
Abstract
Human brown adipose tissue (BAT) is commonly assessed by cold-induced 18F-fluorodeoxyglucose (FDG) PET-CT using several quantification criteria. Uniform criteria for data analysis became available recently (BARCIST 1.0). We compared BAT volume and activity following BARCIST 1.0 criteria against the most commonly used criteria [Hounsfield Units (HU):-250, -50, standardized uptake value (SUV):2.0; HU: Not applied, SUV:2.0 and HU:-180, -10, SUV:1.5] in a prospective study using three independent cohorts of men including young lean adults, young overweight/obese adults and middle-aged overweight/obese adults. BAT volume was the most variable outcome between criteria. While BAT volume calculated using the HU: NA; SUV: 2.0 criteria was up to 207% higher than the BAT volume calculated based on BARCIST 1.0 criteria, it was up to 57% lower using the HU: -250, -50; SUV: 2.0 criteria compared to the BARCIST 1.0. Similarly, BAT activity (expressed as SUVmean) also differed between different thresholds mainly because SUVmean depends on BAT volume. SUVpeak was the most consistent BAT outcome across the four study criteria. Of note, we replicated these findings in three independent cohorts. In conclusion, BAT volume and activity as determined by 18F-FDG-PET/CT highly depend on the quantification criteria used. Future human BAT studies should conduct sensitivity analysis with different thresholds in order to understand whether results are driven by the selected HU and/or SUV thresholds. The design of the present study precludes providing any conclusive threshold, but before more definitive thresholds for HU and SUV are available, we support the use of BARCIST 1.0 criteria to facilitate interpretation of BAT characteristics between research groups.
Similar content being viewed by others

Introduction
Brown adipose tissue (BAT) is present and metabolically active in human adults1. In 2009, several studies using 18F-fluorodeoxyglucose (FDG) positron emission tomography (PET) combined with X-ray computed tomography (CT) (18F-FDG-PET/CT) imaging showed that human BAT can be activated upon cold exposure, that 18F-FDG uptake by BAT is more common in women than in men, and that 18F-FDG uptake by BAT is higher in lean than in obese individuals2,3,4,5. The capacity of BAT to combust energy as well as its beneficial role in glucose6 and lipid7 metabolism makes BAT an attractive therapeutic target in combating adiposity and type 2 diabetes.
Currently, 18F-FDG-PET/CT analysis is the most commonly used method to quantify human BAT volume and activity1. 18F-FDG-PET provides information about glucose uptake by metabolically active tissues including BAT, expressed as standardized uptake value (SUV)8,9. CT, on the other hand, provides anatomical information and allows the identification of various tissues, including adipose tissue and soft tissues, based on the radio-density expressed as Hounsfield units (HU). Therefore, quantification of BAT volume and activity depends to a great extent on the selection and combination of HU and SUV thresholds1. Due to the lack of consensus on the most appropriate HU and SUV thresholds to quantify BAT volume and activity in humans, studies have shown different levels of BAT volume and activity in cohorts with similar characteristics10,11. Consequently, since optimal thresholds are not known, current available data on human BAT volume and activity are speculative at best. Moreover, the use of different HU and SUV thresholds hampers comparability across studies.
Recently, an expert panel launched a set of recommendations for conducting 18F-FDG-PET/CT analysis of human BAT (Brown Adipose Reporting Criteria in Imaging Studies, BARCIST 1.0)1. BARCIST 1.0 recommends using a HU range between -190 and -10, and a SUV threshold of [1.2/(lean body mass (LBM)/body mass (BM))]. The impact of using the BARCIST 1.0 HU and SUV thresholds compared to the most commonly used protocols to quantify BAT volume and activity is currently unknown since, to our knowledge, no studies using these specific thresholds have been reported yet. It is of interest to better understand the relative differences obtained with BARCIST 1.0 thresholds compared to the currently most commonly used thresholds in literature for populations with different age and BMI.
Therefore, in the present study we aimed to compare and quantify BAT volume and activity following BARCIST 1.0 recommendations against the most commonly used HU and SUV thresholds in three different cohorts of men including young lean adults, young overweight/obese adults, and middle-aged overweight/obese adults.
