
Abstract
Studies on the associations between soy food consumption and arterial stiffness are rare. The aim of the present study was to evaluate their associations in Japanese men. A total of 652 eligible men, aged 35–69 years, who underwent the measurement of brachial-ankle pulse wave velocity (baPWV) as an index of arterial stiffness were evaluated in this cross-sectional study. Information on their lifestyle characteristics, including dietary behavior, was obtained from a structured self-administered questionnaire. The frequency of total soy products as well as fermented and non-fermented soy products intakes was calculated, and the amounts of soy protein and soy isoflavone intakes were also estimated; these were then divided into tertiles and their associations with baPWV values were evaluated using general linear models. Higher frequency of fermented soy products intake was associated with decreased baPWV after adjusting for the multivariable covariates (P value for trend was 0.002, in Model 3). This association did not alter after further adjustment with a biomarker of systemic inflammation (serum high-sensitivity C-reactive protein (hs-CRP)) (P value for trend was 0.001, in Model 4). Total soy isoflavone consumption was also inversely associated with baPWV even after adjusting for multivariable covariates including serum hs-CRP (P value for trend was 0.043, in Model 4); however total soy protein consumption was not. These results demonstrated that greater consumption of soy food, especially fermented soy products and soy isoflavone was associated with reduced arterial stiffness, independent of systemic inflammation, in Japanese men.
Similar content being viewed by others

Introduction
Since cardiovascular diseases are major causes of death in developed countries, early detection of cardiovascular damage is desired earnestly to prevent mortality and morbidity from cardiovascular diseases. Atherosclerotic changes in arteries mainly contribute to the pathogenesis of cardiovascular diseases, and increased arterial stiffness is demonstrated to be closely associated with atherosclerosis. Arterial stiffness can be evaluated by measuring arterial pulse wave velocity (PWV). Brachial-ankle PWV (baPWV) measurement is convenient, relatively quick, and reproducible. Moreover, baPWV value correlates well with the carotid-femoral PWV, which is an established index for assessing aortic stiffness1. Therefore, baPWV measurement has become popular in screening for arterial stiffness in Asian countries.
Isoflavone is a chemical compound that is structurally and biologically similar to estrogen2, and is known to have cardiovascular benefits. Dietary isoflavone is available through soybean and soy products. Soybean belongs to the legume family and is recognized as one of the plant foods. Soybeans have been a major component of the traditional Asian (including Japanese) diets, and are usually consumed as processed foods (tofu, natto, miso, shoyu, etc.). Fermented soy products such as miso and natto are often consumed in Japan as Japanese special food3. Soybean products are seen as healthy diets because of their beneficial nature of containing low fat, rich protein, rich vitamins, minerals, and fiber. Due to these beneficial nature and isoflavone content, soybean and soy products are considered to have potential cardiovascular benefits. However, the findings of studies evaluating the effects of soy food or soy isoflavone intake on cardiovascular benefits have been inconsistent4,5,6,7.
The antioxidative activity of fermented soybean products has been reported to be significantly higher than that in non-fermented steamed soybean8,9. Such antioxidative activity receives special attention because of its potential beneficial effect on cardiovascular health. However, reports on the relationships between the consumption of soy food products, especially the consumption of fermented soy products and soy isoflavone, and arterial stiffness which can detect early cardiovascular damage are few. The present study evaluated the possible relationships between frequency of intake of the total soy products, especially fermented soy products, and arterial stiffness using baPWV as the parameter in Japanese men. We also evaluated the relationships between the consumption of soy protein and soy isoflavone and arterial stiffness.
Materials and Methods
Study subjects
This cross-sectional study included men aged 35–69 years who participated in the baseline survey of a prospective cohort study from November 2009 to June 2012 in Tokushima Prefecture, Japan and who received a baPWV measurement at the baseline survey. The subjects were workers, and most of them were office workers and not shift workers. This study was performed as part of the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study, a prospective cohort study. Details of this cohort study have been reported elsewhere10. Briefly, the J-MICC Study aims to examine the relationships of lifestyle and genetic factors as well as their interactions with lifestyle-related diseases.
All the participants in the J-MICC Study provided written informed consent prior to participation. The committees of Nagoya University School of Medicine, Aichi Cancer Center, and Tokushima University Graduate School approved the study protocol. This study was conducted according to the principles of the Declaration of Helsinki, and all methods were performed in accordance with the relevant guidelines and regulations.
