
Abstract
National antimicrobial usage and prescription patterns during the 12 years from 2002 to 2013 were analyzed using the National Health Insurance Service-National Sample Cohort. Antimicrobial usage was analyzed by major illness, sex, age, area of residence, income rank, diagnosis, and type of medical institution for each year. Total antimicrobial prescriptions increased from 15.943 daily defined dose (DDD)/1,000 inhabitants/day in 2002 to 24.219 in 2013. In 2013, 72% of total prescriptions were administered in clinics. Antimicrobials were most frequently prescribed to children younger than 10 years, followed by adults aged 70 years or older and those aged 60–69 years. Penicillins and cephems were the most popular classes of antimicrobial used. In 2013, 48% of total antibiotic usage (11.683 DDD/1,000 inhabitants/day) was due to respiratory diseases. After the Korean government has implemented a series of healthcare policies, antibiotic prescription decreased for the treatment of upper respiratory infection, the causative agents are mostly viruses.
Similar content being viewed by others

Introduction
Although antibiotics have saved the lives of millions of people worldwide since the discovery of penicillin in 1928, the emergence of antibiotic resistance in bacteria is a serious global challenge. Antibiotic resistance develops when bacteria adapt and grow in the presence of antibiotics. Because the development of resistance is linked to how often antibiotics are used, misuse and over-use of antibiotics hasten the development of bacterial drug resistance, rendering existing antibiotics less effective1,2,3. Although infection by multidrug-resistant bacteria poses a grave threat to public health and wellbeing through subsequent increases in hospital stays, medical costs, and mortality4,5,6, the development of new antimicrobials is a practically challenging task.
Because bacterial resistance is increasing and the development of new antimicrobial is declining, securing the efficacy of existing antibiotics for long periods of time is the key to solving the antimicrobial resistance problem. In other words, the key is to suppress the occurrence of bacterial resistance in existing antibiotics. In 2015, World Health Organization (WHO) adopted a global action plan on antimicrobial resistance, which declared it as an urgent public health concern and emphasized prudent antimicrobial prescriptions in human and animal health, based on evidence and the current epidemiology1.
Although the prevalence of antimicrobial resistance in Korea is higher than that in advanced countries such as the United States and Europe7,8, studies on the changes in antimicrobial usage patterns, which drive antimicrobial management policies, were limited in terms of research institutions, regions, and medical facilities9,10,11,12,13,14,15,16. The aim of this study was to analyze antimicrobial usage and prescription patterns at the national level in Korea during the 12-year period from 2002 to 2013. We expect the findings to help identify the major groups in need of intervention and provide grounds for developing public health policies to manage antimicrobial usage.
Methods
Analysis of antimicrobial usage and prescription patterns
We analyzed national antimicrobial usage and prescription patterns during the 12 years from 2002 to 2013 using the National Health Insurance Service-National Sample Cohort (NHIS-NSC)17. The data obtained from the national health database consisted of a national sample of 1,025,340 people (males: 513,258, females: 512,082), accounting for 2.2% of the total Korean population as of the 2002 census.
Systematic stratified sampling was used based on sex, age, and type of health insurance, and the data include socioeconomic variables (e.g., area of residence, income rank, disability), mortality, healthcare use (e.g., medical bills, details of care, diagnosis, and prescription), and health examination data.
Antimicrobials were classified as penicillins, cephems, carbapenems, fluoroquinolones, aminoglycosides, tetracyclines, macrolides, glycopeptides, or folate path inhibitors for analysis. Antimicrobial usage was analyzed by income rank (5 ranks), which was determined using insurance bills per household, by medical institution (general hospital, hospital, long-term care hospital, clinic), and by region (17 cities and provinces). Following medical law in Korea, we classified medical institutions as clinics if they had fewer than 30 beds, as hospitals if they had more than 30 beds, and as general hospitals if they had more than 100 beds. A long-term care hospital was defined as a nursing hospital if it was intended for patients with geriatric or chronic diseases or patients who require postoperative recovery.
Upper respiratory infection (URI) was included as a major illness for analysis of antimicrobial usage patterns. URI, which involves viral pathogens in most cases, rarely requires antimicrobials for treatment and is associated with antimicrobial abuse. Bacterial pneumonia and urinary tract infections require antimicrobial prescriptions, and the incidence of these diseases is increasing with the growing elderly population. The major illnesses analyzed in this study, according to the Korean Standard Classification of Diseases, were respiratory diseases (code J) and genitourinary diseases (code N); more specifically, we analyzed URIs (J00-J06), pneumonia (J13-J17), and urinary tract infections (N10-N12, N136, N151, N159, N20-N21, N30, N34, N390).
