
Abstract
The aim of this study was to determine and evaluate the association between potassium intake and hearing thresholds in the Korean adult population. Data from the Korean National Health and Nutrition Examination Survey were analyzed. Participants were divided into tertiles on the basis of their potassium intake as follows: low, middle, and high. Pure-tone audiometry was performed using an automated audiometer. We calculated as the average threshold at the low-frequency pure-tone average (0.5 and 1 kHz), mid-frequency pure-tone average (2 and 3 kHz), and high-frequency pure-tone average (4 and 6 kHz). The average hearing threshold (AHT) was calculated as the pure-tone average of the thresholds at 0.5~3 kHz. Hearing loss (HL) was defined as an AHT of >40 dB in the better ear. There were 1975 participants each in the low, middle, and high tertile groups. The four different average hearing thresholds significantly decreased with an increase in the potassium intake tertile. Multivariate analysis revealed that the four different average hearing thresholds were significantly lower in the high tertile group than in the other two groups. In addition, univariate and multivariate linear regression analyses showed that the potassium intake level was inversely associated with each of the four different average hearing thresholds. Analyses of participants matched based on propensity scores and participants not matched based on propensity scores yielded similar results. The results of this study suggest that high potassium intake levels were associated with a lower prevalence of HL and lower hearing thresholds in the Korean adult population.
Similar content being viewed by others

Introduction
Hearing loss (HL) is one of the most common public health problems in the world1. With an increase in the life expectancy of the world’s population, many researchers believe that the worldwide prevalence of HL will concurrently increase2. WHO revealed that HL affects approximately 5.3% of the world’s population1. In particular, a report from New Zealand estimated that the prevalence of HL was approximately 5.08% in 2011, which would increase to 7.02% in 20612. Several studies suggest that various factors, including direct vascular injuries, noise, genetic factors, and environmental exposure, are associated with the development of HL3,4,5,6,7. Although some risk factors and interventions have been identified, further research is needed to understand the pathophysiology of HL and determine appropriate prevention strategies.
High-potassium diets are associated with a decrease in or the prevention of various cardiovascular complications8. Haijar et al. showed that systolic blood pressure is negatively correlated with the amount of potassium intake9. A review of 11 cohort studies demonstrated a negative association between potassium intake and strokes10. Considering these benefits, the World Health Organization (WHO) recommends a high-potassium diet (at least 3510 mg/day)11. Although the benefits of a high-potassium diet have been investigated in many recent studies, its association with various other diseases remains to be elucidated in ongoing research.
Microvascular injury to the cochlea is one of the primary causes of HL12. Hwang et al. showed that mice with diet-induced obesity had blood vessels with a smaller diameter and thicker walls in the stria vascularis, and this led to hearing impairment13. Brown et al. investigated the association between a decrease in cochlear vascular reactivity and hearing impairment in old mice14. High potassium intake is associated with a decrease in blood pressure through natriuresis and direct vasodilating effects8,15,16. Previous epidemiological studies found an inverse relationship between potassium intake levels and the development of hypertension (HTN) and stroke17,18. Previous studies showed that various cardiovascular diseases are associated with HL through microvascular injury to the cochlea19,20,21,22. As high-potassium diets are negatively associated with cardiovascular complications, they may be associated with a decrease in microvascular injury to the cochlea and, consequently, a decrease in the incidence of HL. In addition, previous studies demonstrated that a high-potassium diet is associated with an increase in serum aldosterone levels, which prevents hearing impairment through upregulation of Na+-K+ ATPase and Na+-K+-2Cl− cotransporter (NKCC1)23,24,25,26,27. From the above perspectives, we conducted the present study to determine and evaluate the association between potassium intake and hearing thresholds in the Korean adult population.
Materials and Methods
Study population
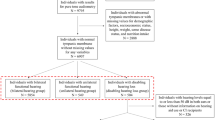
Data from the Korean National Health and Nutrition Examination Survey (KNHANES) 2009–2013 were analyzed for this retrospective, cross-sectional study. The KNHANES is a nationwide, multi-stage, stratified survey of a representative sample of the South Korean population conducted by the Korea Centers for Disease Control and Prevention. There were 23 121 participants (n) aged ≥40 years. From these, 17 096 participants were excluded because of missing clinical data and 100 because of an extremely low (<500 kcal/day) or high (>5000 kcal/day) daily energy intake. Finally, 5925 participants were included in this study, which was approved by the Institutional Review Board of Yeungnam University Hospital (IRB number: 2016-10-056). The board waived the need for informed consent because the subjects’ records and information were anonymized and de-identified prior to the analysis. The study was conducted in accordance with the principles that have their origin in the Declaration of Helsinki.
