
Abstract
The aims of this study were as follows: to estimate the mortality and years of life lost, assessed by disability-adjusted life years (DALYs), due to breast cancer attributable to physical inactivity in Brazilian women; to compare the estimates attributable to physical inactivity and to other modifiable risk factors; and to analyse the temporal evolution of these estimates within Brazilian states over 25 years (1990–2015), compared with global estimates. Databases from the Global Burden of Disease Study for Brazil, Brazilian states, and other parts of the world were used. Physical inactivity has contributed to a substantial number of deaths (1990: 875; 2015: 2,075) and DALYs (1990: 28,089; 2015: 60,585) due to breast cancer in Brazil. Physical inactivity was responsible for more deaths and DALYs (~12.0%) due to breast cancer than other modifiable risk factors (~5.0%). The Brazilian states with better socioeconomic indicators had higher age-standardized rates of mortality and morbidity due to breast cancer attributable to physical inactivity. From 1990 to 2015, mortality due to breast cancer attributable to physical inactivity increased in Brazil (0.77%; 95%U.I.: 0.27–1.47) and decreased (−2.84%; 95%U.I.: −4.35 – −0.10) around the world. These findings support the promotion of physical activity in the Brazilian female population to prevent and manage breast cancer.
Similar content being viewed by others


Introduction
Breast cancer is a disease more common in the female population, and in 2017, it was the leading cause of death among females around the world1,2,3. Breast cancer was also responsible for substantial years of life lost around the world, becoming a type of cancer that, in addition to high mortality, is also responsible for early morbidity1,2,3. This neoplasm has multifactorial aetiology that includes both genetic and modifiable lifestyle factors1,2. Among the lifestyle factors, physical inactivity, obesity, inadequate diet and excessive alcohol use stand out as modifiable risk factors, which, if avoided, could help in the prevention and management of breast cancer1,2. It is not known whether studies have investigated the burden of breast cancer mortality due to all of these modifiable risk factors in the same population.
Physical inactivity appears to reduce the risk of breast cancer through a number of mechanisms, including body fat reduction, which in turn reduces oestrogen and insulin concentrations. Indeed, these hormones have mitogenic effects on mammary cells3,4. Likewise, leptin released from adipose tissue, which has been associated with post-menopausal breast cancer, significantly decreases following aerobic activity2,3,4. Therefore, physical activity may have positive effects on reducing the incidence of breast cancer by modifying endocrine function and improving the immune system5. A systematic review and meta-analysis on the association between physical inactivity and chronic disease outcomes found a strong correlation between physical inactivity and the risk of five chronic diseases, including breast cancer6. In addition, an aggregation of 35 prospective cohort studies reported a 14% reduction in the risk of breast cancer for physically active individuals6.
There are short and persistent adverse, even toxic, effects of breast cancer treatment that might be prevented, attenuated, treated, or rehabilitated through regular physical activity7,8. Breast cancer patients, who exercised while undergoing cancer treatments, were not only able to tolerate the exercise prescriptions but also presented a more favourable trend towards the alleviation of decrements in functional capacity, fatigue levels, and depression when compared to patients who did not exercise. Additionally, and very importantly, no adverse events were reported, and patients seemed to have no problems engaging in regular physical activity7,8. In this sense, physical activity is also important in the tertiary prevention of breast cancer.
Studies analysing data on the global burden of breast cancer mortality and morbidity have found no association with a single specific cause but with several causal factors of the disease1,9,10,11. The information on the burden of mortality or morbidity of a disease due to several causes is important because it provides essential data for the epidemiological monitoring of the disease. However, it does not allow for the identification and quantification of causal chain risk factors that impact the burden of disease12. The study of physical inactivity as a specific risk factor compared with other modifiable risk factors in the global burden of mortality and morbidity of breast cancer may be useful for public policies to intervene not only related to the disease but also related to associated risk factors, which may result, in the medium and long term, in lower incidence of the disease and better quality of life of the affected population12.
Brazil is a middle-income country that has recently improved its national health databases and implemented a series of surveys to better assess noncommunicable diseases, risk factors, prevalence and disease burden13,14. The results of these national health databases showed that there is an inequality in the burden of diseases and risk factors among the states of Brazil13,14. This inequality can be reflected by socioeconomic differences and the level of development of each of the Brazilian regions. In this sense, the investigation of the evolution of breast cancer mortality and morbidity due to physical inactivity in the Brazilian states over 25 years may be useful for health policies.
The aim of this study was to estimate the mortality and years of life lost, assessed by disability-adjusted life years (DALYs), due to breast cancer attributable to physical inactivity in the female population from Brazil and Brazilian states. We also aimed to compare the estimates of mortality and DALYs due to breast cancer attributable to physical inactivity with estimates attributable to other modifiable risk factors. Finally, we aimed to analyse the temporal trends of the estimates of mortality and DALYs due to breast cancer attributable to physical inactivity over 25 years (1990–2015) in comparison with global estimates and according to the socioeconomic status of Brazilian states.