Because the dose, form, and frequency of use vary across antimicrobial products, the daily defined dose (DDD) and yearly antimicrobial usage by active ingredient were calculated as follows to measure standardized usage.
This describes the number of people (per a population of 1,000) who use an antimicrobial every day. As an example, 10 DDD per 1,000 inhabitants per day means that 1% of the population, on average, might receive a certain drug or group of drugs daily. Antimicrobial usage was analyzed by sex, age, area of residence, income rank, diagnosis, and type of medical institution for each year.
Statistical analysis
Trend tests were performed to determine potential differences in antimicrobial usage by year, and linear mixed models using group, time, and group-by-time as fixed effects were used to identify potential differences in the yearly patterns of antimicrobial usage in relation to general characteristics. Data were organized and analyzed using SAS v9.4 software (SAS Institute Inc., Cary, NC, USA).
Results
Antimicrobial prescriptions
Total antimicrobial prescriptions in Korea increased from 15.943 DDD/1,000 inhabitants/day in 2002 to 24.219 in 2013 (Table 1, P < 0.001). By class, penicillins were the most frequently prescribed, followed by cephems, including cephalosporin and cephamycin (Fig. 1). No changes in penicillin prescription patterns occurred over the course of the 12-year period (P = 0.661). Cephem, carbapenem, fluoroquinolone, tetracycline, macrolide, and glycopeptide prescriptions increased, and aminoglycoside and folate path inhibitor prescriptions decreased (Table 1, P < 0.001).

Average antimicrobial prescription according to class of antimicrobials from 2002 to 2013 (DID: Daily Defined Dose/1,000 inhabitants/days).
Data from 2013 were examined to identify the antimicrobials most frequently prescribed in recent years. The total penicillin prescription rate was 7.768 DDD/1,000 inhabitants/day, and antimicrobials containing amoxicillin were the most frequently used. Amoxicillin was popular in 2002, but amoxicillin-clavulanate was more frequently used by 2013 (in DDD/1,000 inhabitants/day: amoxicillin 5.214, amoxicillin-clavulanate 1.777 in 2002; amoxicillin 2.250, amoxicillin-clavulanate 4.943, amoxicillin-sulbactam 0.394 in 2013). Among the cephems, cefaclor (3.222) was the most frequently prescribed, followed by cefuroxime (0.837), and cephradine (0.438). These three drugs accounted for 61% of all cephem prescriptions (7.211). Among fluoroquinolones, levofloxacin (0.978) was the most frequently prescribed, followed by ciprofloxacin (0.675), and ofloxacin (0.594). These three drugs accounted for 89% of the total fluoroquinolone prescriptions (2.565). The total macrolide prescriptions equaled 3.392 DDD/1,000 inhabitants/day, consisting of clarithromycin (1.896), roxithromycin (1.301), and azithromycin (0.193). For tetracycline, aminoglycoside, folate path inhibitor, carbapenem, and glycopeptide, 1.334, 0.807, 0.14, 0.055, and 0.053 DDD/1,000 inhabitants/day were prescribed, respectively.
Regarding the types of medical institutions, the vast majority of antimicrobials were prescribed in clinics, followed by general hospitals, hospitals, and long-term care hospitals (Fig. 2). In 2013, 72% of total prescriptions occurred in clinics (Table 2). Among clinics, penicillins (6.378 DDD/1,000 inhabitants/day) were the most frequently prescribed antimicrobial, followed by cephems (4.796), macrolides (2.639), and fluoroquinolones (1.536). In general hospitals, cephems (1.443) were the most frequently prescribed antimicrobial, followed by fluoroquinolones (0.767), penicillins (0.635), and macrolides (0.488) (Table 2). Antimicrobial prescriptions of all classes, except for that of penicillin in clinics (P = 0.111), increased every year regardless of medical institution (Table 2).

Average antimicrobial prescription according to types of medical institutions from 2002 to 2013 (DID: Daily Defined Dose/1,000 inhabitants/days).