Study variables
Information collected from the participants during the health examination included the following types of clinical and laboratory data: age, sex, presence of diabetes mellitus (DM), presence of HTN, household income (thousand won/month), smoking habits, alcohol intake, education level, physical activity, estimated glomerular filtration rate (eGFR; mL/min/1.73 m2), exposure to explosive noise, exposure to occupational noise, dietary measurements, and hearing thresholds.
DM was defined as a self-reported history of a DM diagnosis, the use of hypoglycemic drugs, a fasting glucose level of ≥126 mg/dL, or an HbA1c of ≥6.5%. HTN was defined as a systolic blood pressure of ≥140 mmHg, a diastolic blood pressure of ≥90 mmHg, a self-reported history of HTN, or the use of anti-HTN drugs. Smokers were classified as current smokers, ex-smokers, or non-smokers. Non-smokers were individuals who had consumed <100 cigarettes in their lifetime, ex-smokers were individuals who had consumed ≥100 cigarettes in their lifetime and had ceased smoking ≥1 year before the survey, and current smokers were individuals who had consumed ≥100 cigarettes in their lifetime and had ceased smoking <1 year before the survey. Alcohol intake was defined by the Korean version of standard drinking, which is based on the WHO classification system28,29. We classified alcohol intake into the following categories: abstinence (no alcohol consumption during the 12 months prior to the evaluation), moderate consumption (women, 0.1–19.99 g of pure alcohol/day; men, 0.1–39.99 g of pure alcohol/day), and heavy consumption (women, ≥20 g of pure alcohol/day; men, ≥40 g of pure alcohol/day). Education levels were divided into the following categories: less than high school, high school, and college or more.
Moderate-intensity activities were defined as activities such as job-related activities and light sports such as slow swimming, double tennis, volleyball, badminton, and table tennis. High-intensity activities were defined as activities such as job-related activities and heavy sports such as running, mountain climbing, fast bicycling, fast swimming, soccer, basketball, rope jumping, squash, and single tennis. Regular exercise was defined as engaging in moderate-intensity activity for >30 min/day for 5 days a week or high-intensity activity for >20 min/day for 3 days a week30. Physical activity was defined as the performance of regular exercise during leisure time in the 3 months before the evaluation. eGFR was calculated using the Chronic Kidney Disease Epidemiology Collaboration formula31.
Dietary assessments
Dietary assessments were performed by trained staff using a 24-h recall method. A previous study showed a strong correlation between the single 24-h recall method and the multi-step process for each 24-h recall method (Pearson’s correlation coefficients for nutrients was 0.624–0.999)32. The total intakes of calories (kcal/day), proteins (g/day), carbohydrates (g/day), fats (g/day), sodium (mg/day), potassium (mg/day), vitamin A (mg/day), carotene (mg/day), retinol (mg/day), thiamine (mg/day), riboflavin (mg/day), niacin (mg/day), and vitamin C (mg/day) were calculated using the nutrient concentrations listed in the Korean Food Composition Table33. The total calorie and protein intakes were compared with the recommended amounts for Koreans and were calculated as the proportion of the age- and sex-matched recommended intake for individuals in Korea (%)34,35. For example, the calorie intake (%), calculated as the total intake calories/age and sex matched, the recommended total intake calories. Fat and carbohydrate intakes (%) were measured as the distribution of intake calories among the total intake calories (fat intake calories/total intake calories and carbohydrates intake calorie/total intake calories)35. The total sodium and potassium intakes were positively associated with the total calorie intake (r = 0.538 for sodium and r = 0.655 for potassium). Therefore, the sodium and potassium intakes (mg/1000 kcal) were calculated as intakes adjusted for the total calorie intake using the residual method36. Subsequently, participants were divided into tertiles on the basis of their potassium intake: low (0–1338 mg/1000 kcal), middle (1339–1761 mg/1000 kcal), and high (1762–10384 mg/1000 kcal). Serum levels of 25-hydroxy-vitamin D3 (vitamin D) were measured by a radioimmunoassay (25-hydroxy-vitamin D125 I RIA Kit; DiaSorin, Stillwater, MN, USA) using the 1470 Wizard Gamma Counter (PerkinElmer, Turku, Finland).
