
Abstract
Thorough anatomic knowledge of the hyoid-larynx complex is necessary for forensic radiologists and ear-nose-throat surgeons, given the many anatomic variations that originate in embryology. In forensics the anomalies must be distinguished from fractures because the latter are indicative of violence on the neck. In this manuscript we describe the anatomical variations that can be found in the hyoid-larynx complex and explain their etiology. 284 radiological scans of excised hyoid-larynx complexes were examined with X-ray and CT. Some rare cases from literature and historical collections were added. Two third of the examined hyoid-larynx complexes deviated from the anatomical standard and showed uni- or bilateral ankylosis in the hyoid bone and/or so-called triticeal cartilages. In one fifth of the cases we found striking anatomical variants, mostly derived from the cartilage of the second pharyngeal arch. Anatomical variations of the hyoid-larynx complex can be explained by embryological development. The aberrant hyoid apparatus and the elongated styloid processes (Eagle syndrome) should be considered as one clinical entity with two different expressions as both anomalies are derived from the cartilage of the second pharyngeal arch. Several variants can mimic fractures in this region, so our study is important for radiologists and forensic experts assessing cases of possible violence on the neck.
Similar content being viewed by others

Introduction
Anatomical variations of the hyoid-larynx complex occur in 4–30% of the general population1,2,3,4. Anomalies of this complex are of great importance for radiological examination and surgery of the neck region1,5. The significance of anomalies has also been well recognized in forensic sciences, as fractures in this complex are important indicators for strangulation and blunt or penetrating trauma on the neck5,6,7,8.
The aim of this study was to provide an overview of variations in the hyoid-larynx complex and explain their etiology based on its development. Our data will be discussed in the light of the currently available literature concerning clinical and forensic relevance, providing an overview of this highly polymorphic complex, from development to death.
Anatomical Variants
Normal anatomy
The normal adult hyoid-larynx complex (Fig. 1a) is described as combination of hyoid apparatus (i.e. styloid processes, stylohyoid ligaments and lesser horns of the hyoid), body and greater horns of the hyoid bone, uncalcified thyroid-, cricoid- and arytenoid cartilages and their ligaments proper. The thyroid cartilage encompasses its superior and inferior horns. No additional cartilaginous structures are present in the trajectories of the stylohyoid ligaments, median thyrohyoid ligament and lateral thyrohyoid ligaments and no ankylosis of the joints between hyoid body and greater and/or lesser horns has occurred. Normal length of the styloid process is generally described as 20–30 mm1,2,9,10,11.

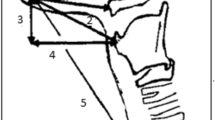
Overview of the normal adult human anatomy of the neck region (a). Lateral view of a schematic representation of the normal anatomy of the adult neck region. (b) Ventral view of the hyoid bone, thyroid and cricoid region with emphasis on the anatomical structures mentioned in this paper. Note that the arytenoid cartilages (dashed lines) lie in fact dorsally of the thyroid cartilage.
Minor variations
Minor variations in hyoid-larynx comprise age-related fusion of the body with greater and/or lesser horns by ankyloses of the joints (Fig. 2a2–6), age-related calcification of the thyroid and presence of a triticeal cartilage in the lateral thyrohyoid ligament (Fig. 2d2)12,13,14,15,16. Morphological variations of the hyoid are closely related to sex5,7,17,18, race5,6,17, body proportions7,19 and age5,7,13,14,18,20,21,22,23,24. European hyoids are broader and shorter than African ones17. Distal ends of the greater horns are significantly longer in women than in men5,18,25, whereas male hyoids are generally larger than female ones18,26,27,28. Inward curving and flattening of the greater horns are typical for the male hyoids7. Furthermore, male hyoids are more susceptible to age modifications7. Besides that, males show a higher degree of thyroid ossification, ultimately leading to the completely ossified os thyroideum12,29. Finally, hyoid muscle attachment sites also show some individual variation. These minor variations occur so often that they cannot be considered as anatomical variants14.