Questionnaire and evaluation for soy product consumption
Information on individual medical histories and lifestyle characteristics, including dietary behavior over the past year, was obtained through a structured self-administered questionnaire. All the responses were reviewed by trained staff at the time of the survey. Leisure-time exercise was estimated on the basis of the International Physical Activity Questionnaire11. Exercise was divided into three levels as follows: light (e.g., walking and hiking), moderate (e.g., light jogging and swimming), and vigorous (e.g., marathon running and competitive sports). The degrees of leisure-time exercise for the three levels were expressed as metabolic equivalent (MET)-hours/week (MET level × hours of activity × events per week) and summed. In this estimation, light, moderate, and vigorous exercises were assigned with 3.4, 7.0, and 10.0 METs, respectively.
Evaluation for soy product consumption
Diet assessment was performed using a validated short food frequency questionnaire (FFQ) in the baseline survey of the J-MICC Study12,13,14,15. This FFQ included questions about the intake of 47 varieties of foods and beverages over the past year. This included questions about the intake of four groups of soy products: (Group1) miso soup; (Group2) tofu (soybean curd) for hiyayakko, yu-dofu; (Group3) natto and soybeans (boiled beans, etc.); and (Group4) fried tofu paste, fried bean curd, and thick deep-fried tofu. Eight categories of the frequency of each soy product intake were obtained as follows: three or more times/day (21/week), twice/day (14/week), once/day (7/week), 5–6 times/week (5.6/week), 3–4 times/week (3.5/week), 1–2 times/week (1.4/week), 1–3 times/month (0.7/week), and never or seldom (0/week). The total frequency of soy products intake was calculated as the sum of the frequencies of the four soy products intakes. According to the National Health and Nutrition Survey 201216, Japanese population rarely consume soybeans compared to natto. Natto occupies the majority of intake in Group3 (natto and soybeans). Miso is Japanese fermented soybean paste, while natto is made from soybeans fermented with Bacillus subtilis. Hence, the frequency of fermented soy products intakes was calculated as the sum of the frequencies of Group1 (miso soup) and Group3 (natto and soybeans) intakes. The frequency of non-fermented soy products intakes was calculated as the sum of the frequencies of Group2 (tofu) and Group4 (fried tofu paste, fried bean curd, and thick deep-fried tofu) intakes.
Next, we estimated the amount of total soy protein and total soy isoflavone intakes, as previously reported17. Since there were no questions on the size of each soy product consumed in the FFQ, 3-day diet records were surveyed four times in approximately 3 months’ intervals (in four seasons in Japan) within one year, in a group of 28 participants. This was used to grasp the serving size of each soy product per meal in our population to estimate the weekly amounts of total soy protein and total soy isoflavone intakes. The portion sizes of (1) miso soup, (2) tofu, (3) natto, soybean, and (4) fried tofu paste, fried bean curd, and thick deep-fried tofu were 9.9 (the amount used as miso), 53.8, 31.7, and 19.5 (g/meal), respectively. The amount of total soy protein intake was estimated by summing the soy protein contained in each specific soy food on the basis of the Standard Tables of Food Composition in Japan 201018. The amount of the total soy isoflavone intake was estimated by summing the soy isoflavone contained in each soy food based on the estimates of the phytoestrogens in foods in Japan19.
Daily intake of total energy was estimated using a program developed by the Department of Public Health, Nagoya City University School of Medicine12,13.
Measurements
baPWV was measured using a waveform analyzer (model BP-203RPE III; Colin, Co. Ltd., Komaki, Japan), as described previously20. In brief, a subject was examined while resting in the supine position in an air-conditioned room. Extremity blood pressure was measured using an oscillometric method, and the ankle brachial index (ABI) was automatically calculated. baPWV was calculated through a time-phase analysis between the right brachial artery pressure and volume waveforms at both ankles. To reduce inter-observer variations, all baPWV measurements were performed by a single researcher throughout the duration of the study. Individual baPWV and ABI data were expressed as the means of the bilateral baPWV and ABI, respectively.
Body mass index (BMI) was calculated as weight (kg) divided by height (m) squared. Venous blood was aspirated from each participant, and serum was separated within 3 hours and stored at −80 °C. Biochemical factors, including lipids and high-sensitivity C-reactive protein (hs-CRP) as a biomarker of systemic inflammation, in the stored sera, were measured at an external laboratory (BML Inc., Tokyo, Japan).