Results
Incident breast cancer cases
In 1990 and in 2015, there were 983,231 (95%U.I.: 925,585–1,063,992) and 2,377,627 (95%U.I.: 2,236,222–2,496,759) incident breast cancer cases worldwide, respectively. In Brazil, 26,558 (95%U.I.: 22,328–29,349) incident breast cancer cases were estimated in 1990 and 79,015 (95%U.I.: 66,251–91,561) in 2015. These values represented, in 1990, an age-standardized rate of incident breast cancer cases (per 100,000 inhabitants) of 48.88 (95%U.I.: 46.10–52.72) around the world and of 54.73 (95%U.I.: 45.52–60.30) in Brazil. In 2015, the age-standardized rate of incident breast cancer cases was 65.49 (95%U.I.: 61.67–68.79) around the world and 74.02 (95%U.I.: 61.90–85.86) in Brazil. From 1990 to 2015, there was a large increase in the age-standardized rate of incident breast cancer cases around the world (39.72%; 95%U.I.: 29.39–49.95) and in Brazil (41.45%; 95%U.I.: 14.56–69.93). Table 1 provides detailed information on incident breast cancer cases (absolute number and age-standardized rate) for each Brazilian state.
Deaths and DALYs due to breast cancer
Around the world, 324,867 (95%U.I.: 312,956–347,331) deaths due to breast cancer due to all causes were estimated in 1990 and 523,487 (95%U.I.: 492,250–543,275) in 2015. In Brazil, 7,264 (95%U.I.: 6,185–7,694) deaths from breast cancer were estimated in 1990 and 16,964 (95%U.I.: 14,880–18,402) in 2015. Supplementary Table S1 provides the details on breast cancer mortality due to all causes (absolute number and age-standardized rate) for each Brazilian state.
Around the world, 9,578,973 (95%U.I.: 9,067,559–10,395,449) DALYs due to breast cancer attributable to all causes were estimated in 1990 and 15,137,828 (95%U.I.: 14,156,028–15,936,286) in 2015. In Brazil, 236,482 (95%U.I.: 205,941–251,674) DALYs were estimated in 1990 and 503,463 (95%U.I.: 443,581–548,345) in 2015. Supplementary Table S2 shows the information on breast cancer DALYs due to all causes (absolute number and age-standardized rate) for each Brazilian state.
Around the world, 63.265 (95%U.I.: 52.177–73.225) deaths due to breast cancer attributable to all risk factors (physical inactivity, alcohol use, high body mass index, diet high in sugar-sweetened beverages) were estimated in 1990 and 103,829 (95%U.I.: 84,505–123,222) in 2015. In Brazil, 1,212 (95%U.I.: 922–1,527) deaths from breast cancer were estimated in 1990 and 3,166 (95%U.I.: 2,359–4,149) in 2015. Supplementary Table S3 shows the information on breast cancer mortality due to all risk factors (absolute number and age-standardized rate) for each Brazilian state.
Around the world, 1,709,585 (95%U.I.: 1,427,601–1,987,977) DALYs due to breast cancer attributable to all risk factors (physical inactivity, alcohol use, high body mass index, diet high in sugar-sweetened beverages) were estimated in 1990 and 2,743,041 (95%U.I.: 2,257,795–3,240,611) in 2015. In Brazil, 35,113 (95%U.I.: 26,347–44,419) DALYs were estimated in 1990 and 82,164 (95%U.I.: 60,819–105,915) in 2015. Supplementary Table S4 shows the information on breast cancer DALYs due to all risk factors for each Brazilian state.
Mortality and morbidity due to physical inactivity
Regarding all-cause mortality and DALYs due to physical inactivity, Supplementary Table S5 and Supplementary Table S6 shows the information on mortality and DALYs by all causes due to physical inactivity for each Brazilian state, respectively.
In relation to breast cancer mortality due to physical inactivity, 29,605 (95%U.I.: 21,397–37,982) deaths were estimated in 1990 and 46,720 (95%U.I.: 34,033–59,421) in 2015 around the world. These values represented an age-standardized rate of deaths per 100,000 inhabitants of 1.54 (95%U.I.: 1.11–1.97) in 1990 and 1.31 (95%U.I.: 0.95–1.66) in 2015. In Brazil, 875 (95%U.I.: 646–1,110) deaths were estimated in 1990 and 2,075 (95%U.I.: 1,528–2,646) in 2015, which represented an age-standardized mortality rate of 1.99 (95%U.I.: 1.46–2.52) in 1990 and 2.00 (95%U.I.: 1.47–2.54) in 2015. From 1990 to 2015, there was a decline in the age-standardized rate of deaths due to breast cancer attributable to physical inactivity (−2.84%; 95%U.I.: −4.35 – −0.10) around the world, while Brazil had an increase (0.77%; 95%U.I.: 0.27–1.47). Table 2 shows the information on mortality due to breast cancer attributable to physical inactivity for each Brazilian state.
In relation to breast cancer DALYs due to physical inactivity, 812,664 (95%U.I.: 585,946–1,048,865) DALYs were estimated in 1990 and 1,252,121 (95%U.I.: 908,348–1,612,391) in 2015 around the world. These values represented an age-standardized mortality rate of 40.32 (95%U.I.: 29.10–51.99) in 1990 and 34.48 (95%U.I.: 25.04–44.41) in 2015. In Brazil, 28,089 (95%U.I.: 20,840–35,448) DALYs were estimated in 1990 and 60,585 (95%U.I.: 44,213–77,331) in 2015, which represented an age-standardized mortality rate of 55.80 (95%U.I.: 41.48–70.51) in 1990 and 55.26 (95%U.I.: 40.39–70.58) in 2015. From 1990 to 2015, DALYs due to breast cancer attributable to physical inactivity remained stable around the world (−3.13%; 95%U.I.: −4.91–0.17), while Brazil had an increase (0.75%; 95%U.I.: 0.21–1.47). Table 3 shows the information on DALYs due to breast cancer attributable to physical inactivity for each Brazilian state.
