
Abstract
Recent data has suggested a definitive role for inflammatory processes in the pathophysiology of epilepsy. In this study we hypothesized that food allergies, as chronic inflammatory processes, underlie the pathophysiology of refractory idiopathic epilepsy and investigated whether food elimination diets may assist in managing refractory epilepsy. The study was conducted on 34 patients up to 16 years of age with refractory convulsions who attended the Allergy Outpatient Clinic, Mofid Children Hospital between 2015 and 2016 with youngest and oldest participants at ages of 3 months and 16 years old, respectively. The participants were categorized into three groups according to the results of skin prick test and serum specific IgE measurements. Elimination diets were instituted for the patients with non IgE-mediated and mixed food allergies. The study was conducted for a period of 12 weeks. The participants were assessed for at least 50% reduction in number of seizures following the intervention. There was a significant reduction in number of seizures (p < 0.001) following the intervention. Seventeen patients (50%) did not experience any seizures after 8 weeks of treatment and 12 patients (35%) had a significant (51–99%) decrease in the number of their seizures. Five patients did not show any changes in their daily seizure frequency. The obtained data suggest that food allergy may play a role in triggering refractory epilepsies and their adequate response to treatment. A trial of elimination diet showed more than 50% seizure reduction in more than 85% of the children studied. However, we believe these results are preliminary and they motivate a fully controlled study in the future.
Similar content being viewed by others


Introduction
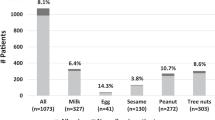
Food allergy is a serious health problem affecting up to 8% of children and increasingly capturing the attention as a modern-day epidemic with poorly understood drivers1. In more than 90% of cases, food allergy is due to the 6 main foods including cow’s milk, egg, soy, wheat, peanut, tree nuts and fish2. In contrast to IgE-mediated food allergies for which an accurate diagnosis can be reached by various tests and history, when history and physical examination is indicative of cell-mediated or mixed mechanisms, a trial of elimination diet based on the history is recommended3,4,5.
Idiopathic refractory epilepsies are estimated to comprise 10% to 20% of childhood epilepsies6, which may adversely affect brain development6. Refractory epilepsy is defined as convulsions that are not controlled with 3 or 4 appropriate first line drugs despite adequate duration and dosage7. There is accumulating evidence that inflammatory processes contribute to pathophysiology of refractory seizures6. Many previous studies have indicated that allergic reactions are major causes of inflammatory processes in epileptic children7. The idea of the role of food allergy in inducing epilepsy is referred to Ward and Patterson in 1927, who performed skin prick test for food allergens on 1000 epileptic individuals and 100 healthy controls and found that 37–67% of patients revealed wheal and flare reactions indicative of prior sensitivity while only 8% of the healthy control group showed positive reactions8. In 1989, Egger reported that of the 45 epileptic children, 25 ceased to have seizures and 11 had fewer seizures during oligo-antigenic diet therapy. In 2001, Frediani et al. evaluated 72 epileptic children and 202 healthy control, age-matched individuals with their families. They found higher rates of cow’s milk allergy and asthma in epileptic children and dermatitis and rhinitis in their mothers and their siblings, respectively9. In 2008, Durkin et al. evaluated 91642 children and found higher rate of epilepsy among children with allergic disorders compared with non-allergic children10 and concluded that allergic inflammation may contribute to epileptogenesis. However, many authors have refuted this hypothesis11.
Recent research data shows a correlation between peripheral inflammation and disease development in central nervous system as the underlying mechanism12,13,14. Thinking of food allergy as a seizure trigger is rather a novel idea and confirmation of this relationship may be difficult. However, once confirmed it may break a new ground in treatment of refractory convulsions in paediatric age group.
In this study, we hypothesized that inflammatory process (involving gut) is an underlying cause in some cases of refractory epilepsy13,14,15,16 and investigated whether a significant relationship exists between these intractable seizures and food allergy.
Patients and Methods
Participants
This prospective, self-controlled and quasi-experimental study was conducted from January 2015 to February 2016 at the Allergic Outpatient Clinic, Mofid Children Hospital, Shahid Beheshti University of Medical Sciences, Tehran. Shahid Beheshti University is responsible for overseeing the health services of more than 5.4 million people in the province of Tehran, including the northern, western and eastern parts of Tehran. Mofid Children Hospital is the only tertiary center that covers all the above areas for treatment of critically ill patients specially patients with refractory seizures.