Anatomical variations of the hyoid-larynx complex First vertical column: normal anatomy. The hyoid bone: purple, second pharyngeal arch cartilage derivatives: blue, third pharyngeal arch cartilage derivatives: yellow, thyroid and thyrohyoid ligaments: red. Cr: cranial, Ca: caudal, L: Lateral, V: ventral, D: dorsal. Arrows indicate variation locations. A-row: normal anatomy of the hyoid bone (a1) and various degrees of ankylosis in ventral view (a2–a6). (a7) Examples of hyoid bone body exostoses; median process and split median process12. B-row: anatomical variations of the greater horn, lateral view. (b1) normal anatomy, (b2) Hypoplastic, (b3) Intermittent, note ankylosis between body and greater horn, (b4) Exostosis, (b5) Curving upward, (b6) Curving downward, (b7) Accessory bone. C-row: anatomical variations of the lesser horn, ventral view. (c1) Normal anatomy, (c2) Unilateral absence, (c3) Bilateral absence, (c4) Hypoplastic, (c5) Unilateral hyperplastic, (c6) Bilateral hyperplastic, (c7) Asymmetrical hyperplastic. (d2–6) show the anatomical variations of the thyrohyoid membrane and body of the hyoid bone, lateral view. (d1) Normal anatomy, (d2) Triticeal cartilage, (d3) Non fusion of the superior horn of the thyroid to the thyroid cartilage, this could easily be mistaken for a fracture. (d4) Unilateral hypoplastic superior horn of the thyroid cartilage. (d5) Uni- or bilateral (P van Driessche, personal communication) absence of the superior horn of the thyroid cartilage. (d6) Articulating connection between greater horn and superior horn of the thyroid cartilage. (d7) The same as in (D6) but with a triticeal cartilage interposed between the two horns. (d8) Rare case with a nearly circumferential ankylosed hyoid bone (caudal view)68. E-row: lateral view on variations of stylohyoid complex and stylohyoid ligament36. (e1) Normal anatomy, (e2) Elongation of the styloid process (SP); Eagle’s syndrome. (e3) A keratohyal (KH) bone in the stylohyoid ligament. (e4) Fundamental type with three bones (stylohyal (SH), keratohyal (KH) and hypohyal (HH)). (e5) Major type A (stylohyal, keratohyal, keratohyal and hypohyal). (e6) Major type B (stylohyal, keratohyal, keratohyal, hypohyal and hypohyal). (e7) Restricted type with a fused keratohyal and hypohyal bone, the so called keratohypohyal (KHH) bone.
Age-related ankylosis
Recently, hyoid bone density and ankyloses of the joints between hyoid body and greater and/or lesser horns are getting more attention as possible predictor for age and sex in victim identification3,30. Age-related ankylosis (Fig. 2a2–6) is a physiological process that increases with age5,13,14,18,20,21,22,23,24. D’Souza reported a mean age of unilateral (Fig. 2a4–5) and bilateral (Fig. 2a2–3) fusion in males of 39.9 and 41.77 years respectively and in females of 37.5 and 45 years20. Body and greater horns usually do not fuse until the 35th to 45th year23,31 and they might even never fuse22,23. Fusion was not reported before the age of 1832 or 2020,30. Non-fusion (Fig. 2a1) or unilateral fusion (Fig. 2a4–5) has been found in people after the age of 60, which makes this process highly polymorphic18,20. Miller et al. suggested that fusion is not a continuous ageing process, but that genetic predisposition is the driving force behind this process18. Furthermore, sex seems to be of no importance to the fusion process18,20. Therefore fusion of the hyoid body with the greater horns cannot be used as an indicator for age or sex20.
Pharyngeal Arch Cartilage Anomalies
Significant anatomical variants are due to the persistence of embryological cartilage33. One example is the complete ossification of the lateral thyrohyoid ligament between greater horns of the hyoid bone and superior horns of the thyroid cartilage, called the congenital hyothyroid bar (Fig. 2d6–7)23,33. Other cases comprise anomalies of the second pharyngeal arch cartilage, such as stylohyoid syndrome (Eagle’s syndrome)(Fig. 2e2) and the aberrant hyoid apparatus (Fig. 2e3–7). The exact incidence of anatomical changes in the stylohyoid chain is difficult to determine, since Eagle’s syndrome and the aberrant hyoid apparatus are often intermingled in literature1. It seems to vary from 4% or 5%1,2,4 to 28% or 30%2,34. Less than 10% of the patients in this group displays clinical symptoms1,2,4,35.
Aberrant hyoid apparatus
Dwight stated in 1907 that Marchetti of Padua’s report from 1652 was the earliest reference to the aberrant hyoid apparatus33, also known as (incompletely or completely) ossified hyoid apparatus23,36,37. Reichert noted the anatomical connection between styloid process and hyoid in 1837, and assigned its origin to the second pharyngeal arch cartilage38. The hyoid apparatus consists of styloid process, stylohyoid ligament and lesser horn of the hyoid1,11,23,37. This chain is completely derived from the second pharyngeal arch cartilage (Reichert’s) and can be subdivided into five, or even seven11, osteocartilaginous elements from the base of the skull to the hyoid (Table 1)1,4,10,11,33,37,39,40,41,42. In 1923 Olivier designated the (partly) ossified hyoid apparatus into three main types, depending on the number of bones in the trajectory of the hyoid apparatus (Table 1)36.