Antimicrobial prescriptions by sociodemographic features
No difference was observed in the use of antimicrobials according to gender (Fig. 3, P = 0.54), with antimicrobial prescription increasing every year in both males and females (Fig. 3, P < 0.001). The use of antimicrobials varied with age group (Fig. 4, P < 0.001). Antimicrobials were most frequently prescribed to children younger than 10 years, followed by adults aged 70 years or older and those aged 60–69 years (Fig. 4). In 2013, penicillins were the most frequently prescribed antimicrobial in children younger than 10 years, followed by cephems and macrolides, whereas cephems were the most frequently prescribed antimicrobial in adults aged 70 years or older, followed by fluoroquinolones, penicillins, and macrolides (data not shown).

Antimicrobial prescription according to sex from 2002 to 2013.

Antimicrobial prescription according to age group from 2002 to 2013.
When antimicrobial prescription patterns were analyzed by stratifying the income levels of the sample into five groups (from the upper 20th percentile to the lower 20th percentile), no difference was found according to income level (Fig. 5, P = 0.65), with antimicrobial prescriptions increasing every year in all five income groups (Fig. 5, P < 0.001). Areas of residence were classified into 17 cities and provinces using the subjects’ addresses on resident registrations to examine differences in antimicrobial prescription patterns across regions. Antimicrobial prescriptions increased in all cities and provinces (P < 0.001), without regional differences (P = 0.47, data not shown).

Antimicrobial prescription according to income levels of the sample into five groups (from upper 20 percentiles to lower 20 percentiles) from 2002 to 2013.
Antimicrobial prescriptions by major illness
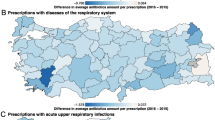
For major illness prescribed for antimicrobials, more than half of all antimicrobial agents used were due to respiratory diseases (Fig. 6). Antimicrobial prescriptions for respiratory diseases increased every year (Table 3, P < 0.001). In 2013, 48% (11.683 DDD/1,000 inhabitants/day) of total antibiotic usage was due to respiratory diseases. Although not statistically significant, antimicrobial prescriptions for URIs decreased from 4.9 DDD/1,000 inhabitants/day in 2002 to 3.625 in 2013 (P = 0.109, Table 3). Antimicrobial prescriptions for genitourinary diseases, including urinary tract infections, increased every year (Table 3, P < 0.001).

Average antimicrobial prescription according to major illness from 2002 to 2013 (DID: Daily Defined Dose/1,000 inhabitants/days; URI: upper respiratory tract infection).
By class, penicillins were the most frequently prescribed antimicrobial for respiratory diseases (5.281 DDD/1,000 inhabitants/day) in 2013, followed by cephems (3.113), macrolides (2.307), and fluoroquinolones (0.697), and similar trend was observed for URIs. For genitourinary diseases, fluoroquinolones were the most frequently prescribed antibiotics (0.796), followed by cephems (0.488), and a similar trend was observed for urinary tract infections.
When antibiotic use was compared between 2013 and 2002, cephem, macrolide and fluoroquinolone use increased, but penicillin use was not increased for respiratory diseases. For genitourinary diseases, prescription of cephem, macrolide, penicillin and fluoroquinolone increased (see Table 3).
Discussion
This study explored the changes of antimicrobial usage in Korea from 2002 to 2013 through analyzing the NHIS-NSC data using DDD developed by the WHO for drug statistics methodology.
Antimicrobial resistance in human pathogens shows substantial geographic differences across the globe. Although antimicrobial resistance remains low in Northern European countries, it is high in Southern European, Latin American and Asian countries. In Asia, extended spectrum β-lactamase (ESBL)-producing Enterobacteriaceae are of concern and are increasing. In 2009 and 2010, 28 percent of Enterobacteriaceae isolated from the patients with urinary tract infections in 11 countries were ESBL producers18. In China, in 2011, ESBL-producing E. coli accounted for 71 percent of E. coli isolates, and more than half of K. pneumoniae strains produced ESBL19. Infections with carbapenem-resistant Enterobacteriaceae are increasingly reported from healthcare facilities, not only in developed countries20, but also in low- and middle income countries. Treatment for carbapenem-resistant Enterobacteriaceae is much more complicated than ESBL-producing stains because of limited treatment options.