Physical inactivity was responsible for 12.0% and 12.2% of all deaths due to breast cancer in Brazil in 1990 and 2015, respectively. The other risk factors (alcohol use, high body mass index, diet high in sugar-sweetened beverages) were responsible for 4.7% and 6.5% of all deaths due to breast cancer in Brazil in 1990 and 2015, respectively. Regarding DALYs due to breast cancer, physical inactivity was responsible for 11.9% and 12.0% of all DALYs in 1990 and 2015, respectively. The other risk factors (alcohol use, high body mass index, diet high in sugar-sweetened beverages) were responsible for 2.9% and 4.3% of all DALYs due to breast cancer in Brazil in 1990 and 2015, respectively (Fig. 1).

Percentage contribution of all causes, all risk factors and physical inactivity in mortality and DALYs by breast cancer in Brazilian women (≥25 years old). All risk factors = physical inactivity, alcohol use, high body-mass index, diet high in sugar-sweetened beverages.
In Brazil, mortality due to breast cancer attributable to all causes, all risk factors, and physical inactivity increased with increasing age in 1990 and 2015. DALYs due to breast cancer attributable to all causes, all risk factors, and physical inactivity were similar in the age groups 50–69 years and 70+ years (Fig. 2).

Rate and 95% uncertainty interval (per 100,000 inhabitants) of death and DALYs from breast cancer in women due to all causes, all risk factors, and physical inactivity in Brazil according to age. All risk factors = physical inactivity, alcohol use, high body-mass index, diet high in sugar-sweetened beverages.
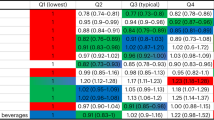
The Brazilian states with better socioeconomic indicators showed higher age-standardized rates of deaths (1990: rho = 0.77, p < 0.01; 2015: rho = 0.47, p < 0.01) and DALYs (1990: rho = 0.74, p < 0.01; 2015: rho = 0.42, p = 0.03) due to breast cancer attributable to physical inactivity. The Brazilian states that showed higher age-standardized rates of deaths (per 100,000 inhabitants) due to breast cancer attributable to physical inactivity were Rio de Janeiro, southeastern Brazil (1990: 2.7, 95%U.I.: 1.8–3.6; 2015: 2.5, 95% U.I.: 1.7–3.4); Rio Grande do Sul, southern Brazil (1990: 2.5, 95%U.I.: 1.6–3.2; 2015: 2.3, 95% U.I.: 1.5–3.2); and São Paulo, southeastern Brazil (1990: 2.3, 95% U.I.: 1.6–3.0; 2015: 2.1, 95%U.I.: 1.5–2.8). The Brazilian states that showed higher age-standardized rates of DALYs (per 100,000 inhabitants) due to breast cancer attributable to physical inactivity were Rio de Janeiro, southeastern Brazil (1990: 76.5, 95%U.I.: 50.2–99.7; 2015: 71.3, 95%U.I.: 48.6–96.7); Rio Grande do Sul, southern Brazil (1990: 67.8, 95%U.I.: 46.0–89.6; 2015: 60.7, 95%U.I.: 39.9–86.0); and São Paulo, southeastern Brazil (1990: 63.5, 95%U.I.: 45.9–82.3; 2015: 56.6, 95%U.I.: 39.7–76.0) (Figs 3, 4 and 5).

Age-standardized rate (per 100,000 inhabitants) of deaths and DALYs from breast cancer in women (≥25 years old) attributable to physical inactivity in the Brazilian states, 1990 and 2015.

Relationship between age-standardized rate of deaths from breast cancer due to physical inactivity and Sociodemographic Index of the Brazilian states in 1990 and 2015. The Brazilian states with better Socioeconomic Development Index (SDI) showed higher age-standardized mortality rate (Rho: Spearman’s correlation coefficient; 1990: rho = 0.77, p < 0.01; 2015: rho = 0.47, p < 0.01). Brazilian states - AC: Acre; AL: Alagoas; AP: Amapá; AM: Amazonas; BA: Bahia; CE: Ceará; DF: Distrito Federal; ES: Espírito Santo; GO: Goiás; MA: Maranhão; MT: Mato Grosso; MS: Mato Grosso do Sul; MG: Minas Gerais; PA: Pará; PB: Paraíba; PR: Paraná; PE: Pernambuco; PI: Piauí; RR: Roraima; RO: Rondônia; RJ: Rio de Janeiro; RN: Rio Grande do Norte; RS: Rio Grande do Sul; SC: Santa Catarina; SP: São Paulo; SE: Sergipe; To: Tocantins.

Relationship between age-standardized rate of DALYs from breast cancer due to physical inactivity and Socioeconomic Development Index of the Brazilian states in 1990 and 2015. The Brazilian states with better Socioeconomic Development Index showed higher age-standardized rate of DALYs (Rho: Spearman’s correlation coefficient; 1990: rho = 0.74, p < 0.01; 2015: rho = 0.42, p = 0.03). Brazilian states - AC: Acre; AL: Alagoas; AP: Amapá; AM: Amazonas; BA: Bahia; CE: Ceará; DF: Distrito Federal; ES: Espírito Santo; GO: Goiás; MA: Maranhão; MT: Mato Grosso; MS: Mato Grosso do Sul; MG: Minas Gerais; PA: Pará; PB: Paraíba; PR: Paraná; PE: Pernambuco; PI: Piauí; RR: Roraima; RO: Rondônia; RJ: Rio de Janeiro; RN: Rio Grande do Norte; RS: Rio Grande do Sul; SC: Santa Catarina; SP: São Paulo; SE: Sergipe; To: Tocantins.
