
Abstract
The purpose of the present study was to describe the temporal trends in prevalence and management status of hypertension in Korea between 1998 and 2015. Data of adults who were aged 30 years or older were extracted from the Korea National Health and Nutrition Examination Survey, a nationwide representative population-based survey. Hypertension was prevalent in 30.5% of Korean adults. The age and sex standardized prevalence showed little change between 1998 and 2015. The elderly population and men showed higher prevalence. The rates of awareness, treatment, and control showed substantial improvements among hypertensive subjects between 1998 and the time period of 2007‒2009 (awareness, from 23.5 to 66.3%; treatment, from 20.4 to 60.3%; and control, from 4.9 to 42.1%), after which the numbers reached a plateau and no significant changes were observed subsequently (67.3%, 63.6%, and 46.2%, respectively, between 2013 and 2015). The management status remained poor especially among the young population and in men. In conclusion, the hypertension prevalence remained stable at approximately 30% in Korea between 1998 and 2015. While awareness, treatment, and control of hypertension improved remarkably, the young population and particularly men showed a suboptimal management status.
Similar content being viewed by others
Introduction
Hypertension is a leading health risk1. The World Health Organization estimates that approximately 40% of adults have hypertension2. Annually, 9.4 million deaths are attributable to complications from elevated blood pressure (BP)3,4. Elevated BP accounts for 45% of all cardiovascular mortalities, and 51% of stroke-related deaths2.
Studies have reported that the global prevalence of hypertension has continuously risen during recent decades along with the trend of global aging5. Because hypertension is the most important contributing risk factor for disease burden, the importance of adequate prevention, diagnosis, and control of hypertension is emphasized more than ever before. Globally, however, less than half of all individuals with elevated BP are aware of their diagnosis, and less than one third of those under treatment show adequately controlled BP6,7.
The rates of awareness, treatment, and control of hypertension have shown to vary according to the region, sex, income, and educational levels6,8,9,10,11,12. While it is of great importance to recognize the current status in hypertension diagnosis and treatment at the country level, there are limited data published from Korea13,14. In Korea, a national surveillance program called the Korea National Health and Nutrition Examination Survey (KNHANES), is conducted annually since 1998 to assess the health and nutritional status at the national level15. To obtain nationally representative data, the survey includes approximately 10,000 individuals each year, and includes a health interview, health examination, and nutrition survey.
This study aimed to report the temporal trends in the prevalence, awareness, treatment, and control of hypertension in Korea using the nationwide survey data from 1998 to 2015. We analysed the epidemiology among various demographic and socioeconomic subgroups in an attempt to identify methods to improve hypertension management in Korea.
Methods
Ethics committee approval
This study was conducted in accordance with the Declaration of Helsinki, and the protocol was approved by the Seoul National University Hospital Institutional Review Board. Due to the retrospective nature of this study, the requirement of patient’s informed consent was waived.
Data source
KNHANES is a nationwide representative survey that examines the general health and nutritional status of Koreans15. The first three surveys were conducted in 1998, 2001, and 2005. The design of KNHANES was modified from being conducted once every 3 years to every year beginning in 2007 (KNHANES IV includes data from 2007 to 2009, KNHANES V from 2010 to 2012, and KNHANES VI from 2013 to 2015). The number of subjects that were surveyed was approximately 35,000 for each survey during the first three surveys (1998, 2001 and 2005). Subsequently, in 2007, the survey included 5,000 subjects, which then increased to 10,000 per year since 2008. Study subjects were surveyed using a complex, stratified, multistage, cluster sampling. The sample weights are constructed to represent the Korean population by accounting for the complex survey design, survey non-response, and post-stratification. While the KNHANES includes subjects of all age groups (1 year and older), we included individuals who were 30 years or older in this study.