Statistical analyses
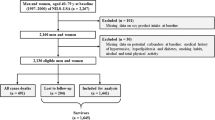
Of the 708 men initially included in this cross-sectional study, we excluded in total, 56 men (with overlapping characteristics) as follows (shown in Fig. 1): (1) 28 men with a history of ischemic heart disease or stroke; (2) 5 men with a low right or left ABI (ABI ≤ 0.9), which suggested peripheral arterial occlusive disease; (3) 5 men whose estimated daily total energy intake was extremely high (>4,000 kcal/day) or low (<1,000 kcal/day); and (4) 21 men who had no data on serum lipid or hs-CRP, frequency of soy products intakes, or any factors required in the multivariate models. Data on a total of 652 men were finally analyzed.

A flow chart of the analyzed subjects. From 708 men who underwent the measurement of baPWV in the baseline survey, we finally analyzed 652 eligible men. baPWV, brachial-ankle pulse wave velocity; ABI, ankle-brachial pressure index.
The total frequency of soy products intakes was divided into tertiles; the lowest category was used as the reference. Continuous variables were expressed as mean ± standard deviation (SD) or median values (25th percentile, 75th percentile). Categorical variables were expressed as numbers (%). The analysis of variance, Kruskal-Wallis test, or chi-square test was used to compare the characteristics between the tertile categories of the total frequency of soy products intakes, where appropriate.
General linear models were used to evaluate the relationships of frequency of total, fermented, and non-fermented soy products intakes (tertiles) as well as the amount of total soy protein and total soy isoflavone intakes (tertiles) with baPWV after adjusting for the covariates in four model groups. In Model 1, age (continuous) and systolic blood pressure (5 categories: <120, 120 to <140, 140 to <160, or ≥160 mmHg without medical treatment, and use of antihypertensive agent), which are recognized as being very closely associated with arterial stiffness were adjusted for. In Model 2, adjustment was made for age, systolic blood pressure, BMI (kg/m2, quartiles), smoking habit (current or others), alcohol drinking (current or others), exercise (MET-hours/week, quartiles), hypercholesterolemia (≥220 mg/dL or receiving medical treatment, no/yes) low high-density lipoprotein (HDL) cholesterol (<40 mg/dL, no/yes), elevated triglyceride levels (≥150 mg/dL, no/yes), diabetes (receiving medical treatment, no/yes), and daily energy intake (kcal/day, quartiles). In Model 3, the covariates adjusted for in Model 2 as well as coffee intake (≤1 cup/day, >1 to 3 cups/day, and >3 cups/day), calcium intake (mg/day, continuous, log-transformed) and total fiber intake (g/day, continuous, log-transformed) which might be associated with baPWV were adjusted for. Moreover, in Model 4, the covariates adjusted for in Model 3 as well as serum hs-CRP levels (mg/L; quartiles) were adjusted for. baPWV values and total fiber intake showed right skewed distributions and were included in the analyses after logarithmic transformation. Tests for trends were performed by assigning the ordinal variables of 1, 2, and 3 for each tertile category.
All calculations and statistical tests were performed using SAS version 9.4 (SAS Institute Inc., Cary, NC, USA). Statistical tests were based on 2-sided probabilities, and the level of significance was set at P < 0.05.
Results
The mean age (SD) and median BMI (25th, 75th) of the study subjects were 48.8 (8.6) years and 24.2 (22.3, 26.1) kg/m2, respectively. The median baPWV (25th, 75th) was 1,404 (1274, 1563) cm/s.
Characteristics of the subjects according to the frequency of total soy products and fermented soy products intakes
Tables 1 and 2 show the respective characteristics of the subjects according to the frequency of total and fermented soy products intakes. Subjects with greater frequency of total, as well as fermented soy products intakes showed higher degree of leisure-time exercise, higher energy intake, and greater consumption of calcium, total fiber, total soy protein, and total soy isoflavone, and lower prevalence of current smoking. Subjects in the highest tertiles of total as well as fermented soy products intakes showed the highest mean ages. baPWV values were marginal-significantly different between the tertiles of the frequency of fermented soy products intake (P value was 0.080), and these values gradually decreased as the frequency of fermented soy products intake increased.