In this study refractory seizure was defined according to definition of “drug resistant epilepsy” as “failure of adequate trials of two tolerated, appropriately chosen and used antiepileptic drug schedules (whether as monotherapies or in combination) to achieve sustained seizure free”17.
Inclusion criteria
Patients with a definition of an idiopathic refractory seizure according to the above mentioned diagnostic criteria, aged 3 months to 16 years with a diagnosis of non-IgE mediated food allergy were included.
Exclusion criteria
Patients with IgE-mediated food allergy including patients with anaphylaxis (due to their strict self-restrictive diets for prevention of severe hypersensitivity reactions), non-adherence to the avoidance diets, any growth faltering due to negative impacts of elimination diets and refractory seizures due to secondary causes (cerebral palsy, metabolic disorders, etc.) were excluded.
Sample size calculation
The sample size of this study was determined according to similar studies performed previously evaluating the efficacy of ketogenic diets on refractory seizures18,19,20,21,22 due to the lack of previous studies with hypoallergenic regimens.
Those studies demonstrated 50% seizure reduction in 38–50% of the patients after establishment of ketogenic diet. Considering type one error of 5% and type 2 error of 20%, the calculated sample size was 16 patients but due to probable loss of patients during the follow-up period, a total of 34 patients were enrolled in this study.
Signed informed consent was obtained from patients’ parents or their caregivers in accordance with the Code of Ethics of the World Medical Association (Declaration of Helsinki).
Study Design
Patients enrolment to study was based on convenience in available, continuous and non-random manner.
Since the anticonvulsants could not be stopped due to ethical and therapeutic issues, a parallel control group was not considered and the patients’ clinical situation were compared with their own, before and after the intervention.
Demographic and laboratory data
A questionnaire including demographic data and allergic signs and symptoms consisting of dermatological, upper and lower respiratory and gastrointestinal complaints was prepared and completed for each participant. All patients underwent diagnostic evaluations including complete blood count (for eosinophilia), serum specific IgE measurement and skin prick test for at least 6 common food allergens (cow’s milk, egg, peanut, soy, wheat and sea foods) and aeroallergens (house dust mite and common mixed aeroallergens).
A wheal of 3 mm or greater compared with negative control (saline) in skin prick test was considered positive.
Those with previous history of immediate reaction to food allergens, with development of objective or convincing symptoms after ingestion of the offending food and positive skin prick tests were diagnosed as IgE-mediated food allergy and were excluded from the study.
Dietary Protocol
Since six common foods are implicated in triggering food allergy with IgE- and non IgE-mediated mechanisms and due to the lack of standard allergic tests in delayed type food allergies with non IgE-mediated mechanisms, a six food elimination diet remains as an appropriate diagnostic and therapeutic tool in patients with negative skin prick test23. Therefore, all patients with positive skin prick test and negative history of immediate reactions were considered as mixed type (IgE and non-IgE mediated) and those with negative skin prick test were regarded as non-IgE (cell-mediated) type food allergies. Dietary avoidance was recommended for both groups. Those children with refractory seizures who met the inclusion criteria and were compliant with the dietary protocol, were treated according to the following protocol.
For breastfed infants less than 6 months of age, a six-food elimination diet in addition to the specific allergens with positive results in skin prick test was initiated for their mothers and exclusive breast feeding for their nursing infant was implemented. In formula-fed infants less than 6 months of age, elemental based formula (Neocate, Nutricia) was prescribed exclusively. For breastfed infants over six months of age, a six-food elimination diet (cow’s milk, egg, peanut, soy, wheat, sea foods) in addition to the specific offender food with positive results in skin prick test were initiated for both mother and the nursing child. In formula-fed infants, a Neocate formula in addition to a six food elimination diet was started. In children, a six-food elimination diet (cow’s milk, egg, peanut, soy, wheat, sea foods) in addition to the specific offender food with positive results in skin prick test was started.
All the infants were continuously being monitored for any deviation from their growth and developmental curve parameters during a total period of twelve weeks (8 weeks of implementing the above mentioned dietary intervention and for the 4 following weeks after). In the case of any growth and developmental abnormalities, the patient was excluded from the study to avoid further developmental delay.
Primary Outcome Measures
The primary outcome measures were defined as any reduction in seizure frequency after implementation of the hypoallergenic diet. The results of this study were evaluated in three distinct groups as complete elimination of seizures, or >90% reduction in seizures,or >50% reduction in seizures15,16.