Variables
A health interview, health examination, and nutrition survey are included in the KNHANES. Information on age, sex, income, and education level was obtained using standardized questionnaires during a home interview performed by trained medical personnel. In this study, income levels were categorized into quartiles according to the subject’s yearly household income. Educational status was categorized as no education or primary school graduate (primary), middle school graduate (middle), high school graduate (high), or college or university graduate or above (college/university). Area of residence was classified into urban or rural areas.
Health examination procedures were performed based on standardized protocols by trained medical personnel. All equipment was calibrated periodically. BP was measured three times on the subjects’ right arm using an appropriately sized arm cuff and mercury sphygmomanometer (Baumanometer; WA Baum Co., New York, NY, USA) after the subject rested in a seated position for at least 5 minutes. The final BP value was calculated as the average of the second and third measurements16. Hypertension was defined as systolic BP ≥ 140 mmHg, diastolic BP ≥ 90 mmHg, or use of antihypertensive drugs17. In this study, a subject was considered being aware of hypertension if he/she had a medical diagnosis of hypertension by medical personnel. Treatment rate was calculated by dividing the number of subjects taking antihypertensive medications for more than 20 days per month by the number of subjects with hypertension. Adequate BP control was defined as having an average systolic and diastolic BP of < 140/90 mmHg. Control rate (1) was defined as the proportion of subjects with adequate BP control among those with hypertension. Control rate (2) was defined as the proportion of subjects with adequate BP control among those who were receiving hypertension treatment.
Statistical analysis
Data are presented as mean ± standard error or % (standard error). Sampling weights based on the sample design of each KNHANES were used for all statistical analyses15. Since a complex survey design was used in KNHANES, the rates of hypertension prevalence, awareness, treatment, and control were estimated by weighted means to avoid biased estimates. The variables representing strata, cluster, and weight were included in the raw data. The rates of awareness, treatment, and control of hypertension were then estimated by combining the 3 years from each survey (KNHANES IV, 2007–2009, KNHANES V, 2010–2012, and KNHANES VI, 2013–2015) using the integrated weights. Age standardization was done based on the 2005 Korean population to compare temporal trends, except for hypertension control rate (2) (adequate control of hypertension among subjects who were receiving antihypertensive medications) because the number of subjects in the age group of 30–39 years was less than 20. Statistical analyses were conducted using SPSS Statistics (IBM Corp., Armonk, NY, USA) and R programming version 3.2.4 (http://www.R-project.org; The R Foundation for Statistical Computing, Vienna, Austria).
Results
Characteristics of hypertensive subjects
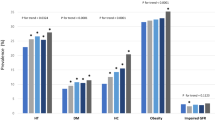
Table 1 shows the profile of subjects with hypertension during the study period. The mean age of hypertensive subjects was 59.8 years in 2013‒2015, which showed a gradual increase from 54.9 years in 1998. Among those with hypertension, 53.1% were men, 21.2% had diabetes; 60.4% dyslipidaemia; and 50.1% were obese. The mean total cholesterol, and LDL cholesterol were 191.2 ± 0.7 and 112.4 ± 0.8, respectively.
Prevalence of hypertension
Prevalence of hypertension was 28.9% in 1998, lowest in 2007 (25.1%), and slightly higher in 2015 (32.0%) (Fig. 1A). This fluctuation seemed to be due to the aging population (Supplementary Fig. 1). When standardized with age distribution, the prevalence of hypertension was grossly stable (Fig. 1B). The prevalence of hypertension in each age group remained unchanged during the study period (Fig. 1C). Hypertension was more prevalent in men than in women (35.1% and 29.1%, respectively, in 2015) (Table 2). While both sexes showed increasingly higher prevalence with older ages, men and women exhibited different patterns (Fig. 1D). For example, among those who were between 30‒39 years, the proportion of hypertensive individuals was markedly higher among men (15.9%) than among women (1.6%). However, the overall rate of hypertension was similar in men and women aged 60‒69 years, and eventually became higher among women than men among those aged 70 years or older. The prevalence did not differ to a large degree according to the area of residence (Supplementary Fig. 2A); however, prevalence tended to be higher in lower income quartiles and lower education levels (Supplementary Fig. 2B,C). Detailed data on the prevalence of hypertension are described in Supplementary Tables 1‒3, which present the prevalence of hypertension from 1998 to 2015 in all subjects and by sex.