Relationships between the frequency of total, fermented, and non-fermented soy products intakes and arterial stiffness
Table 3 shows the adjusted associations of the frequency of total, fermented, and non-fermented soy products intakes with baPWV (analyzed by general linear models). Higher frequency of total soy products intakes was associated with decreased baPWV after adjusting for the multivariable covariates including coffee, calcium, and total fiber intake (P value for trend was 0.005, in Model 3). This association did not alter after further adjustment with serum hs-CRP (P value for trend remained 0.005, in Model 4).
Further analyses categorizing soy products into fermented or not fermented, revealed that the frequency of fermented soy products intakes was inversely associated with baPWV after adjusting for multivariable covariates including serum hs-CRP (P value for trend was 0.001, in Model 4). However, the frequency of non-fermented soy products intakes was not associated with baPWV.
Relationships of total soy protein and total soy isoflavone consumption with arterial stiffness
As shown in Table 4, total soy isoflavone consumption was inversely associated with baPWV even after adjusting for multivariable covariates including serum hs-CRP (P value for trend was 0.043, in Model 4). In contrast, the inverse association between total soy protein consumption and baPWV attenuated, becoming non-significant when adjusting for coffee, calcium, and total fiber intake (Model 3), or additionally, serum hs-CRP (Model 4).
Discussion
The current study revealed that greater consumption of total soy products, especially fermented soy products and soy isoflavone, was dose-dependently associated with decreased arterial stiffness, independent of traditional atherosclerotic risk factors or systemic inflammation, in Japanese men.
Since cardiovascular diseases are leading causes of death in developed countries, measures against cardiovascular damage is important to prevent mortality and morbidity from cardiovascular diseases. Soybean and soy products contain rich protein, vitamins, minerals, fiber, and isoflavone; therefore, they are paid special attention due to the potential cardiovascular benefits. Findings of a most recent meta-analysis concluded that soy consumption was negatively associated with the risk of cardiovascular diseases, stroke, and coronary heart disease risk4. However, in the subgroup meta-analyses, a statistically significant protective effect of soy consumption on cardiovascular disease risk was primarily observed in Asian populations4. In contrast, Low et al.5 in a meta-analysis combining cohort studies, showed no association between soy intake and the risk of stroke or coronary heart disease, although a significantly inverse association between soy intake and the risk of stroke and coronary heart disease was observed in case-control studies. Thus, currently, the conclusions for the favorable effect of soy intake on the risk of cardiovascular diseases have remained inconsistent.
Soybeans are usually consumed as processed foods (tofu, natto, miso, shoyu, etc.) in Japan, and fermented soy products such as miso and natto are Japanese special food7. Therefore, we additionally evaluated the associations between soy food consumption and arterial stiffness by categorizing soy food into fermented or not fermented. The frequency of fermented soy products intakes was inversely associated with arterial stiffness after adjusting for multivariable covariates, while frequency of non-fermented soy products intakes was not. In a population-based cohort study in Japan, natto intake was associated with the decreased risk of cardiovascular disease mortality21. Natto possesses strong fibrinolytic activity and anti-coagulation profiles22,23. Natto is also demonstrated to have favorable effect on blood pressure24. Antioxidative activity has potential beneficial effect on cardiovascular health, and the antioxidative activity of fermented soybean products has been reported to be significantly higher than that in non-fermented steamed soybean8,9. The findings of these reports lend support to the results of our study. The present study also revealed that intake of total soy isoflavone, which has antioxidative activity, was inversely associated with arterial stiffness even after adjusting for multivariable covariates. When estimated total isoflavone consumption was used as a continuous variable (mg/week) (not by tertiles), it was also inversely correlated with baPWV: age-adjusted rank order correlation coefficient between total soy isoflavone consumption and baPWV (continuous, cm/sec) was −0.147 (P < 0.001). These results are concordant with the results in a previous systemic review which reported that soy isoflavone supplementation provides an effective means of reducing arterial stiffness25. However, according to the previous reports in Europe, dietary isoflavone intake was not associated with cardiovascular disease risk in Dutch women6 or with cardiovascular disease mortality in Spanish adults7. Low et al.5 also reported in their meta-analysis that no association between soy isoflavone intake and the risk of stroke and coronary heart disease was identified. Currently, as similar to the effect of soy food intake, the effect of soy isoflavone intake on the cardiovascular risk have remained inconsistent. Possible explanations for these inconsistencies include the differences in study designs, different