Assessment of hearing thresholds
Histories of exposure to explosive and occupational noise were classified as positive or negative, as previously described6. An explosive noise was defined as a sudden loud noise, such as an explosion or gunshot. Exposure to occupational noise was positive if participants had worked in a location with loud machinery for ≥3 months. Exposure to loud noise was positive if participants needed to raise their voice to have a conversation. The hearing thresholds were measured using an automated audiometer at 0.5, 1, 2, 3, 4, and 6 kHz. For both ears of each subject, the threshold values at 0.5 and 1 kHz were averaged to obtain the low-frequency pure-tone average (Low-Freq), the values at 2 and 3 kHz were averaged to obtain the mid-frequency pure-tone average (Mid-Freq), and the values at 4 and 6 kHz were averaged to obtain the high-frequency pure-tone average (High-Freq). In the present study, the average hearing threshold (AHT) was calculated as the pure-tone average of the thresholds at 0.5, 1, 2, and 3 kHz. HL was defined as an AHT of >40 dB in the better ear.
Statistical analyses
Data were analyzed using SPSS version 21 (SPSS, Chicago, IL, USA). Categorical variables are expressed as numbers and percentages and continuous variables are expressed as means ± standard deviations or standard errors. The distribution of continuous variables was evaluated using the Kolmogorov-Smirnov test. Pearson’s χ2 test or Fisher’s exact test was used to analyze categorical variables. For continuous variables, means were compared using t -tests or one-way analysis of variance, followed by post-hoc Tukey comparisons. Linear regression analysis was performed to assess the independent predictors of hearing thresholds. Logistic regression analyses were used to estimate the odds ratios and 95% confidence intervals (CIs), which were used to determine the relationship between HL and potassium intake levels.
Multivariate analysis was adjusted for age, sex, DM, HTN, household income, smoking habits, alcohol intake, education level, physical activity, eGFR, calorie intake, protein intake, fat intake, carbohydrate intake, sodium intake, occupational noise exposure, explosive noise exposure, vitamin A intake, carotene intake, retinol intake, thiamine intake, riboflavin intake, niacin intake, vitamin C intake, and serum vitamin D levels. Multivariate analyses were performed using analysis of covariance, multiple linear regression, or multiple logistic regression to determine the independent predictors of hearing thresholds or HL.
Because of substantial differences in the baseline characteristics of the participants in the tertile groups, propensity analysis was performed to minimize bias. To balance the baseline characteristics between the high tertile group and middle and low tertile groups (collectively, non-high group), we estimated propensity scores using logistic regression models and the following variables: age, sex, DM, HTN, household income, smoking habits, alcohol intake, education level, physical activity, eGFR, total energy, protein intake, fat intake, carbohydrate intake, sodium intake, occupational noise exposure, and explosive noise exposure. Participants in the high tertile group were matched with participants in the non-high group using 1:1 nearest neighbor matching without replacement and with a matching tolerance (caliper) of 0.2; the nearest neighborhood matching was based on propensity scores. Before the groups were matched, the standardized mean difference was 0.860, and after matching, the standardized mean difference was 0.094. Before matching, the mean propensity scores for participants in the high tertile group and non-high group were 0.4329 and 0.2836, respectively. After matching, the mean scores were 0.4012 and 0.3848, respectively. A P-value of <0.05 was considered statistically significant.
Results
Clinical characteristics of the participants
The study population predominantly comprised women (57.1%; Table 1). The mean age was higher for men than for women, and the proportion of participants with DM or HTN was higher among the men than among the women. All nutrient intakes except the sodium intake were higher in men than in women. There were 1975 participants each in the low, middle, and high tertile groups (Table 2). The mean potassium intake in the low, middle, and high tertile groups was 1085 ± 189, 1539 ± 121, and 2262 ± 606 mg/1000 kcal, respectively. The proportion of participants with HTN and that of participants with DM were higher in the low tertile group than in the high tertile group. With an increase in the potassium intake tertile, the rates of HTN, heavy alcohol consumption, occupational noise exposure, and explosive noise exposure and the proportions of men and current smokers decreased, while the carbohydrate intake, sodium intake, and proportion of participants who exercised regularly increased. The mean age and the proportion of participants with DM were the highest in the low tertile group. The household income was the highest in high tertile group, while the education level, eGFR, protein intake, and fat intake were the lowest in the low tertile group. There were significant differences in most baseline characteristics among the tertile groups.
Association between potassium intake tertile and hearing thresholds
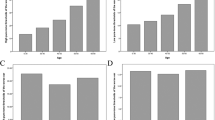
In the low, middle, and high tertile groups, Low-Freq (mean ± standard error) was 20.2 ± 0.4, 17.9 ± 0.3, and 16.6 ± 0.3 dB, respectively (P < 0.001 for trend, Fig. 1); Mid-Freq was 26.9 ± 0.4, 23.4 ± 0.4, and 21.9 ± 0.4 dB, respectively (P < 0.001 for trend); High-Freq was 40.9 ± 0.5, 36.9 ± 0.5, and 34.7 ± 0.5 dB, respectively (P < 0.001 for trend); and AHT was 23.6 ± 0.4, 20.6 ± 0.3, and 14.3 ± 0.3 dB, respectively (P < 0.001 for trend). The four different average hearing thresholds significantly decreased with an increase in the potassium intake tertile. Multivariate analysis revealed that the four different average hearing thresholds were significantly lower in the high tertile group than in the low and middle tertile groups. In addition, univariate and multivariate linear regression analyses showed that the potassium intake level was inversely associated with each of the four different average hearing thresholds (Table 3).