Trends in the prevalence of hypertension in Korea: (A) crude prevalence, (B) age-standardized prevalence, (C) prevalence across different age groups, and (D) prevalence according to sex and age in 2013‒2015.
Awareness of hypertension
Awareness of hypertension dramatically improved over the decades—from 23.5% in 1988 to 67.3% in 2013‒2015 (Fig. 2A) (Supplementary Fig. 3A, which shows age-standardized rates). However, the rate reached a plateau in the period of 2007‒2009 and did not significantly change thereafter. Women were more frequently aware of having hypertension than men. When stratified into age groups, the awareness rate showed a wide variation: >80% among those aged 60 years or older, 61.4% among those aged 50‒59 years, 43.9% among those aged 40‒49 years, and 20.2% among those aged 30‒39 years (Fig. 2B). This pattern was similar between men and women (Supplementary Tables 4‒6). The rate of awareness did not differ significantly between urban and rural areas, or among income quartiles (Supplementary Fig. 3B,C); no consistent gradient according to the education levels was observed (Supplementary Fig. 3D).

Trends in the awareness of hypertension in Korea: (A) overall awareness and (B) awareness across different age groups.
Treatment of hypertension
The rate of hypertension treatment had a similar pattern as the awareness rate. While 20.4% of subjects with hypertension received treatment in 2006, the number went up to 63.6% in 2013‒2015 (Fig. 3A). Treatment rate plateaued in the period of 2007‒2009, with no significant improvement thereafter. The pattern of the rate of treatment in each age group was similar to that observed for awareness rate (Fig. 3B). There were small gaps between the awareness and treatment rates, although these gaps tended to be greater in younger age groups (Supplementary Tables 7‒9). No significant variations were found according to the residence, income, and education (Supplementary Fig. 4).

Trends in the treatment of hypertension in Korea: (A) overall treatment and (B) treatment across different age groups.
Control of hypertension
Among hypertensive patients, adequately controlled BP (control rate [1]) markedly improved from 1998 (4.9%) to the period of 2013‒2015 (46.2%) (Fig. 4A). The rate greatly varied according to the subjects’ age — approximately 60% among elderly compared to <10% among 30‒39-year-olds (see Fig. 4B) (Supplementary Tables 10‒12).

Trends in the control of hypertension in Korea. Control (1) is the rate of control among subjects with hypertension: (A) overall control and (B) control across different age groups. Control (2) is the rate of control among subjects with hypertension who were receiving treatment: (C) overall control and (D) control across different age groups.
Among hypertensive patients who were receiving treatment (control rate [2]), 72.0% had an adequate level of BP control compared to 23.8% in 1998 (Fig. 4C). However, different from the prevalence, awareness, treatment, and control (1) rates, as described above, control rate (2) showed little variation among different age groups and between sexes (Fig. 4D) (Supplementary Tables 13‒15). The subjects’ other socioeconomic factors did not significantly affect the control rate (Supplementary Figs 5 and 6).
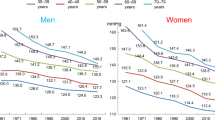
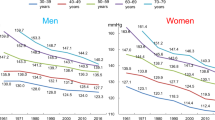
Overall, the improvement in detection and management of hypertension contributed to observed decrease in BP in the general Korean population: 127/79 mmHg in 1998, to 118/76 mmHg in 2013‒2015 (Fig. 5). This trend was also consistent between sexes and among the age groups (Supplementary Fig. 7). The absolute degree of reduction was greater among the aged population and in women.

Temporal trends of mean blood pressure in the general Korean population.