amounts of soy intake in target populations, and different types of consumed soy products. The amount of soy consumption, especially intake amounts of fermented soy products, is higher in Asian populations than in Western populations26. In addition, the prevalence of equol producer is higher in Asian populations (about 50–60%)27 than in Western populations (about 20–30%)28. Equol is a metabolite of the dietary isoflavone produced by the action of intestinal bacteria in response to soy isoflavone intake27. Equol has selective affinity for the estrogen receptor β, that is also expressed in the vasculature. Equol possesses a longer half-life and higher bioavailability than genistein and daidzein, being the major isoflavones in soybean, and equol has been suggested to have the highest antioxidant properties of the isoflavones27,29. Recently, equol producer status has been reported to be inversely associated with arterial stiffness in Japanese women around menopause and early postmenopause30 and coronary calcification in Japanese men31. Equol supplementation has also been reported to decrease arterial stiffness in men32 and women33. Then, equol may have greater anti-atherosclerotic properties than other isoflavones. Because fermented soy products can skip the initial steps of soy metabolism in the intestine, they may contribute to larger production of equol than non-fermented soy food. Further studies determining equol-producing abilities of the individuals will be needed to determine the relationships between soy isoflavone consumption and cardiovascular health.
Coffee is often consumed worldwide including Japan. Coffee contains rich antioxidants such as chlorogenic acid and other bioactive compounds34. Epidemiologic studies have demonstrated inverse associations between coffee intake and diabetes35 and metabolic syndrome36,37, which are high risk conditions for atherosclerosis. A previous study conducted by us demonstrated that coffee consumption was inversely associated with arterial stiffness in Japanese men38. Dietary calcium is also suggested to be inversely associated with cardiovascular risk and mortality39,40; however, excessive calcium intake via supplementation may have adverse influence on vascular events41. Calcium is considered to be involved in the regulation of vascular smooth muscle cell contractility42 and reducing platelet aggregation43. Sufficient dietary fiber intake is also demonstrated to be associated with a reduced risk of cardiovascular disease through its impact on the glycemic response44,45. Soybean products contain rich calcium and fiber. Therefore, we additionally adjusted for coffee intake, calcium intake, and total fiber intake, which may be associated with arterial stiffness in the analyses. The inverse associations between the frequency of fermented soy products intakes as well as soy isoflavone consumption and arterial stiffness were slightly attenuated but remained significant, although the association between soy protein consumption and arterial stiffness became non-significant. This finding suggests that fermented soy products as well as soy isoflavone intake may be associated with reduced arterial stiffness. This association may be slightly dependent on intakes of coffee as well as calcium and fiber which are rich in soy products, however, other independent mechanisms may exist.
Chronic systemic inflammation has been recognized as a key player in the pathogenesis of various diseases including cardiovascular disease46,47. Hs-CRP is a sensitive biomarker of systemic inflammation48, and hs-CRP measurement in blood has recently become popular in clinical and health examination settings for assessing low-grade systemic inflammation. After further adjusting for serum hs-CRP levels (Model 4), the inverse associations between the frequency of fermented soy products intakes as well as soy isoflavone consumption and arterial stiffness did not alter. Therefore, the observed associations with arterial stiffness might be independent of chronic systemic inflammation.
The present study has several limitations. First, because of the cross-sectional study design, causal relationships between soy products and soy isoflavone consumption and reduced arterial stiffness could not be established. Second, information about the frequency of soy products intakes was self-reported; therefore, non-differential misclassification might have been inevitable. Moreover, we could not obtain information on the size of the consumed foods. Hence, we calculated the intake of soy products per meal from a four, 3-day diet records of 28 participants, in order to estimate soy protein and isoflavone consumption. Correlation coefficients between the estimated consumptions of soy protein and isoflavone from the FFQs and the diet records were 0.47 and 0.59 (Spearman’s rank correlation), respectively17. Additionally, the amounts of soy protein and soy isoflavone intakes as well as the total energy intake may be underestimated due to our short FFQ; however, their ranking might be satisfactory. Third, we did not determine the equol-producing abilities of the subjects. Fourth, although we adjusted for a number of potential confounding factors in the analyses, residual confounding could not be eliminated. Fourth, our study included a relatively small number of subjects. Finally, because all of our subjects were Japanese men, the results may not be generalizable to women or to other ethnic populations.