Hearing thresholds according to potassium intake tertiles. Multivariate analysis was adjusted for age, sex, diabetes mellitus, hypertension, household income, smoking habits, alcohol intake, education level, physical activity, eGFR, calorie intake, protein intake, fat intake, carbohydrate intake, sodium intake, occupational noise exposure, explosive noise exposure, vitamin A intake, carotene intake, retinol intake, thiamine intake, riboflavin intake, niacin intake, vitamin C intake, and serum vitamin D levels (P < 0.001 for trends in all analyses). The data are expressed as mean and standard error values. *P < 0.05 versus the low tertile group. #P < 0.05 versus the middle tertile group. Abbreviations: AHT, average hearing threshold; Low-Freq, low frequency threshold; Mid-Freq, middle frequency threshold; High-Freq, high frequency threshold; eGFR, estimated glomerular filtration rate.
Association between potassium intake levels and HL
The prevalence of HL in the low, middle, and high tertile groups was 15.3% (n = 302), 11.1% (n = 220), and 7.8% (n = 155), respectively (P < 0.001). Univariate logistic regression showed that, compared with those in the high tertile group, participants in the low tertile group exhibited a 2.120-fold (95% CI, 1.727–2.601; P < 0.001) higher odds for HL, while those in the middle tertile group exhibited a 1.472-fold (1.186–1.826; P < 0.001) higher odds for HL (Table 4). Multivariate analysis revealed that, compared with those in the high tertile group, participants in the low tertile group exhibited a 1.642-fold (1.152–2.340; P = 0.006) higher odds for HL, while those in the middle tertile group exhibited a 1.469-fold (1.080–1.998; P = 0.014) higher odds for HL. There was no significant difference in the odds ratio between the middle and low tertile groups.
Analyses of participants matched based on propensity scores
For propensity score matching, we divided all participants into high tertile and non-high groups. In total, 1755 pairs were selected from the 3950 participants in the non-high group. The estimated distribution of propensity scores was similar after matching, and no significant differences in participant characteristics were observed between the high tertile and non-high groups (Fig. 2 and Table 5). Low-Freq in the non-high and high tertile groups was 18.8 ± 15.0 and 16.5 ± 13.1 dB, respectively (P < 0.001), Mid-Freq was 24.0 ± 18.5 and 21.9 ± 17.1 dB, respectively (P = 0.001), High-Freq was 36.9 ± 22.6 and 34.7 ± 21.2 dB, respectively (P = 0.003), and AHT was 21.4 ± 15.9 and 19.2 ± 14.2 dB, respectively (P < 0.001). The prevalence of HL in the non-high and the high tertile groups was 12.5% (n = 220) and 7.8% (n = 137), respectively (P < 0.001). Univariate logistic regression showed that the participants in the non-high group exhibited a 1.693-fold (95% CI, 1.352–2.119; P < 0.001) higher odds of HL compared with those in the high tertile group. Analyses of participants matched based on propensity scores and participants not matched based on propensity scores yielded similar results.

Distribution of propensity scores before and after matching. The distribution of propensity scores before matching differed between the high tertile group and the middle and low tertile groups (collectively, non-high group), although there was no difference after matching.
Subgroup analyses by sex, DM, and HTN
There were significant differences in baseline characteristics between men and women (Table 1). We performed subgroup analyses according to sex, DM, and HTN. The participants in each group (men and women, DM and non-DM, HTN and non-HTN) were divided into three tertiles on the basis of their potassium intake. The number of men in the low, middle, and high tertile groups was 847, 848, and 847, respectively. The four different average hearing thresholds were significantly higher in the low tertile group than in the other tertile groups (Fig. S1). The prevalence of HL in the low, middle, and high tertile groups was 19.0% (n = 161), 14.2% (n = 120), and 11.8% (n = 100), respectively (P < 0.001). The number of women in the low, middle, and high tertile groups was 1127, 1128, and 1128, respectively. Mid-Freq and High-Freq were significantly higher in the low tertile group than in the other tertile groups (Fig. S2). Low-Freq and AHT significantly decreased with an increase in the potassium intake tertile. The prevalence of HL in the low, middle, and high tertile groups was 12.2% (n = 138), 7.9% (n = 89), and 6.1% (n = 69), respectively (P < 0.001). In addition, univariate linear regression analyses showed that the potassium intake level was inversely associated with each of the four different average hearing thresholds in women and Low-Freq, Mid-Freq, and AHT in men (Table S1).