Discussion
In this study, we found that as of 2015, 30.5% of Koreans had hypertension. Among hypertensive subjects, 67.3% were aware of their diagnosis, 63.6% received treatment, and 46.2% had adequately controlled BP. The awareness, treatment, and control rates significantly improved since 1998, when the first KNHANES survey was conducted. However, they reached a plateau in 2007‒2009, and no significant changes were detected thereafter. We also found that there is still room for improvement among people with hypertension who are young and in hypertensive men, as they showed the lowest levels of awareness, treatment, and control.
This study showed that the prevalence of hypertension in Korea remained grossly unchanged from 1998 to 2015. The crude prevalence showed modest fluctuations, but the age-adjusted prevalence was stationary during the study period. Male sex and old age were associated with higher prevalence of hypertension, while there were little disparities according to area of residence, income level, and education. Previous studies have reported wide variations in the prevalence of hypertension across geographic regions (Supplementary Table 16)6,8,9,10,11,12. The prevalence in Korea shown in this study was among the lowest and was similar to that in the United States8,9. The prevalence was lower than the rate reported in Japan, which shares a similar ethnic background, geography, and lifestyle as Korea10,18. However, when split into age and sex subgroups, both Korea and Japan displayed a similar prevalence of hypertension. As the Korean population is rapidly aging, the prevalence of hypertension is expected to constantly increase in the future.
There was a dramatic improvement in the identification and control of hypertension during the study period. The awareness and treatment rates increased more than three-fold, and the control rate increased approximately ten-fold between 1998 and the period of 2013‒2015. The overall control status observed in Korea was among the best globally (Supplementary Table 16). Several changes in the Korean society may have influenced this phenomenon. First, daily sodium consumption has decreased; the mean sodium intake is relatively high in Korea compared to global levels19. However, the amount was reported to be decreasing among the Korean population20, and this study also confirmed that sodium consumption was decreasing among those with hypertension. Second, there has been an increase in nationwide efforts towards early detection of hypertension. For example, subscribers of the National Health Insurance system, which covers 97% of the Korean population, are entitled to receive a standardized medical examination every 2 years since 201121. This free service includes general physical examination and laboratory tests, such as fasting glucose and blood lipid levels. If a recipient’s BP is high, he/she is recommended to visit a primary physician for further evaluation. In 2015, over 60% of Korean adults received the free screening service. In addition, the government, in conjunction with professional societies, is implementing various measures for the primary prevention of chronic diseases. Third, there have been advances in healthcare policy. For example, a pharmaceutical policy reform which was enforced in 2000, mandated the separation of drug prescription and dispensing22. While the policy aimed at reducing the overuse and misuse of drugs, it inevitably increased medical service consumers’ visits to physicians. These changes in practice patterns may have contributed to the improvement in hypertension awareness and treatment.
Recent data demonstrated a significant decrease in mortality from cardiovascular diseases in Korea23. A more dramatic reduction was observed in cerebrovascular disease incidence and mortality24. This study indicated that the mean BP of the general Korean population declined by 8.6/3.7 mmHg over the last 18 years. There is strong evidence suggesting that a BP reduction of 10/5 mmHg is associated with an 18% reduction in cardiovascular mortality25,26. Therefore, it may be assumed that the improvement in hypertension management was one of the major contributors to the recent reductions in cardiovascular mortality.
This study revealed low rates of detection and poor control of hypertension among Korean individuals who are young and in men, which is a common observation globally6,8,9,10,11,12, though the gaps are smaller in several countries such as the United States, Japan, and Germany8,18,27. Of note, the countries listed above also showed better awareness and management of hypertension than in Korea, which provides an important insight. Early detection should be encouraged, and antihypertensive treatment should be commenced as soon as clinically indicated for young Korean men. These early interventions might also assist in breaking through the stagnation of awareness, treatment, and control rates that have occurred since 2007‒2009.
Measures to improve hypertension management in individuals who are young and male are required. Previous studies have shown that infrequent healthcare visits are an important risk factor for low awareness and management28. A study in Korea also showed that only a small proportion of young patients (in their 30 s and 40 s) with hypertension received BP measurements during previous years29. Self-measured BP at home has shown to be an effective measure to improve adherence to treatment30. In addition, there are other methods that have shown efficacy, such as simplification of the drug regimen and home-based digital programs31,32.