In conclusion, our study demonstrated that greater consumption of soy products, especially fermented soy products, as well as soy isoflavone was associated with reduced arterial stiffness, independent of the classical atherosclerotic risk factors and of chronic systemic inflammation, in Japanese men. Prospective or interventional studies that additionally include women are required to confirm our findings.
References
Lehmann, E. D. Clinical value of aortic pulse-wave velocity measurement. Lancet 354, 528–529 (1999).
Ren, M. Q., Kuhn, G., Wegner, J. & Chen, J. Isoflavones, substances with multi-biological and clinical properties. Eur. J. Nutr. 40, 135–146 (2001).
Lin, C. H., Wei, Y. T. & Chou, C. C. Enhanced antioxidative activity of soybean koji prepared with various filamentous fungi. Food Microbiol. 23, 628–633 (2006).
Yan, Z., Zhang, X., Li, C., Jiao, S. & Dong, W. Association between consumption of soy and risk of cardiovascular disease: A meta-analysis of observational studies. Eur. J. Prev. Cardiol. 24, 735–747, https://doi.org/10.1177/2047487316686441 (2017).
Lou, D., Li, Y., Yan, G., Bu, J. & Wang, H. Soy Consumption with Risk of Coronary Heart Disease and Stroke: A Meta-Analysis of Observational Studies. Neuroepidemiology 46, 242–252, https://doi.org/10.1159/000444324 (2016).
van der Schouw, Y. T. et al. Prospective study on usual dietary phytoestrogen intake and cardiovascular disease risk in Western women. Circulation 111, 465–471 (2005).
Zamora-Ros, R. et al. Dietary flavonoid and lignan intake and mortality in a Spanish cohort. Epidemiology 24, 726–733 (2013).
Berghofer, E., Grzeskowiad, B., Mundigler, N., Sentall, W. B. & Walcak, J. Antioxidative properties of faba bean-, soybean- and oat tempeh. Int. J. Food Sci. Nutr. 49, 45–54 (1998).
Santiago, L. A., Hiramatsu, M. & Mori, A. Japanese soybean paste miso scavenges free radicals and inhibits lipid peroxidation. J. Nutr. Sci. Vitaminol. 38, 297–304 (1992).
Hamajima, N., J-MICC Study Group. The Japan Multi-Institutional Collaborative Cohort Study (J-MICC Study) to detect gene-environment interactions for cancer. Asian Pac. J. Cancer Prev. 8, 317–323 (2007).
Craig, C. L. et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 35, 1381–1395 (2003).
Tokudome, S. et al. Development of a Data-based Short Food Frequency Questionnaire for Assessing Nutrient Intake by Middle-aged Japanese. Asian Pac. J. Cancer Prev. 5, 40–43 (2004).
Tokudome, Y. et al. Relative validity of a short food frequency questionnaire for assessing nutrient intake versus three-day weighed diet records in middle-aged Japanese. J. Epidemiol. 15, 135–145 (2005).
Goto, C. et al. Validation study of fatty acid consumption assessed with a short food frequency questionnaire against plasma concentration in middle-aged Japanese people. Scand. J. Nutr. 50, 77–82 (2006).
Imaeda, N. et al. Reproducibility of a short food frequency questionnaire for Japanese general population. J. Epidemiol. 17, 100–107 (2007).
Ministry of Health, Labour and Welfare. The National Health and Nutrition Survey in Japan, 2012. Tokyo: Ministry of Health, Labour and Welfare (2014).
Nakamoto, M. et al. Inverse association between soya food consumption and insulin resistance in Japanese adults. Public Health Nutr. 18, 2031–2040, https://doi.org/10.1017/S136898001400247X (2015).
Ministry of Education, Culture, Sports, Science, and Technology. Standard tables of food composition in Japan - 2010 -. Tokyo: Official Gazette Co-operation of Japan (2010).
Ministry of Health, Labour and Welfare. Q and A on soy and soy isoflavone (in Japanese). Internet, http://www.mhlw.go.jp/houdou/2006/02/h0202-1a.html (accessed 15 February 2017).
Tomiyama, H. et al. Influences of age and gender on results of noninvasive brachial-ankle pulse wave velocity measurement–a survey of 12517 subjects. Atherosclerosis 166, 303–309 (2003).