The number of non-DM participants in the low, middle, and high tertile groups was 1651, 1652, and 1652, respectively. The four different average hearing thresholds significantly decreased with an increase in the potassium intake tertile (Fig. S2). The prevalence of HL in the low, middle, and high tertile groups was 13.6% (n = 224), 10.0% (n = 165), and 6.8% (n = 113), respectively (P < 0.001). The number of DM participants in the low, middle, and high tertile groups was 323, 324, and 323, respectively. The four different average hearing thresholds were significantly higher in the low tertile group than in the high tertile group. The prevalence of HL in the low, middle, and high tertile groups was 23.8% (n = 77), 17.3% (n = 56), and 13.0% (n = 42), respectively (P = 0.001).
The number of non-HTN participants in the low, middle, and high tertile groups was 1176, 1177, and 1177, respectively. The four different average hearing thresholds were significantly higher in the low tertile group than in the other tertile groups (Fig. S3). The prevalence of HL in the low, middle, and high tertile groups was 12.2% (n = 143), 7.4% (n = 87), and 5.8% (n = 68), respectively (P < 0.001). For HTN participants, the numbers of participants in low, middle, and high potassium intake tertiles were 798, 799, and 798, respectively. The four different average hearing thresholds were significantly lower in the high tertile group than in the other tertile groups. The prevalence of HL in the low, middle, and high tertile groups was 19.2% (n = 153), 17.3% (n = 138), and 11.0% (n = 88), respectively (P < 0.001).
Discussion
In the present study, we determined and evaluated the association between potassium intake and hearing thresholds in the Korean adult population. The results indicated an association of potassium intake levels with the four different average hearing thresholds (Low-Freq, Mid-Freq, High-Freq, and AHT) and HL. Univariate and multivariate analyses showed that the four different average hearing thresholds were lower in the high tertile group than in the middle and low tertile groups. Linear regression analyses showed inverse associations between potassium intake levels and the four different average hearing thresholds. Logistic regression analyses showed an association between potassium intake levels and HL.
Various nutrients have been reported to be associated with hearing impairment6,35,37,38,39. Some studies showed an association between factors depicting the general nutrition status, such as body indices or serum albumin levels, and hearing impairment37. Using a body composition analyzer, Lee et al. showed an association between sarcopenia and hearing impairment38. Kang et al., who analyzed a cohort similar to ours, showed that the levels of micronutrients, including vitamins C and D, are associated with hearing thresholds6. Some reports showed associations between dietary patterns and hearing35,39. Prospective or cross-sectional studies examining the association between nutrients and hearing impairment may be on-going.
Potassium is an important electrolyte that plays key roles in cell metabolism and maintenance of the cell membrane potential. The range of normokalemia is narrow (3.5–5.0 mEq/L), and hypokalemia or hyperkalemia can lead to serious complications, such as cardiac arrest or respiratory failure40. The kidney is an important organ with a wide excretion rate (5–500 mEq/day), and the development of hyperkalemia or hypokalemia in an individual on a regular diet (35–110 mEq/day) is rare41. Several researchers have focused on the association between cardiovascular disease and dietary potassium levels8,9,10. Generally, high-potassium diets reverse the effects of cardiovascular diseases through increases in diuresis and decreases in smooth muscle proliferation, free radicals, and platelet aggregation41.
There are few animal or human studies regarding the direct or indirect effects of a high-potassium diet on hearing impairment. The mechanisms underlying the relationship between a high-potassium diet and hearing impairment are poorly understood. However, there are some suggestions regarding this issue. Small changes beyond the normal serum potassium level would be critical. Therefore, favorable results for hearing impairment in individuals on a high-potassium diet may be associated with the secondary effect of a decrease in the extracellular fluid and blood pressure through natriuresis caused by high-potassium diet, rather than changes in the serum potassium level. Previous studies that investigated the association between HTN and cochlear damage provide indirect evidence of the association between a high-potassium diet and hearing impairment. Tachibana et al. showed that hypertensive rats exhibited cochlear damage through a decrease in the oxygen supply from the stria vascularis42. McDormick et al. showed a positive association between cochlear potential and blood pressure43.