Partial ossification of the hyoid apparatus is not uncommon but the appearance of a complete bony chain is rare in humans37. This condition is usually bilateral where both sides can differ in symmetry33, but it also occurs unilaterally23,33,37. This chain passes between internal and external carotid arteries33. There is usually some movement possible by a joint or a ligamentous connection between different parts of the chain or at least between the ossified chain and hyoid body33.
The aberant hyoid apparatus is hypothesized to originate from persisting second pharyngeal arch cartilage that continued to grow and gradually ossified into a bony chain11,33. The joints in the chain often show some degree of bone clubbing, which implies a continuation of growth33.
Symptoms include difficulty in swallowing33 and restriction of neck movement36, but they rarely occur before the age of 40 because of the age dependent ossification of the cartilaginous bar37. However, striking examples have also been seen in children23. Associated compressive pathologies1, like glossopharyngeal neuralgia43 or referred pain due to irritation of the sensory nerve branches44 have been noted. Also, arterial anomalies in the affected region are not uncommon37.
Eagle’s syndrome
The stylohyoid syndrome, or Eagle’s syndrome (Fig. 2e2), describes a collection of clinical symptoms related to anomalies in size and location of the styloid process, which disturbs surrounding anatomical structures1,2,4,9,10,23,34,41,45,46,47. This condition may be uni- or bilateral and varies in severity9,10. The styloid process consists of the tympanohyal and stylohyal part (Table 1)10,33. This cylindrical, needle shaped bone, with a cartilaginous tip that normally lies between the internal and external carotid artery, projects ventrocaudally from the inferior side of the petrous bone1,9,10. It provides an anchorage for the stylopharyngeus, stylohyoid and styloglossus muscles1. During normal development, the cranial part of the second pharyngeal arch cartilage ossifies and forms the styloid process, which is connected to the lesser horn of the hyoid through the stylohyoid ligament38. There is no agreement on normal length of the styloid process34. It is described as 20–30 mm1,2,9,10,11,46, 30–35 mm34 or even 45 mm48. The length might be age dependent since an elongated process is more often observed in patients of 30 years and older1,2,9, though it has recently also been described in a 9-year-old boy49.
The otolaryngologist Watt Eagle described two clinical presentations of stylohyoid syndrome9,10,46,47. First the more common classic type, which is characterized by foreign body sensation in the throat2,9,34,41,46 and dysphagia2,34,41. The recurrent dull and not sharply localized facial and cervical pain2,4,9,23,34,45,46, radiates towards temporo-mandibular joint34,47, mandible34, maxillar or mandibular teeth34, ear1,2,23,34,46, mastoid region2, neck1,34, tongue1, and throat. Pain usually increases toward the end of the day, with turning of the head and after long speaking or singing34,50. Eagle also included all cases with distortion of nerve function by the elongated styloid process, involving sensory and motor fibers of the 5th, 7th, 9th and 10th cranial nerves41,46. Patients can suffer from increased salivation2,46, a distorted sensation of taste46, esophageal and pharyngeal spasms and recurrent coughing46,51. The above described symptoms generally occur immediately after tonsillectomy and Eagle believed that the cause of the symptoms was the scar tissue formation, stretching the nerve endings4,9,46.
In the second clinical presentation of stylohyoid syndrome, the stylo-carotid syndrome, symptoms are found along the distribution of the internal or external carotid artery, due to impingement on the vessel. The styloid process affects the circulation of the carotid arteries and induces irritation of sympathetic nerves in their arterial sheaths9,41. With an affected internal carotid artery, patients will complain of parietal headaches and pains in the distribution area of the ophthalmic artery4,9,41,46. The elongated styloid process can push the internal carotid artery laterally, which may be painful on palpation46. When the external carotid artery is affected, pain will be referred to the temple and infraorbital region9,41. There is even a hypothesis that tinnitus can be caused by stylo-carotid syndrome. This could be explained because pulsating waves from the artery are conducted through the elongated styloid process towards skull and cochlea41,46.
A vegetative syndrome, including pallor, sweating, hypotension and even brief loss-of-consciousness episodes, due to irritation of the carotid perivascular plexus or carotid body by the elongated styloid process, has also been reported1,2,41,52. Wilmoth and Leger described this phenomenon as ‘Syncope styloidea’, which occurred in patients with a combination of a high bifurcation of the common carotid artery and an elongated styloid process41.
The elongated styloid process can be palpated in the tonsillar fossa during clinical examination2,46. For radiological imaging, the computed tomography (CT) preferably with 3D reconstruction is the modality of choice2,4. Sagittal CT-angiography can be useful in diagnosing stylo-carotid syndrome.