Ethical Code
This research is confirmed in Iranian Registry of Clinical Trials with registration reference of IRCT20171022036925N2 on 10/03/2018 (www.irct.ir/user/trial/27457/view).
The study protocol was approved by the Ethics Committee of Mofid Children Hospital. It is worth mentioning that all the information was confidential and all the appropriate measures have been taken to insure patients’ confidentiality.
Statistical Analysis
This study used common statistics to summarize data and to describe the variables of a data set and descriptive statistics such as domain, mean and standard deviation.
After completing the forms, statistical analysis was performed using Paired t-Test, X2 and Fisher’s exact test. SPSS software version 16 was used. In all tests p < 0.05 was considered significant.
Results
The youngest patient was 3 months old and the oldest was 16 years old with a mean age of 4 year (±3.5 SD). Seventeen patients (50%) were female and 17 were male (female/male ratio was 1). The mean age of seizure onset was 2 years (±2.5 SD). The mean age for initiation of anticonvulsant drugs was 3 years (±3.2 SD) (with a minimum age of one month and a maximum age of 10 years). A careful history revealed an allergic disorder in 29 of those patients (85.3%). Sixteen patients (47.1%) had cutaneous allergic involvement, 17 patients (50%) had some types of upper respiratory tract allergies and 21 patients (61.8%) had lower respiratory tract allergies. Gastrointestinal allergies were detected in 13 patients (38.2%). There were no complications including weight loss in patients receiving hypoallergenic diets in this study.
The patients’ data have been summarized in Table 1.
Table 2 shows EEG and MRI findings in the patients.
The most implicated food in skin prick tests were hen’s egg (32.4%), cow’s milk (20.6%), soy (20.6%) and peanut (20.6%), respectively (Table 3).
Tables 4 and 5 demonstrate that house dust mite with 11.8% and tree pollens with 23.5% positivity in skin prick test were the most common indoor and outdoor aeroallergens in the studied patients, respectively.
Allergic Nasal and dermatological symptoms including nasal congestion and eczematous dermatitis were the most presented clinical sign and symptoms (Table 6).
Positive skin prick test was detected in 27 patients (79.4%). Twelve patients (35%) were sensitive to outdoor allergens and 6 (17.6%) had sensitivity to indoor allergens. The most common allergens among outdoor allergens were trees, grass and weed (23.5%, 17.6% and 17.6% respectively). Mites (11.8%) and cats (9.5%) were the most common indoor allergens detected by skin prick test. The definitive dominancy of food allergens is well demonstrated, as 73.5% of the positive skin prick tests were due to food allergens including egg (23.4%), cow’s milk (20.6%), soy (20.6%) and peanut (20.6%).
The daily average number of seizures in the studied population prior to intervention (food elimination diets) was 7.3 ± 0.4. It was reduced to 3.1 ± 0.5 after 8 weeks of strict diet. The mean rate of response to the intervention was 85.2% (±32.8 SD). Six patients (17.6%) demonstrated 50% to 89% reduction in the number of seizures, a significant decrease in seizures (90–99%) was also shown in other 6 cases (17.6%) and 17 patients (50%) became totally seizure free after 8 weeks of restrict dietary intake. These findings remained unchanged after 4 weeks of follow-up.
All of these findings were significant and meaningful. Only 5 patients did not show any significant response to therapy with no changes in their daily seizure frequency with elimination diets. There was no significant relationship between the response to therapy (defined as more than 50% reduction in the number of daily seizures after implementation of an 8-week period of elimination diets) and age (p = 0.49), gender (p = 0.33), skin prick test results (p = 0.1) and the type of seizure (p = 0.1).
Discussion
The purpose of this study was to determine the relationship between refractory seizures and food allergies as an important cause of intestinal inflammation and consequently to investigate the role of food avoidance in certain patients with evidence of food allergy to control refractory seizures. Therefore, we sought for the effect of hypoallergenic diets on refractory seizures and we found a significant decline in the rate of daily seizures not only after an eight-week allergen elimination diet but also in the following 4 weeks of follow-up (p < 0.001).
There is a wealth of experience about the role of ketogenic diets on refractory seizures18,19,20,21,22,23,24,25,26,27.
The results on less than 20% seizure free after institution of ketogenic diet 24) compared to our results with hypoallergenic diets showing seizure freedom in 50% of patients and seizure reduction in more than 85% of patients during 12 weeks of elimination diet, are convincing.
