
Abstract
Monitoring immune system activation of wild animals has garnered increasing interest within the field of ecological immunology, leading to an urgent need for non-invasive biomarkers measuring these changes. Urinary neopterin, a marker of the cell-mediated immune response, is validated as an immune-related biomarker in captive and laboratory animals. However, wild animals naturally host higher and chronic pathogen loads. Therefore, detection and quantification of additional infections via neopterin might not be possible against the background of a chronically challenged immune system. To assess the suitability of urinary neopterin in wild animals, we measured neopterin corrected for specific gravity with an enzyme immunoassay in 185 samples collected before, during and after a respiratory disease outbreak in 28 individuals from a group of wild chimpanzees (Taï National Park, Côte d’Ivoire). Urinary neopterin levels were significantly higher during periods when individuals showed respiratory symptoms versus before and after the outbreak. Furthermore, urinary neopterin levels were significantly higher in individuals that died, with higher levels already apparent before the outbreak, suggesting individuals may have an already activated immune system. Measuring urinary neopterin levels, with other biomarkers of energetic condition, stress challenges, and reproduction will contribute towards a deeper understanding of life-history trade-offs in wild animals.
Similar content being viewed by others
Introduction
Being able to measure variation in immune system activation of wild animals has both practical applications towards monitoring the health status of wild populations threatened by disease1, as well as providing theoretical groundwork within the field of ecological immunology2. However, animal physiologists first require the validation of biological markers that can accurately monitor changes in immune system activation3. Specifically, the identification of immune-related biomarkers within non-invasively collected samples is of utmost importance to monitor patterns of immune system activation in free-ranging animals. While non-invasive methods have been used extensively in measuring various endocrine markers within the context of behavioural ecology4,5,6, there has been a limited availability of such methods for monitoring immunity and its role in wildlife disease ecology3.
Traditional methods of health monitoring typically require invasive methods (e.g., blood draws), leading to undue stress while not being applicable or feasible for longitudinal studies of wild large-bodied animals4,7. Non-invasive means of health monitoring, such as using urinary dipsticks8,9,10, behavioural observations11,12, and visual inspection for ecto- and endo-parasites13,14, can lack the required level of precision, and therefore need to be performed in conjunction with other methods to provide meaningful insights into an individual’s health status.
Neopterin, a pteridine, is an early inflammation marker in the cell-mediated immune response (Th1-type)15,16. It is produced by monocytes/macrophages, with production stimulated by interferon-gamma17. In humans, increases in serum neopterin levels have been described in reaction to several viral and bacterial infections, with elevated levels also observed in chronic infections18. Changes in neopterin levels are strongly associated with disease progression, severity and outcome16,19,20— with higher levels typically corresponding to a higher probability of mortality18,21. As neopterin is released as part of the activation of the non-specific immune response, it can also serve as a useful marker in monitoring immune system activation in the context of subclinical, unknown pathogens or diseases18.
Given its reliable application in the study of immune system activation in humans, neopterin has shown promise and garnered the interest of animal physiologists3,22, with particular note that neopterin is chemically stable, even under field conditions7,22, and released with no significant diurnal variation18,23. It is also detectable in several matrices including serum, saliva, and urine—with urinary levels correlating with serum measurements3,15,16, allowing for non-invasive collection. Therefore, measuring urinary neopterin levels has the potential to be of major diagnostic value in measuring and monitoring immune system activation in response to several known and unknown pathogens, as well as systemic conditions, in wild animals.
In zoo, laboratory, and semi-wild non-human primates, urinary neopterin has been successfully validated as a measure for immune system activation22,23,24. For example, in zoo bonobos (Pan paniscus), urinary neopterin levels exhibited a significant increase in response to observed respiratory infection symptoms23. Furthermore, in an experimental study with SIV-infected rhesus macaques (Macaca mulatta), elevated urinary neopterin levels were observed corresponding to persistent acute infections21. While showing clear responses to disease, the potential role of urinary neopterin in the study of life-history traits, however, has just recently been explored. Urinary neopterin levels of semi-free ranging Barbary macaques (Macaca sylvanus), were observed to increase with subject’s age, showing the potential of urinary neopterin measurements in research on immunosenescence in wildlife24.