American College of Cardiology (ACC) and American Heart Association (AHA) recently published a new guideline for hypertension, which suggested more aggressive diagnostic and treatment approaches than before33. According to these, hypertension was defined as a BP ≥ 130/80 mmHg and hypertensive patients were recommended to maintain their BP under <130/80 mmHg. However, European hypertension guidelines as well as Korean ones have maintained the previous cut-off value of 140/90 mmHg34. In a previous study, we demonstrated that the prevalence of hypertension would increase from 30.4% to 49.2% when the 2017 ACC/AHA guidelines are directly applied in Korea35.
The major strength of this study was the use of the nationally representative KNHANES data. It enabled reliable estimation of the trends of hypertension in Korea over 18 years. The limitations of this study also need to be considered. First, the KNHANES is designed as a cross-sectional study and longitudinal follow-up is limited36. Second, there have been modifications in the questionnaires from KNHANES I to VI; thus, there were minor variations in the definitions of hypertension across the study period. Third, BP measurements were performed during a single visit. Repeated visits or ambulatory measurements have shown to minimize the chance of misclassification37. Lastly, the Korean Society of Hypertension recently published the Korea Hypertension Fact Sheet 2018 in Korean38. Some of the present study’s results are similar to those of the Fact Sheet.
In conclusion, this study reported the trends in hypertension prevalence, awareness, treatment, and control in Korea. Among Korean adults aged 30 years or older, 30.4% had hypertension. While the prevalence was largely unchanged, the awareness, treatment, and control rates drastically improved from 1998 to 2007, at which time the rates plateaued and remained constant subsequently. Strategies need to be implemented to increase hypertension detection, management, and control among young people and men in Korea.
References
GBD 2016 Risk Factors Collaborators. Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet 390, 1345–1422, https://doi.org/10.1016/S0140-6736(17)32366-8 (2017).
World Health Organization. A global brief on Hypertension (2013).
World Health Organization. Global status report on noncommunicable diseases 2010 (2011).
Ivers, N. et al. Audit and feedback: effects on professional practice and healthcare outcomes. Cochrane Database Syst Rev, CD000259, https://doi.org/10.1002/14651858.CD000259.pub3 (2012).
Forouzanfar, M. H. et al. Global Burden of Hypertension and Systolic Blood Pressure of at Least 110 to 115 mm Hg, 1990–2015. JAMA 317, 165–182, https://doi.org/10.1001/jama.2016.19043 (2017).
Chow, C. K. et al. Prevalence, awareness, treatment, and control of hypertension in rural and urban communities in high-, middle-, and low-income countries. JAMA 310, 959–968, https://doi.org/10.1001/jama.2013.184182 (2013).
Olsen, M. H. et al. A call to action and a lifecourse strategy to address the global burden of raised blood pressure on current and future generations: the Lancet Commission on hypertension. Lancet 388, 2665–2712, https://doi.org/10.1016/S0140-6736(16)31134-5 (2016).
Guo, F., He, D., Zhang, W. & Walton, R. G. Trends in prevalence, awareness, management, and control of hypertension among United States adults, 1999 to 2010. Journal of the American College of Cardiology 60, 599–606, https://doi.org/10.1016/j.jacc.2012.04.026 (2012).
Zhang, Y. & Moran, A. E. Trends in the Prevalence, Awareness, Treatment, and Control of Hypertension Among Young Adults in the United States, 1999 to 2014. Hypertension 70, 736–742, https://doi.org/10.1161/HYPERTENSIONAHA.117.09801 (2017).
Report for a Health and Labor Sciences Research Grant. Comprehensive research on life-style related diseases including cardiovascular diseases and diabetes mellitus [H22-Jyunkankitou-Seisyu-Sitei-017], https://hs-web.shiga-med.ac.jp/Nippondata/NIPPONDATA2010/research/Data%20table/3_ketsuatsu.pdf (2013).