Discussion
Among the main findings of this study, it was found that over 25 years, estimates of deaths and DALYs due to breast cancer attributable to all causes were stable in Brazil and decreased around the world. A survey conducted in the Eastern Mediterranean Region analysed the trends of deaths and DALYs from 2005 to 2015 by different cancers and found that mortality and DALY rates due to breast cancer stabilized over a 10-year period1. In Denmark and Finland, a reduction in breast cancer mortality rates over 25 years (1985–1989 to 2009–2013) has been reported15, and in the U.S., there was a decline in breast cancer mortality rates from 1990 to 2009 in all ethnic groups16. From 1990 to 2015, public health policies were created in Brazil, which resulted in improvements in cancer screening and treatment services, such as the National Oncology Policy17. The improvement in health services may reflect in the larger diagnosis of cancer cases, which justifies the increased incidence in 2015. Additionally, this improvement in health services is perhaps reflected in the stability of the age-standardized rate of deaths and DALYs; however, the continued progress of these services is important for a significant decline18,19. According to the Brazilian Society of Radiotherapy, in 2013, 335 radiotherapy devices were needed to treat patients, but only 230 were available. As a result, approximately 90,000 patients stopped receiving radiotherapy in that year19. Thus, more effective actions for the prevention, screening and treatment of breast cancer are urgent in Brazil.
Among the risk factors for breast cancer, this study found that 12% of deaths and DALYs in Brazil were due to physical inactivity, and 4% to 6% were due to other risk factors (alcohol use, high body mass index, diet high in sugar-sweetened beverages). This percentage represented more than 3,000 deaths and more than 89,000 DALYs in Brazil due to breast cancer attributable to physical inactivity in the years analysed (1990 and 2015). A systematic review with meta-analysis20 analysed 22 prospective cohort studies that totalled 123,574 participants followed for a period ranging from 4.3 to 12.7 years and found that 5,462 subjects had breast cancer outcomes (e.g., breast cancer-related deaths or recurrences). Compared to those who reported low/no lifetime recreational pre-diagnosis physical activity, participants who reported high lifetime recreational pre-diagnosis physical activity levels had a significantly lower risk of breast cancer-related death. Significant risk reductions for breast cancer-related death was also demonstrated for more recent pre-diagnosis recreational physical activity, post-diagnosis physical activity, and meeting recommended post-diagnosis physical activity guidelines (e.g., ≥8 MET-h/wk)20. Another systematic review with meta-analysis21 reported results similar and added the information that the association between pre- or post-diagnosis physical activity and total mortality among breast cancer survivors did not differ according to BMI, menopausal status, or tumour oestrogen receptor status. These reviews concluded that regular physical activity is a protective factor for pre- and post-diagnosis breast cancer mortality and support the results of this study.
The biological mechanisms that explain the relationship between breast cancer and physical inactivity clarify why physical inactivity has contributed to deaths and DALYs. One of the factors that cause breast cancer is the excess of circulating sex hormones, especially oestrogen, which can lead to the formation of mutations and carcinogenesis by stimulating the production of free radicals exhibiting genotoxicity22. Physical activity decreases oestradiol and increases sex hormone-binding globulin, which is a steroid-binding plasma glycoprotein whose main function is to reduce the amount of oestradiol23. Another factor that can lead to breast cancer is hyperinsulinaemia, which promotes the synthesis and activity of insulin-like growth factor (IGF-1)24. Physical activity can reduce insulin levels and insulin resistance, thereby decreasing fasting glucose and total IGF-125. Chronic inflammation is another factor that contributes to breast cancer development and progression through processes such as the polarization of immunosuppressive tumour-associated macrophages via cytokines and the subsequent production of tumour growth factors26. Physical exercise causes a reduction in the circulating amount of proinflammatory biomarkers and increases the circulating amount of anti-inflammatory substances27.
No studies that estimated the number of DALYs due to breast cancer attributable to physical inactivity were found. The studies found estimated the number of DALYs due to breast cancer attributable to all causes1,9, as this observation was also noted in the present study. Thus, this study adds to the growing body of evidence that healthy years of life are lost due to breast cancer, not only from all causes but specifically due to physical inactivity. Brazil had a stabilization of age-standardized rates of deaths and DALYs due to breast cancer attributable to physical inactivity over 25 years, and on the other hand, a decrease was observed around the world. The expansion and improvement of services for the screening and treatment of breast cancer and more effective actions to stimulate physical activity in the population may result in a decline in these rates in Brazil18,19. In the last 25 years, Brazil has implemented important public policies to encourage physical activity, such as the National Health Promotion Policy28, the creation of community physical activity programmes and the inclusion of physical activity in health monitoring and surveillance systems28,29. Additional actions are required, such as improving the built environment of the cities to enable physical activity30. Brazilian studies have shown that air pollution, few green areas and poor quality of urban infrastructure are still challenges31,32 that affect the engagement of the population in physical activities30. Another necessary action is to direct actions to encourage the practice of physical activity among children33. Data from the Active Healthy Kids Global Alliance have demonstrated that only half of children in Brazil meet physical activity recommendations and that there are few government incentives to promote physical activity in this age group33.
We found an increase in mortality and DALYs due to breast cancer attributable to physical inactivity with advancing age. The literature has shown that physical inactivity increases with age34, and this finding may justify our results. This study found that age-standardized rates of deaths and DALYs due to breast cancer attributable to physical inactivity were higher in Brazilian states with better socioeconomic conditions. According to the World Health Organization35, the increase in income and improvements in living standards in developing countries (which are observed more frequently in states with better socioeconomic conditions) have been accompanied by an increase in the incidence of breast cancer in women. This finding may be due to factors such as longer life, greater exposure to risk factors, higher fat intake, lower levels of physical activity, obesity and lower pregnancy rates than those of women who live in cities with worse economic conditions35. Another factor that may explain the high mortality and DALYs due to breast cancer attributable to physical inactivity in Brazilian states with better socioeconomic conditions is the fact that in these states, health services are better structured and serve more people than in states with worse socioeconomic conditions18. Serving more people may result in more diagnoses of breast cancer according to Brazilian Oncology Observatory18.