For wild animal populations, it is suggested that the immune system is permanently challenged compared to captive animals as individuals often harbour multiple infections and are under constant pathogen pressure25. Such challenged immune systems are therefore expected to respond differently to novel and/or acute infections26,27. For example, humans and animals in tropical and rural environments that had elevated levels of chronic parasitic infection exhibited a decrease in vaccine efficacy; this was attributed to the chronic infections leading to an altered immune response28. Additionally, observation of various bird species in wild and captive settings exhibited different immune strategies based on their environments, which may reflect variability in energetic condition and pathogen load26,27,29. Therefore, patterns of immune system activation observed in captive settings might differ from those observed in response to an infection in wild individuals26,27,29. It is therefore possible that detection and quantification of an additional infection via certain immune-related biomarkers might be impossible against the background levels of an already chronically challenged immune system. A comparison of urinary neopterin levels across several studies in humans17,30 indicates that individuals living in environments with lower levels of pathogen prevalence do exhibit lower urinary neopterin levels. Therefore, it is necessary to determine whether an immune-related biomarker validated in captive animals, such as urinary neopterin, can also indicate changes in the immune system of wild animals.
Immune system activation is also a dynamic process with time delays observed between infection and the response of different components of the immune system31. Previous experimental studies measuring neopterin in humans and captive animals using frequent sampling show a temporal pattern with a delay in elevation following exposure, then a sharp, short-term peak measured at the end of the incubation period and before the production of specific antibodies, followed by a slow decline to baseline3,18,32. As the timing and magnitude of the peak varies between individuals and type of infections3,18,21, detecting changes in immune system activation during an acute outbreak in wild populations that often have limited sample availability adds an additional challenge. In this study, we aim to determine whether urinary neopterin levels are a valid non-invasive biomarker of immune system activation through monitoring changes in neopterin levels around a severe respiratory outbreak in a group of habituated wild chimpanzees of the Taï Chimpanzee Project in the Taï National Park, Côte d’Ivoire. We also aim to determine whether urinary neopterin levels correspond to observed signs of illness and can predict likelihood of survival.
Material and Methods
Study site and subjects
Data were collected between February 2009 and September 2010 in Taï National Park, Côte d’Ivoire. The study site is in an evergreen rainforest, which experiences an average annual rainfall of 1800 mm and average temperatures between 24 and 28 °C33,34. The site has two rainy (March-June, September-October) and two dry seasons (July-August, November-February)33.
The habituated South community of chimpanzees is part of the Taï Chimpanzee Project (established in 1979) and has been regularly followed since the 1980s35. At the beginning of the presented study, the group comprised of 37 individuals with 18 males (6 infants, 3 juveniles, 3 adolescents, 6 adults) and 19 females (7 infants, 2 adolescents, 10 adults) (age-sex class see: [35]).
Respiratory Outbreak
In November 2009, a respiratory outbreak of high morbidity was observed in the group (Table 1). Signs of illness (e.g., coughing, lethargy, and nasal discharge)36 were first observed in five individuals on November 26th, and progressively spread throughout the group, peaking on November 30th when 73% (n = 27) of the observed individuals exhibited disease symptoms. The first day when all individuals were observed free of disease symptoms was on December 20th. Across the entire outbreak, 84% of individuals developed severe respiratory symptoms (85% of infants, 100% of juveniles and adolescents, and 75% of adults) (Table 1). Fourteen individuals died from the disease including eight adults (3 males, 5 females) and six infants (2 males, 4 females). Twelve individuals (7 adults, 5 adolescent and juveniles) with particularly severe disease symptoms were treated with a long-acting antibiotic shot (Extencilline, Sanofi-Aventis, France) through remote injection with nine surviving36 (Table 1).
Molecular analyses from necropsy samples of some deceased individuals allowed identification of the human respiratory syncytial virus (HRSV-A) as the major causative agent of the outbreak36. Lung samples obtained from two chimpanzees deceased during the outbreak also showed evidence of co-infection with the human respiratory bacterium Streptococcus pneumoniae, which in combination with a respiratory virus, can lead to higher rates of fatality36.
Sample collection
To investigate whether urinary neopterin levels increased during the respiratory outbreak, urine samples (N = 185) were selected from the biobank collection, taken as part of the long-term health monitoring program1. Samples were selected for each individual based on behavioural observations and veterinary health reports of respiratory disease symptoms and divided into three sampling periods categorized as: (1) pre-outbreak (PRE): from February 2009 until an individual exhibited disease symptoms; (2) outbreak (OB): from the first day an individual showed disease symptoms until the day it was symptom-free; (3) and post-outbreak (POST): from convalescence until September 2010. If available, at least three PRE and POST control samples were included from February 2009 to September 2010 to determine an individual’s baseline asymptomatic (and assumed healthy) neopterin levels. However, not all individuals had equal or available sampling from all three sampling periods either due to early deaths during the outbreak or because sampling of juveniles and infants was not conducted in a systematic way (Table 2). Urine samples were available from 28 individuals; 18 of which had available samples when symptomatic. Males (N = 13) between 2 and 45 years old and females (N = 15) between <1 to 44 years old were tested.
