
Abstract
Modifying behavior towards healthier lifestyles could prevent a significant number of malignant tumors. We evaluated the prevalence of healthy habits against cancer in Spanish women free of this disease, taking as a reference the recommendations for cancer prevention included in the European Code Against Cancer (ECAC), and we explored the characteristics associated with it. Our population comprised 3,584 women recruited in a population-based cross-sectional study carried out in 7 breast cancer screening programs. Information was directly surveyed and used to calculate a score based on ECAC recommendations referred to bodyweight, physical activity, diet, breastfeeding, tobacco, alcohol and hormone replacement therapy use. The degree of adherence was estimated with a score that evaluated null (0 points), partial (0.5 points) and full adherence (1 point) of each specific recommendation. Associations were explored using binary and ordinal logistic regression models. The median score was 5.7 out of 9 points. Recommendations with lower adherence were those related to intake of red/processed meat and foods high in salt (23% of total adherence), physical activity (24%) and body weight (29%), and recommendations with greater adherence where those related to hormone replacement therapy use (91%), vegetable intake (84%), alcohol (83%) and tobacco (61%). Overall adherence was better among older women, parous women, and in those living in rural areas, and worse among women with higher caloric intake. These recommendations should be evaluated periodically. Screening programs can be an appropriate place to disseminate this information.
Similar content being viewed by others

Introduction
Cancer is the second leading cause of death globally. It was responsible for 9.6 million deaths in 2018 accounting for one of every 6 deaths1. In Spain it was the second cause of mortality in women, accounting for 20% in 20152. In comparison with other European countries, the incidence of cancer in Spanish women (227.1 cases per 100,000) is below the European mean (253.3 per 100,000). However, it is the second country with the lowest mortality due to this cause, with 65.9 deaths per 100,000 in 20183. Despite the stabilization of breast cancer incidence, there has been an increase in colorectal and tobacco-related cancers, and geographic differences in incidence rates have been described4. Malignant tumors also imply a substantial economic burden across European Union5. It has been estimated that the health-care cost of cancer in Spain was 4114 million euros in 2009, equivalent to €102 per citizen. It accounted for 4% of total Spanish health-care expenditure, and the 0.86% of gross domestic product. Breast cancer had the greatest overall economic burden5.
Cancer is a complex illness resulting from the interaction between genes and environmental factors such as tobacco6,7,8, obesity/overweight9,10,11,12, unhealthy diets10,12,13, physical inactivity10,12,14,15, alcohol intake8,10,12,16, certain environmental and occupational exposures6,17,18, ionizing radiation19,20, several infectious agents21, and hormone therapy22,23. A significant number of cases could be prevented avoiding or reducing exposure to these risk factors24. Several studies have analyzed adherence to cancer prevention guidelines and their relationship to this disease25,26,27, but have not analyzed the sociodemographic and lifestyle factors influencing such adherence28. In Spain, although trends for many risk factors -such as alcohol consumption or healthier diets- have improved in recent years, the prevalence of tobacco consumption among men remains high; there has been an upward trend in smoking among women aged 45–64 years, and physical inactivity has conditioned an increase in obesity figures in the general population29.
To emphasize the importance of cancer prevention, the International Agency for Research on Cancer (IARC) published in 2014 the new edition of the European Code Against Cancer (ECAC), with 12 recommendations regarding primary and secondary prevention: (1) Do not smoke; (2) Support smoke-free policies; (3) Be a healthy body weight; (4) Be physically active; (5) Have a healthy diet (three recommendations are included here: 5.1 eat plenty of whole grains, pulses, vegetables and fruits; 5.2 limit high-calorie foods and avoid sugary drinks; 5.3 avoid processed meat and limit red meat and foods high in salt); (6) Limit your alcohol intake; (7) Avoid too much sun; (8) Protect yourself against cancer-causing substances in your workplace; (9) Take action to reduce high radon levels; (10) Breastfeed your baby and limit use of hormone replacement therapy (HRT); (11) Ensure your children take part in vaccination programmes for hepatitis B (newborns) or human papillomavirus (girls); (12) Take part in cancer screening programmes for bowel cancer (men and women), breast and cervical cancer (women)30,31.
Our objective is to evaluate the prevalence of healthy habits against cancer in women who attend breast cancer screening programs in Spain, taking as a reference of good practices the recommendations of ECAC related to smoking, obesity, diet, alcohol, breastfeeding and HRT use. We also try to explore what sociodemographic and lifestyle factors are associated. This information can be useful to define priorities and public health actions with the purpose of reducing the burden of cancer in the population and the inequalities between different Spanish geographical areas.