Another pathogenesis is upregulation of Na+-K+ ATPase and NKCC1 through aldosterone. Previous studies showed that a high-potassium diet is associated with an increase in aldosterone, which leads to upregulation of Na+-K+ ATPase in both renal tubules and the stria vascularis23,24. Ding et al. also showed that aldosterone upregulated NKCC1 in an in vitro study25. Tardos et al. showed that serum aldosterone levels decrease with age in humans and are inversely associated with the severity of presbycusis26. In addition, an in vivo study showed that long-term aldosterone treatment increases NKCC1 expression, which prevents the progression of age-related HL27. Upregulation of Na+-K+ ATPase and NKCC1 through aldosterone would be helpful in maintaining a proper potassium recycle and endocochlear potential, which may be associated with the preventive effects of a high-potassium diet. Although our study did not analyze aldosterone levels, the abovementioned studies provide indirect evidence regarding the association between a high-potassium diet and hearing impairment.
Steinke et al. showed that mutation or post-translational modification of CLC-K/Barttin is important for potassium secretion into the endocochlea, but the incidence of Bartter’s syndrome caused by these abnormalities may be rare in the general population (1.2/million)44,45,46. Abnormalities in CLC-K/Barttin chloride channels combined with clinical significance would be ignored in population-based study.
Dietary patterns are influenced by various characteristics such as age, sex, and socioeconomic status. The clinical effects of diet are small but long-standing, unlike those of other interventions or drugs. These effects may be associated with the differences in baseline characteristics among groups in the present study. Using both multivariate analyses and propensity score matching, we tried to adjust for these differences. The results of multivariate analyses were similar to those of univariate analyses. In addition, we adjusted for the differences in baseline characteristics between the non-high group (middle and low tertile) and the high tertile group using propensity score matching. These analyses showed that the four different average hearing thresholds and HL were both inversely associated with potassium intake levels.
Our study was a retrospective, cross-sectional study, and proper adjustment for confounding factors was a major concern for our study design. There were significant differences in baseline characteristics among the potassium tertile groups. Although multivariate analysis is useful for adjusting different characteristics, additional data regarding propensity analysis would be helpful to overcome these confounding factors or differences in baseline characteristics. In the present study, propensity scores were calculated between the high tertile and non-high groups, and participants matched based on propensity scores were analyzed.
In the present study, participants were divided into tertile groups according to potassium intake levels. A dichromatic approach, such as the inclusion of normal and abnormal groups, will be prone to false-positive results. Analyses using more categories would be helpful to identify changes in hearing according to potassium intake levels; however, several categories will be associated with complex results that may be difficult to understand. We used tertile levels in the present study, which were easy to understand and minimized false-positive results.
This study had a few limitations. Firstly, it was a cross-sectional design with a failure to establish causality. Second, the study evaluated potassium intake levels using the food intake survey and the 24-h recall method, and possible errors in potassium measurements may have biased the results. Third, between groups, statistically significant differences in hearing thresholds were small. Fourth, there is possibility of a selection bias because of the exclusion of 17 096 participants with missing data. The excluded participants represented approximately 74.0% of the population. In particular, data regarding hearing thresholds was missing for 13 338 participants. Our study did not perform additional analyses regarding missing data. Fifth, in our study, multivariate analyses were adjusted for many, but not all confounding factors. Possible confounding factors, such as history of ototoxic drug use, recent trauma, genetic susceptibility to hearing impairment, or omega-3 fatty acid intake, were not considered in the present study. Further prospective studies that include follow-up data, more confounding factors, and speech discrimination are necessary to overcome selection bias and evaluate a possible correlation between potassium intake levels and hearing impairment. Including speech discrimination can not only help to confirm hearing impairment, but also to understand the effect it has in daily life.
In conclusion, high potassium intake levels were associated with a lower prevalence of HL and lower hearing thresholds in the Korean adult population. Further research should determine whether interventions that improve the potassium intake may help in preventing hearing impairment in the Korean adult population.
References
World Health Organization. Deafness and hearing loss. Geneve: World Health Organization, https://www.who.int/en/news-room/fact-sheets/detail/deafness-and-hearing-loss (2019).
Exeter, D. J., Wu, B., Lee, A. C. & Searchfield, G. D. The projected burden of hearing loss in New Zealand (2011–2061) and the implications for the hearing health workforce. N Z Med J 128, 12–21 (2015).
Lee, F. S., Matthews, L. J., Dubno, J. R. & Mills, J. H. Longitudinal study of pure-tone thresholds in older person. Ear Hear. 26, 1–11 (2005).
Van Eyken, E., Van Camp, G. & Van Laer, L. The complexity of age-related hearing impairment: contributing environmental and genetic factors. Audiol Neurootol 12, 345–358 (2007).
Cruickshanks, K. J. et al. Education, occupation, noise exposure history and the 10-yr cumulative incidence of hearing impairment in older adults. Hear Res. 264, 3–9 (2010).
