to different literatures, the most commonly used definition of seizure remission is given by the International League Against Epilepsy, defined as being free from all types of seizures for at least one year8. The patient’s response requires careful diagnosis of the types of seizures, knowledge of pharmacotherapy, and patient compliance with treatment10. Although responses to the treatment of epilepsy are well studied in developed countries, limited data are available in developing countries, including Ethiopia. The effectiveness and tolerability of AEDs may vary among patients with different ethnicities11,12. This makes it difficult to extrapolate treatment response data from developed countries. Besides, the predictive factors of the response to epilepsy treatment are very variable in different populations13. Therefore, knowledge of the response to epilepsy treatment and its predictors based on regional data is crucial for developing effective treatment strategies.
Currently, a large number of people with epilepsy live in Ethiopia. It was reported that the prevalence of epilepsy in Ethiopia was 5.2 to 29.5 per 1000 populations14,15, but data on epilepsy treatment response and predictors are scarce in this population. The aim of this study was therefore to assess the response to epilepsy treatment and to identify the factors contributing to a poor seizure remission.
Methods
Study design and setting
A retrospective cohort study was conducted in patients with newly diagnosed epilepsy on follow-up at the epilepsy clinic of Jimma university medical center. Jimma university medical center is a specialized university hospital in southwest Ethiopia serving for about 15 million people living in the catchment area.
Study populations
All consecutive adult patients with newly diagnosed epilepsy who have been on regular follow up at the epilepsy clinic of Jimma university medical center from May 2010- May 2015 were recruited and followed until May 2017. The inclusion criteria were all newly diagnosed epilepsy patients, whose age was ≥18 years and patients who were treated for at least two years. Patients were excluded if they had a follow up period less than two years, transferred in from another facility like the health centers or private clinics, and those patients with incomplete medical records (i.e. patients with missing follow up data such as loss of initial chart or patient lost to follow up). Jimma University Medical Center introduced an electronic medical record of patients with epilepsy in 2010. Since then, 639 adult patients with newly diagnosed epilepsy have been registered. Of these, a total of 404 patients met the inclusion criteria and were included in the study.
Ethical approval
This study was approved by the Institutional Review Board (IRB) of the Jimma University, Institute of Health (reference number: IHRPGC/209/207) and the committee waived the need for informed consent as it was a retrospective study. The study was conducted in accordance with the Declaration of Helsinki. Written permission was obtained to access the patient’s medical records from the hospital’s medical director. The confidentiality of personal information has been strictly preserved. To ensure confidentiality, the name and other identifiers of the patients have not been registered. The data collected was stored in a locked cabinet and only the researchers had access to it.
Data collection
A data abstraction form has been developed to record relevant information from existing medical records. The data abstraction tool was prepared after reviewing similar studies13,16,17. We trained four data collectors on the purpose of the study and data collection methods, including the retrieval of data from patient records. The data collectors then reviewed the records of the eligible patients under the supervision of the research coordinator. Patient demographics (sex, age, family history of epilepsy), disease characteristics (pre-treatment number of seizures, duration of epilepsy, etiology, type of epilepsy), neurological examinations, comorbidities, AED treatments, treatment responses, adherence to treatment, and adverse effects were recorded.
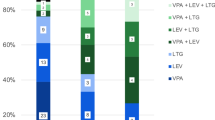
Treatment
The treatment provided in the current study was performed as part of routine care. Upon diagnosis, an appropriate AED was chosen considering seizure type, side effects, and drug interaction profiles. Monotherapy was the first antiepileptic drug used in all the patients. Initially, the minimum effective dose was prescribed and dose increases were made to control seizures or up to the maximum tolerated dose. The treatment regimens have been modified according to the patient’s response and tolerance. If the patient developed intolerable side effects with the initial drug or if the drug does not improve the seizure outcome, it was replaced with an alternative drug. However, if the initial monotherapy was tolerated and improves the seizure outcome, but did not completely provide seizure remission, a combination of drugs was prescribed. The AEDs prescribed in our study were the old AEDs (phenytoin, phenobarbital, carbamazepine, and valproate). Adherence to AEDs was checked at each visit and recorded. More than 95% of adherence to treatment is needed to prevent epileptic seizures and omitting a single dose can provoke a seizure18. Therefore, we classify the patient’s adherence based on the all-or-nothing rule. The patient was considered adherent if there was no missed dose.