Differential diagnostic considerations for Eagle’s syndrome are numerous cranio-facio-cervical pain syndromes1,4, e.g. neuralgias of the glossopharyngeal nerve, trigeminal nerve1 and pterygopalatine ganglion9, temporomandibular disorders9,53, dental problems1,9, cervical arthropathies or pharyngeal infections and tumors1.
Therapy consists of conservative management with anti-inflammatory drugs and analgesics, or transoral surgical resection of the styloid apophysis2,4,41,46, an operation that has been performed since 187210.
Materials and Methods
Radiology
Two-hundred eighty-four excised hyoid-larynx complexes were radiologically examined and collected in a forensic-radiological database between 2002 and 201354. The database contained anonymized patient data. Approval by a medical ethical committee for this retrospective investigation in anonymized deceased patients is not required to perform this type of study in the Netherlands. It concerned a retrospective study with anonymized data from deceased persons, so written informed consent was not required. When analyzing the data none of the research team members had access to identifying information of the persons.
Age ranged from 0 to 98 years (mean: 44 years), male-female ratio was 1:1. Radiological (X-ray) examination of the excised complexes started in the early 2000s with the use of a mammograph in the following eight directions: AP, left lateral, right lateral cranio-caudal, left oblique 30 and 60 degrees, right oblique 30 and 60 degrees. A few years later this examination in eight directions was replaced by a digital bucky, supplemented with a CT scan of the excised complex. This combination became the gold standard. In later phases of the study a whole-body CT was often performed before autopsy, in addition to radiological examination of the excised complex with bucky and CT. The complex could then be virtually extracted from the whole-body CT dataset: see de Bakker et al. (2016) for protocols54. An independent researcher together with an experienced radiologist scored all radiological cases for deviations from standard anatomy as shown in Fig. 1.
Vrolik specimens
In addition to the radiological cases, we studied some profound cases with anatomical variants from the anatomical museum of the Amsterdam UMC of the University of Amsterdam, Museum Vrolik55. Images of these cases served as illustration of rare variants.
Results
Radiological examination of the 284 excised hyoid-larynx complexes showed that only 37% met the anatomical standard (Fig. 1). A remarkable 63% of the 284 cases showed various degrees of anatomical variants. Two variations were most observed: the age-dependent uni- or bilateral ankylosis of the hyoid body with the greater horns (n = 33 and 70 respectively) and uni- or bilateral presence of triticeal cartilages in the lateral thyrohyoid ligament (n = 11 and 12 respectively) (Table 2). These minor variations do not have clinical implications. Nineteen percent of this sample of 284 excised complexes, however, portrayed relevant anatomical variants (Table 2, last column).
All variations found in this study (Table 2) supplemented with rare cases described in literature and from Museum Vrolik were summarized in Fig. 2, in an attempt to provide an overview of all currently known deviations from normal anatomy of the hyoid-larynx complex. Moreover, 27 out of 33 cases with unilateral fusion between hyoid body and greater horn from which laterality and sex were known, were tabulated in Table 3. Right sided fusion was observed more frequently (n = 17) than left sided fusion (n = 10) in both sexes.
Discussion
Two thirds of the examined hyoid-larynx complexes deviated from the anatomical standard (Fig. 1). This was mostly due to minor variations like age-dependent ankylosis of the hyoid and presence of triticeal cartilages. Almost one fifth of the cases comprised more striking anatomical variants. Some of these variants have not been described in literature before. Note, however, that this sample of 284 cases may be a biased sample, because it is based on the suspicion of the pathologist of a fracture in the hyoid-larynx complex in a forensic context. Also, we examined explanted complexes and therefore elongation of the styloid process could not be determined.
Embryonic etiology of anatomical variants
When comparing the most profound deviant cases with our 3D reconstructions of embryonic development56 (freely available at http://www.3datlasofhumanembryology.com), we noted how their etiology could be explained by embryonic development (Fig. 3).

Anatomical variants of hyoid explained by embryological development. Overview of six of the most profound anatomical variants (a1,b1,c1,d1,e1,f1), compared with the embryonic development of that part of the hyoid-larynx complex (a2,b2,c2,d2,e2,f2)56. The hyoid bone (anlage) is shown in purple, second pharyngeal arch cartilage derivatives are shown in blue, third pharyngeal arch cartilage derivatives are shown in yellow and the thyroid cartilages are shown in red. The ‘L’ indicates the left side of the patient. Each arrow indicates the location of the variant. The shown variants are: conventional radiograph of an exostosis of the hyoid body (a1)(Fig. 2a7), conventional radiograph of an elongation of both lesser horns (b1)(Fig. 2c7), dried specimen of an ossified hyoid apparatus; the fundamental type (c1)* (Fig. 2e4), conventional radiograph of the left greater horn curved downward (d1)(Fig. 2b6), conventional radiograph of a bony connection between the greater and the superior horn, i.e. the congenital hypothyroid bar (e1,f1) (Fig. 2d7,d6). *On display in Museum Vrolik. Collection Louis Bolk, 1912. Photo by Sanne Mos & Marco de Marco; courtesy of Museum Vrolik, Amsterdam UMC, University of Amsterdam. With permission.