Methods
Participants
A total of thirty men from three independent cohorts were included in this prospectively designed study. Participants’ characteristics are shown in Table 1. The study cohorts were: (i) 10 young lean adults (21–29 years old; BMI 19–24 kg/m2, white Caucasians)12, (ii) 10 young overweight/obese adults (18–25 years old; BMI 25–35 kg/m2)13, and (iii) 10 middle-aged overweight/obese adults (35–53 years old; BMI 26–30 kg/m2). The study conducted in young overweight/obese adults was approved by the Human Research Ethics Committee of both University of Granada (n°924) and Servicio Andaluz de Salud (Centro de Granada, CEI-Granada). The Medical Ethical Committee of the Leiden University Medical Center approved the other study cohorts (2473 and NCT02294084). All volunteers provided written informed consent before participation. All studies were performed in accordance with the Declaration of Helsinki.
Systematic review on most commonly used thresholds
To identify the most commonly used HU and SUV thresholds for 18F-FDG-PET/CT scans in BAT research, we conducted a systematic literature search on MEDLINE (from January 1st 2007 to March 10th 2017) for studies reporting human BAT volume and activity. We used the Medical Subject Heading (MeSH) terms “Adipose Tissue, Brown” in combination with type of population (men, women, and adults) and instrument used (“PET/CT”, “PET-CT”, and “18-FDG”). We excluded human studies that did not use 18F-FDG-PET/CT scans to assess BAT volume and activity, studies conducted in animal models or not written in English, and reviews. In addition, we searched the reference lists of all identified relevant publications. No restrictions were considered regarding study design (cross sectional, case-control, cohort study) or data collection (prospective or retrospective). To avoid duplicate data, we identified articles that included the same group of participants by reviewing inter-study similarities in any of the following characteristics: country in which the study was conducted, investigators who performed the study, source of patients, recruitment period, and inclusion criteria. When the same investigators reported results obtained on the same group of patients in several publications, only the first published study was included.
Cooling protocol
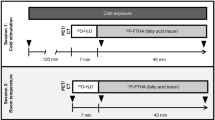
To activate BAT, we applied personalized cooling protocols prior to 18F-FDG-PET/CT scans. Slightly different water-cooling methods were used between the different cohorts due to differences in local equipment and protocols. In the young lean and middle-aged overweight/obese cohorts two water-perfused temperature-controlled mattresses (Blanketrol III, Cincinnati Sub-Zero Products, Cincinnati, OH, USA) were used, as previously described12. In short, participants were sandwiched between two water-perfused mattresses starting at a temperature of 32 °C, which was subsequently gradually decreased. When shivering occurred (after 30–40 min), temperature was raised by 3–4 °C and a stable cooling period of 2 h started. In the cohort of young overweight/obese adults a water perfused vest (Polar Products Inc., Ohio, USA) was used14. Shivering threshold was determined 48–72 h before the 18F-FDG-PET/CT scan. Immediately before the 18F-FDG-PET/CT scan, participants wore the water perfused vest for 2 h set at approx. 4 °C above the temperature that caused the onset of shivering. In all three studies, after 1 h of stable cooling 18F-FDG was injected (Table 1) and after 2 h of cooling 18F-FDG-PET/CT imaging was performed.
Body composition
Fat mass and lean body mass were measured by Dual Energy X-ray Absorptiometry (DEXA) in the three cohorts (Table 1).
18F-FDG-PET/CT scan
Cold-induced BAT volume and activity were assessed by 18F-FDG-PET/CT scanning. Table 1 shows details of the PET/CT scanners as well as doses of 18F-FDG injected in each study cohort. In the three studies, for the CT acquisition a peak kilovoltage of 120 was applied, while for the PET acquisition a scan time of 6 min per bed position was set. In total, 6 bed positions were scanned for the young lean and middle-aged overweight/obese adults (from top of the head to pelvis) and 2 bed positions for the young overweight/obese adults (from atlas vertebra to mid-chest, which was a requirement set by the Human Research Ethics Committee to limit radiation burden).