Nagata, C. et al. Dietary soy and natto intake and cardiovascular disease mortality in Japanese adults: the Takayama study. Am. J. Clin. Nutr. 105, 426–431, https://doi.org/10.3945/ajcn.116.137281 (2017).
Sumi, H., Hamada, H., Tsushima, H., Mihara, H. & Muraki, H. A novel fibrinolytic enzyme (nattokinase) in the vegetable cheese natto; a typical and popular soybean food in the Japanese diet. Experientia 43, 1110–1111 (1987).
Kurosawa, Y. et al. A single-dose of oral nattokinase potentiates thrombolysis and anti-coagulation profiles. Sci. Rep. 5, 11601, https://doi.org/10.1038/srep11601 (2015).
Kim, J. Y. et al. Effects of nattokinase on blood pressure: a randomized, controlled trial. Hypertens. Res. 31, 1583–1588 (2008).
Pase, M. P., Grima, N. A. & Sarris, J. The effects of dietary and nutrient interventions on arterial stiffness: a systematic review. Am. J. Clin. Nutr. 93, 446–454 (2011).
Peterson, J. J., Dwyer, J. T., Jacques, P. F. & McCullough, M. L. Associations between flavonoids and cardiovascular disease incidence or mortality in European and US populations. Nutr. Rev. 70, 491–508 (2012).
Setchell, K. D. & Clerici, C. Equol: history, chemistry, and formation. J. Nutr. 140, 1355S–1362S, https://doi.org/10.3945/jn.109.119776 (2010).
Setchell, K. D. & Cole, S. J. Method of defining equol-producer status and its frequency among vegetarians. J. Nutr. 136, 2188–2193 (2006).
Setchell, K. D. & Clerici, C. Equol: pharmacokinetics and biological actions. J. Nutr. 140, 1363S–1368S, https://doi.org/10.3945/jn.109.119784 (2010).
Yoshikata, R., Myint, K. Z. & Ohta, H. Relationship between equol producer status and metabolic parameters in 743 Japanese women: equol producer status is associated with antiatherosclerotic conditions in women around menopause and early postmenopause. Menopause 24, 216–224, https://doi.org/10.1097/GME.0000000000000743 (2017).
Ahuja, V. et al. Significant inverse association of equol-producer status with coronary artery calcification but not dietary isoflavones in healthy Japanese men. Br. J. Nutr. 117, 260–266, https://doi.org/10.1017/S000711451600458X (2017).
Hazim, S. et al. Acute benefits of the microbial-derived isoflavone metabolite equol on arterial stiffness in men prospectively recruited according to equol producer phenotype: a double-blind randomized controlled trial. Am. J. Clin. Nutr. 103, 694–702, https://doi.org/10.3945/ajcn.115.125690 (2016).
Yoshikata, R., Myint, K. Z. Y. & Ohta, H. Effects of Equol Supplement on Bone and Cardiovascular Parameters in Middle-Aged Japanese Women: A Prospective Observational Study. J. Altern. Complement. Med. https://doi.org/10.1089/acm.2018.0050 [Epub ahead of print] (2018 May 3).
Gómez-Ruiz, J. A., Leake, D. S. & Ames, J. M. In vitro antioxidant activity of coffee compounds and their metabolites. J. Agric. Food Chem. 55, 6962–6969 (2007).
Huxley, R. et al. Coffee, decaffeinated coffee, and tea consumption in relation to incident type 2 diabetes mellitus: a systematic review with meta-analysis. Arch. Intern. Med. 169, 2053–2063 (2009).
Hino, A. et al. Habitual coffee but not green tea consumption is inversely associated with metabolic syndrome: An epidemiological study in a general Japanese population. Diabetes Res. Clin. Practice 76, 383–389 (2007).
Takami, H. et al. Inverse Correlation Between Coffee Consumption and Prevalence of Metabolic Syndrome: Baseline Survey of the Japan Multi-Institutional Collaborative Cohort (J-MICC) Study in Tokushima, Japan. J. Epidemiol. 23, 12–20 (2013).
Uemura, H. et al. Consumption of coffee, not green tea, is inversely associated with arterial stiffness in Japanese men. Eur. J. Clin. Nutr. 67, 1109–1114, https://doi.org/10.1038/ejcn.2013.132 (2013).