The number of breast cancer survivors in Brazil was not investigated in the present study; however, this number may also have increased during the 25 years, since there have been improvements in health services18,19. For this particular population, regular physical activity has physical and psychological benefits20,21. In addition, it can prevent recurrence of the disease20,21. Thus, physical activity should be prioritized at any stage of breast cancer.
The findings from this study can be useful for improving public health in Brazil because we found a large number of deaths and DALYs due to breast cancer attributable to modifiable risk factors. This information reinforces the need to act in the prevention of breast cancer not only through mammography screening but also through a healthy lifestyle. Adopting a healthy lifestyle has a lower cost to public health than the future treatment of the disease2. Thus, the present study reinforces the need for public policies focused on primary health care5. On the other hand, it can be inferred from this study that modifiable risk factors can help in tertiary prevention7,8, since different research has shown that adopting a healthy lifestyle should be a therapeutic adjunct for breast cancer patients20,21. This study did not stratify breast cancer cases according to the staging of the disease, but the numbers of deaths and DALYs attributable to physical inactivity and other risk factors provide benchmark for public health in Brazil in its prioritization of healthy lifestyles for women who both have and have not received a diagnosis of breast cancer.
This study has important limitations. First, this study did not stratify by the type of breast cancer to identify which type has the greatest relation with physical inactivity36. Second, this study did not exclude genetic cases of breast cancer mutations and did not stratify breast cancer according to the different types of treatment (e.g., chemotherapy with anthracyclines, radiotherapy, or other) to identify which has the greatest relation with physical inactivity37. Third, our study does not include all risk factors for breast cancer, such as the dosage of hormone replacement therapy and other pharmaceutical factors considered to be risks for this disease. Fourth, the present study only includes physical activity measured by questionnaires that are considered subjective measures of physical activity and are associated with measurement bias38. Fifth, the non-stratification of physical activity by domains is another limitation. Sixth, the use of a simulation model may be considered another limitation, although this model has evidence of validity39.
The strength of this study was the estimation of mortality and DALYs by physical inactivity throughout Brazil. From this information, it was possible to estimate mortality rates and DALYs due to breast cancer attributable to physical inactivity. This is the first study that used data from all states to make these estimates, which increases the accuracy and resolution of the information. Thus far, it has been known that physical inactivity was a risk factor for breast cancer, but it had not been estimated the degree to which it was related to morbidity (DALYs) and mortality, especially across two time periods (1990 and 2015).
It could be concluded that physical inactivity has contributed to a substantial number of deaths and DALYs due to breast cancer in Brazil and around the world. Physical inactivity was responsible for more deaths and DALYs due to breast cancer than other modifiable risk factors. Estimates of mortality and morbidity from breast cancer as a result of physical inactivity in Brazil increased between 1990 and 2015 compared to global estimates. Brazilian states with better socioeconomic indicators had higher mortality and morbidity rates from breast cancer due to physical inactivity. These findings support the promotion of physical activity in the Brazilian female population to help prevent and manage breast cancer.
Methods
Study overview
The Global Burden of Disease Study (GBD) 2015 includes an annual assessment covering 195 countries and territories from 1990 to 2015. It covers 310 diseases and injuries, 2,619 sequelae and 79 risk factors by age and sex. Detailed descriptions of the methodology and approach of the GBD 2015 have been published elsewhere13,14,40.
Data from this study included only information on the female population. For data on the association between breast cancer and physical activity and between breast cancer and other risk factors, the information corresponds to women aged ≥25 years.
Breast cancer estimates
All neoplasms, as defined by the 10th revision of the International Statistical Classification of Diseases (ICD-10) to one of the 29 GBD cancer groups, were mapped. ICD-10 codes for the incidence, morbidity and mortality due to breast cancer were C50-C50.929, D05-D05.92, D24-D24.9, D48.6-D48.62, D49.3, and N60-N60.991,9.
Input data for cancer mortality estimates came from the vital statistics mortality data and the cancer registry incidence data. The latter were transformed into mortality estimates using separately modelled mortality-to-incidence ratios (MIR)1,9. Crude data were processed to make them comparable and to account for “garbage codes”, which are codes assigned to causes that are not usable from the perspective of public health40. These causes were redistributed to the most likely underlying cause of death based on the regression model1. Through the use of a Cause of Death Ensemble modelling (CODEm) approach with cause-specific covariates, mortality estimates for each individual cause were computed41. These estimates were scaled to fit into an independently modelled all-cause mortality estimate using the CoDCorrect algorithm39.
Cancer survival was calculated using a MIR-based scaling factor. A 10-year prevalence of each cancer and each incidence cohort was calculated using these cancer survival estimates. The total prevalence was divided into four sequelae with variable disability weights: (1) diagnosis and treatment, (2) remission, (3) metastasis, and (4) terminal phase. A constant duration for sequelae (1), (3), and (4) was assumed. Sequela duration (2) was the remaining prevalence after subtracting the fixed sequelae duration. Years of life lost (YLLs) were computed by multiplying deaths by the normative standard life expectancy at each age of death39. For each sequela, years lost due to disability (YLDs) were calculated by multiplying the prevalence of each sequela by its disability weight. Finally, DALYs were calculated by summing premature death (YLLs) and YLDs. More information about these estimates can be found elsewhere39.