The median process
A median process of the hyoid body (n = 7) can be explained by the body’s embryological origin (Fig. 3a). The hyoid bone anlage33,57, a cylindrical shaped growth center ventrally positioned along the cranio-caudal axis in-between the left and right-sided bar of the second pharyngeal arch cartilage, marks the first appearance of the hyoid body56. We hypothesize that the median process is a remnant of this cylindrical shaped anlage.
Second pharyngeal arch cartilage anomalies
Elongation of lesser horns (Fig. 3b), styloid process (Fig. 3e2) and ossification of the hyoid apparatus (Fig. 3c) can all be explained by a degree of stylohyoid ligament ossification. The second pharyngeal arch cartilage persisted as cartilaginous bar in this trajectory after which it ossified partially (Fig. 3b1,e2) or completely (Fig. 3c1). Up until now, Eagle’s syndrome (Fig. 2e2) and the aberrant hyoid apparatus (Fig. 2e3-7) are traditionally discussed in literature as two separate entities, leading to much confusion concerning definitions and clinical presentation. Considering the embryonic etiology of these syndromes, we propose that they are merely two expressions of a broad spectrum, all due to the partial or complete persistence of the second pharyngeal arch cartilage. These anomalies are all found in the trajectory between the lesser horn of the hyoid and the styloid process. Therefore, they should be considered as one entity, preferably referred to as ‘second pharyngeal arch cartilage anomalies’.
Third pharyngeal arch cartilage anomalies (congenital hyothyroid bar)
The 3D reconstructions of the embryological development of the hyoid-larynx complex show a clear connection between the dorsal part of the bars of the third pharyngeal arch cartilages and the superior horns of the thyroid, derived from condensed mesenchymal tissue. This profound connection will become the lateral thyrohyoid ligament. Fig. 3d1,e1,f1 all show various degrees of a persisting connection between greater and superior horns. The most common variation in this trajectory is presence of a triticeal cartilage (n = 11 unilateral and n = 12 bilateral). In Fig. 3d1 the left greater horn describes a 90 degree angle pointing caudal towards superior horn. In Fig. 3e1 an accessory bone articulates between the elongated superior and greater horns. In Fig. 3f1 the greater horn articulates directly with the ossified superior horn. These cases can be explained by ossification of persisting embryological cartilaginous components in the trajectory of the lateral thyrohyoid ligament and is therefore referred to as congenital hyothyroid bar23.
One case of duplication of the greater horns has been reported5. The hyoid would miss the lesser horns and shows a duplication of the greater horns. We suggest that these duplicated horns, in fact, are more likely to be elongated lesser horns (Fig. 2c6–7).
Clinical relevance
Symptoms of variants in the hyoid-larynx complex are often not recognized by clinicians34. Great care should be taken in situations of tracheal intubation in these patients, because of the risk of regurgitation and aspiration58,59,60. Anomalies of this complex are of great importance for radiological examination and surgery of the neck region, but they should also be known by forensic experts, anthropologists, anatomists and dentists1,5 to appreciate the clinical impact of these variants and to avoid judicial errors in cases of assumed strangulation or blunt neck trauma.
Forensic relevance
Fractures in the hyoid-larynx complex are one of the best indicators of strangulation5,6,7,8, but they can also be caused by for instance hanging, traffic accidents, osteoporosis senilis, sporting accidents and after intubation8,14,20,24,42,61,62,63,64. Due to the considerable frequency of anatomical variations of the hyoid-larynx complex, great care should be taken when diagnosing traumatic lesions of this complex5,8,12.
In the normal process of ageing, the triticeal cartilage (Fig. 2d2) in the lateral thyrohyoid ligament often calcifies, which enables radiographic detection. However, when this cartilage is intensely and inhomogeneous calcified, it should not be mistaken for an avulsed fracture of the upper horn of the thyroid cartilage23,65. Therefore, oblique radiographs should be used for further radiological examination, to distinguish a fracture from an inhomogeneously calcified cartilage12.
Most fractures are found in the upper thyroid horns8. Fracturing of the hyoid occurs mainly between greater horns and body, when ankylosis is incomplete, or in the posterior part of the greater horn8,14,63,66. Since ankylosis of the hyoid joints is age dependent, fractures occur more frequent in persons aged above 305,8,13,14,18,20,21,22,23,24,67. D’Souza even stated that when a victim is over 38 years, clinicians and forensic experts can expect a fractured hyoid, after pressure on the neck20. Joint luxation between hyoid body and greater horn has also been reported in cases of strangulation63.