Laboratory methods
Urinary neopterin levels were determined using a commercial competitive neopterin ELISA (Neopterin ELISA, Ref. RE59321, IBL International GmBH, Hamburg, Germany), which had been previously validated for quantifying urinary neopterin in captive chimpanzees23. Urine samples were thawed, vortexed, centrifuged and diluted to 1:400 with the kit provided assay buffer. When measured concentrations were off the linear range of the assay, samples were re-diluted up to 1:1600 until they fell within this range. The ELISA assays were performed following kit instructions and as described in [23]. All samples, standards, and controls were measured in duplicates with results expressed in nmol/L. The inter-assay variation of nine plates was 9.1% for high- and 9.9% for low-quality controls. Intra-assay variation was 6.1% for high- and 8.6% for low-quality controls.
Urinary specific gravity (SG) was measured using a digital handheld refractometer (TEC, Ober-Ramstadt, Germany). The population average for all chimpanzees measured was 1.017. To correct for variation in volume and concentration, final urinary neopterin levels were expressed in urinary neopterin (nmol/L) corrected for SG (corr. SG)37.
Statistical analyses
To explore factors explaining variation in urinary neopterin levels (nmol/L corr. SG), a Linear Mixed Model (LMM)38 was fitted in R v3.3.139 using the R package lme4 v1.1–17 (function lmer)40. The total sample size for these analyses was 185 samples from 28 individuals. The response variable, urinary neopterin levels (nmol/L corr. SG), was log-transformed. The full model included as fixed effects sampling period (PRE, OB, POST), sex, age, collection time, whether the individuals were treated with antibiotics, and whether they survived. Age and collection time were z-transformed to a mean of zero and standard deviation of one. Individual was included as a random intercept effect with random slopes for age and collection time within individual41. To determine the effect of sampling period, the full model was compared to the null model42 lacking this fixed effect, but being otherwise identical, using likelihood ratio tests (R-function anova with argument “test” set as “Chisq”)42. We tested the significance of individual predictors using likelihood ratio tests comparing the full model with models lacking them one at a time41. We assessed model stability by excluding individuals one at a time and comparing model estimates derived from these data with those of the full dataset. This test revealed the model to be stable. To test for collinearity, Variance Inflation Factors (VIF)43 were determined using the R-package car v.3.0-0 (R-function vif)44 applied to a linear model lacking the random effects. This revealed that collinearity (VIF scores <1.8) was not an issue43,45. Pairwise comparisons between sampling period on urinary neopterin levels were conducted using the R-package multcomp v1.4–8 (R-function glht)46 that provides p-values based on Wald approximation.
In a second model, we tested whether changes in urinary neopterin levels differed between individuals who survived or died during the outbreak period, using a reduced dataset because urine samples collected during the POST period and samples collected after antibiotic treatment needed to be excluded32,47,48. Analysis was also restricted to only include samples before the 9th day after showing symptoms, which corresponds to the last day when an animal died after showing symptoms (N = 5). This was to account for the fact that animals who survived exhibited decreasing neopterin levels towards the end of the outbreak and during convalescence, compared to individuals who died earlier during the outbreak when neopterin levels were still high (see Supplementary Fig. S1). The total sample size for this analysis was 86 samples from 26 individuals. In this model, sampling period (PRE and OB) was tested in an interaction with survival as an additional fixed effect. This interaction was added as individuals who did not survive may already have had compromised health before showing symptoms compared to those that survived. Animals that survived may also be able to mount a more appropriate immune response to infection versus animals that did not survive. The LMM included the same fixed effects as the previous model. To determine the effect of survival, the full model was compared to the null model42 lacking survival and its interaction with sampling period, but being otherwise identical, using likelihood ratio tests (R-function anova with argument “test” set as “Chisq”)42. Neither model stability nor collinearity (VIF scores <1.4 for non-interaction terms)43,45 were an issue.
Ethical Statement
This study only made use of non-invasive samples. Data and sample collection and transport was approved by the Ministry of Environment and Forests, Ministry of Research, and Office Ivoirien des Parcs et Réserves in Côte d’Ivoire. All experiments were performed in accordance with relevant guidelines and regulations.