Physical inactivity estimate
Surveys of the general adult population performed using random sampling procedures that assessed self-reported physical activity in all life domains (leisure/recreation, work, household and transport) were included. Due to the absence of a consistent relationship at the individual level between the amount of physical activity performed in each domain and total activity, it was not possible to use studies that included only recreational/leisure activities12.
For the global estimates, data were primarily derived from two standardized questionnaires, the Global Physical Activity Questionnaire (GPAQ) and the International Physical Activity Questionnaire (IPAQ), although any other survey instrument that asked about intensity, frequency and duration of physical activities performed across all activity domains was included12.
In the case of Brazil, surveys such as the telephone-based Surveillance of Risk and Protective Factors for Chronic Diseases, the Brazil World Health Survey, and the International Prevalence Study on Physical Activity were also consulted13,14. More details can be found at http://ghdx.healthdata.org/gbd-2015/data-input-sources and in a previous publication12.
To standardize all estimates of physical inactivity in Brazil and around the world, data from the population aged 25 years or more were considered. Reported physical activity was accumulated for durations of at least ten consecutive minutes across all life domains. Physical activity frequency, duration and intensity were used to calculate the total metabolic equivalent (MET) minutes per week12. Estimates were made for subjects classified as physically inactive (<600 METS-min/week)12.
Others risk factor estimates (alcohol use, high body-mass index, diet high in sugar-sweetened beverages)
In addition to physical inactivity, the GBD study defined other modifiable risk factors for breast cancer. This definition took into account the quality of the information, the evidence, and the quality of the prediction models12.
For alcohol use, the theoretical minimum-risk exposure level (TMREL) was assumed to be no alcohol use (e.g., 0 g/day)12. Thus, it was considered a risk if there were some alcohol consumption/day. To generate estimates of alcohol consumption in grams per day, data from population surveys were used in combination with estimates of per capita consumption from the Food and Agriculture Organization42 and the Global Information System on Alcohol and Health database43. Per capita consumption is an aggregate measure of recorded, unrecorded, and tourist per capita consumption of alcohol (UNWTO database44,45) derived from sales, production, and other economic statistics. While population-based surveys provide accurate estimates of the prevalence of lifetime abstainers, former drinkers and current drinkers, they typically underestimate real alcohol consumption levels12. As a result, the per capita consumption figures across all ages and both sexes from the FAO and GISAH are considered to be a better estimate of overall volume of consumption12. Per capita consumption, however, does not provide the age- and sex-specific consumption estimates needed to compute alcohol-attributable burden of disease. Therefore, we use the age-sex pattern of consumption among drinkers modelled from the population survey data and the overall volume of consumption from the FAO and GISAH to determine the total amount of alcohol consumed by the country and states.
The TMREL of BMI was determined based on the BMI level that was associated with the lowest risk of all-cause mortality in prospective cohort studies43. In this study, the TMREL of BMI was 20–25 kg/m². Thus, a BMI > 25 kg/m² was considered a risk. We used data from multi-country survey programmes, national surveys, and longitudinal studies that were available in the Global Health Data Exchange (GHDx) and provided either self-report or measured data on height and weight. A complete description of the data-seeking and update process for the GHDx is provided elsewhere12. In addition, a systematic review of national and subnational studies was conducted for studies published until 31 December 201512. We adjusted self-reported data for overweight prevalence, obesity prevalence, and mean BMI using hierarchical mixed-effects regression models, fit using maximum likelihood separately by sex.
Exposure to a diet high in sugar-sweetened beverages was defined as an average daily consumption of greater than 2.5 grams per day of beverages with ≥50 kcal per 226.8-gram serving, including carbonated beverages, sodas, energy drinks, and fruit drinks, but excluding 100% fruit and vegetable juices. In this study, the TMREL of diets high in sugar-sweetened beverages was 0–5 grams/day. Thus, consumption greater than 5 grams/day was considered a risk12. We used dietary data from multiple sources, including nationally and sub-nationally representative nutrition surveys, household budget surveys, and the United Nations FAO food balance sheets and supply utilization accounts. All dietary data were standardized to 2000 kcal/day. For each dietary factor, we estimated the global age pattern of consumption based on nutrition surveys (e.g., 24-hour diet recall) and applied that age pattern to the FAO data.
Further details about the modelling used for the risk factors were previously published12. Brazil’s surveys for all these risk factors are available at http://ghdx.healthdata.org/gbd-2015/data-input-sources.
Analytical methods
The contribution of all causes, all risk factors and physical inactivity to mortality and DALYs due to breast cancer was estimated using a comparative risk assessment approach in which observed health outcomes are compared to those that would have been observed with a counterfactual set of exposures where no one was exposed12. For this approach, we used the simulation model by the CODEm to estimate indicators by age, sex, country, state, year, and cause, that is, an analytical tool that tests several possible statistical models of causes of death and creates a combined set of models that offers the best predictive performance. The DisMod-MR 2.1 software (World Health Organization©, Geneva, Switzerland), a meta-regression tool, was used for the derivation of simultaneous estimates of incidence, prevalence, remission, disability, and mortality attributable to risk factors, such as physical inactivity12,39. In this study, the results of these models were used to proportionally distribute deaths from breast cancer from all causes, all risk factors, and physical inactivity39. Modelling details can be found in the literature12.