Some anatomical variants resemble fractures. All examples in Fig. 2 should be kept in mind when the hyoid-larynx complex is examined during medico-legal examination but especially examples b3, b7, d2, d3, d6 and d7 should always be considered when a suspected fracture is found in those locations. When the difference between variant and fracture remains ambiguous after autopsy and radiological examination, histological examination of the affected part should be performed.
Ethical approval
For this type of study formal consent is not required. This article does not contain any studies with animals performed by any of the authors.
Conclusion
We provided an overview of the known anatomical variants of the hyoid-larynx complex, with relevance for clinicians and forensic experts. Etiology of the variants has been declared by their development. Since the aberrant hyoid apparatus and Eagle’s syndrome are often intermingled in literature as they are both explained by persistence of second pharyngeal arch cartilage, we propose to refer to them as ‘second pharyngeal arch cartilage anomalies’.
References
De Paz, F. J., Rueda, C., Barbosa, M., Garcia, M. & Pastor, J. F. Biometry and statistical analysis of the styloid process. Anat. Rec. 295, 742–747 (2012).
de Santana, P. J. Jr et al. Which is your diagnosis? Radiol Bras 42, 11–12 (2009).
Naimo, P., O’Donnell, C., Bassed, R. & Briggs, C. The use of computed tomography in determining development, anomalies, and trauma of the hyoid bone. Forensic Sci Med Pathol 11, 177–185 (2015).
Petrovic, B., Radak, D., Kostic, V. & Covickovic-Sternic, N. Styloid syndrome: a review of literature. Srp Arh Celok Lek 136, 667–674 (2008).
Gok, E., Kafa, I. M. & Fedakar, R. Unusual variation of the hyoid bone: bilateral absence of lesser cornua and abnormal bone attachment to the corpus. Surg Radiol Anat 34, 567–569 (2012).
Kindschuh, S. C., Dupras, T. L. & Cowgill, L. W. Determination of sex from the hyoid bone. Am J Phys Anthropol 143(2), 279–284 (2010).
Urbanova, P., Hejna, P., Zatopkova, L. & Safr, M. The morphology of human hyoid bone in relation to sex, age and body proportions. Homo 64, 190–204 (2013).
Saukko, P., Knight, B. Knight’s Forensic Pathology, Fourth edition (CRC Press, Taylor & Francis Group, 2015).
Eagle, W. W. Symptomatic elongated styloid process; report of two cases of styloid process-carotid artery syndrome with operation. Arch Otolaryngol 49, 490–503 (1949).
Eagle, W. W. Elongated styloid process; symptoms and treatment. AMA Arch Otolaryngol 67, 172–176 (1958).
Wellinger, C., Dugast, P. & Desnos, J. The hyoid apparatus. Rhumatologie 18, 15–26 (1966).
Di, N. N., Lombardo, S., Costantinides, F. & Di, N. C. Anomalies and alterations of the hyoid-larynx complex in forensic radiographic studies. Am J Forensic Med Pathol 25, 14–19 (2004).
Pollanen, M. S. & Chiasson, D. A. Fracture of the hyoid bone in strangulation: comparison of fractured and unfractured hyoids from victims of strangulation. J Forensic Sci 41, 110–113 (1996).
Soerdjbalie-Maikoe, V. & van Rijn, R. R. Embryology, normal anatomy, and imaging techniques of the hyoid and larynx with respect to forensic purposes: a review article. Forensic Sci Med Pathol 4, 132–139 (2008).
Watanabe, H., Kurihara, K. & Murai, T. A morphometrical study of laryngeal cartilages. Med Sci Law 22, 255–260 (1982).
Radlanski, R. J. & Renz, H. An atlas of prenatal development of the human orofacial region. Eur J Oral Sci 118, 321–324 (2010).
Kindschuh, S. C., Dupras, T. L. & Cowgill, L. W. Exploring ancestral variation of the hyoid. J Forensic Sci 57, 41–46 (2012).
Miller, K. W., Walker, P. L. & O’Halloran, R. L. Age and sex-related variation in hyoid bone morphology. J Forensic Sci 43, 1138–1143 (1998).
Pollard, J. et al. Mechanisms of hyoid bone fracture after modelling: evaluation of anthropological criteria defining two relevant models. Forensic Sci Int 212, 274–275 (2011).
D’Souza, D. H., Harish, S. S. & Kiran, J. Fusion in the hyoid bone: usefulness and implications. Med Sci Law 50, 197–199 (2010).
Gupta, A., Kohli, A., Aggarwal, N. K. & Banerjee, K. K. Study of age of fusion of hyoid bone. Leg Med 10, 253–256 (2008).