Materials and Methods
Study population
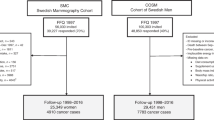
DDM-Spain study (Determinants of Mammographic Density in Spain) is a cross-sectional multicenter study that recruited, between October 2007 and July 2008, 3,584 healthy women, aged 45 to 68 years, from 7 specific screening centers within the Spanish breast cancer screening programme network. In Spain, all women aged 50 to 69 years, regardless of their nationality or legal status, are screened under these government-sponsored population-based programs every 2 years (in some regions women aged 45 to 49 are also included). Attendance rates range from 62.9% to 88.0% of its target population, depending on the region. Seven screening centers located in Aragon, Balearic Islands, Castile-Leon, Catalonia, Galicia, Navarre, and Valencian Region participated in DDM-Spain. The recruiting centers contacted all screening attendants by telephone and invited them to participate in the study. Those who accepted were interviewed at their screening center the day scheduled for their mammogram, shortly after the first telephone contact. As a measure to minimize erroneous information, women were re-contacted by phone to corroborate inconsistent or unclear data after the interview. Furthermore, a subsample of 150 women were re-interviewed to test the consistency of the information reported, particularly regarding their diet, given the difficulty inherent to food frequency questionnaires, with very good agreement between the first and second questionnaires32. The overall participation rate was 74.5% (64.7%–84.0%).
The study was approved by the Research Ethics Committee of the Carlos III Institute of Health, and all participants signed an informed consent form. All research was conducted in accordance with relevant guidelines and regulations. Further information about the DDM-Spain study can be consulted elsewhere33,34,35.
Study variables
Structured face-to-face questionnaires were administered by trained interviewers to collect data about women’s sociodemographic, reproductive, and lifestyle habits. The survey included a 117-item validated semi quantitative food frequency questionnaire that collected the eating habits of the previous 12 months36,37. In addition, an anthropometric examination of all participants was conducted following standardized procedures, and using the same scale, stadiometer and measuring tape models in all study centers.
We elaborated an index based on the following 9 ECAC recommendations (including diet sub-recommendations) for primary prevention of cancer: (1) Do not smoke; (2) Be a healthy body weight; (3) Be physically active; (4) Eat plenty of whole grains, pulses, vegetables and fruits; (5) Limit high-calorie foods and avoid sugary drinks; (6) Avoid processed meat, limit red meat and foods high in salt; (7) Limit your alcohol intake; (8) Breastfeed your baby; and (9) Limit HRT use. We could not include other ECAC recommendations due to lack of information. A maximum score of 1 was assigned when the recommendation was fully met, an intermediate value of 0.5 when the recommendation was not far from being met and 0 points otherwise (see Supplementary Table S1). Given their heterogeneity, specific recommendations related to diet were evaluated separately, using the cut-off points proposed by a previous study25.
The final score was obtained as the sum of the individual scores. Therefore, the ECAC score ranged from 0 (none of these recommendations was met) to 9 (all of them were fully met). Taking into account the distribution of the score, three categories of adherence were considered: low adherence (<5), moderate adherence (5–<6.5) and high adherence (≥6.5). These cut-off points were determined as tertiles of each individual score.
The following characteristics were evaluated as possible determinants of adherence to the ECAC recommendations: age, menopausal status (defined as absence of menstruation in the last 12 months), geographic area, self-reported socioeconomic level at the time of the interview and at birth, educational level, ethnicity, civil status, town-size of residence, occupational status, frequency of eating out, having to take care children and/or elderly people at home, family history of cancer, and reproductive factors (number of miscarriages/abortions and number of deliveries).
Statistical analyses
Descriptive analyses of women’s characteristics were performed using means and standard deviations for continuous variables and absolute figures and percentages for categorical variables. Significant differences were tested using Pearson chi-square for categorical variables and Student’s t-test for continuous variables.
The association between the three categories of adherence, as a measure of overall compliance to ECAC recommendations, and sociodemographic and lifestyle characteristics, was evaluated using ordinal logistic regression models. First of all, a minimum adjustment model was used, for each factor including only age and place (location of the screening center) as possible confounders. Then, a final multivariate model was fitted considering all those factors associated with the score in the previous model (p < 0, 10) (namely, age, screening center, educational level, size of residence town, eating out, civil status, and number of deliveries).
The effect of these factors on the adherence to individual ECAC recommendations was also evaluated using multivariate logistic regression models. A separate model was fitted for each specific recommendation, considering the same determinants included in the multivariate model mentioned before. In the case of the geographical location of the screening center, the average value of all of them was used as a reference. These models were also adjusted for the overall adherence to the other recommendations, which were obtained by adding up the scores of all individual recommendations, except the one under study.