Quantification of human BAT volume and activity
PET/CT images were analyzed using the Beth Israel plugin for FIJI2 software by two trained researchers (BMT and KJN)15. Disagreements between both researchers were arranged in a consensus meeting. The regions of interest (ROIs) were semi-automatically outlined from atlas vertebrae (Cervical 1) to thoracic vertebrae 4 (see Figure S1) using a 3D-Axial technique11. The ROIs were placed in this range because (i) this region predominantly shows BAT activity and (ii) it is the region that is consistently scanned in all three study cohorts. Regions such as mouth, nose, or thyroid were not included to avoid potential false positives within the ROIs. We calculated the standardized uptake value (SUV) as [18F]-FDG uptake (kBq/mL)/(injected dose [kBq]/patient weight [g])]. We defined BAT volume, SUVmean, BAT metabolic activity, SUVmax and SUVpeak following BARCIST 1.0 criteria1. In short, BAT volume was calculated as the sum of the volumes identified as BAT in each ROI (1 to 6, see Figure S1). SUVmean was calculated by the weighted average of SUVmean derived from each ROI (1 to 6). SUVpeak was the highest average SUV in a 1 ml spherical volume. This sphere may, or may not, be centered on the highest SUVmax over all ROIs (1 to 6). We also drew a ROI on the descending aorta as reference tissue (Table 1)1. To quantify BAT, we applied the criteria of BARCIST 1.0, in addition to the three most used combinations of thresholds detected in the systematic review (see below).
Statistical analysis
Differences across HU and SUV thresholds were analyzed using analysis of variance (ANOVA) with Bonferroni adjustments for post-hoc comparisons. Separate analyses were conducted for each study cohort. The inter-observer (BMT and KJN) reliability was assessed using Lin’s concordance coefficient (LCC)16. All analyses were conducted using the Statistical Package for Social Sciences (SPSS, v. 22.0, IBM SPSS Statistics, IBM Corporation) and the level of significance was set to ≤0.05. Data are presented as mean ± standard deviation unless otherwise stated.
Results
Characteristics of participants
Table 1 summarizes the characteristics of the participants and the study conditions in the three cohorts.
Systematic review: Selection of HU and SUV thresholds
After having read titles and abstracts, 344 studies were excluded from a total of 471; 131 were checked for relevance (full text); and 123 met the inclusion criteria. After excluding redundant studies, i.e. studies that used the same participants and images, a total of 116 studies were finally included (Table S1). Table 2 shows a summary of the HU and SUV thresholds used in the quantification of human BAT by 18F-FDG-PET/CT. We found nine different combinations of HU and SUV thresholds published twice or more, and 26 different combinations of HU and SUV thresholds published just once. HU and/or SUV thresholds were not mentioned in as many as 32 studies. We selected the three most frequently used combinations of HU and SUV thresholds (Table 2): HU: -250, -50; SUV: 2.0, HU: N.A.; SUV: 2.0 and HU: -180, -10; SUV: 1.5 for comparison with the BARCIST 1.0 criteria.
High inter-observer reliability was found regardless of thresholds applied
Lin’s concordance coefficient (LCC) of BAT volume and in the three cohorts was above 0.950, except in one case (0.906; SUVpeak in overweight/obese adults; HU: NA, SUV: 2.0; Table S2). When BARCIST 1.0 criteria were applied, the LCC were 0.962–0.996, 0.980–0.996 and 0.983–1.000, for BAT volume, SUVmean, and SUVpeak, respectively (Table S2).