Incident breast cancer cases, absolute number of deaths, mortality rates and DALYs (per 100,000 inhabitants—crude and age-standardized) were used as metrics. The sum of DALYs across the population, or the burden of the disease, can be considered a measurement of the gap between current health status and the ideal health situation46.
In the GBD study, 95% uncertainty intervals (95%U.I.) were calculated to provide information on the variability of estimates resulting from errors due to the sampling process and non-sample errors due to adjustments of data sources and modelling39.
The GBD 2015 created the Socioeconomic Development Index (SDI)39 for all evaluated locations by calculating per capita income, formal education at 15 years of age and fertility rate. This index was used to compare the metrics used among Brazilian states. For this analysis, the Spearman correlation coefficient was applied.
The datasets generated during and/or analysed during the current study are available from the corresponding author upon reasonable request. All data generated or analysed during this study are included in this published article (and its supplementary information files).
References
Global Burden of Disease Cancer Collaboration. et al. Global, Regional, and National Cancer Incidence, Mortality, Years of Life Lost, Years Lived With Disability, and Disability-Adjusted Life-years for 32 Cancer Groups, 1990 to 2015: A Systematic Analysis for the Global Burden of Disease Study. JAMA Oncol. 3, 524–548 (2017).
Kerr, J., Anderson, C. & Lippman, S. M. Physical activity, sedentary behaviour, diet, and cancer: an update and emerging new evidence. Lancet Oncol. 18, e457–e471 (2017).
Pudkasam, S., Tangalakis, K., Chinlumprasert, N., Apostolopoulos, V. & Stojanovska, L. Breast cancer and exercise: The role of adiposity and immune markers. Maturitas. 105, 16–22 (2017).
Stamatakis, E. et al. Does strength promoting exercise confer unique health benefits? A pooled analysis of eleven population cohorts with all-cause, cancer, and cardiovascular mortality endpoints. Am. J. Epidemiol. [Epub ahead of print].
Colditz, G. A. & Bohlke, K. Priorities for the primary prevention of breast cancer. CA. Cancer J. Clin. 64, 186–194 (2014).
Kyu, H. H. et al. Physical activity and risk of breast cancer, colon cancer, diabetes, ischemic heart disease, and ischemic stroke events: systematic review and dose-response meta-analysis for the Global Burden of Disease Study 2013. BMJ. 354, i3857 (2016).
Fairman, C. M., Focht, B. C., Lucas, A. R. & Lustberg, M. B. Effects of exercise interventions during different treatments in breast cancer. J. Community Support Oncol. 14, 200–209 (2016).
Battaglini, C. L. et al. Twenty-five years of research on the effects of exercise training in breast cancer survivors: A systematic review of the literature. World J. Clin. Oncol. 5, 177–90 (2014).
GBD 2015 Eastern Mediterranean Region Cancer Collaborators et al. Burden of cancer in the Eastern Mediterranean Region, 2005–2015: findings from the Global Burden of Disease 2015 Study. Int. J. Public Health. [Epub ahead of print].
Jensen, J. D. et al. Trends in breast cancer in the elderly in Denmark, 1980-2012. Acta Oncol. 55, 59–64 (2016).
Sipetic-Grujicic, S. et al. Comparison of male and female breast cancer incidence and mortality trends in Central Serbia. Asian Pac. J. Cancer Prev. 14, 5681–5685 (2013).
Global Burden of Disease Risk Factors Collaborators. et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1659–1724 (2016).
Souza, M. F. M., França, E. B. & Cavalcante, A. Burden of disease and health situation analysis: results of the Global Burden of Disease (GBD) Brazil network. Rev. Bras. Epidemiol. 20, 1–3 (2017).
Malta, D. C. et al. Risk factors related to the global burden of disease in Brazil and its Federated Units, 2015. Rev. Bras. Epidemiol. 20, 217–232 (2017).
Kvåle, R. et al. Prostate and breast cancer in four Nordic countries: A comparison of incidence and mortality trends across countries and age groups 1975–2013. Int. J. Cancer. 141, 2228–2242 (2017).
Ademuyiwa, F. O. et al. US breast cancer mortality trends in young women according to race. Cancer. 121, 1469–1476 (2015).
National Institute of Cancer from Brazil. Controle do Câncer de Mama: Documento de Consenso, http://www1.inca.gov.br/ (2015).
Brazilian Oncology Observatory. Cancer as the first cause of death in Brazilian municipalities, https://observatoriodeoncologia.com.br/cancer-como-a-primeira-causa-de-morte-nos-municipios-brasileiros-em-2015/ (2018).
Ferrigno, R. Overview of Radiotherapy in Brazil, http://www.sbradioterapia.com.br (2013).
Lahart, I. M., Metsios, G. S., Nevill, A. M. & Carmichael, A. R. Physical activity, risk of death and recurrence in breast cancer survivors: A systematic review and meta-analysis of epidemiological studies. Acta Oncol. 54, 635–654 (2015).
Schmid, D. & Leitzmann, M. F. Association between physical activity and mortality among breast cancer and colorectal cancer survivors: a systematic review and meta-analysis. Ann. Oncol. 25, 1293–1311 (2014).
Krolik, M. & Milnerowicz, H. The effect of using estrogens in the light of scientific research. Adv. Clin. Exp. Med. 21, 535–543 (2012).
Emaus, A. et al. Physical activity, heart rate, metabolic profile, and estradiol in premenopausal women. Med. Sci. Sports Exerc. 40, 1022–1030 (2008).
Irwin, M. L. et al. Randomized controlled trial of aerobic exercise on insulin and insulin-like growth factors in breast cancer survivors: the Yale Exercise and Survivorship study. Cancer Epidemiol. Biomarkers Prev. 18, 306–313 (2009).