It is known that allergic diseases are very common conditions with inflammation accounting for their main patho-mechanism25,26,27. In a study performed by Silverberg et al., epileptic children were found to have a high prevalence of allergic disease (~46%)22,26,28,29. Therefore, they suggested that epilepsy may be a comorbidity of severe childhood allergic disease22. Similarly, we noticed the following allergic symptoms including chronic dermatitis, lower respiratory tract allergy symptoms, and gastrointestinal tract symptoms including gastroesophageal reflux, chronic constipation, diarrhoea, abdominal cramp and perianal symptoms in the medical histories of twenty-nine patients (85%) in the present study.
The role of food allergens specially cow’s milk protein and wheat, as triggering factors in seizures have been emphasized by few case reports in literature. Egger studied the role of oligo-antigenic diets on 63 children with epilepsy whose seizures ceased during the diet therapy30. Lucarelli suggested the role of cow’s milk allergy in children suffering from Rolandic epilepsy with complete clinical remission in 85% of the cases with a cow’s milk free diet and reappearance of the seizures with reintroduction of cow’s milk into diet31. Kok et al. reported an infant presented with anaphylaxis to wheat who had developed generalized tonic clonic seizures 1.5 hours after initial reaction. Her skin prick test to wheat became positive later at 13 months old. The authors concluded that the complex immunological mechanism regulating the allergic reaction to food might play a significant role in this epileptic manifestation28.
In addition, concomitant seizure disorder has been reported in eosinophilic gastrointestinal disorder (EGID)32.
There are growing evidence emphasizing the role of inflammation as the main cause of seizure8,29.The proposed mechanisms underlying the peripheral inflammation causing seizure activity indicate the interaction between the nervous and the immune systems14 and implicate inflammation-related elements including cytokines, endogenous opioids, the nitric oxide signalling pathway and prostaglandins33. There are considerable reasons to believe that allergy may act as seizure precipitant in refractory epilepsies31.
Riazi et al. suggested that systemic inflammation may induce a mirror inflammatory response in the brain with short or long-term effects on seizure susceptibility8. Any disruption in blood brain barrier due to peripheral inflammation may play a key role in this regard14. A definitive role is suggested for pro-inflammatory cytokines including IL-1β and TNF-α in the brain and particularly in neuronal transmission34,35. In Silverberg study on mice a single tonic-clonic seizure induced IL-4 and IgE-negative T and B cells to infiltrate brain; therefore, suggested that inflammatory pathways in allergic diseases may be activated in brain which contribute toward epilepsy22. Riazi et al. also identified a microglial-dependent increase in CNS excitability mediated by TNF which is due to a potential link between peripheral and central inflammation36. Falsaperla and Vitaliti presented 3 cases with gastroenteritis involvement as the site of peripheral inflammation. They suggested a peripheral inflammation due to food allergy involving the gastrointestinal tract with subsequently stimulated antigen presenting cells, T helper2 lymphocyte subsets and their secretion of pro-inflammatory cytokines. Durkin et al. suggested milk proteins in cow’s milk allergic patients as the major cause for gastrointestinal inflammation, and hence, induction and migration of T-lymphocytes sensitized to cow’s milk protein within the blood brain barrier13. Epilepsy also has been reported as a documented neurological manifestation of celiac disease with a prevalence of 0.8–6%37. Gluten sensitivity may also present with neurological manifestations so that the underlying disease may easily become unrecognized and untreated37.
As gastrointestinal tract is a prominent organ involved in non-IgE mediated food allergy, it can be assumed that allergic inflammation in gastrointestinal tract (as a peripheral cause of inflammation) could be the reason for the seizures in our patients. A recently raised theory called gut brain axis, suggests a bidirectional communication between gut and brain which may be a justification for our claim38,39.
Our findings may suggest the possibility of a better seizure control with least pharmacological intervention; however, lack of a parallel simultaneous control group might be considered as a limitation to this study. Other limitations include non-randomized patient selection, lack of a control group without any treatments, small sample size, short duration of the study and possibility of patients’ poor compliance with the dietary regime. With regard to the high effect size in our study, the effect of confounders could be ignored. A blinded study on food eliminations is needed to confirm the outcome of this dietary study and further studies may characterize the specific role of cytokines in the development of refractory epilepsies in food allergy.