Analyses were performed using STATA/MP 12.0 software.
Results
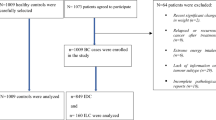
Of the 3584 women recruited, we analyzed those from which we obtained complete data for the variables age and location of the screening center (3550). The distribution of sociodemographic and life-style characteristics of these women is shown in Table 1. Mean age was 56 years. Most women were postmenopausal (77%), of medium socioeconomic status (71%), of low social status at birth (58%), with secondary education (56%), Caucasian (99%), and married (80%). Most of them lived in small cities (75%) and were active workers or had worked in the past (86%). Only 8% of women lived with people who needed care at home and 48% reported eating out at least 2 times/month (on average, these women ate out between 5 and 6 times per month). Only 9% of them were nulliparous, 28% had more than two children and 21% reported one or more miscarriages/abortions. Regarding family history of cancer, a substantial proportion reported having a first or second degree relative with a diagnosis of cancer at any location (46%). The overall score ranked between 1 and 9 with a mean of 5.71. 33% of the women showed low adherence to the ECAC recommendations. This percentage was 50% for moderate adherence and 17% for high adherence. On average, women with higher adherence were older, while low adherence was more prevalent among those women with higher educational level, single, nulliparous, those who lived in more populated towns, those gainfully employed, and in those who reported frequently eating out and consumed more calories (Table 1). In relation to individual recommendations, adherence was very high regarding the limitation of HRT use (91%), the frequent intake of grains, pulses, vegetables and fruits (84%) and low alcohol consumption (83%), and the adherence was lower for the low consumption of processed meat, red meat and foods high in salt (23% of total adherence) and for the recommendation of physical activity (24%) (Fig. 1).

Degree of adherence to European Code Against Cancer recommendations.
Table 2 shows the association of those sociodemographic, reproductive and lifestyle factors with the overall score of adherence (P < 0.10), adjusting only for age and screening center (simple model) and additionally including all of them in a final model (right columns). According to the geographical location of the screening center, women from Zaragoza showed a statistically significant higher adherence to ECAC recommendations, whereas women from Palma had the worst degree of adherence. Better adherence was observed in older women (ORage≥60:1.25; CI:1.07–1.45), in women who lived in rural and intermediate towns (OR:1.28; CI:1.09–1.50) and among those with more children (OR≥3 children:1.90; CI:1.39–2.58). Conversely, younger women, single, and those who consumed more calories showed lower adherence to cancer recommendations. We did not observe differences in global adherence by educational level in the multivariated model.
Tables 3–5 show the association of these characteristics with adherence to each specific ECAC recommendation. Table 3 includes recommendations related to tobacco, body weight and physical activity; Table 4 presents the three recommendations related with a healthy diet and Table 5 shows the last three: alcohol, breastfeed and HRT use. Due to the small number of women who did not adhere to the “limit high-calorie foods and sugary drinks” recommendation, the first two categories (non adherent and partially adherent women) of this variable were combined in a single group, which was used as a reference. While older women showed higher adherence to recommendations related to smoking and breastfeeding, these same women presented worse adherence to recommendations related to body weight and physical activity. Women with higher educational level seemed to have greater adherence to recommendations related to maintaining a healthy weight, but they adhered worse to the recommendations related to alcohol and HRT use. Women living in rural or intermediate towns had higher adherence to recommendations related to tobacco, physical activity and consumption of high calorie foods and sugary drinks. Women who reported eating out several times per month had higher adherence to the recommendation of being physically active, but failed to limit their alcohol intake and the consumption of red/processed meat and salty food. Parous women drank less alcohol, but were less prone to maintain a healthy body weight and to limit the consumption of high calorie foods, sugary drinks, red/processed meat and salty food. Furthermore, compared to women with 1–2 children, those with 3 or more children had greater adherence to the recommendation of breastfeeding, as expected. On the other hand, while divorced women reported better adherence to maintaining a healthy weight, widows ate larger amounts of grains, pulses, vegetables and fruits and married and divorced women ate less quantity of high-calorie foods and sugary drinks. Finally, women who consumed more calories had a healthier weight and did more physical activity, but also consumed more grains, pulses, vegetables, fruits, high-calorie foods, sugary drinks, red and processed meat, salty food and alcohol.