Kang, J. W., Choi, H. S., Kim, K. & Choi, J. Y. Dietary vitamin intake correlates with hearing thresholds in the older population: the Korean National Health and Nutrition Examination Survey. Am J Clin Nutr 99, 1407–1413 (2014).
Simpson, A. N., Matthews, L. J. & Dubno, J. R. Lipid and C-reactive protein levels as risk factors for hearing loss in older adults. Otolaryngol Head Neck Surg 148, 664–670 (2013).
Palmer, B. F. & Clegg, D. J. Achieving the benefits of a high-potassium, paleolithic diet, without the toxicity. Mayo Clin Proc 91, 496–508 (2016).
Hajjar, I. M., Grim, C. E., George, V. & Kotchen, T. A. Impact of diet on blood pressure and age-related changes in blood pressure in the US population: analysis of NHANES III. Arch Intern Med 161, 589–593 (2001).
Aburto, N. J. et al. Effect of increased potassium intake on cardiovascular risk factors and disease: systematic review and meta-analyses. BMJ. 346, f1378, https://doi.org/10.1136/bmj.f1378 (2013).
World Health Organization. WHO issues new guidance on dietary salt and potassium. Geneva: World Health Organization, http://www.who.int/mediacentre/news/notes/2013/salt_potassium_20130131/en/ (2013)
Fetoni, A. R., Picciotti, P. M., Paludetti, G. & Troiani, D. Pathogenesis of presbycusis in animal models: a review. Exp Gerontol. 46, 413–425 (2011).
Brown, J. N., Miller, J. M. & Nuttall, A. L. Age-related changes in cochlear vascular conductance in mice. Hear Res. 86, 189–194 (1995).
Hwang, J. H., Hsu, C. J., Yu, W. H., Liu, T. C. & Yang, W. S. Diet-induced obesity exacerbates auditory degeneration via hypoxia, inflammation, and apoptosis signaling pathways in CD/1 mice. PLoS One. 8, e60730, https://doi.org/10.1371/journal.pone.0060730 (2013).
Cheng, C. J., Truong, T., Baum, M. & Huang, C. L. Kidney-specific WNK1 inhibits sodium reabsorption in the cortical thick ascending limb. Am J Physiol Renal Physiol 303, F667–F673 (2012).
Haddy, F. J. Roles of sodium, potassium, calcium, and natriuretic factors in hypertension. Hypertension 18(Suppl 5), III179–183 (1991).
Appel, L. J. et al. Dietary approaches to prevent and treat hypertension: a scientific statement fromthe American Heart Association. Hypertension. 47, 296–308 (2006).
Ascherio, A. et al. Intake of potassium, magnesium, calcium, and fiber and risk of stroke among US men. Circulation. 98, 1198–1204 (1998).
Gates, G. A., Cobb, J. L., D’Agostino, R. B. & Wolf, P. A. The relation of hearing in the elderly to the presence of cardiovascular disease and cardiovascular risk factors. Arch Otolaryngol Head Neck Surg 119, 156–161 (1993).
Fuortes, L. J., Tan, S., Pomrehn, P. & Anderson, C. Prospective evaluation of associations between hearing sensitivity and selected cardiovascular risk factors. Am J Ind Med 28, 275–280 (1995).
Nomura, K., Nakao, M. & Morimoto, T. Effect of smoking on hearing loss: quality assessment and meta-analysis. Prev Med. 40, 138–44 (2005).
Horikawa, C. et al. Diabetes and risk of hearing impairment in adults: a meta-analysis. J Clin Endocrinol Metab 98, 51–58 (2013).
ten Cate, W. J., Curtis, L. M. & Rarey, K. E. Effects of low-sodium, high-potassium dietary intake on cochlear lateral wall Na+, K(+)-ATPase. Eur Arch Otorhinolaryngol 251, 6–11 (1994).
McDonough, A. A., Veiras, L. C., Guevara, C. A. & Ralph, D. L. Cardiovascular benefits associated with higher dietary K+ versus lower dietary Na+: Evidence from population and mechanistic studies. Am J Physiol Endocrinol Metab 312, E348–E356 (2017).
Ding, B. et al. Direct control of Na(+)-K(+)-2Cl(−)-cotransport protein (NKCC1) expression with aldosterone. Am J Physiol Cell Physiol 306, C66–C75 (2014).
Tadros, S. F., Frisina, S. T., Mapes, F., Frisina, D. R. & Frisina, R. D. Higher serum aldosterone correlates with lower hearing thresholds: a possible protective hormone against presbycusis. Hear Res. 209, 10–18 (2005).
Halonen, J. et al. Long-term treatment with aldosterone slows the progression of age-related hearing loss. Hear Res. 336, 63–71 (2016).