Umesawa, M. et al. JPHC Study Group Dietary calcium intake and risks of stroke, its subtypes, and coronary heart disease in Japanese: the JPHC Study Cohort I. Stroke 39, 2449–2456, https://doi.org/10.1161/STROKEAHA.107.512236 (2008).
Kaluza, J. et al. Dietary calcium and magnesium intake and mortality: a prospective study of men. Am. J. Epidemiol. 171, 801–807, https://doi.org/10.1093/aje/kwp467 (2010).
Bolland, M. J. et al. Effect of calcium supplements on risk of myocardial infarction and cardiovascular events: meta-analysis. BMJ 341, c3691, https://doi.org/10.1136/bmj.c3691 (2010).
Maillard, M. P., Tedjani, A., Perregaux, C. & Burnier, M. Calcium-sensing receptors modulate renin release in vivo and in vitro in the rat. J. Hypertens. 27, 1980–1987, https://doi.org/10.1097/HJH.0b013e32832f0d22 (2009).
van Meijl, L. E., Vrolix, R. & Mensink, R. P. Dairy product consumption and the metabolic syndrome. Nutr. Res. Rev. 21, 148–157, https://doi.org/10.1017/S0954422408116997 (2008).
Erkkila, A. T. & Lichtenstein, A. H. Fiber and cardiovascular disease risk: How strong is the evidence? J. Cardiovasc. Nurs. 21, 3–8, https://doi.org/10.1097/00005082-200601000-00003 (2006).
Kokubo, Y. et al. JPHC Study Group. Dietary fiber intake and risk of cardiovascular disease in the Japanese population: The Japan Public Health Center-based study cohort. Eur. J. Clin. Nutr. 65, 1233–1241, https://doi.org/10.1038/ejcn.2011.100 (2011).
Danesh, J. et al. C-reactive protein and other circulating markers of inflammation in the prediction of coronary heart disease. N. Engl. J. Med. 350, 1387–1397 (2004).
Buckley, D. I., Fu, R., Freeman, M., Rogers, K. & Helfand, M. C-reactive protein as a risk factor for coronary heart disease: a systematic review and meta-analyses for the U.S. Preventive Services Task Force. Ann. Intern. Med. 151, 483–495 (2009).
Pepys, M. B. & Baltz, M. L. Acute phase proteins with special reference to C-reactive protein and related proteins (pentaxins) and serum amyloid A protein. Adv. Immunol. 34, 141–212 (1983).
Acknowledgements
The authors thank the following researchers for providing us the useful food frequency questionnaire and a program to calculate nutrient intake; Shinkan Tokudome at National Institute of Health and Nutrition (formerly Nagoya City University), Chiho Goto at Nagoya Bunri University, Nahomi Imaeda at Shigakkan University, Yuko Tokudome at Nagoya University of Arts and Sciences, Masato Ikeda at University of Occupational and Environmental Health, Shinzo Maki at Aichi Prefectural Dietetic Association. This study was funded by Grants-in-Aid for Scientific Research on Priority Areas of Cancer (No. 17015018), on Innovative Areas (No. 221S0001), and Platform of Supporting Cohort Study and Biospecimen Analysis (JSPS KAKENHI Grant Number JP16H06277) from the Japanese Ministry of Education, Culture, Sports, Science and Technology, and by Grants-in-Aid for Scientific Research (C) (JSPS KAKENHI Grant Number JP15K08778) from the Japan Society for the Promotion of Science.
Author information
Authors and Affiliations
Contributions
H.U. collected data, designed research, analyzed data, and wrote the manuscript. S.K.-K. collected data, analyzed data, and reviewed the manuscript. M.N. and M.Y. collected data and reviewed the manuscript. M.F. and Y.I. reviewed the manuscript. K.A. collected data and reviewed the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Uemura, H., Katsuura-Kamano, S., Nakamoto, M. et al. Inverse association between soy food consumption, especially fermented soy products intake and soy isoflavone, and arterial stiffness in Japanese men. Sci Rep 8, 9667 (2018). https://doi.org/10.1038/s41598-018-28038-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-28038-0
This article is cited by
-
The effect of soy isoflavones on arterial stiffness: a systematic review and meta-analysis of randomized controlled trials
European Journal of Nutrition (2021)
-
GWAS of 165,084 Japanese individuals identified nine loci associated with dietary habits
Nature Human Behaviour (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