Follow-up
During the first six months after starting treatment, patients were followed up at the epilepsy clinic every 2 to 4 weeks. Thereafter, patients underwent follow-up visits at least every 3 months. As our data were collected during standard medical care, patients were evaluated every 4 weeks for the first 6 months and every 3 months thereafter. At each follow-up visit, the response to AEDs treatment (i.e. the patient/ caregiver was asked to report the number of seizures between visits to the clinic), prescribed medications, adverse events, and adherence were routinely recorded. These data were extracted into a data abstraction sheet developed for this study, and the response to drug therapy was assessed at the end of the follow-up. The follow-up period was calculated from the date of the initial diagnosis to the last visit or death, whichever comes first. The final assessment of seizure control was conducted after at least two years of follow-up. For comparison purposes, we divided the patients into two groups based on achieving remission of seizures over one year. Patients who had seizure remission for at least one year were classified in the “remission” group and the remaining patients in the “non-remission” group.
Definitions
In this study, we followed the definition of epilepsy published in 2014 by the International League for Epilepsy (ILAE) ILAE19. Accordingly, epilepsy was defined by (1) at least two unprovoked seizures occurring >24 hours apart; (2) an unprovoked seizure and a likelihood of further seizures similar to the general recurrence risk after two unprovoked seizures occurring in the next 10 years; and (3) diagnosis of the epilepsy syndrome. Investigations were performed as clinically indicated, including electroencephalography and brain imaging (computed tomography and/or magnetic resonance imaging) to assist in the diagnosis, classification of epilepsy and screening for structural abnormalities. The types of epilepsy have been classified into generalized, focal and unclassified. The etiology of epilepsy was classified as genetic, structural/metabolic, unknown, according to the ILAE classification criteria for epilepsy and epileptic syndromes20.
Seizure remission was defined as an attainment of at least one-year seizure freedom. Early remission was defined as an achievement of a one-year seizure-free period started immediately or in the first 6 months. Late remission was defined as achievement of a one-year seizure-free period, starting later than 6 months after treatment initiation. After achievement of the one-year seizure-free period, a patient may become seizure free and persisting until the end follow-up visit (Sustained remission) or recurrence of seizures (relapse) may occur. Remitting-relapsing course was defined as a seizure fluctuating between periods of seizure freedom and relapse. Remission at last visit was defined as at least a 1-year seizure free period at the last follow-up visit, with or without previous relapses. A worsening course was defined as seizure continues after relapsing. No remission was defined as no seizure remission through the entire follow-up period. According to these definitions, outcome patterns of seizure remissions and relapses were reported in four main categories: Early and sustained remission, late but sustained remission, remitting-relapsing course (the patients had early or late remission but relapse occurred) and no remission.
Statistical analysis
Data were entered into EPI-Data version 4.2.0.0 and exported to SPSS (IBM SPSS Statistics for Windows, Version 21.0. Armonk, NY: IBM Corp) for analysis. We presented the data using the mean (SD) and median for continuous variables or frequency for categorical variables. A univariable Cox proportional hazards model was performed to determine the association of each independent variable with seizure remission. Subsequently, variables with a p-value < 0.25 in the univariable analysis were included in the multivariable Cox proportional hazards model to identify independent predictors of remission. A p-value of < 0.05 (α = 0.05) was used to declare a statistically significant association.
Results
Demographic and clinical characteristics of patients
We identified 639 patients with newly diagnosed epilepsy during the study period. Of these, 404 patients met our inclusion criteria and were included in the final analysis (Fig. 1).

Flow diagram of patients included in the study.
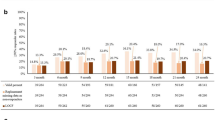
Of the patients included, 60.1% were male. The mean age at onset of seizure was 27.4 years (Standard deviation (SD) = 11.2). A family history of epilepsy was present in 9.9% of cases. Generalized epilepsy was the predominant type of epilepsy, accounting for 78.7% of cases. More than half (63.86%) of the patients had more than five episodes of seizures at the time of diagnosis. The cause of epilepsy was genetic in 9.9% of patients, structural/metabolic in 32.7% of patients and unknown in 57.4% of patients. Comorbid disease (including depression, anxiety, bipolar disorder, psychosis, human immunodeficiency virus, dyspepsia, asthma) was present in 13.4% of patients. Status epilepticus occurred in 4.7% of patients. More than sixty percent of the patients adhered to the treatment of epilepsy. The median duration of the follow-up was 44.0 months (3.6 years) (range 2–7 years) (Table 1).