Between 2000 and 2010, global consumption of antibiotic drugs increased by 36%21. There is a high variability of antimicrobial consumption across countries. Among the Organisation for Economic Co-operation and Development (OECD) countries, Chile and Netherlands reported the lowest volume (9.4 and 11.4 DDD/1,000 inhabitants/day, respectively) and Greece and Italy reported 30.1 and 34.9 DDD/1,000 inhabitants/day, respectively in 201322. Antimicrobial use in Japan was 14.7 in 2009 and 15.8 DDD/1,000 inhabitants/day23. Korea remains a country with heavy antimicrobial usage16,24; its 2013 national average (28.4 DDD/1,000 inhabitants/day) exceeds the OECD average (20.4 DDD/1,000 inhabitants/day)22. New systems were introduced in Korea upon the turn of the 21st century to increase the quality of medicine and reduce the use of antimicrobials25,26, including the separation of dispensing and prescribing in 2000, drug-use assessment (including antimicrobials) in 2001, public reporting of the rate of antibiotics use for URI in 2006, and assessment of antimicrobial use for surgical prophylaxis27.
The changing patterns of antibiotics usage in Korea have been reported from the past28. A study that compared antimicrobial usage in Korea before and after the separation of dispensing and prescribing in July 2000 reported that antimicrobial usage before the separation was 28.1 DDD/1,000 inhabitants/day in 1998 and 30.8 in 1999, which decreased to 19.8 in 2001 and 17 in 2002 after the separation25. Studies that analyzed antimicrobial usage after the separation of dispensing and prescribing drugs using health insurance found that usage was 23.62 in 200411. A previous study, ‘Annual Products of Medicine in 2008′, analyzed the cost and amounts of antibiotics produced and compared them with previous data. The cost and amounts of antibiotics are indirect parameters of drug utilization, and that study did not consider imported antibiotics. In this study, the DDD was used because it facilitates the presentation and comparison of drug consumption statistics at international, national and regional levels. Although drug consumption can be measured in cost, number of units, number of prescriptions or the physical quantity of drugs, these variables can vary between regions and countries over time. Because of such limitation in comparisons of drug consumption at an international level, a technical unit of measurement, DDD, is recommended by the WHO to measure drug utilization in countries29. Moreover, the NHIS-NSC data used in this study were claim data that could be used to estimate nationwide antibiotics usage directly14.
This study found that antimicrobial usage increased, from 15.943 DDD/1,000 inhabitants/day in 2002 to 24.219 in 2013. Analysis of usage by year showed a sharp increase from 2002 to 2010, but had been consistent since 2010. Since antimicrobial usage is increasing despite the enforcement of relevant policies, it can be suspected that these policies are not effective enough, or that the growth of the elderly population has increased antimicrobial usage. However, the rate at which antibiotics use increases is declining in recent years, and it seems that the antibiotic policy is beginning to show its effects.
URI, a disease that encompasses simple colds, allergic rhinitis, middle ear infections, and pharyngitis, is viral in most cases, and antimicrobials are rarely required, suggesting that antimicrobial usage for this particular disease should be managed closely30. Although changing prescribing behaviors can be difficult, guidelines exist for acute rhinosinusitis31, acute uncomplicated bronchitis32, and pharyngitis33, and proven evidence-based methods can be used to optimize antibiotic therapy in outpatient settings34,35,36.
Over the last decade the Korean government has implemented a series of healthcare policies directed to URI consisting of drug utilization review in the outpatient service in 2001 and public reporting of the rate of antibiotics use for URI in 2006. As a result of government policy for URI, antimicrobial usage for URIs tended to decline, though the trend was not statistically significant, from 4.9 DDD/1,000 inhabitants/day in 2002 to 3.625 in 2013. The proportion of total antimicrobial usage for acute URIs decreased from 30% in 2002 to 14% in 2013. In particular, antimicrobials prescribed for URI decreased after public reporting of the rate of antibiotics use for URI in 2006 (4.982 in 2005 and 4.000 in 2006).
Perception change of primary physician and a public campaign for ‘appropriate antibiotic use’ could contribute to decrease of antimicrobial usage. Studies using clinical scenarios involving the common cold or standard patients showed that physicians’ responses in favor of antibiotic prescription in acute URTIs fell from 75.0% in 1991 to 54.7% in 2003 and to 27.2% in 2010 although the clinical cases and study subjects differed between the studies37,38,39,40. A public campaign for ‘appropriate antibiotic use’ organized by the Korean Society of Infectious Diseases and the Korean Society for Chemotherapy, and sponsored by the Korea CDC, was launched in Korea in 201141.