Results
Sampling period significantly predicted urinary neopterin levels (full-null model comparison, likelihood ratio tests: χ2 = 45.450, df = 2, P < 0.001). Urinary neopterin levels in samples collected when individuals were symptomatic during the outbreak (OB) (mean ± SD = 7952.5 ± 3797.9 nmol/L corr. SG) were significantly higher than in samples collected PRE (mean ± SD = 3220.0 ± 3962.9 nmol/L corr. SG) and POST (mean ± SD = 3453.2 ± 2830.8 nmol/L corr. SG) outbreak (Table 3, Fig. 1). The post-hoc comparison showed no significant difference in urinary neopterin levels between PRE and POST outbreak urinary neopterin levels (Table 4). During the OB, urinary neopterin levels (N = 18 individuals) increased from PRE levels by an average of 3.3, and up to 10.4 in one individual who survived (Fig. 1).

Average individual urinary neopterin (nmol/L corr. SG) levels during the study sampling periods (NPRE = 28, NOB = 18, NPOST = 18 individuals) for 185 samples. Cross marks represent individuals who did not survive (N = 10); open circles represent individuals who survived (N = 18). No line is shown for individuals with non-continuous sampling (N = 5).
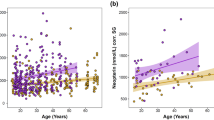
The reduced model showed that animals who died had significantly higher urinary neopterin levels than animals who survived (full-null model comparison, likelihood ratio tests: χ2 = 7.747, df = 2, P < 0.021) (Table 5, Fig. 2). However, there was no significant effect of the interaction between health period and survival (χ2 = 0.891, df = 1, P < 0.345) on urinary neopterin levels. Compared to individuals who survived, individuals who died had higher urinary neopterin levels both before the start of the outbreak (mean ± SD = 4308.5 ± 5414.9 nmol/L corr. SG vs mean ± SD = 2384.7 ± 2014.4 nmol/L corr. SG), and during the beginning of the outbreak (mean ± SD = 9541.9 ± 3351.0 nmol/L corr. SG vs mean ± SD = 9101.2 ± 3004.4 nmol/L corr. SG) (Fig. 2).

Average individual urinary neopterin (nmol/L corr. SG) levels before (NPRE = 26) and during the outbreak (NOB = 11) for chimpanzees who died (N = 8) and those who survived (N = 18) during the outbreak (N = 86 samples). Grey boxes represent those who died during the outbreak; white boxes represent those who survived. The median is indicated by the thick horizontal black line with the interquartile range represented within the boxes. The vertical lines indicate the upper and lower whisker with points as outliers.
Discussion
In this study, we monitored changes in urinary neopterin levels in wild chimpanzees during a respiratory outbreak of human respiratory syncytial virus (HRSV-A), with levels exhibiting a significant increase corresponding to observed respiratory symptoms. The average increase in urinary neopterin levels observed in this group of wild chimpanzees was comparable to results seen in a within-animal comparison of zoo bonobos who developed respiratory symptoms23. No significant differences in urinary neopterin levels were found between samples collected before (PRE) and after (POST) the respiratory outbreak—indicating a return to an individual’s baseline neopterin levels after recovery. The results of this study, therefore, indicate that changes in urinary neopterin levels can be used as an indicator of the activation of the non-specific immune system response, not only in captive, but also in wild great apes.
We furthermore investigated whether animals that died during the outbreak already had elevated neopterin levels before the outbreak, which may be indicative of an already compromised immune system. The interaction between sampling period and survival was not significant, with average urinary neopterin levels being similar during the beginning of the outbreak between those that survived and died. This may be due to the low sample size of animals who died during the outbreak. Therefore, it is possible that the significantly higher neopterin levels of individuals who died was mainly driven by samples taken before the outbreak, indicating an already challenged immune system. Additionally, an analysis of necropsy samples from some individuals that died during the outbreak revealed a co-infection with S. pneumoniae, a bacterium that may lead to chronic asymptomatic infections that can prove fatal once an individual is weakened by an acute infection36. This suggests that, while the degree of increase between individuals who did and did not survive did not differ significantly, elevated urinary neopterin levels before and during the outbreak of those that did not survive may still be indicative of an unfavourable disease outcome as previously described in humans18,49. This was also seen in an experimental study inducing sepsis in baboons (Papio sp.)50, as well as an experimental study exposing rhesus macaques to SIV21.