There were significant differences in the degree of adherence to these recommendations by geographical area. The greatest heterogeneity was observed for consumption of grains, pulses, vegetables and fruits (high adherence in Palma and low in Corunna), the limitation in alcohol consumption (high adherence in Corunna and Barcelona and low in Burgos) and the limitation in the consumption of high-calorie foods and sugary drinks (high adherence in Zaragoza and Corunna and low in Burgos). Maintaining a healthy body weight was mainly observed in Zaragoza and Burgos. This last city was also the one with greater adherence to the recommendation of being physically active. Valencia was the city that consumed the least amount of red/processed meat and salty food. Palma had very poor adherence to the breastfeeding recommendation. Burgos and Pamplona were the most HRT users. Finally, differences in smoking were less marked.
Discussion
Although in recent years many studies have explored the association of the adherence to cancer prevention guidelines with cancer risk or mortality25,26,27, very few have explored the sociodemographic and lifestyle factors influencing such adherence28. The present study tries to know how Spanish women behave with respect to cancer risk factors, taking as a reference the recommendations of the ECAC. The study also tries to identify which sociodemographic and lifestyle factors are conditioning the acquisition of healthier lifestyles, in order to intervene in them with public health actions. Our results show that global adherence to these recommendations by Spanish women attending breast cancer screening is moderate, higher for HRT use, alcohol intake and consumption of vegetables, fruits and grains, and lower for consumption of processed meat, red meat and foods high in salt, physical activity and body weight. In general, overall adherence was higher among older women, parous women and in those living in rural areas. Our results also highlight differences in adherence to specific recommendations according to women’s characteristics, which should inform prevention campaigns. Thus, older women should increase physical activity and take better care of their body weight, while younger women should stop smoking as well as decrease the intake of red and processed meat and salty products. Women who eat out frequently should give attention to their consumption of alcohol and red/processed meat and salty food. Women with children should also reduce the intake of this type of food, as well as high calorie food and sugary drinks, and take better care of their body weight. Finally, women with higher caloric intake should reduce the consumption of the mentioned products, as well as their alcohol intake. The adherence to recommendations was very heterogeneous in the different geographical locations, being Zaragoza and Palma the cities with healthier and unhealthier lifestyles respectively.
Our study has some limitations that must be taken into account. Firstly, we could not evaluate other recommendations included in the ECAC for cancer prevention due to lack of information on passive smoking, sun and sunbeds exposure, occupational exposure to carcinogens and use of protective equipment, natural radiation and status of vaccination against hepatitis B (HPV vaccination has been introduced recently in our country). Secondly, with the exception of body mass index (BMI), the information on women characteristics was self-reported, so behaviors considered socially desirable or healthy may have been overestimated by our participants, consciously or unconsciously. Regarding the representativeness of the study population, it has been argued that women attending screening programs may have different sociodemographic characteristics and tend to be more aware of the importance of prevention than the general population38. However, coverage of breast cancer screening in Spain reached almost 100% of the target population in all Autonomous Communities in 2006, with high participation rates39, which supports the external validity of our results. In addition, according to data provided by the National Health Survey for Spanish women in the same age range40, our women were very similar to the national sample in terms of prevalence of alcohol consumption, prevalence of non-smokers, prevalence of intense physical activity and use of hormone replacement therapy.
The relative independence of each ECAC recommendation justify the discussion of our results separately.
Don’t smoke
Tobacco smoking is the single largest preventable cause of cancer in the European Union. Although Spain is one of the European countries with higher proportion of smokers41, a reduction has been observed following the implementation of the last smoke-free legislation. In 2011, the prevalence of current smokers (daily and casual) in adult women was 22.8%40, very similar to the data reported here.
Adherence to tobacco recommendation was higher in older women, in less educated women and in those living in middle-sized towns and rural areas. Smoking prevalence in Spanish females varied greatly by birth cohort and education. The tobacco epidemic started earlier among highly educated women, and those born between 1960 and 1980 were exposed to large amounts of targeted advertisement at a vulnerable age42. These generations are represented in our study by those women younger than 50. Currently, although prevalence has declined at all levels, it is still higher in women with higher education40. Regarding population size, Idris et al.43 also reported higher prevalence of smoking in women living in urban areas of Spain, being these inequalities more pronounced among those with low educational level.
Be a healthy body weight
Body fatness is an important problem in Spain, where the prevalence of overweight and obesity have increased progressively, reaching a rate of 24.1% of obese women and 54.6% of overweight women in 201444. Given these figures, it is not strange to find that this recommendation shows the lowest level of adherence (71% of no adherence). Older women and those with more deliveries presented higher BMI in our study. The association of obesity with age is well known45, and the increased BMI associated with increasing parity (independently of socioeconomic and other lifestyle factors) has also been previously described46. On the other hand, women with higher educational level tended to present healthier BMI. Rodriguez Caro et al.47, in a recent study, described that education was the most important source of social differences in obesity among women in Spain, being this educational gradient greater at the end of the BMI distribution.