Prognostic patterns of patients with newly diagnosed epilepsy
Overall, 261 (64.6%) of the patients achieved remission of seizures for at least one year.
The remaining 143 patients (35.4%) never experienced remission while continuing treatment.
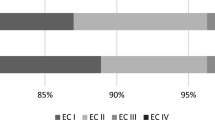
As shown in Fig. 2 an analysis was made to look for the epilepsy prognostic patterns. These prognostic patterns were categorized into four different patterns: Early and sustained remission (pattern I), late but sustained remission (pattern II), remitting-relapsing course (pattern III) and no remission (pattern IV). Early and sustained remission was observed in 17.6% and late but sustained remission in 9.4% of patients. Remitting-relapsing course was observed in 37.6% of patients. A total of 35.4% of patients never achieved seizure remission for one full year during follow-up and were categorised in the no-remission pattern (Fig. 2).

Prognostic patterns of patients with newly diagnosed epilepsy.
Analysis of predictors of poor seizure remission
A univariable Cox proportional hazards analysis was performed to determine the association of independent variables with the seizure remission and demonstrated that the number of seizures prior to AED treatment (crude hazard ratios CHR) = 0.57, 95% CI: 0.44–0.72), adherence to AEDs (CHR = 0.53, 95% CI: 0.41–0.69), and the presence of adverse event (CHR = 0.67, 95% CI: 0.52–0.86) were significantly associated with poor seizure remission (Supplementary Table S1). However, in the multivariable Cox proportional hazards model, only the number of pretreatment seizures and poor adherence to AED therapy were associated with poor seizure remission. Patients with a higher pretreatment seizures had a 36% reduced chance of achieving seizure remission (AHR = 0.64, 95% CI: 0.49–0.83), and patients with a poor treatment adherence were 43% less likely to achieve seizure remission (adjusted hazard ratios (AHR) = 0.57, 95% CI: 0.44–0.75) (Table 2).
Discussion
To our knowledge, this is the largest study conducted in Ethiopia on a cohort of patients of reasonable sample size and over a longer follow-up period, dealing with epilepsy response and predictors of poor seizure remission. Generalized epilepsy was the predominant type of epilepsy, accounting for 78.7% of cases. This is inconsistent with most epidemiological studies conducted in China21, Egypt (47.6%)16, Italy (34.8%)22 and Istanbul (47.0%)23. Similar high rates were observed, however, in Ethiopia (Amhara region) (72.91%)24, Ethiopia (Tigray region) (84.4%)25, Senegal (78%)26, and South Africa (96%)27. Factors including the etiological differences and ethnic difference might contribute for this discrepancy. Furthermore, the reason for this high proportion of generalized epilepsy in developing countries, particularly in Africa, might be influenced by the poor availability of medically sophisticated diagnostic tests, the level of training of the neurologists in the interpretation of EEG and, therefore, misclassification could also be expected28.
We observed that only 261 patients (64.6%) had seizure remission, similar to the rate observed in a large cohort of Scottish patients29 (63.7%) and suggest that a significant proportion of patients had not achieved remission. However, this result was lower than that of a study conducted in China (80%)21. Similarly, a slightly higher remission rate (69.1%) was reported by Shen et al.9. In contrast to these findings, only 45% of patients living in rural areas of China had a remission of seizures for at least one year17. A possible explanation for the discrepancy of these studies could be differences in methodology, such as the definitions used for remission and duration of follow-up, type of medications used, exclusion of non-adherent patients in some studies and the possibility of genetic influence.
According to seizure remission patterns, 46% of our patients entered early remission and about 18% entered late remission. This result is consistent with the results of Shen et al., who reported early remission in 51.6% of patients and delayed remission in 17.5% of patients9. Another study in Italy also found that 56.2% of patients had early remission30. More than one-third of our patients never went into remission during the follow-up period. Similarly, a significant proportion of patients had not experienced remission in earlier studies conducted in China (31%)9 and Scotland (25%)13. We found that remitting-relapsing course was the most common (37.6%) prognostic pattern in line with an Italian study31. This indicates that achieving a seizure remission at any time after the start of treatment does not exclude further relapses and adequate follow-up is important for all patients, including patients in remission.