In 2008, the use of antimicrobials increased significantly. After the implementation of public reporting in 2006, diagnostic coding which has not been designated for antibiotic use evaluation were increased significantly. For example, the most common respiratory tract infections was J03 acute tonsillitis in 2005 but changed to J20 acute bronchitis in 2009. Increased use of antimicrobials in 2008 may be explained in part by diagnostic shift in the outpatient setting although the cause of increasing trends in total antimicrobial usage needs to be determined27.
The use of aminoglycosides decreased from 1.494 in 2002 (10% of total antimicrobial usage) to 0.807 in 2013 (3% of total antimicrobial usage). Although amoxicillin was the most popular penicillin in 2002, amoxicillin-clavulanate was more popular in 2013, suggesting a preference for combined drugs to overcome bacterial resistance. Whereas the use of penicillins did not increase, the use of cephems increased more than two-fold over our study period. Cephem use was only half of that of penicillins in 2002, but prescriptions increased to a level comparable with that of penicillins in 2013. The most frequently used cephem was cefaclor; its usage in 2013 was 3.222 DDD/1000 inhabitants/day, which accounted for half of the total cephem usage (7.211). The fact that the use of cefaclor, a second-generation cephem, exceeded that of oral third-generation cephems such as cefixime and cefpodoxime (though their use increased as well) could be related to insurance policies that do not cover primary treatment with third-generation cephems. Furthermore, the side effects (e.g., diarrhea) of amoxicillin-clavulanate, which is used to overcome resistance, could contribute to the preference for cefaclor. Macrolide and fluoroquinolone prescriptions also increased, and prescriptions for clarithromycin, levofloxacin, and ciprofloxacin increased by particularly high degrees. Use of sulfamethoxazole-trimethoprim, a drug typically used to treat urinary tract infections, declined, possibly due to concerns of resistance of Escherichia coli—the most common pathogen in urinary tract infections.
Regarding age, antimicrobials were most heavily used in children under the age of 10, followed by adults aged 70 years or older and those aged 60–69 years. Penicillins were the most popular antimicrobial among children. Fluoroquinolones are not used in children due to the potential side effects. Cephems were preferred over penicillins among adults aged 20 years or older, and cephems and fluoroquinolones were preferred over penicillins among adults aged 70 years or older in 2013.
In this study analyzed all antimicrobial used, there was no difference was found according to income level. Recent study for antimicrobial used for acute URIs found that income level was negatively correlated with prescription rate and suggested demand factors as well as supply factors contributed antibiotic overuse15. We hypothesize that demand factors have a greater impact on mild illnesses such as acute URIs.
In 2013, 72% of total prescriptions occurred in clinics. This is attributable to the fact that a greater number of patients are treated in clinics than in other types of medical institutions. Thus, antimicrobial usage in clinics should be closely monitored.
In conclusion, antimicrobial usage increased in Korea from 2002 to 2013, with 70% of the prescriptions made in clinics, and penicillins and cephems being the most popular classes of antimicrobials. In 2013, 48% of all antimicrobials were prescribed for respiratory diseases, and antimicrobial prescriptions for URIs are declining. On the cusp of a post-antibiotics era, monitoring antimicrobial use can be an important strategy to prolong the activities of existing antimicrobials.
Data availability
The datasets generated during the current study are available from the corresponding author on reasonable request.
References
World Health Organization. Global action plan on antimicrobial resistance (2015).
Centres for Disease Control and Prevention, (US). In Antibiotic resistance threats in the United States, 2013 (Centres for Disease Control and Prevention, US Department of Health and Human Services, 2013).
House, W. National action plan for combating antibiotic-resistant bacteria. The White House, Washington, DC (2015).
Martn-Loeches, I., Diaz, E. & Valls, J. Risks for multidrug-resistant pathogens in the ICU. Curr. Opin. Crit. Care 20, 516–524 (2014).
Esterly, J. S. et al. Impact of carbapenem resistance and receipt of active antimicrobial therapy on clinical outcomes of Acinetobacter baumannii bloodstream infections. Antimicrob. Agents Chemother. 55, 4844–4849 (2011).