The combination of HU and SUV thresholds markedly affects estimation of BAT volume and activity across different cohorts
Representative images of BAT volume and activity of the three study cohorts resulting from different HU and SUV threshold combinations are shown in Fig. 1. Firstly, we determined the quantitative effect of the four threshold combinations on BAT volume in young lean adults (Fig. 2A), young overweight/obese adults (Fig. 2B), and middle-aged overweight/obese adults (Fig. 2C). Compared to the BARCIST 1.0 criteria, higher BAT volumes were consistently observed using the HU: NA; SUV: 2.0 criteria in young lean adults [+155%; 249 (186, 312) ml; mean (95% CI)], young overweight/obese adults [+207%; 244 (114, 374) ml], and middle-aged overweight/obese adults [+124%; 106 (42, 170) ml]. In contrast, BAT volumes estimated with the HU: -250, -50; SUV: 2.0 criteria compared to the BARCIST 1.0 criteria, yielded significantly smaller values in young lean adults [-57%; 92 (79, 106) ml], young overweight/obese adults [-42%; 49 (29, 70) ml], and middle-aged overweight/obese adults [-54%; 46 (28, 64) ml] (see Table S3). No significant differences were observed between BAT volumes estimated by HU: -180, -10; SUV: 1.5 criteria compared to BARCIST 1.0 criteria in young lean adults [0%; 0 (-5, 5) ml], however, we found higher BAT volumes in young overweight/obese adults [+40%; 47 (24, 69) ml] and middle-aged overweight/obese adults [+45%; 38 (18, 58)].

Representative images of brown adipose tissue volume and activity of the three study cohorts by threshold of Hounsfield units (HU) and standardized uptake value (SUV). Blue dots indicate BAT volume and red dots indicate maximal BAT activity (SUV max). BMI: Body mass index; HU: Hounsfield units; NA: Not applied; SUV: Standardized uptake value.

Brown adipose tissue (BAT) volume and activity determined by various thresholds of Hounsfield unit (HU) and Standardized uptake value (SUV) for three study cohorts. BAT volume (A–C), SUVmean (D–F), and SUVpeak (G–I) were determined in young lean adults (A,D,G), young overweight/obese adults (B,E,H), and middle-aged overweight/obese adults (C,F,I). Data are means and standard deviation (n = 10 per cohort). Significant differences between thresholds are indicated by parallel horizontal bars (all P ≤ 0.05). BARCIST 1.0: HU:-190, -10; SUV: Individualized [1.2/(lean body mass/body mass)]; BMI: Body mass index; NA: Not applied. See Table S4 for exact absolute and relative differences between thresholds.
HU and SUV thresholds moderately affect estimation of BAT activity (SUVmean) across different cohorts
We next determined the effect of the four threshold combinations on SUVmean in young lean adults (Fig. 2D), young overweight/obese adults (Fig. 2E), and middle-aged overweight/obese adults (Fig. 2F). Compared to the BARCIST 1.0 criteria, higher SUVmean were observed using the HU: -250, -50; SUV: 2.0 criteria in young lean adults [+18%; 0.8 (0.9–0.6) g/ml] and in middle-aged overweight/obese adults [+13%; 0.3 (0.2–0.5) g/ml]. In young lean adults, a lower SUVmean was estimated using the HU: NA; SUV: 2.0 criteria compared to BARCIST 1.0 criteria [-9%; 0.4 (0.2, 0.6) g/ml]. Lower BAT activity was detected using HU: -180, -10; SUV: 1.5 criteria against BARCIST 1.0 criteria in young overweight/obese adults [-14%; 0.5 (0.4, 0.7) g/ml] and middle-aged overweight/obese adults [-11%; 0.3 (0.2–0.4) g/ml] (Table S3).
HU and SUV thresholds slightly affect estimation of maximal BAT activity (SUVpeak) values across different cohorts
In addition, we determined the effect of the four threshold combinations on SUVpeak in young lean adults (Fig. 2G), young overweight/obese adults (Fig. 2H), and middle-aged overweight/obese adults (Fig. 2I). We found similar results in the SUVpeak values (all P > 0.05), however, there were significant differences in the middle-aged overweight/obese adults, where SUVpeak values calculated with HU: NA; SUV: 2.0 criteria were higher than calculated with BARCIST 1.0 criteria [+10%; 0.6 (0.2, 0.9) g/ml]. Figure S2 shows means and 95% CI of BAT volume and activity determined by various thresholds of HU and SUV for the three study cohorts.