Another aim of the study was to identify the predictor of poor seizure remission in patients with epilepsy. We demonstrated that patients with a high number of pre-treatment seizures were associated with poor treatment seizure remission. In line with current findings, previous studies have shown that a higher number of seizures prior to treatment was associated with lower chances of remission30,31,32,33,34,35. The role of the number of seizures prior to treatment is based on the theory that prolonged and recurrent seizures may contribute to neuronal damage and the development of new epileptic foci36. In addition, a high number of pre-treatment seizures may correlate with the intrinsic severity of the disease which is more likely to give a poor response to drug therapy37. This indicates that a seizure must be recognized soon and appropriate treatment is required to prevent injury, premature death, cognitive impairment, and psychosocial stigma34,35. The patient’s poor adherence to antiepileptic therapy was also a significant predictor of poor remission. This finding is consistent with other similar studies and suggests that lack of adherence is an important cause of uncontrolled seizures38,39.
The findings of our study have some important implications for clinical practice. Our study found that a high number of pre-treatment seizures was a predictor of poor seizure remission. The high number of seizures before treatment could be due to different factors related to the patient.
According to an earlier study in Ethiopia, the initial choice of the place of epilepsy treatment for the majority (60%) of the patients was traditional and religious healers rather than modern therapies40. Health care-seeking behavior was also poor and the majority (87%) of patients had not been treated with AEDs in a community-based study15. Another study on stigma related to epilepsy revealed that the majority of participants did not want to disclose their disease to the community41. All these factors could contribute to poor treatment seeking behaviors until several seizures occur. In the current study, we found that a high number of pretreatment seizures were significantly associated with poor remission. However, the pretreatment duration of epilepsy was not significantly associated with poor seizure remission. This suggests a high number of pretreatment seizure in a short or long period of time is the most important factor rather than the longer pre-treatment duration of seizures. Therefore, activities such as awareness-raising campaigns and the dissemination of information through the media could help patients seek treatment of epilepsy before subsequent several seizures occur. Non-adherent patients also had a high risk of poor remission. Therefore, all health care providers must provide health education to prevent nonadherence.
Finally, some important limitations must be taken into account in our study. Due to the retrospective nature of the study, the data extracted from the secondary source were prone to the absence of important characteristics such as family history. However, attempts have been made to exhaustively search for variables throughout the record, from the initial visit to the end of the follow-up. The other limitation of this study was the inclusion of non-adherent patients that could reduce the remission rate. However, excluding these patients may result in an unpowered sample, since a large number of patients were not adherent. In addition, the inclusion of these patients will help to mimic the real-world experiences of our patients. Due to these limitations, our results should be interpreted with caution and further prospective studies are suggested.
Conclusion
Our study showed that only about two-thirds of patients had achieved seizure remission during follow-up. In addition, patients in remission had a high risk of relapse, which made the remitting-relapsing course the most common outcome pattern. The high number of pre-treatment seizures and nonadherence with AEDs were independent predictors of poor remission of seizures. Patients with these characteristics should be given special attention.
Data availability
The dataset analyzed during the current study is available from the corresponding author upon reasonable request.
Change history
07 February 2020
An amendment to this paper has been published and can be accessed via a link at the top of the paper.
References
Wagner, R. G. et al. Incidence, remission and mortality of convulsive epilepsy in rural northeast South Africa. PloS one 10, e0129097 (2015).
WHO. Atlas: Epilepsy Care in the World. Geneva: World Health Organization; (2005).
Paul, A. et al. An estimate of the prevalence of epilepsy in Sub–Saharan Africa: a systematic analysis. Journal of global health 2 (2012).
Allers, K. et al. The economic impact of epilepsy: a systematic review. BMC Neurol 15, 245, https://doi.org/10.1186/s12883-015-0494-y (2015).
Neligan, A. et al. The long-term risk of premature mortality in people with epilepsy. Brain 134, 388–395 (2011).
Sperling, M. R. The consequences of uncontrolled epilepsy. CNS Spectr 9, 98–101 (2004).