Be physically active
There is strong evidence that physical activity protects against colon, breast and endometrial cancer, and probably also against lung cancer10,12,15. In Spain, the prevalence of physical inactivity is increasing, reaching a rate of 44% in 201348.
In our study, the proportion of women who classified themselves as mostly inactive was 24%, which is lower than that reported by the National Health Survey in relation to adherence to the World Health Organization recommendations for physical activity (35.8%)49. The adherence of our women differed by age and size of town. The greater frequency of physical activity in younger people has been described in Europe48, and Whelan et al.28 also described greater adherence to the physical activity recommendation among this collective. The higher prevalence of physical activity among women living in rural areas could be related to regular walking, since Spain is the second country of the European Union where regular walking is more prevalent48, and the rural areas are a favourable environment for this type of activity.
Have a healthy diet: Recommendations on (1) increasing intake of whole grains, pulses, vegetables and fruits, (2) limiting/avoiding high-calorie foods and sugary drinks, (3) avoiding/limiting processed meat, meat and foods high in salt
We have evaluated these recommendations separately because the degree of adherence is very heterogeneous in our population. Although most women meet the recommendation of high consumption of fruits and vegetables, adherence to the recommendation to limit consumption of red and processed meat, fast food, and salty foods has been very low, mainly among younger women. Regarding fast food, high-calorie foods and sugary drinks, the percentage of women with lack of adherence was very low, except in the case of fast food. In fact, the consumption and the variety of prepared dishes has risen significantly in recent years in Spanish households50 and, as in our study, the demand for these products increases with the size of the population51. The consumption of meat products in 2009 accounted for 20.8% of total food expenditure52, and 21.8% in 201553. The demand for these products outside the home experienced a significant increase from 1995 to 2009, retreating subsequently due to the crisis52. As in our study, middle-upper-class households showed the highest consumption. However, contrary to what was observed in 2009 in Spanish households52, the parous women of our study showed a higher demand for these products.
Alcohol
It has been estimated that about 4.2% of all cancer cases in women are attributable to alcohol consumption in the European Region54. In Spain, this figure is around 4%55. In our study, more than 80% of women totally accomplished this recommendation, which is in consonance with the considerable decrease in alcohol intake observed in the last decade56,57. Adherence to this recommendation was higher among younger women and lower among those with a university degree and among those who reported eat out frequently and consumed more calories. The latest alcohol survey in Spain58 also shows that, in general, alcohol consumption has shifted towards older women, with greater prevalence among women aged 55–64. However, the highest prevalence is observed in adolescents and young adults, women between 15 and 24 years old58. On the other hand, alcohol consumption in Spanish women is considerably higher at the highest educational levels: 71.7% of university women had drunk alcohol in the last year, compared to 27.9% of women without studies58.
Breastfeeding
In Spain, the percentage of children under 5 who have been totally or partially breastfed has increased since 1995 thanks to the Initiative for the Humanization of Birth and Breastfeeding Assistance (IHAN) (launched by WHO and UNICEF to encourage hospitals, health services, and maternity wards to adopt practices that promote and support exclusive breastfeeding from birth)59. According to the latest National Health Survey, 66.5% of infants were exclusively or partially breastfed up to 3 months of age, and 47.0% up to 6 months in 201159. In our study, older women presented higher adherence to this recommendation, which might be due to a higher proportion of housewives at time of delivery, compared to younger cohorts, which facilitated the extension of the lactation period. Obviously, multiparous women comply better with this recommendation, which includes life-long accumulated breastfeeding. Moreover, a previous successful experience with breastfeeding can also make women more prone to breastfeed the next child.
Hormonal replacement therapy
Spain is one of the European countries with the lowest HRT use60, which has declined progressively from 2001 to 2007, but remains stable since then61. It has been estimated that the prevalence of current HRT use in 2014 was 0.21% in women older than 40 years, with the 40–45 age group being the most prevalent61. This recommendation shows the highest degree of adherence in our study (8.6% ever used HRT). Our rate is similar to the prevalence described in another population-based Spanish multicenter study (9.8%) in which HRT use was associated with higher social class62. This study, also reported that women born in the 1940s (older women of our study) were the most exposed to HRT62.