Hänsch, C. F. Throat-skeleton fractures by strangulation. Z Rechtsmed 79, 143–147 (1977).
Porrath, S. Roentgenologic considerations of the hyoid apparatus. Am J Roentgenol Radium Ther Nucl Med 105, 63–73 (1969).
Ubelaker, D. H. Hyoid fracture and strangulation. J Forensic Sci 37, 1216–1222 (1992).
Pollanen, M. S. & Ubelaker, D. H. Forensic significance of the polymorphism of hyoid bone shape. J Forensic Sci 42, 890–892 (1997).
Jelisiejewa, T., Szmurlo, J. & Kuduk, I. Studies on the morphology of the hyoid bone in man. Folia Morphol 27, 189–198 (1968).
Reesink, E. M., Van Immerseel, A. A. H., Brand, R. & Bruintjes, T. D. Sexual Dimorphism of the Hyoid Bone? Int J Osteoarchaeol 9, 357–360 (1999).
Shimizu, Y. et al. Age-related morphological changes in the human hyoid bone. Cells Tissues Organs 180, 185–192 (2005).
Jurik, A. G. Ossification and calcification of the laryngeal skeleton. Acta Radiol Diagn 25, 17–22 (1984).
Fisher, E. et al. Hyoid bone fusion and bone density across the lifespan: prediction of age and sex. Forensic Sci Med Pathol 12, 146–157 (2016).
Pendergrass, E. P., Hodes, P. J. & Schaeffer, J. P. The Head and Neck in Roentgen Diagnosis. Second edition (Charles C. Thomas, 1956).
Vanezis, P. Pathology of Neck Injury (Butterworths, 1989).
Dwight, T. IX. Stylo-hyoid Ossification. Ann Surg 46, 721–735 (1907).
Shul’ga, I. A., Zaitsev, N. V. & Zaitseva, V. S. Variants of the structure of the stylohyoid complex. Vestn Otorinolaringol 6, 72–73 (2006).
Chiang, K. H., Chang, P. Y. & Chou, A. S. B. Eagle’s syndrome with 3-D reconstructed CT: two cases report. Chin J Radiol 29, 353–357 (2004).
Lykaki, G. & Papadopoulos, N. The ossified hyoid apparatus–morphology, interpretation, clinical and functional significance. Presentation of a rare case and highlights of the literature. Anat Anz 166, 187–193 (1988).
Vougiouklakis, T. Overview of the ossified stylohyoid ligament based in more than 1200 forensic autopsies. J Clin Forensic Med 13, 268–270 (2006).
Reichert, C. Ueber die Visceralbogen der Wirbelthiere im Allgemeinen und deren Metamorphosen bei den Vögeln und Säugethieren in Archiv für Anatomie, Physiologie und Wissenschaftliche Medicin (ed. Müller, J.) 120–222 (von Verlag, 1837).
von Lanz, T. & Wachschmuth, W. Praktische Anatomie, Bd. 1/2 Hals, S.69. (Springer, 1955).
Harburger, A. Étude anatomique clinique et radiologique de l’appareil hyoïdien normal et anormal chez l’homme. Arch Int de Laryngol 4, 1047–1076 (1925).
Lesoine, W. Anomalies of the hyoid bone chain. HNO 14, 70–73 (1966).
Marcucci, L. L’ Apparato Joideo: Anatomia, Fisiopatologia e Clinia (Ricerche ed Osservazioni Personali), Third edition (L’Ateneo Parmense, 1959).
Graf, C. J. Glossopharyngeal neuralgia and ossification of the stylohyoid ligament. J Neurosurg 16, 448–453 (1959).
Frommer, J. Anatomic variations in the stylohyoid chain and their possible clinical significance. Oral Surg Oral Med Oral Pathol 38, 659–667 (1974).
Chi, J. & Harkness, M. Elongated stylohyoid process: a report of three cases. N Z Dent J 95, 11–13 (1999).
Eagle, W. W. Elongated styloid process; further observations and a new syndrome. Arch Otolaryngol 47, 630–640 (1948).
Eagle, W. W. The symptoms, diagnosis and treatment of the elongated styloid process. Am Surg 28, 1–5 (1962).
Jung, T., Tschernitschek, H., Hippen, H., Schneider, B. & Borchers, L. Elongated styloid process: when is it really elongated? Dentomaxillofac Radiol 33, 119–124 (2004).
Garriz-Luis, M., Irimia, P., Alcalde, J. M., Dominguez, P. & Narbona, J. Stylohyoid Complex (Eagle) Syndrome Starting in a 9-Year-Old Boy. Neuropediatrics 48, 53–56 (2017).
Shimada, K. & Gasser, R. F. Morphology of the mandibulo-stylohyoid ligament in human adults. Anat Rec 222, 207–210 (1988).