Bruno, E. Results of an Action-Research on Epilepsy in Rural Mali. 7, https://doi.org/10.1371/journal.pone.0044469 (2012).
Kwan, P. et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia 51, 1069–1077 (2010).
Shen, C. et al. Factors predictive of late remission in a cohort of Chinese patients with newly diagnosed epilepsy. Seizure 37, 20–24 (2016).
Krumholz, A. et al. Evidence-based guideline: Management of an unprovoked first seizure in adults Report of the Guideline Development Subcommittee of the American Academy of Neurology and the American Epilepsy Society. Neurology 84, 1705–1713 (2015).
Roses, A. D. Pharmacogenetics and future drug development and delivery. The Lancet 355, 1358–1361 (2000).
Löscher, W., Klotz, U., Zimprich, F. & Schmidt, D. The clinical impact of pharmacogenetics on the treatment of epilepsy. Epilepsia 50, 1–23 (2009).
Brodie, M., Barry, S., Bamagous, G., Norrie, J. & Kwan, P. Patterns of treatment response in newly diagnosed epilepsy. Neurology 78, 1548–1554 (2012).
Almu, S., Tadesse, Z., Cooper, P. & Hackett, R. The prevalence of epilepsy in the Zay Society, Ethiopia–an area of high prevalence. Seizure 15, 211–213 (2006).
Tekle-Haimanot, R., Forsgren, L. & Ekstedt, J. Incidence of epilepsy in rural central Ethiopia. Epilepsia 38, 541–546 (1997).
Ashmawi, A., Hosny, H., Abdelalim, A., Bianchi, E. & Beghi, E. The long-term prognosis of newly diagnosed epilepsy in Egypt: A retrospective cohort study from an epilepsy center in Greater Cairo. Seizure 41, 86–95 (2016).
Kwan, P. et al. Long‐term outcome of phenobarbital treatment for epilepsy in rural China: A prospective cohort study. Epilepsia 54, 537–542 (2013).
Johnbull, O. S., Farounbi, B., Adeleye, A. O., Ogunrin, O. & Uche, A. P. Evaluation of factors influencing medication adherence in patients with epilepsy in rural communities of Kaduna State, Nigeria. Neuroscience and Medicine 2, 299 (2011).
Fisher, R. S. et al. ILAE official report: a practical clinical definition of epilepsy. Epilepsia 55, 475–482 (2014).
Berg, A. T. et al. Revised terminology and concepts for organization of seizures and epilepsies: report of the ILAE Commission on Classification and Terminology, 2005–2009. Epilepsia 51, 676–685 (2010).
Zhang, Y., Yu, N., Su, L. & Di, Q. A prospective cohort study of prognosis for newly diagnosed epilepsy in east China. BMC Neurology 13, 116 (2013).
Giussani, G. et al. Long-term prognosis of epilepsy, prognostic patterns and drug resistance: a population-based study. European journal of neurology 23, 1218–1227, https://doi.org/10.1111/ene.13005 (2016).
Onal, A. E. et al. Epilepsy prevalence in a rural area in Istanbul. Seizure 11, 397–401 (2002).
Birru, E. M., Shafi, M. & Geta, M. Drug therapy of epileptic seizures among adult epileptic outpatients of University of Gondar Referral and Teaching Hospital, Gondar, North West Ethiopia. Neuropsychiatr Dis Treat 12, 3213–3219 (2016).
Niriayo, Y. L. et al. Treatment outcome and associated factors among patients with epilepsy. Sci Rep 8, 17354–17354, https://doi.org/10.1038/s41598-018-35906-2 (2018).
Ndoye, N. F. et al. Prevalence of epilepsy its treatment gap and knowledge, attitude and practice of its population in sub-urban Senegal an ILAE/IBE/WHO study. Seizure 14, 106–111, https://doi.org/10.1016/j.seizure.2004.11.003 (2005).
Christianson, A. L. et al. Epilepsy in rural South African children–prevalence, associated disability and management. South African medical journal = Suid-Afrikaanse tydskrif vir geneeskunde 90, 262–266 (2000).
Banerjee, P. N., Filippi, D. & Allen Hauser, W. The descriptive epidemiology of epilepsy-a review. Epilepsy research 85, 31–45, https://doi.org/10.1016/j.eplepsyres.2009.03.003 (2009).