Although the increase in neopterin levels during the outbreak was significant, there was a large overlap between PRE and OB levels, as well as a high degree of variation in the PRE levels across individuals (Fig. 1). This is in accordance with past studies on human urinary neopterin levels that found that the range of urinary neopterin in active tuberculosis infections overlapped with both those in latent infections, as well as controls without any history of disease48. The variations observed in this study may be the result of an already existing immune challenge faced before the outbreak, such as co-infections36. However, due to limited sample availability during the outbreak (i.e., only six individuals had ≥3 samples during the outbreak), the absolute peak in urinary neopterin may not have been detected within an individual, contributing to the large overlap between urinary neopterin levels of sick and healthy individuals. Therefore, further studies are needed to investigate the causes of variation in urinary neopterin levels across seemingly healthy individuals. Currently, on a practical level, and as shown in a study of captive apes23, it is not possible to define a range of values indicating “healthy” versus “unhealthy” neopterin levels. For the moment, a detection indicating a change in health with elevated levels seems to be only possible by performing a within-subject comparison51,52,53.
How energy is allocated varies throughout an individual’s lifetime, with life-history models predicting a trade-off between promoting growth, maintaining health, and maximizing reproduction54,55,56. In recent years, how the immune system may play a role in the evolution of life-history traits has attracted considerable interest1,57,58. Specifically, investigations into the effects of sociality on variation in immune system activation and, ultimately, lifetime reproductive fitness, has given rise to the field of ecological immunology2. Therefore, being able to accurately measure and monitor variation in an individual’s immune system activation throughout an animal’s lifetime in a natural environment can provide valuable insights on the trade-offs of immune activation in the context of ecoimmunology23,59,60. Increasing evidence suggests that individual health is a key factor in mediating links between sociality, fitness, and disease susceptibility61 with social factors also, in turn, influencing immune functions62,63,64. In particular, there has been evidence showing an altered immune response following certain stressors leading to a suppression of T-cell function64. For example, suppressed urinary neopterin levels were observed to correspond with periods of psychological stress in medical students63. In this context, the non-invasive measurement of neopterin within and between wild populations, in combination with biomarkers of energetic condition, stress and reproductive system activation, will lead to a deeper understanding of these life-history trade-offs23,65.
While this study validated urinary neopterin as a biomarker of immune system activation during a severe respiratory infection, this method may have additional practical implications for the field of wildlife and conservation biology. In particular, it may aid in monitoring non-lethal, chronic infections of low intensity such as malaria in great apes, which often lack obvious sickness behaviors66. Neopterin has also been shown in humans to increase after vaccination32,47. And, given the threat of infectious diseases in decimating wildlife populations1,36,67, it therefore has potential use in non-invasively detecting the effectiveness of vaccinations and treatments in wild animals.
In conclusion, the biomarker urinary neopterin allowed for the monitoring of immune system activation in a wild chimpanzee group during a severe respiratory outbreak. Until factors leading to high across individual variability in asymptomatic individuals have been identified, longitudinal sampling is required to determine an individual’s baseline levels and to account for potential variations that occur due to natural temporal fluctuations and seasonality. This is particularly important when monitoring wild individuals who most likely harbour chronic low-level infections or are asymptomatic carriers of various pathogens. Additionally, measuring urinary neopterin in wild populations, in combination with other biomarkers of health and condition, will increase our understanding on variations in life-history strategies and contribute towards the growing field of ecoimmunology.
Data Availability
The R code and datasets analysed during the current study are available from the corresponding author on reasonable request.
References
Leendertz, F. H. et al. Pathogens as drivers of population declines: The importance of systematic monitoring in great apes and other threatened mammals. Biol. Conserv. 131, 325–337 (2006).
Demas, G. E. & Nelson, R. Ecoimmunology. (Oxford University Press, 2012).
Higham, J. P. et al. Evaluating noninvasive markers of nonhuman primate immune activation and inflammation. Am. J. Phys. Anthropol. 158, 673–684 (2015).
Behringer, V. & Deschner, T. Non-invasive monitoring of physiological markers in primates. Horm. Behav. 91, 3–18 (2017).
Higham, J. P. Field endocrinology of nonhuman primates: past, present, and future. Horm. Behav. 84, 145–155 (2016).
Anestis, S. F. Hormones and social behavior in primates. Evol. Anthropol. Issues News Rev. 19, 66–78 (2010).
Danish, L. M., Heistermann, M., Agil, M. & Engelhardt, A. Validation of a novel collection device for non-invasive urine sampling from free-ranging animals. Plos One 10, e0142051 (2015).
Kaur, T. & Huffman, M. A. Descriptive urological record of chimpanzees (Pan troglodytes) in the wild and limitations associated with using multi-reagent dipstick test strips. J. Med. Primatol. 33, 187–196 (2004).
Leendertz, S. A. J. et al. A longitudinal study of urinary dipstick parameters in wild chimpanzees (Pan troglodytes verus) in Côte d’Ivoire. Am. J. Primatol. 72, 689–698 (2010).