Discussion
To our knowledge, the present study is the first empirical investigation to compare and quantify BAT volume and activity following BARCIST 1.0 criteria against the most used HU and SUV thresholds in three independent cohorts of men of different age and BMI. We observed that BAT volume calculated using the HU: NA; SUV: 2.0 criteria may differ up to 2.6-fold, 3.1-fold, and 2.2-fold from the BAT volume calculated based on BARCIST 1.0 criteria in young normal-weight, young overweight/obese, and middle-aged overweight/obese adults, respectively. Similarly, BAT activity (expressed as SUVmean), based on BARCIST 1.0 criteria differed up to 18% and 13% when compared with BAT activity based on the HU: -250, -50; SUV: 2.0 criteria, for young lean adults and middle-aged overweight/obese adults, respectively. On the other hand, differences were not significant when maximal BAT activity was expressed as SUVpeak for young cohorts, while we found that SUVpeak based on the HU: NA; SUV: 2.0 was 10% higher than calculated with BARCIST 1.0 criteria in middle-aged overweight/obese adults. The findings of this study show that human BAT volume and to a lesser extent BAT activity (expressed as SUVmean) depend largely on the selected HU and SUV thresholds. Moreover, we observed that the various threshold combinations similarly influenced BAT volume and BAT activity (SUVmean) in the three cohorts independently of age, BMI or different methodologies applied to activate and measure BAT17.
HU and SUV thresholds markedly affect BAT volume across different cohorts
The scientific community has been speculating about the volume of BAT that is present in adult men, and showed mean values of approx. 70 ml3, 100 ml2,18, 300 ml19, and 450 ml20. This highlights the knowledge gap regarding the amount of BAT present in adults and that maximizing its volume and metabolic activity could impact human physiology. We found that the highest BAT volumes were consistently observed with those thresholds that did not apply a criterion for HU (i.e. HU: NA, SUV: 2.0). Because the gold standard to quantify BAT is the 18F-FDG-PET in combination with CT, it is evident that a threshold of HU should be applied, although the most appropriate threshold of HU remains to be elucidated. We observed lower BAT volumes with the most frequently used threshold combination in literature (HU: -250, -50, SUV: 2.0) compared to BARCIST 1.0. These differences could be based on the fact that BARCIST 1.0 uses an HU range starting at -10 while the most commonly protocol used an HU range starting at -50, albeit it is known that the range of adipose tissue in the CT images starts at an HU value of -1011,21. Moreover, it was recently shown22 that the density of the BAT might change after a cold exposure, especially in the range from -50 to -10. Actually, it is not feasible to distinguish BAT from WAT or other tissues using exclusively CT criteria. Thus, more studies are needed to increase our understanding of BAT density measured by a CT scan23.
The main advantage of the BARCIST 1.0 recommendations is the inclusion of an individualized SUV threshold adapted to the individual’s lean body mass. Estimated BAT volumes did not differ between BARCIST 1.0 and HU: -180, -10; SUV: 1.5 criteria in the young lean adults, probably because the SUV criteria were virtually identical using both thresholds (1.54 ± 0.09 vs. 1.5 g/ml, respectively). Nevertheless, we found higher estimated BAT volume with HU: -180, -10; SUV: 1.5 compared to BARCIST 1.0, because the SUV threshold applied in BARCIST was higher for young overweight/obese adults and middle-aged overweight/obese adults (1.98 ± 0.17 g/ml and 1.75 ± 0.15 g/ml, Table 1). Therefore, the relative changes in BAT volume are largely influenced by the use of a SUV threshold corrected by lean body mass1,11.