Chen, Z., Brodie, M. J., Liew, D. & Kwan, P. Treatment Outcomes in Patients With Newly Diagnosed Epilepsy Treated With Established and New Antiepileptic Drugs: A 30-Year Longitudinal Cohort Study. JAMA Neurol 75, 279–286, https://doi.org/10.1001/jamaneurol.2017.3949 (2018).
Del Felice, A. et al. Early versus late remission in a cohort of patients with newly diagnosed epilepsy. Epilepsia 51, 37–42 (2010).
Beghi, E. et al. Prognostic patterns and predictors in epilepsy: a multicentre study (PRO-LONG). Journal of neurology, neurosurgery, and psychiatry, https://doi.org/10.1136/jnnp-2019-320883 (2019).
MacDonald, B. et al. Factors predicting prognosis of epilepsy after presentation with seizures. Annals of neurology 48, 833–841 (2000).
Kurita, T., Sakurai, K., Takeda, Y., Horinouchi, T. & Kusumi, I. Very long-term outcome of non-surgically treated patients with temporal lobe epilepsy with hippocampal sclerosis: a retrospective study. PloS one 11, e0159464 (2016).
Kwan, P. & Brodie, M. J. Early Identification of Refractory Epilepsy. New England Journal of Medicine 342, 314–319, https://doi.org/10.1056/NEJM200002033420503 (2000).
Gilad, R., Lampl, Y., Gabbay, V., Eshel, Y. & Pinhas, I. S. Early treatment of a single generalized tonic clonic seizure to prevent recurrence. Arch Neurol 53, 1149–52 (1996).
Holmes, G. L. Epilepsy in the developing brain: lessons from the laboratory and clinic. Epilepsia 38, 12–30 (1997).
Rogawski, M. A. & Johnson, M. R. Intrinsic severity as a determinant of antiepileptic drug refractoriness. Epilepsy currents 8, 127–130, https://doi.org/10.1111/j.1535-7511.2008.00272.x (2008).
Hovinga, C. A. et al. Association of non-adherence to antiepileptic drugs and seizures, quality of life, and productivity: Survey of patients with epilepsy and physicians. Epilepsy & Behavior 13, 316–322, https://doi.org/10.1016/j.yebeh.2008.03.009 (2008).
Gabr, W. M. & Shams, M. E. Adherence to medication among outpatient adolescents with epilepsy. Saudi Pharmaceutical Journal 23, 33–40 (2015).
Bifftu, B. B., Dachew, B. A., Tiruneh, B. T. & Alemu, W. G. First choice of treatment place in the pathways to epileptic care at the outpatient department of University of Gondar Hospital, Northwest Ethiopia: Cross-sectional institutional based study. PLoS One 12, e0181310, https://doi.org/10.1371/journal.pone.0181310 (2017).
Fanta, T., Azale, T., Assefa, D. & Getachew, M. Prevalence and Factors Associated with Perceived Stigma among Patients with Epilepsy in Ethiopia. Psychiatry J 2015, 627345, https://doi.org/10.1155/2015/627345 (2015).
Acknowledgements
We would like to acknowledge Jimma University medical center staff for their cooperation in conducting our study. We are also grateful for the data collectors who were involved in data collection. This study was funded by Jima University. The funder had no role in the study design, data collection, analysis and decision to publish.
Author information
Authors and Affiliations
Contributions
K.G designed the study, analyzed the data, interpreted the results and drafted the first version of the manuscript. F.B and L.C assisted design the study, analyze and interpret the data, and supervised the study. T.G participated in the interpretation of the data and revised the manuscript critically. All authors reviewed and approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gidey, K., Chelkeba, L., Gemechu, T.D. et al. Treatment response and predictors in patients with newly diagnosed epilepsy in Ethiopia: a retrospective cohort study. Sci Rep 9, 16254 (2019). https://doi.org/10.1038/s41598-019-52574-y
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-52574-y
This article is cited by
-
Prevalence and risk factors associated with drug-resistant epilepsy in adult epileptic patients
The Egyptian Journal of Neurology, Psychiatry and Neurosurgery (2023)
-
Treatment Outcomes of Newly Diagnosed Epilepsy: A Systematic Review and Meta-analysis
CNS Drugs (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