In conclusion, our results show that the degree of adherence to the lifestyle ECAC recommendations for cancer prevention among Spanish women attending breast cancer screening was, in general, moderate. Two out of three women adhered totally or partially. Some recommendations should be encouraged, particularly those related to obesity, meat and salty food consumption and breastfeeding. In Spain, where most people never heard about ECAC recommendations, outreach campaigns targeting both the general public and health professionals are needed, as well as government policies and actions that facilitate healthier choices and create environments that promote behavioral change towards healthier lifestyles. The high participation rates in the Spanish breast cancer screening programmes reflect the interest of these women in cancer prevention. This may be a critical moment to provide information on lifestyles useful to decrease their risk of cancer. It would also be very interesting that the National Strategy in Cancer periodically evaluate the degree of adherence to cancer prevention recommendations defined in the ECAC in different population areas, in order to measure the effectiveness of this tool promoted by IARC.
Data Availability
The datasets generated are not publicly available due to restrictions imposed by the Carlos III Ethic Committee, but are available from the principal investigator on reasonable request.
References
WHO. World Health Organization. WHO Media centre. Cancer fact sheet, http://www.who.int/mediacentre/factsheets/fs297/en/ (2017).
CNE. Centro Nacional de Epidemiología. Mortalidad por cáncer y otras causas en España. Año 2015, http://www.isciii.es/ISCIII/es/contenidos/fd-servicios-cientifico-tecnicos/fd-vigilancias-alertas/fd-epidemiologia-ambiental-y-cancer/Mortal2015.pdf (2017).
Ferlay, J. et al. Global Cancer Observatory: Cancer Today, https://gco.iarc.fr/today (2018).
Galceran, J. et al. Cancer incidence in Spain, 2015. Clin Transl Oncol (2017).
Luengo-Fernandez, R., Leal, J., Gray, A. & Sullivan, R. Economic burden of cancer across the European Union: a population-based cost analysis. Lancet Oncol. 14, 1165–1174 (2013).
Cogliano, V. J. et al. Preventable exposures associated with human cancers. J Natl Cancer Inst. 103, 1827–1839 (2011).
Leon, M. E. et al. European Code against Cancer, 4th Edition: Tobacco and cancer. Cancer Epidemiol. 39(1), S20–33 (2015).
WHO/IARC. World Health Organitation. International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Personal habits and indoor combustions. Vol 100 E, http://monographs.iarc.fr/ENG/Monographs/vol100E/mono100E.pdf (2012).
Anderson, A. S. et al. European Code against Cancer 4th Edition: Obesity, body fatness and cancer. Cancer Epidemiol. 39(1), S34–45 (2015).
Latino-Martel, P. et al. Alcoholic beverages, obesity, physical activity and other nutritional factors, and cancer risk: A review of the evidence. Crit Rev Oncol Hematol. 99, 308–323 (2016).
Renehan, A. G., Tyson, M., Egger, M., Heller, R. F. & Zwahlen, M. Body-mass index and incidence of cancer: a systematic review and meta-analysis of prospective observational studies. Lancet. 371, 569–578 (2008).
WCRF/AICR. World Cancer Research Fund International/American Institute for Cancer Research. Diet, nutrition, physical activity and cancer: a global perspective. Continuous update project expert report 2018, https://www.wcrf.org/dietandcancer (2018).
Norat, T. et al. European Code against Cancer 4th Edition: Diet and cancer. Cancer Epidemiol. 39(1), S56–66 (2015).
Friedenreich, C. M., Neilson, H. K. & Lynch, B. M. State of the epidemiological evidence on physical activity and cancer prevention. Eur.J.Cancer. 46, 2593–2604 (2010).
Leitzmann, M. et al. European Code against Cancer 4th Edition: Physical activity and cancer. Cancer Epidemiol. 39(1), S46–55 (2015).
Scoccianti, C. et al. European Code against Cancer 4th Edition: Alcohol drinking and cancer. Cancer Epidemiol. 45, 181–188 (2016).
Espina, C. et al. European Code against Cancer 4th Edition: Environment, occupation and cancer. Cancer Epidemiol. 39(1), S84–92 (2015).
WHO/IARC. World Health Organitation. International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Outdoor pollution. Vol 109, http://monographs.iarc.fr/ENG/Monographs/vol109/mono109.pdf (2016).
McColl, N. et al. European Code against Cancer 4th Edition: Ionising and non-ionising radiation and cancer. Cancer Epidemiol. 39(1), S93–100 (2015).
WHO/IARC. World Health Organitation. International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Radiation. Vol 100 D, http://monographs.iarc.fr/ENG/Monographs/vol100D/mono100D.pdf (2012).
WHO/IARC. World Health Organitation. International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Biological agents. Vol 100 B, http://monographs.iarc.fr/ENG/Monographs/vol100B/mono100B.pdf (2012).
Friis, S. et al. European Code against Cancer 4th Edition: Medical exposures, including hormone therapy, and cancer. Cancer Epidemiol. 39(1), S107–119 (2015).