HU and SUV thresholds moderately affect BAT activity (SUVmean) across different cohorts
SUVmean is the average SUV within a volume, therefore, if BAT volume differs due to HU or SUV thresholds in the three cohorts, SUVmean is also expected to differ by the thresholds selection. Indeed, SUVmean is not consistent across studies as it is influenced by many methodological factors as described previously17 such as cooling protocols or instruments, as well as study populations8,9. We showed that when a SUV individualized threshold was used and the SUV values are alike (such as HU: -180, -10; SUV: 1.5 criteria in young lean adults), then the SUVmean values are similar. However, we observed that an application of a higher SUV threshold results in higher SUVmean values, regardless of the HU thresholds applied or the cohort studied because the SUV threshold of 2.0 includes higher 18F-FDG uptake of BAT deposits. On the other hand, when an HU threshold was omitted (i.e. HU: NA; SUV: 2.0 criteria), the SUVmean values were lower regardless of the cohort studied. In this case, all 18F-FDG present in the selected ROIs of the PET images is used for quantification of BAT activity even though part of 18F-FDG would represent uptake by other tissues that were not excluded for the analysis due to lack of HU criteria.
HU and SUV thresholds slightly affect maximal BAT activity (SUVpeak) values across different cohorts
BARCIST 1.0 recommends to report SUVpeak instead of SUVmax to avoid overestimation in the quantification of BAT activity1, because SUVmax is the single highest uptake pixel in the ROI and could easily be an outlier whereas SUVpeak is the highest average SUV in a 1 cc spherical volume, thereby reducing a potential effect of outliers. This sphere may, or may not, be centered on the highest SUVmax. Letiner et al.11 found that PET image resolution substantially influences observed BAT SUVmax but whether this resolution also affects SUVpeak in currently unknown. Compared to the BARCIST 1.0 criteria, we found similar SUVpeak values across thresholds in young lean men and overweight/obese men. However, differences were observed between the thresholds that did not use HU vs. all the other thresholds in middle-aged overweight-obese adults. This could be based on the lower amount of 18F-FDG injected with respect to the size/body weight of the participant [ratio between amount of 18F-FDG to BMI (6.8 ± 0.3, 6.5 ± 0.8, and 3.8 ± 0.3 MBq/(kg/m2) in young lean adults, young overweight/obese adults, and middle-aged overweight/obese adults, respectively]. Therefore, the distribution of the tracer among the various tissues may partially explain this finding. In fact, lower doses of 18F-FDG, as used in the cohort of middle-aged overweight/obese adults, may increase noise in the image and, therefore, raise SUVpeak levels1,8,9. We found that SUVmax was located in BAT regions irrespective of the threshold used in young lean and young overweight/obese men. However, in middle-aged overweight/obese men, SUVmax was found in an unexpected region when no threshold for HU was used. Therefore, omission of HU threshold may have resulted in an artificial SUVmax and consequently SUVpeak, especially in the middle-aged overweight-obese men who received a low dose of 18F-FDG. Similar differences between thresholds and cohort studies were found with SUVmax (data not shown). Therefore, in light of these findings, we support that SUVpeak is the most consistent BAT-related outcome between criteria in the three independently cohorts of adults.
Limitations
We quantified BAT in six different ROIs from cerebellum to thoracic vertebra 4 (Figure S1). Although most of the BAT detected in humans is localized in the areas covered by the selected ROIs11, we may have missed BAT depots in axillary, paraspinal or abdominal adipose tissue located in anatomical areas beneath the thoracic vertebra 411. Our ROIs did not include mouth, nose, or thyroid to avoid false positive results, yet, results persisted when a single ROI from cerebellum to thoracic vertebrae 4 was drawn and when HU criteria were applied (data not shown). In addition, we do not know if these findings can be replicated when the SUV threshold of BARCIST criteria is used in combination with other ranges of HU. Besides the selection of HU and SUV thresholds, quantification of human BAT volume and activity also depends on other methodological issues such as the cooling protocol, 18F-FDG-PET/CT methodology, segmentation software17, tracer used (18F-FDG vs. 18F-FTHA24), intrinsic factors of the participants such as age, sex, or body composition, or extrinsic factors as outdoor temperature25 or daily light26, which limit comparisons across studies. To improve the understanding of human BAT measured by 18F-FDG-PET/CT, the reconstruction settings should be harmonized in a similar manner as proposed by the EANM guidelines for 18F-FDG tumor PET imaging27. In the present study, the PET/CT scans from young overweight/obese adults did not follow these guidelines, therefore we cannot guarantee that the recovery coefficients of the used reconstructions are the same. Moreover, methodological differences between cohorts did not allow us to check whether differences between HU and SUV thresholds are of different magnitude. Also the use of different cooling techniques (cooling vests vs. mattresses) and protocols might have introduced some bias. This study included only healthy male adults. The results should be applicable to other populations, such as women and men with different fat distributions, although this should be verified by replication in other cohorts with larger sample size. Moreover, biopsies of BAT-classical depots would be necessary to identify the density window (in terms of HU) of this tissue in different populations.