Fairey, A. S. et al. Effects of exercise training on fasting insulin, insulin resistance, insulin-like growth factors, and insulin-like growth factor binding proteins in postmenopausal breast cancer survivors: a randomized controlled trial. Cancer Epidemiol. Biomarkers Prev. 12, 721–727 (2003).
Pierce, B. L. et al. Elevated biomarkers of inflammation are associated with reduced survival among breast cancer patients. J. Clin. Oncol. 27, 3437–3444 (2009).
Gleeson, M. et al. The anti-inflammatory effects of exercise: mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 11, 607–615 (2011).
Malta, D. C. et al. A Política Nacional de Promoção da Saúde e a agenda da atividade física no contexto do SUS. Epidemiol. Serv. Saude. 18, 79–86 (2009).
Malta, D. C. et al. National Policy for the Health Promotion, description of the implementation of the physical activity and body practices, 2006–2014. Rev. Bras. Ativ. Fis. Saude. 19, 286–299 (2014).
Reis, R. S., Hino, A. A., Rech, C. R., Kerr, J. & Hallal, P. C. Walkability and physical activity: findings from Curitiba, Brazil. Am. J. Prev. Med. 45, 269–275 (2013).
Freitas, C. U. et al. Air pollution in Brazilian cities: selecting health impact indicators for surveillance. Epidemiol. Serv. Saude. 22, 445–454 (2013).
Lotufo, P. A. Green areas, clean air and cardiovascular health in the city of São Paulo. Sao Paulo Med. J. 135, 1–3 (2017).
Tremblay, M. S. et al. GlobalMatrix 2.0: Report Card Grades on the Physical Activity of Children and Youth Comparing 38 Countries. J. Phys. Act. Health. 13, S343–S366 (2016).
Casado-Pérez, C. et al. Time trends in leisure time physical activity and physical fitness in the elderly: five-year follow-up of the Spanish National Health Survey (2006-2011). Maturitas. 80, 391–398 (2015).
Adams, P. The breast cancer conundrum. Bull. World Health Organ. 91, 626–627 (2013).
Solà, M. et al. Sentinel Node Biopsy in Special Histologic Types of Invasive Breast Cancer. J. Breast Health. 12, 78–82 (2016).
Nounou, M. I. et al. Breast Cancer: Conventional Diagnosis and Treatment Modalities and Recent Patents and Technologies. Breast Cancer. 9, 17–34 (2015).
Strath, S. J. et al. Guide to the assessment of physical activity: Clinical and research applications: a scientific statement from the American Heart Association. Circulation. 128, 2259–2279 (2013).
Global Burden of Disease Mortality and Causes of Death Collaborators. et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: a systematic analysis for the Global Burden of Disease Study 2015. Lancet 388, 1459–1544 (2016).
Naghavi, M. et al. Algorithms for enhancing public health utility of national causes-of-death data. Popul. Health Metr. 8, 9 (2010).
Foreman, K. J., Lozano, R., Lopez, A. D. & Murray, C. J. Modeling causes of death: an integrated approach using CODEm. Popul. Health Metr. 10, 1 (2012).
Food and Agriculture Organization of the United Nations. FAOSTAT Statistics Database, http://www.fao.org/statistics/en/ (2016).
World Health Organization. WHO Global Health Observatory - recorded adult per capita alcohol consumption, total per country. Geneva, Switzerland: World Health Organization (2016).
UN World Tourism Organization. UN World Tourism Organization Compendium of Tourism Statistics 2015, http://statistics.unwto.org/news/2015-02-11/compendium-tourism-statistics-2015-edition (2016).
Global BMI Mortality Collaboration et al. Body-mass index and all-cause mortality: individual-participant-data meta-analysis of 239 prospective studies in four continents. Lancet. 388, 776–786 (2016).
Murray, C. J. L., Salomon, J. A., Mathers, C. D. & Lopez, A. D. Summary Measures in Population Health: Concepts, Ethics, Measurement, and Applications (World Health Organization, 2002).
Acknowledgements
The study was supported by grants from Bill & Melinda Gates Foundation (GBD Global) and Ministry of Health from Brazil (GBD 2015 Brazil-states; Process No. 25000192049/2014–14). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Author information
Authors and Affiliations
Contributions
D.A.S.S., M.S.T., M.F.M.S., M.R.G., M.M., M.N., D.C.M. conceived and designed the experiments. D.A.S.S., M.S.T., M.F.M.S., M.R.G., M.M., M.N., D.C.M. performed the experiments. D.A.S.S. and M.N. analyzed the data. D.A.S.S., M.S.T., M.F.M.S., M.R.G., M.M., M.N., D.C.M. contributed reagents/materials/analysis tools. D.A.S.S., M.S.T., M.F.M.S., M.R.G., M.M., M.N., D.C.M. wrote the paper. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Silva, D.A.S., Tremblay, M.S., Souza, M.d.F.M.d. et al. Mortality and years of life lost due to breast cancer attributable to physical inactivity in the Brazilian female population (1990–2015). Sci Rep 8, 11141 (2018). https://doi.org/10.1038/s41598-018-29467-7
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-29467-7
This article is cited by
-
Inequalities in the burden of female breast cancer in Brazil, 1990–2017
Population Health Metrics (2020)
-
Physical inactivity as a risk factor for all-cause mortality in Brazil (1990–2017)
Population Health Metrics (2020)
-
Physical inactivity as risk factor for mortality by diabetes mellitus in Brazil in 1990, 2006, and 2016
Diabetology & Metabolic Syndrome (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