MacIntosh, A. J. J., Huffman, M. A., Nishiwaki, K. & Miyabe-Nishiwaki, T. Urological screening of a wild group of Japanese Macaques (Macaca fuscata yakui): Investigating trends in nutrition and health. Int. J. Primatol. 33, 460–478 (2012).
Weary, D. M., Huzzey, J. M. & von Keyserlingk, M. A. G. Board-invited review: Using behavior to predict and identify ill health in animals. J. Anim. Sci. 87, 770–777 (2009).
MacIntosh, A. J. J., Alados, C. L. & Huffman, M. A. Fractal analysis of behaviour in a wild primate: behavioural complexity in health and disease. J. R. Soc. Interface 8, 1497–1509 (2011).
Duboscq, J., Romano, V., Sueur, C. & MacIntosh, A. J. J. Network centrality and seasonality interact to predict lice load in a social primate. Sci. Rep. 6 (2016).
Gillespie, T. R. Noninvasive assessment of gastrointestinal parasite infections in free-ranging primates. Int. J. Primatol. 27, 1129–1143 (2006).
Berdowska, A. & Zwirska-Korczala, K. Neopterin measurement in clinical diagnosis. J. Clin. Pharm. Ther. 26, 319–329 (2001).
Eisenhut, M. Neopterin in diagnosis and monitoring of infectious diseases. J. Biomark. 2013, 1–10 (2013).
Fuchs, D., Weiss, G. & Wachter, H. Neopterin, biochemistry and clinical use as a marker for cellular immune reactions. Int. Arch. Allergy Immunol. 101, 1–6 (1993).
Murr, C., Widner, B., Wirleitner, B. & Fuchs, D. Neopterin as a marker for immune system activation. Curr. Drug Metab. 3, 175–187 (2002).
Denz, H. et al. Value of urinary neopterin in the differential diagnosis of bacterial and viral infections. J. Mol. Med. 68, 218–222 (1990).
Prat, C. et al. Procalcitonin and neopterin correlation with aetiology and severity of pneumonia. J. Infect. 52, 169–177 (2006).
Dittmer, U. et al. Repeated exposure of rhesus macaques to low doses of simian immunodeficiency virus (SIV) did not protect them against the consequences of a high-dose SIV challenge. J. Gen. Virol. 76, 1307–1315 (1995).
Heistermann, M. & Higham, J. P. Urinary neopterin, a non-invasive marker of mammalian cellular immune activation, is highly stable under field conditions. Sci. Rep. 5 (2015).
Behringer, V., Stevens, J. M. G., Leendertz, F. H., Hohmann, G. & Deschner, T. Validation of a method for the assessment of urinary neopterin levels to monitor health status in non-human-primate species. Front. Physiol. 8 (2017).
Müller, N., Heistermann, M., Strube, C., Schülke, O. & Ostner, J. Age, but not anthelmintic treatment, is associated with urinary neopterin levels in semi-free ranging Barbary macaques. Sci. Rep. 7, 41973 (2017).
Fair, P. A. et al. The environment as a driver of immune and endocrine responses in dolphins (Tursiops truncatus). Plos One 12, e0176202 (2017).
Matson, K. D. Are there differences in immune function between continental and insular birds? Proc. R. Soc. B Biol. Sci. 273, 2267–2274 (2006).
Mendes, L., Piersma, T., Hasselquist, D., Matson, K. D. & Ricklefs, R. E. Variation in the innate and acquired arms of the immune system among five shorebird species. J. Exp. Biol. 209, 284–291 (2006).
LaBeaud, A. D., Malhotra, I., King, M. J., King, C. L. & King, C. H. Do antenatal parasite infections devalue childhood vaccination? PLoS Negl. Trop. Dis. 3, e442 (2009).
Buehler, D. M., Piersma, T. & Irene Tieleman, B. Captive and free-living red knots Calidris canutus exhibit differences in non-induced immunity that suggest different immune strategies in different environments. J. Avian Biol. 39, 560–566 (2008).
Filteau, S. M., Raynes, J. G., Simmank, K. & Wagstaff, L. A. Vitamin A status does not influence neopterin production during illness or health in South African children. Br. J. Nutr. 80, 75 (1998).
Fenton, A., Lello, J. & Bonsall, M. Pathogen responses to host immunity: the impact of time delays and memory on the evolution of virulence. Proc. R. Soc. B Biol. Sci. 273, 2083–2090 (2006).
Mendy, J. et al. C-reactive protein, neopterin and Beta2 microglobulin levels pre and post TB treatment in The Gambia. BMC Infect. Dis. 16 (2016).