WHO/IARC. World Health Organitation. International Agency for Research on Cancer. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans. Pharmaceuticals. Vol 100 A, http://monographs.iarc.fr/ENG/Monographs/vol100A/mono100A.pdf (2012).
Whiteman, D. C. & Wilson, L. F. The fractions of cancer attributable to modifiable factors: A global review. Cancer Epidemiol. 44, 203–221 (2016).
Castello, A. et al. Lower Breast Cancer Risk among Women following the World Cancer Research Fund and American Institute for Cancer Research Lifestyle Recommendations: EpiGEICAM Case-Control Study. PLoS One. 10, e0126096 (2015).
Kohler, L. N. et al. Adherence to Diet and Physical Activity Cancer Prevention Guidelines and Cancer Outcomes: A Systematic Review. Cancer Epidemiol Biomarkers Prev. 25, 1018–1028 (2016).
Romaguera, D. et al. Is concordance with World Cancer Research Fund/American Institute for Cancer Research guidelines for cancer prevention related to subsequent risk of cancer? Results from the EPIC study. Am J Clin Nutr. 96, 150–163 (2012).
Whelan, H. K. et al. Alberta’s Tomorrow Project: adherence to cancer prevention recommendations pertaining to diet, physical activity and body size. Public Health Nutr, 1–11 (2017).
Regidor, E., Gutierrez-Fisac, J. L., de los Santos Ichaso, M. & Fernandez, E. Trends in principal cancer risk factors in Spain. Ann Oncol. 21 3, iii37–42 (2010).
Schuz, J. et al. European Code against Cancer 4th Edition: 12 ways to reduce your cancer risk. Cancer Epidemiol. 39(1), S1–10 (2015).
WHO/IARC. World Health Organitation. International Agency for Research on Cancer. European Code Against Cancer, http://cancer-code-europe.iarc.fr/index.php/en/ (2016).
Navarrete-Muñoz, E. M. et al. Reproducibilidad de un cuestionario de frecuencia alimentaría (CFA) para evaluar la dieta en mujeres adultas españolas. XXVIII Reunión Científica de la Sociedad Española de Epidemiología. Gac Sanit. 24(E2), 113 (2010).
Lope, V. et al. Childhood factors associated with mammographic density in adult women. Breast Cancer Res Treat. 130, 965–974 (2011).
Lope, V. et al. Obstetric history and mammographic density: a population-based cross-sectional study in Spain (DDM-Spain). Breast Cancer Res Treat. 132, 1137–1146 (2012).
Pollan, M. et al. Adult weight gain, fat distribution and mammographic density in Spanish pre- and post-menopausal women (DDM-Spain). Breast Cancer Res Treat. 134, 823–838 (2012).
Vioque, J. et al. Reproducibility and validity of a food frequency questionnaire among pregnant women in a Mediterranean area. Nutr J. 12, 26 (2013).
Willett, W. C. et al. Reproducibility and validity of a semiquantitative food frequency questionnaire. Am J Epidemiol. 122, 51–65 (1985).
Alcaraz, M., Lluch, A., Miranda, J., Pereiro, I. & Salas, M. D. [Study of non-participation in the breast cancer screening program in the city of Valencia (Spain)]. Gac Sanit. 16, 230–235 (2002).
Ascunce, N. et al. [Breast cancer screening: characteristics and results of the Spanish programs]. Med Clin (Barc). 141, 13–23 (2013).
MSCBS. Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta Nacional de Salud de España 2011/12, https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuesta2011.htm (2016).
EC. European Commission. Special Eurobarometer 385. Attitudes of Europeans towards tobacco, http://ec.europa.eu/public_opinion/archives/ebs/ebs_385_en.pdf (2012).
Bilal, U. et al. Gender equality and smoking: a theory-driven approach to smoking gender differences in Spain. Tob Control. 25, 295–300 (2016).
Idris, B. I. et al. Higher smoking prevalence in urban compared to non-urban areas: time trends in six European countries. Health Place. 13, 702–712 (2007).
WHO. World Health Organization. Global Health Observatory (GHO) data. Overweight and obesity. (WHO, 2017).
Gallagher, D. et al. How useful is body mass index for comparison of body fatness across age, sex, and ethnic groups? Am J Epidemiol. 143, 228–239 (1996).
Bobrow, K. L. et al. Persistent effects of women’s parity and breastfeeding patterns on their body mass index: results from the Million Women Study. Int J Obes (Lond). 37, 712–717 (2013).
Rodriguez-Caro, A., Vallejo-Torres, L. & Lopez-Valcarcel, B. Unconditional quantile regressions to determine the social gradient of obesity in Spain 1993-2014. Int J Equity Health. 15, 175 (2016).