Rehm, J. et al. Alcohol use. In: Ezzati M, Lopez A, Rodgers A, Murray CJL eds. Comparative Quantification of Health Risks: global and regional burden of disease attributable to selected major risk factors. Geneva, World Health Organization. 12959–1108 (2004).
The Korea Centers for Disease Control and Prevention. Alcohol drinking, http://health.mw.go.kr/HealthInfoArea/HealthInfo/View.do?idx=5800&subIdx=4&searchCate=&searchType=&searchKey=&pageNo=&category=1&category_code=301301306&dept=3&sortType=date&page=1&searchField=titleAndSummary&searchWord= (2019).
World Health Organization. Global recommendations on physical activity for health. Geneva: World Health Organization, http://apps.who.int/iris/bitstream/10665/44399/1/9789241599979_eng.pdf (2010).
Levey, A. S. et al. A new equation to estimate glomerular filtration rate. Ann Intern Med 150, 604–612 (2009).
Kang, H., Jung, H. J. & Paik, H. Y. Analysis of Foods and Nutrients Intake Obtained at the Final Probing Step in 24-hour Recall Method. Korean J Nutr 42, 158–170 (2009).
Rural Resource Development Institute. Food composition table. (Rural Resource Development Institute Press, Korea, 2006).
The Korean Nutrition Society. Dietary Reference Intakes for Koreans. (The Korean Nutrition Society press, Korea, 2015).
Km, S. Y., Sim, S., Kim, H. J. & Choi, H. G. Low-fat and low-protein diets are associated with hearing discomfort among the elderly of Korea. Br J Nutr 114, 1711–1717 (2015).
Willett, W. Nutritional Epidemiology. (Oxford University Press, New York, 2013).
Michikawa, T. et al. Markers of overall nutritional status and incident hearing impairment in community-dwelling older Japanese: The Kurabuchi Study. J Am Geriatr Soc 64, 1480–1485 (2016).
Lee, J., Han, K., Song, J. J., Im, G. J. & Chae, S. W. Sarcopenia and hearing loss in older Koreans: Findings from the Korea National Health and Nutrition Examination Survey (KNHANES) 2010. PLoS One 11, e0150281, https://doi.org/10.1371/journal.pone.0150281 (2016).
Rosenhall, U., Idrizbegovic, E., Hederstiema, C. & Rothenberg, E. Dietary habits and hearing. In J Audiol 54(Suppl1), S53–56 (2015).
Mount, D. B & Zandi-Nejad, K. Disorders of Potassium Balance. In Brenner and Rector’s The Kidney, chap. 17, 640–688 (Elsevier Press, USA, 2012).
Rigsby, C. S., Pollock, D. M. & Dorrance, A. M. Dietary potassium supplementation improves vascular structure and ameliorates the damage caused by cerebral ischemia in normotensive rats. Nutr Metab (Lond) 5, 3, https://doi.org/10.1186/1743-7075-5-3 (2008).
Tachibana, M. et al. The site of involvement of hypertension within the cochlea. A comparative study of normotensive and spontaneously hypertensive rats. Acta Otolaryngol. 97, 257–265 (1984).
McCormick, J. G., Harris, D. T., Hartley, C. B. & Lassiter, R. B. Spontaneous genetic hypertension in the rat and its relationship to reduced ac cochlear potentials: implications for preservation of human hearing. Proc Natil Acad Sci USA 79, 2668–2672 (1982).
Steinke, K. V. et al. Human CLC-K Channels Require Palmitoylation of Their Accessory Subunit Barttin to Be Functional. J Biol Chem 290, 17390–17400 (2015).
Rudin, A. Bartter’s syndrome. A review of 28 patients followed for 10 years. Acta Med Scand 224, 165–171 (1988).
Koulouridis, E. & Koulouridis, I. Molecular pathophysiology of Bartter’s and Gitelman’s syndromes. World J Pediatr 11, 113–125 (2015).
Acknowledgements
This study was supported by the Medical Research Center Program through the National Research Foundation of Korea (NRF), funded by the Ministry of Science, ICT and Future Planning [grant number 2015R1A5A2009124] and the NRF Grant funded by the Korea government (MSIT) [grant number 2018R1C1B6007775]. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
S.H.K. and J.Y.D. conceived the research idea; K.H.C. and J.Y.L. performed the experiments and the statistical analyses; D.J.J. and S.H.K. wrote the paper; J.Y.D. and S.H.K. had primary responsibility for final content. All authors approved the final version of the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Jung, D.J., Lee, J.Y., Cho, K.H. et al. Association between a High-Potassium Diet and Hearing Thresholds in the Korean Adult Population. Sci Rep 9, 9694 (2019). https://doi.org/10.1038/s41598-019-45930-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-45930-5
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