Doran, D. Influence of seasonality on activity patterns, feeding behavior, ranging, and grouping patterns in Taï chimpanzees. Int. J. Primatol. 18, 183–206 (1997).
Wittig, R. M. Taï Chimpanzees. In Encyclopedia of Animal Cognition and Behavior (eds Vonk, J. & Shackelford, T.) 1–7 (Springer International Publishing, https://doi.org/10.1007/978-3-319-47829-6_1564-1 2018).
Boesch, C. & Boesch-Achermann, H. The Chimpanzees of the Taï Forest: Behavioral Ecology and Evolution. (Oxford University Press, 2000).
Köndgen, S. et al. Evidence for Human Streptococcus pneumoniae in wild and captive chimpanzees: A potential threat to wild populations. Sci. Rep. 7 (2017).
Miller, R. C. Comparison of specific gravity and creatinine for normalizing urinary reproductive hormone concentrations. Clin. Chem. 50, 924–932 (2004).
Baayen, R. H. Analyzing Linguistic Data. (Cambridge University Press, 2008).
R Core Team. R: A Language and Environment for Statistical Computing. (R Foundation for Statistical Computing, 2016).
Bates, D., Mächler, M., Bolker, B. & Walker, S. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 67 (2015).
Barr, D. J., Levy, R., Scheepers, C. & Tily, H. J. Random effects structure for confirmatory hypothesis testing: keep it maximal. J Mem Lang 68 (2013).
Forstmeier, W. & Schielzeth, H. Cryptic multiple hypotheses testing in linear models: overestimated effect sizes and the winner’s curse. Behav. Ecol. Sociobiol. 65, 47–55 (2011).
Field, A. Discovering Statistics Using SPSS. (Sage Publications, 2009).
Fox, J. & Weisberg, S. An {R} Companion to Applied Regression. (Sage, 2011).
Quinn, G. P. & Keough, M. J. Experimental Design and Data Analysis for Biologists. (Cambridge University Press, 2002).
Hothorn, T., Bretz, F. & Westfall, P. Simultaneous inference in general parametric models. Biom. J. 50, 346–363 (2008).
de Zeeuw, J. et al. Serum levels of neopterin during antimicrobial treatment for Mycobacterium ulcerans infection. Am. J. Trop. Med. Hyg. 89, 498–500 (2013).
Eisenhut, M. et al. Determination of urinary neopterin/creatinine ratio to distinguish active Tuberculosis from latent Mycobacterium tuberculosisinfection. J. Biomark. 2016, 1–6 (2016).
Ruokonen, E., Ilkka, L., Niskanen, M. & Takala, J. Procalcitonin and neopterin as indicators of infection in critically ill patients. Acta Anaesthesiol Scand 46, 398–404 (2002).
Redl, H., Schlag, G., Tögel, E., Assicot, M. & Bohuon, C. Procalcitonin release patterns in a baboon model of trauma and sepsis: Relationship to cytokines and neopterin:. Crit. Care Med. 28, 3659–3663 (2000).
Diamondstone, L. S. et al. Factors influencing serum neopterin and β2-microglobulin levels in a healthy diverse population. J. Clin. Immunol. 14, 368–374 (1994).
Reibnegger, G. et al. Approach to define “normal aging” in man. Immune function, serum lipids, lipoproteins and neopterin levels. Mech. Ageing Dev. 46, 67–82 (1988).
Spencer, M. E. et al. Serum levels of the immune activation marker neopterin change with age and gender and are modified by race, BMI, and percentage of body fat. J. Gerontol. A. Biol. Sci. Med. Sci. 65A, 858–865 (2010).
Perrin, N. & Sibly, R. M. Dynamic models of energy allocation and investment. Annu. Rev. Ecol. Syst. 24, 379–410 (1993).
Stearns, S. C. Life history evolution: successes, limitations, and prospects. Naturwissenschaften 87, 476–486 (2000).
Bergstrom, M. L., Emery Thompson, M., Melin, A. D. & Fedigan, L. M. Using urinary parameters to estimate seasonal variation in the physical condition of female white-faced capuchin monkeys (Cebus capucinus imitator). Am. J. Phys. Anthropol. 163 (2017).
Nunn, C. L. & Altizer, S. M. Infectious diseases in primates: behavior, ecology and evolution. (Oxford University Press, 2006).
Urlacher, S. S. et al. Tradeoffs between immune function and childhood growth among Amazonian forager-horticulturalists. Proc. Natl. Acad. Sci. 115, E3914–E3921 (2018).