Li, W. et al. Hypertension prevalence, awareness, treatment, and control in 115 rural and urban communities involving 47 000 people from China. J Hypertens 34, 39–46, https://doi.org/10.1097/HJH.0000000000000745 (2016).
Roy, A. et al. Changes in hypertension prevalence, awareness, treatment and control rates over 20 years in National Capital Region of India: results from a repeat cross-sectional study. BMJ open 7, e015639, https://doi.org/10.1136/bmjopen-2016-015639 (2017).
Adler, A. J. et al. Reducing Cardiovascular Mortality Through Prevention and Management of Raised Blood Pressure: A World Heart Federation Roadmap. Glob Heart 10, 111–122, https://doi.org/10.1016/j.gheart.2015.04.006 (2015).
Park, C. S. et al. The Association between Parameters of Socioeconomic Status and Hypertension in Korea: the Korean Genome and Epidemiology Study. J Korean Med Sci 31, 1922–1928, https://doi.org/10.3346/jkms.2016.31.12.1922 (2016).
Kweon, S. et al. Data resource profile: the Korea National Health and Nutrition Examination Survey (KNHANES). Int J Epidemiol 43, 69–77, https://doi.org/10.1093/ije/dyt228 (2014).
Korean National Health And Nutrition Survey, https://knhanes.cdc.go.kr/knhanes/eng/index.do (2017).
Kim, S. et al. Relation between secondhand smoke exposure and cardiovascular risk factors in never smokers. J Hypertens 35, 1976–1982, https://doi.org/10.1097/HJH.0000000000001426 (2017).
Miura, K., Nagai, M. & Ohkubo, T. Epidemiology of hypertension in Japan: where are we now? Circ J 77, 2226–2231 (2013).
Hong, J. W., Noh, J. H. & Kim, D. J. Factors Associated With High Sodium Intake Based on Estimated 24-Hour Urinary Sodium Excretion: The 2009–2011 Korea National Health and Nutrition Examination Survey. Medicine (Baltimore) 95, e2864, https://doi.org/10.1097/MD.0000000000002864 (2016).
Kim, H. J. & Oh, K. Methodological issues in estimating sodium intake in the Korea National Health and Nutrition Examination Survey. Epidemiol Health 36, e2014033, https://doi.org/10.4178/epih/e2014033 (2014).
Kim, Y. S. & Lee, J. A. National health examination expansion policy. J Korean Med Assoc 60, 104–107 (2017).
Kwon, S. Pharmaceutical reform and physician strikes in Korea: separation of drug prescribing and dispensing. Soc Sci Med 57, 529–538 (2003).
Lee, S. W., Kim, H. C., Lee, H. S. & Suh, I. Thirty-Year Trends in Mortality from Cerebrovascular Diseases in Korea. Korean Circ J 46, 507–514, https://doi.org/10.4070/kcj.2016.46.4.507 (2016).
Lee, S. W., Kim, H. C., Lee, H. S. & Suh, I. Thirty-year trends in mortality from cardiovascular diseases in Korea. Korean Circ J 45, 202–209, https://doi.org/10.4070/kcj.2015.45.3.202 (2015).
Thomopoulos, C., Parati, G. & Zanchetti, A. Effects of blood pressure lowering on outcome incidence in hypertension. 1. Overview, meta-analyses, and meta-regression analyses of randomized trials. J Hypertens 32, 2285–2295, https://doi.org/10.1097/HJH.0000000000000378 (2014).
Blood Pressure Lowering Treatment Trialists, C. Blood pressure-lowering treatment based on cardiovascular risk: a meta-analysis of individual patient data. Lancet 384, 591–598, https://doi.org/10.1016/S0140-6736(14)61212-5 (2014).
Sarganas, G. & Neuhauser, H. K. The persisting gender gap in hypertension management and control in Germany: 1998 and 2008–2011. Hypertens Res 39, 457–466, https://doi.org/10.1038/hr.2016.5 (2016).