Patel, G., Huprikar, S., Factor, S. H., Jenkins, S. G. & Calfee, D. P. Outcomes of carbapenem‐resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infection control and hospital epidemiology 29, 1099–1106 (2008).
Sader, H. S., Farrell, D. J., Flamm, R. K. & Jones, R. N. Antimicrobial susceptibility of Gram-negative organisms isolated from patients hospitalized in intensive care units in United States and European hospitals (2009–2011). Diagn. Microbiol. Infect. Dis. 78, 443–448 (2014).
Lee, Y. S. et al. Recent trends in antimicrobial resistance in intensive care units in Korea. Korean Journal of Nosocomial Infection Control 19, 29–36 (2014).
Sohn, H. S., Oh, O. H., Kwon, J. W. & Lee, Y. S. Higher systemic antibiotic consumption in a population of South Korea (2008–2009). Int. J. Clin. Pharmacol. Ther. 51, 585–592 (2013).
Yoon, Y. K. et al. Trends of antibiotic consumption in Korea according to national reimbursement data (2008–2012): a population-based epidemiologic study. Medicine 94, e2100 (2015).
Kim, D. S., Jang, S. M. & Kim, N. S. Epidemiologic investigation on antibiotic use using defined daily dose. J Korean Acad Manag Care Pharm 2, 47–59 (2010).
Yoon, Y. K. et al. Surveillance of antimicrobial use and antimicrobial resistance. Infection and Chemotherapy 40, 93–101 (2008).
Kim, S. C., Park, Y. C., Kim, B. G. & Nam, D. H. Outpatient antibiotic prescription by pediatric and ENT physicians in Ulsan city. Korean Journal of Clinical Pharmacy 20 (2010).
Park, J., Han, E., Lee, S. O. & Kim, D. Antibiotic use in South Korea from 2007 to 2014: A health insurance database-generated time series analysis. Plos one 12, e0177435 (2017).
Jung, Y., Cho, H., Ji, E., Park, E. J. & Jang, S. Geographic variations in antibiotic prescription for pediatric acute upper respiratory tract infections in South Korea. Int. J. Clin. Pharmacol. Ther (2018).
Song, Y. et al. A national pharmacoepidemiological study of antibiotic use in Korean paediatric outpatients. Arch. Dis. Child., 310981 (2017).
Lee, J., Lee, J. S., Park, S., Shin, S. A. & Kim, K. Cohort profile: The national health insurance service–national sample cohort (NHIS-NSC), South Korea. Int. J. Epidemiol., dyv319 (2016).
Lu, P. et al. Epidemiology and antimicrobial susceptibility profiles of Gram-negative bacteria causing urinary tract infections in the Asia-Pacific region: 2009–2010 results from the Study for Monitoring Antimicrobial Resistance Trends (SMART). Int. J. Antimicrob. Agents 40, S43 (2012).
Xiao, Y. et al. Mohnarin report of 2011: monitoring of bacterial resistance in China [J]. Chinese Journal of Nosocomiology 22, 4946–4952 (2012).
Lerner, A. et al. Spread of KPC-producing carbapenem-resistant Enterobacteriaceae: the importance of super-spreaders and rectal KPC concentration. Clinical Microbiology and Infection 21, 470.e7 (2015).
Van Boeckel, T. P. et al. Global antibiotic consumption 2000 to 2010: an analysis of national pharmaceutical sales data. The Lancet Infectious Diseases 14, 742–750 (2014).
Cecchini, M., Langer, J. & Slawomirski, L. Antimicrobial Resistance in G7 Countries and Beyond: Economic Issues, Policies and Options for Action. Paris: Organization for Economic Co-operation and Development (2015).
Muraki, Y. et al. Japanese antimicrobial consumption surveillance: first report on oral and parenteral antimicrobial consumption in Japan (2009–2013). Journal of global antimicrobial resistance 7, 19–23 (2016).
Youngster, I. et al. Antibiotic Use in Children–A Cross-National Analysis of 6 Countries. J. Pediatr. 182, 244.e1 (2017).
Lee, E. K. Analysis of the changes in antibiotic use and resistance. Health Welfare Policy Forum 77, 72–82 (2003).
Kim, B. N. Overview of antibiotic use in Korea. Infection & Chemotherapy 44, 250–262 (2012).