French, S. S., Moore, M. C. & Demas, G. E. Ecological immunology: The organism in context. Integr. Comp. Biol. 49, 246–253 (2009).
Viney, M. E., Riley, E. M. & Buchanan, K. L. Optimal immune responses: immunocompetence revisited. Trends Ecol. Evol. 20, 665–669 (2005).
Kappeler, P. M., Cremer, S. & Nunn, C. L. Sociality and health: impacts of sociality on disease susceptibility and transmission in animal and human societies. Philos. Trans. R. Soc. B Biol. Sci. 370, 20140116–20140116 (2015).
Cohen, S., Janicki-Deverts, D., Turner, R. B. & Doyle, W. J. Does hugging provide stress-buffering social support? A study of susceptibility to upper respiratory infection and illness. Psychol. Sci. 26, 135–147 (2015).
Dunbar, P. R., Hill, J. & Neale, T. J. Urinary neopterin quantification indicates altered cell-mediated immunity in healthy subjects under psychological stress. Aust. N. Z. J. Psychiatry 27, 495–501 (1993).
Maes, M. Evidence for an immune response in major depression: A review and hypothesis. Prog. Neuropsychopharmacol. Biol. Psychiatry 19, 11–38 (1995).
Emery Thompson, M. Energetics of feeding, social behavior, and life history in non-human primates. Horm. Behav. 91, 84–96 (2017).
De Nys, H. M., Löhrich, T., Wu, D., Calvignac-Spencer, S. & Leendertz, F. H. Wild African great apes as natural hosts of malaria parasites: current knowledge and research perspectives. Primate Biol. 4, 47–59 (2017).
Grützmacher, K. et al. Human quarantine: Toward reducing infectious pressure on chimpanzees at the Taï Chimpanzee Project, Côte d’Ivoire. Am. J. Primatol., 22619, https://doi.org/10.1002/ajp.22619 (2017).
Wu, D., Behringer, V., Wittig, R. M., Leendertz, F. & Deschner, T. Urinary neopterin increases during a respiratory outbreak in wild chimpanzees (Taï National Park, Côte d’Ivoire). 88 (2017).
Acknowledgements
We thank the Ministry of Environment and Forests, Ministry of Research, Office Ivoirien des Parcs et Réserves, and Centre Suisse de Recherche Scientifique in Côte d’Ivoire for their logistical support; and the Taї Chimpanzee Project field assistants and veterinarians for their help in the field. Thank you to Vera Schmeling and Janette Gleiche for lab assistance; and Frauke Olthoff and Anja Zschoke for their technical support. Thank you also to Dr. Gaëlle Bocksberger for R coding help; Dr. Lars Kulik for R statistical advice; and Dr. Roger Mundry for R statistical advice and comments on the manuscript. We also thank members of the DFG-research group FOR2136 “Sociality and Health in Primates” for their feedback and discussion. This research was supported by the Deutsche Forschungsgemeinschaft (DFG) and conducted as part of the research group “Sociality and Health in Primates” (FOR2136, DE 1135/2-1 and LE1813/10-1). A preliminary version of this work was presented previously in August 2017 at the 7th European Federation for Primatology (Strasbourg, France) conference as part of the “Sociality and Health in Primates” symposium with the abstract published in Folia Primatologica68.
Author information
Authors and Affiliations
Contributions
T.D., V.B., F.H.L. and R.M.W. designed the study and participated in writing the manuscript. D.F.W. took the lead in writing, created all figures, and participated in laboratory work. V.B., T.D. and D.F.W. participated in data analysis. T.D. supervised the study. All authors contributed to and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Wu, D.F., Behringer, V., Wittig, R.M. et al. Urinary neopterin levels increase and predict survival during a respiratory outbreak in wild chimpanzees (Taï National Park, Côte d’Ivoire). Sci Rep 8, 13346 (2018). https://doi.org/10.1038/s41598-018-31563-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-31563-7
This article is cited by
-
Neopterin Levels in Bonobos Vary Seasonally and Reflect Symptomatic Respiratory Infections
EcoHealth (2023)
-
Urinary neopterin reflects immunological variation associated with age, helminth parasitism, and the microbiome in a wild primate
Scientific Reports (2022)
-
Urinary neopterin of wild chimpanzees indicates that cell-mediated immune activity varies by age, sex, and female reproductive status
Scientific Reports (2021)
-
Social and sexual behaviors predict immune system activation, but not adrenocortical activation, in male rhesus macaques
Behavioral Ecology and Sociobiology (2021)
-
Detection of neopterin in the urine of captive and wild platyrrhines
BMC Zoology (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