EC. European Commission. Special Eurobarometer 412. Sport and physical activity, http://ec.europa.eu/public_opinion/archives/ebs/ebs_412_en.pdf (2014).
MSCBS. Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta Nacional de Salud. España 2011/12. Serie Informes monográficos n° 4. Actividad física, descanso y ocio., https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2011/informesMonograficos/Act_fis_desc_ocio.4.pdf (2014).
MAPAMA. Ministerio de Agricultura y Pesca, Alimentación y Medio Ambiente. Panel de Consumo Alimentario. Últimos datos, http://www.mapama.gob.es/es/alimentacion/temas/consumo-y-comercializacion-y-distribucion-alimentaria/panel-de-consumo-alimentario/ultimos-datos/default.aspx (2017).
Martín Cerdeño, V. J. Consumo de platos preparados en los hogares españoles. Distribución y Consumo. 122 (2012).
Martín Cerdeño, V. J. Consumo de carne y productos cárnicos. Evolución y tendencias más recientes. Distribución y Consumo. 111 (2010).
MAPAMA. Ministerio de Agricultura y Pesca, Alimentación y Medio Ambiente. Informe del Consumo de alimentación en España 2015. (2016).
Praud, D. et al. Cancer incidence and mortality attributable to alcohol consumption. Int J Cancer. 138, 1380–1387 (2016).
Schutze, M. et al. Alcohol attributable burden of incidence of cancer in eight European countries based on results from prospective cohort study. BMJ. 342, d1584 (2011).
La Vecchia, C. et al. Trends in alcohol consumption in Europe and their impact on major alcohol-related cancers. Eur J Cancer Prev. 23, 319–322 (2014).
Sordo, L. et al. Estimating average alcohol consumption in the population using multiple sources: the case of Spain. Popul Health Metr. 14, 21 (2016).
MSCBS. Ministerio de Sanidad, Consumo y Bienestar Social. Encuesta Nacional de Salud. España 2011/12. Serie Informes monográficos n° 1. Consumo de alcohol, https://www.mscbs.gob.es/estadEstudios/estadisticas/encuestaNacional/encuestaNac2011/informesMonograficos/ENSE2011_12_MONOGRAFICO_1_ALCOHOL4.pdf (2013).
MSCBS. Ministerio de Sanidad, Consumo y Bienestar Social. Informe anual del Sistema Nacional de Salud 2012. Edición revisada 2015, http://www.mscbs.gob.es/estadEstudios/estadisticas/sisInfSanSNS/tablasEstadisticas/infsns2012.pdf (2015).
Ameye, L., Antoine, C., Paesmans, M., de Azambuja, E. & Rozenberg, S. Menopausal hormone therapy use in 17 European countries during the last decade. Maturitas. 79, 287–291 (2014).
Balade Martinez, L., Montero Corominas, D. & Macias Saint-Gerons, D. [Utilization of hormone replacement therapy in Spain: Trends in the period 2000–2014]. Med Clin (Barc). 147, 287–292 (2016).
Costas, L. et al. Hormonal contraception and postmenopausal hormone therapy in Spain: time trends and patterns of use. Menopause. 22, 1138–1146 (2015).
Acknowledgements
This study was supported by the Spanish Public Health Research Fund (FIS PI060386 & PS09/0790); by the Spanish Ministry of Health, Social Policy and Equality (EC11-273), by the Carlos III Institute of Health (ISCIII) (AESI PI15CIII/00013); by the Spanish Ministry of Economy and Competitiveness, Juan de la Cierva de Incorporación grant (IJCI-2014-20900); by the EPY 1306/06 Collaboration Agreement between Astra-Zeneca and the Carlos III Institute of Health; and a grant from the Spanish Federation of Breast Cancer patients (FECMA EPY 1169/10). The authors wish to thank the participants in the DDM-Spain study for their contribution to breast cancer research.
Author information
Authors and Affiliations
Contributions
Conception and design: M.P., M.J.T., V.L., D.S., C.V., N.A., C.S., P.M., C.P.P., C.S.C., N.A. and B.P.G. Data analysis: M.J.T., V.L., A.C. and M.P. Interpretation of data: M.J.T., V.L., A.C., N.A., B.P.G. and M.P. Drafting of the manuscript: M.J.T., V.L. and M.P. All authors reviewed the manuscript, approved the final draft and decided to submit it for publication.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Toribio, M.J., Lope, V., Castelló, A. et al. Prevalence of healthy lifestyles against cancer in Spanish women. Sci Rep 9, 10638 (2019). https://doi.org/10.1038/s41598-019-47180-x
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-47180-x
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