Kim, B., Kim, H. B. & Oh, M. Antibiotic Control Policies in South Korea, 2000–2013. Infection & chemotherapy 48, 151–159 (2016).
Kim, Y. J. et al. The Changing Patterns of Antibiotics Usage in Korea during 1981–2008. Infection & Chemotherapy 44 (2012).
Hutchinson, J. M. et al. Measurement of antibiotic consumption: A practical guide to the use of the Anatomical Therapeutic Chemical classification and Defined Daily Dose system methodology in Canada. Canadian Journal of Infectious Diseases and Medical Microbiology 15, 29–35 (2004).
Gonzales, R., Malone, D. C., Maselli, J. H. & Sande, M. A. Excessive antibiotic use for acute respiratory infections in the United States. Clinical infectious diseases 33, 757–762 (2001).
Chow, A. W. et al. IDSA clinical practice guideline for acute bacterial rhinosinusitis in children and adults. Clinical Infectious Diseases 54, e112 (2012).
Irwin, R. S. et al. Diagnosis and management of cough: ACCP evidence-based clinical practice guidelines. Chest-Chicago- 129, 24S (2006).
Shulman, S. T. et al. Clinical practice guideline for the diagnosis and management of group A streptococcal pharyngitis: 2012 update by the Infectious Diseases Society of America. Clinical infectious diseases 55, e102 (2012).
McDonagh, M. et al. Improving antibiotic prescribing for uncomplicated acute respiratory tract infections (2016).
Arnold, S. R. & Straus, S. E. Interventions to improve antibiotic prescribing practices in ambulatory care. The Cochrane Library (2005).
Drekonja, D. M. et al. Antimicrobial stewardship in outpatient settings: a systematic review. infection control & hospital epidemiology 36, 142–152 (2015).
Lee, Y. S. et al. Private practitioners’ antimicrobial prescription patterns for acute respiratory infections in children. J Korean Public Health Assoc 17, 3–19 (1991).
Kim, N. S., Jang, S. N. & Jang, S. M. Factors influencing antibiotics prescribing of primary health physicians in acute upper respiratory infections. Journal of preventive medicine and public health = Yebang Uihakhoe chi 38, 1–8 (2005).
Kim, D. S. Physician’s belief on antibiotic use in upper respiratory tract infections. HIRA Policy Trend 5, 33–41 (2011).
Cho, H. & Kim, C. Discolored nasal discharge did not increase the antibiotic prescription rate for the common cold patients. Pharmacoepidemiol. Drug Saf. 14, 139–141 (2005).
Chung, D. R. & Song, J. National campaign for appropriate antibiotic use in Korea. Infection & Chemotherapy 44, 164–167 (2012).
Acknowledgements
The study was approved by National Health Insurance Service Ilsan Hospital institutional review board as required by local hospital policy (NHIMC 2017-04-013) with permission of the National Health Insurance Service-National Sample Cohort (REQ.0000008046). This study was funded by grants from the National Health Insurance Service Ilsan Hospital (2016-20-001).
Author information
Authors and Affiliations
Contributions
Y.A.K. and Y.S.P. equally contributed in study design, manuscript writing and data analysis. T.Y. helped with data analysis and preparation of the tables. H.L. and K.L. critically reviewed manuscript. All authors reviewed and approved the manuscript for submission.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Kim, Y.A., Park, Y.S., Youk, T. et al. Changes in Antimicrobial Usage Patterns in Korea: 12-Year Analysis Based on Database of the National Health Insurance Service-National Sample Cohort. Sci Rep 8, 12210 (2018). https://doi.org/10.1038/s41598-018-30673-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-30673-6
This article is cited by
-
Impact of prolonged carbapenem use-focused antimicrobial stewardship on antimicrobial consumption and factors affecting acceptance of recommendations: a quasi-experimental study
Scientific Reports (2023)
-
Clinical and molecular epidemiology of invasive group B Streptococcus infections in adults in a referral center in Korea
European Journal of Clinical Microbiology & Infectious Diseases (2022)
-
Development of key quality indicators for appropriate antibiotic use in the Republic of Korea: results of a modified Delphi survey
Antimicrobial Resistance & Infection Control (2021)
-
Clinical characteristics and risk factors for cefaclor-induced immediate hypersensitivity: a retrospective observation at two university hospitals in Korea
Allergy, Asthma & Clinical Immunology (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