Lavallee, M. & Turcotte, J. Y. Changes in the stylohyoid chain and Eagle’s syndrome. Union Med Can 113, 413–416 (1984).
Warot, P. Elongated styloid apophysis. Rev Otoneuroophtalmol 48, 145–152 (1976).
Zaki, H. S., Greco, C. M., Rudy, T. E. & Kubinski, J. A. Elongated styloid process in a temporomandibular disorder sample: prevalence and treatment outcome. J Prosthet Dent 75, 399–405 (1996).
de Bakker, H. M., Soerdjbalie-Maikoe, V., Kubat, B., Maes, A. & de Bakker, B. S. Forensic imaging in legal medicine in the Netherlands: Retrospective analysis of over 1700 cases in 15 years’ experience. J Forensic Radiol Imaging 6 (2016).
de Rooy, L., van den Bogaard, H. Forces of Form: The Vrolik Museum (Amsterdam University Press, 2010).
de Bakker, B. S., de Bakker, H. M., Soerdjbalie-Maikoe, V. & Dikkers, F. G. The development of the human hyoid-larynx complex revisited. Laryngoscope 128, 1829–1834 (2018).
Rodriguez-Vazquez, J. F. et al. Human fetal hyoid body origin revisited. J Anat 219, 143–149 (2011).
Ames, W. A. & McNiellis, N. Stylohyoid ligament calcification as a cause of difficult intubation? Anaesthesia 53, 415–416 (1998).
Aris, A. M., Elegbe, E. O. & Krishna, R. Difficult intubation stylohyoid ligament calcification. Singapore Med J 33, 204–205 (1992).
Brimacombe, J., Brands, E., Wells, J. & Douglas, J. Difficult LMA insertion due to prominent stylohyoid ligaments. Anaesth Intensive Care 32, 595–596 (2004).
Dunsby, A. M. & Davison, A. M. Causes of laryngeal cartilage and hyoid bone fractures found at postmortem. Med Sci Law 51, 109–113 (2011).
Kleinberg, S. Brief communications: Fracture of the hyoid bone. Ann Surg 99, 547–556 (1934).
Lesoine, W. On fractures and dislocations of the hyoid bone. HNO 14, 122–124 (1966).
Porr, J., Laframboise, M. & Kazemi, M. Traumatic hyoid bone fracture - a case report and review of the literature. J Can Chiropr Assoc 56, 269–274 (2012).
Khokhlov, V. D. Injuries to the hyoid bone and laryngeal cartilages: effectiveness of different methods of medico-legal investigation. Forensic Sci Int 88, 173–183 (1997).
Pollanen, M. S., Bulger, B. & Chiasson, D. A. The location of hyoid fractures in strangulation revealed by xeroradiography. J Forensic Sci 40, 303–305 (1995).
Leksan, I., Marcikic, M., Nikolic, V., Radic, R. & Selthofer, R. Morphological classification and sexual dimorphism of hyoid bone: new approach. Coll Antropol 29, 237–242 (2005).
Klovning, J. J. & Yursik, B. K. A nearly circumferential hyoid bone. Am J Otolaryngol 28, 194–195 (2007).
Acknowledgements
A.F.M. Moorman and K.H. de Jong are acknowledged for their useful comments on the research design. We acknowledge all radiologists, forensic radiographers, pathologists and pathology assistants who have contributed to our forensic-radiological database. We thank L de Rooy and M de Marco of Museum Vrolik and photographer Sanne Mos for providing the picture for Figure 3c1. A Sizarov is acknowledged for translating the Russian literature. RJ Oostra, M.J.B. van den Hoff and J.M. Ruijter are acknowledged for critically reading the manuscript.
Author information
Authors and Affiliations
Contributions
B.S.B. and H.M.B. wrote the main manuscript, prepared the figures and were responsible for the embryological and radiological content respectively. V.S.M. and F.G.D. critically commented on the manuscript and were responsible for the pathology contribution and the clinical relevance respectively.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
de Bakker, B.S., de Bakker, H.M., Soerdjbalie-Maikoe, V. et al. Variants of the hyoid-larynx complex, with implications for forensic science and consequence for the diagnosis of Eagle’s syndrome. Sci Rep 9, 15950 (2019). https://doi.org/10.1038/s41598-019-52476-z
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-52476-z
This article is cited by
-
Lowered hyoid bone overlapping the thyroid cartilage in CT angiograms
Surgical and Radiologic Anatomy (2024)
-
Anatomische Varianten der oberen Wirbelsäule – ihre Bedeutung für die manuelle Medizin
Manuelle Medizin (2023)
-
Comparison of findings identified at traditional invasive autopsy and postmortem computed tomography in suicidal hangings
International Journal of Legal Medicine (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