References
Allen, K. J. & Koplin, J. J. Prospects for prevention of food allergy. The Journal of Allergy and Clinical Immunology: In Practice. 4(2), 215–20 (2016).
Nowak-Wegrzyn, A., Burks, A. W. & Sampson, H. A. Reactions to Foods. In: Adkinson N. F. et al. e, editors. Middleton’s Allergy Principles and Practice. 2. 8th ed. Philadelphia: Elsevier-Saunders; p. 1310. (2014).
Sicherer, S. H. Epidemiology of food allergy. The Journal of allergy and clinical immunology. 127(3), 594–602 (2011).
Santos, A. F. & Brough, H. A. Making the most of in vitro tests to diagnose food allergy. The Journal of Allergy and Clinical Immunology: In Practice. 5(2), 237–48 (2017).
Nowak-Wegrzyn, A. & Sampson, H. A. Adverse reactions to foods. The Medical clinics of North America. 90(1), 97–127 (2006).
Strom, M. A. & Silverberg, J. I. Allergic disease is associated with childhood seizures: An analysis of the 1997–2013 National Health Interview Survey. The Journal of allergy and clinical immunology. 137(3), 951–3.e2 (2016).
Ishikawa, N., Kobayashi, Y., Fujii, Y. & Kobayashi, M. Increased interleukin-6 and high-sensitivity C-reactive protein levels in pediatric epilepsy patients with frequent, refractory generalized motor seizures. Seizure. 25, 136–40 (2015).
Riazi, K., Galic, M. A. & Pittman, Q. J. Contributions of peripheral inflammation to seizure susceptibility: cytokines and brain excitability. Epilepsy research. 89(1), 34–42 (2010).
Livingston, J. H. Management of intractable epilepsy. Archives of disease in childhood. 66(12), 1454–6 (1991).
Ghazavi, A. et al. The Ketogenic and Atkins diets effect on intractable epilepsy: A comparison. Iranian journal of child neurology. 8(3), 12 (2014).
Ward, J. F. & Patterson, H. A. Protein sensitization in epilepsy: a study of one thousand cases and one hundred normal controls. Archives of Neurology &. Psychiatry. 17(4), 427–43 (1927).
Frediani, T. et al. Allergy and childhood epilepsy: a close relationship? Acta neurologica Scandinavica. 104(6), 349–52 (2001).
Durkin, H. G., Joks, R. O. & Silverberg, J. I. Allergic Disease in US Children Is Associated with Increased Prevalence of Epilepsy. Journal of Allergy and Clinical Immunology. 131(2), AB200 (2013).
Asadi-Pooya, A. A., Mintzer, S. & Sperling, M. R. Nutritional supplements, foods, and epilepsy: is there a relationship? Epilepsia. 49(11), 1819–27 (2008).
Riazi, K. et al. Intestinal inflammation alters the susceptibility to pentylenetetrazole‐induced seizure in mice. Journal of gastroenterology and hepatology. 19(3), 270–7 (2004).
Falsaperla, R. et al. Epileptic seizures as a manifestation of cow’s milk allergy: a studied relationship and description of our pediatric experience. Expert review of clinical immunology. 10(12), 1597–609 (2014).
Kwan, P. et al. Definition of drug resistant epilepsy: consensus proposal by the ad hoc Task Force of the ILAE Commission on Therapeutic Strategies. Epilepsia. 51(6), 1069–77 (2010).
Freeman, J. M. et al. A blinded, crossover study of the efficacy of the ketogenic diet. Epilepsia. 50(2), 322–5 (2009).
Freeman, J. M. et al. The efficacy of the ketogenic diet-1998: a prospective evaluation of intervention in 150 children. Pediatrics. 102(6), 1358–63 (1998).
Keene, D. L. A systematic review of the use of the ketogenic diet in childhood epilepsy. Pediatric neurology. 35(1), 1–5 (2006).
Lefevre, F. & Aronson, N. Ketogenic diet for the treatment of refractory epilepsy in children: a systematic review of efficacy. Pediatrics. 105(4), e46–e (2000).
Neal, E. G. et al. The ketogenic diet for the treatment of childhood epilepsy: a randomised controlled trial. The Lancet Neurology. 7(6), 500–6 (2008).
Kagalwalla, A. F. et al. Effect of six-food elimination diet on clinical and histologic outcomes in eosinophilic esophagitis. Clinical gastroenterology and hepatology: the official clinical practice journal of the American Gastroenterological Association. 4(9), 1097–102 (2006).