Ostchega, Y., Hughes, J. P., Wright, J. D., McDowell, M. A. & Louis, T. Are demographic characteristics, health care access and utilization, and comorbid conditions associated with hypertension among US adults? Am J Hypertens 21, 159–165, https://doi.org/10.1038/ajh.2007.32 (2008).
Oh, M. U., Choi, M., Kim, G. S. & Sunwoo, S. Association Between Hypertension Management and Blood Pressure Screening Among Adults in 30s and 40s. Korean J Health Promot 13, 61–68 (2013).
Parati, G. et al. European Society of Hypertension practice guidelines for home blood pressure monitoring. J Hum Hypertens 24, 779–785, https://doi.org/10.1038/jhh.2010.54 (2010).
Milani, R. V., Lavie, C. J., Bober, R. M., Milani, A. R. & Ventura, H. O. Improving Hypertension Control and Patient Engagement Using Digital Tools. Am J Med 130, 14–20, https://doi.org/10.1016/j.amjmed.2016.07.029 (2017).
Claxton, A. J., Cramer, J. & Pierce, C. A systematic review of the associations between dose regimens and medication compliance. Clin Ther 23, 1296–1310 (2001).
Whelton, P. K. et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation 138, e426–e483, https://doi.org/10.1161/CIR.0000000000000597 (2018).
Williams, B. et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J 39, 3021–3104, https://doi.org/10.1093/eurheartj/ehy339 (2018).
Lee, J. H. et al. Blood Pressure Control and Cardiovascular Outcomes: Real-world Implications of the 2017 ACC/AHA Hypertension Guideline. Sci Rep 8, 13155, https://doi.org/10.1038/s41598-018-31549-5 (2018).
Kim, Y. The Korea National Health and Nutrition Examination Survey (KNHANES): current status and challenges. Epidemiol Health 36, e2014002, https://doi.org/10.4178/epih/e2014002 (2014).
Melgarejo, J. D. et al. Prevalence, Treatment, and Control Rates of Conventional and Ambulatory Hypertension Across 10 Populations in 3 Continents. Hypertension 70, 50–58, https://doi.org/10.1161/HYPERTENSIONAHA.117.09188 (2017).
Korean Society of Hypertension. Korea Hypertension Fact Sheet 2018, http://www.koreanhypertension.org/reference/guide?mode=read&idno=4166 (2018).
Acknowledgements
We thank Ms. Moon Ju Kim for data collection and statistical analysis.
Author information
Authors and Affiliations
Contributions
S.H. Kang, S.S. Hwang, H.Y. Lee, and C.H. Kim conceived the study; S.H. Kang, S.H. Kim, J.H. Cho analysed the data; S.H. Kang and C.H. Kim prepared the manuscript; J.H. Cho, C.H. Yoon, S.S. Hwang, H.Y. Lee, T.J. Youn, and I.H. Chae critically reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kang, SH., Kim, SH., Cho, J.H. et al. Prevalence, Awareness, Treatment, and Control of Hypertension in Korea. Sci Rep 9, 10970 (2019). https://doi.org/10.1038/s41598-019-46965-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-46965-4
This article is cited by
-
Association between toothbrushing and cardiovascular risk factors: a cross-sectional study using Korean National Health and Nutrition Examination Survey 2015–2017
BMC Oral Health (2024)
-
History and evolution of blood pressure measurement
Clinical Hypertension (2024)
-
Incidence rates of retinal vascular occlusive diseases from 2011 to 2020 in South Korea: a nationwide cohort study
BMC Ophthalmology (2024)
-
Epidemiology and comorbidities in idiopathic pulmonary fibrosis: a nationwide cohort study
BMC Pulmonary Medicine (2023)
-
Trends in hypertension prevalence, awareness, treatment, and control in South Korea, 1998–2021: a nationally representative serial study
Scientific Reports (2023)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