Li, H.-f, Zou, Y. & Ding, G. Therapeutic success of the ketogenic diet as a treatment option for epilepsy: a meta-analysis. Iranian journal of pediatrics. 23(6), 613 (2013).
Dumitrascu, D. Allergy as a systemic disease. Roumanian archives of microbiology and immunology. 60(3), 227–36 (2001).
Borish, L. Allergic rhinitis: systemic inflammation and implications for management. The Journal of allergy and clinical immunology. 112(6), 1021–31 (2003).
Gustafsson, D., Sjoberg, O. & Foucard, T. Development of allergies and asthma in infants and young children with atopic dermatitis–a prospective follow-up to 7 years of age. Allergy. 55(3), 240–5 (2000).
Chong, K. W., Ling, S. & Loh, W. An unusual case of infant seizures with anaphylaxis to wheat. Asia Pacific allergy. 8(2), e13 (2018).
Vezzani, A., French, J., Bartfai, T. & Baram, T. Z. The role of inflammation in epilepsy. Nature reviews Neurology. 7(1), 31–40 (2011).
Vitaliti, G. et al. Nervous system involvement in clinical peripheral inflammation: A description of three pediatric cases. Journal of pediatric neurosciences. 11(3), 277–81 (2016).
Lucarelli, S. et al. Cow’s milk allergy and rolandic epilepsy: a close relationship? Archives of disease in childhood. 97(5), 481 (2012).
Guajardo, J. R. et al. Eosinophil-associated gastrointestinal disorders: a world-wide-web based registry. The Journal of pediatrics. 141(4), 576–81 (2002).
Egger, J., Carter, C. M., Soothill, J. F. & Wilson, J. Oligoantigenic diet treatment of children with epilepsy and migraine. The Journal of pediatrics. 114(1), 51–8 (1989).
Crayton, J. W., Stone, T. & Stein, G. Epilepsy precipitated by food sensitivity: report of a case with double-blind placebo-controlled assessment. Clinical EEG (electroencephalography). 12(4), 192–8 (1981).
Silverberg, J. I., Joks, R. & Durkin, H. G. Allergic disease is associated with epilepsy in childhood: a US population-based study. Allergy. 69(1), 95–103 (2014).
Riazi, K. et al. Microglial activation and TNFα production mediate altered CNS excitability following peripheral inflammation. Proceedings of the National Academy of Sciences (2008).
Balosso, S. et al. Molecular and functional interactions between tumor necrosis factor-alpha receptors and the glutamatergic system in the mouse hippocampus: implications for seizure susceptibility. Neuroscience. 161(1), 293–300 (2009).
Montiel-Castro, A. J., González-Cervantes, R. M., Bravo-Ruiseco, G. & Pacheco-López, G. The microbiota-gut-brain axis: neurobehavioral correlates, health and sociality. Frontiers in integrative neuroscience. 7, 70 (2013).
Cryan, J. F. & Dinan, T. G. Mind-altering microorganisms: the impact of the gut microbiota on brain and behaviour. Nature reviews neuroscience. 13(10), 701 (2012).
Acknowledgements
The authors would like to thank Dr. Amir HashemiTari Consultant Psychiatrist at East London NHS Foundation Trust, London, United Kingdom and Mrs Fatemeh Abdollah Gorji. The current study was supported by grant from Paediatric Neurology Research Center of Mofid Hospital affiliated to Shahid Beheshti University of Medical Sciences.
Author information
Authors and Affiliations
Contributions
Study concept and design: Dr. Mansouri, Dr. Karimzadeh, Dr. Gorjipour Acquisition of Data: Dr. Hassanvand Amouzadeh, Dr. Gorjipour, Analysis and Interpretation of Data: Dr. Sohrabi Drafting of the Manuscript: Dr. Darougar, Dr. Mansouri Critical Revision of the Manuscript: Dr. Mansourir, Dr. Sohrabi, Dr. Darougar Statistical Analysis: Dr. Sohrabi Administrative, technical and material support: Dr. Mansouri Study supervision: Dr. Mansouri.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gorjipour, H., Darougar, S., Mansouri, M. et al. Hypoallergenic diet may control refractory epilepsy in allergic children: A quasi experimental study. Sci Rep 9, 6875 (2019). https://doi.org/10.1038/s41598-019-43252-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-019-43252-0
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