Conclusions
BAT volume and activity as determined by 18F-FDG PET/CT highly depend on the quantification criteria used. Future human BAT studies should conduct sensitivity analysis with different thresholds in order to understand whether results are driven by the selected HU and SUV thresholds. According to our findings, when following an individualized cooling protocol, SUVpeak is the most consistent marker of maximal BAT activity across study cohorts independent of the HU and SUV threshold used, which may therefore facilitate comparisons across studies. The design of the present study precludes providing any conclusive threshold, but before more definitive thresholds for HU and SUV are available, we support the use of BARCIST 1.0 criteria to facilitate interpretation of BAT characteristics between research groups.
References
Chen, K. Y. et al. Brown Adipose Reporting Criteria in Imaging STudies (BARCIST 1.0): Recommendations for Standardized FDG-PET/CT Experiments in Humans. Cell Metab. 24, 210–222 (2016).
Cypess, A. M. et al. Identification and importance of brown adipose tissue in adult humans. N. Engl. J. Med. 360, 1509–17 (2009).
van Marken Lichtenbelt, W. D. et al. Cold-activated brown adipose tissue in healthy men. N. Engl. J. Med. 360, 1500–8 (2009).
Virtanen, K. A. et al. Functional brown adipose tissue in healthy adults. N. Engl. J. Med. 360, 1518–25 (2009).
Saito, M. et al. High incidence of metabolically active brown adipose tissue in healthy adult humans: effects of cold exposure and adiposity. Diabetes 58, 1526–1531 (2009).
Peirce, V. & Vidal-Puig, A. Regulation of glucose homoeostasis by brown adipose tissue. Lancet Diabetes Endocrinol. 1, 353–360 (2013).
Hoeke, G., Kooijman, S., Boon, M. R., Rensen, P. C. N. & Berbeé, J. F. P. Role of Brown Fat in Lipoprotein Metabolism and Atherosclerosis. Circ. Res. 118, 173–182 (2016).
Bauwens, M. et al. Molecular imaging of brown adipose tissue in health and disease. Eur. J. Nucl. Med. Mol. Imaging 41, 776–791 (2014).
van der Lans, A. A. J. J. et al. Cold-activated brown adipose tissue in human adults: methodological issues. AJP Regul. Integr. Comp. Physiol. 307, R103–R113 (2014).
Paulus, A., van Marken Lichtenbelt, W., Mottaghy, F. M. & Bauwens, M. Brown adipose tissue and lipid metabolism imaging. Methods 1–9 (2017). https://doi.org/10.1016/j.ymeth.2017.05.001.
Leitner, B. P. et al. Mapping of human brown adipose tissue in lean and obese young men. 6–11, https://doi.org/10.1073/pnas.1705287114 (2017).
Bakker, L. E. H. et al. Brown adipose tissue volume in healthy lean south Asian adults compared with white Caucasians: a prospective, case-controlled observational study. lancet. Diabetes Endocrinol. 2, 210–217 (2014).
Sanchez-Delgado, G. et al. Activating brown adipose tissue through exercise (ACTIBATE) in young adults: Rationale, design and methodology. Contemp. Clin. Trials 45, 416–25 (2015).
Martinez-Tellez, B. et al. A New Personalized Cooling Protocol to Activate Brown Adipose Tissue in Young Adults. Front. Physiol. 8, 1–10 (2017).
Schindelin, J. et al. Fiji: an open-source platform for biological-image analysis. Nat. Methods 9, 676–682 (2012).
Lin, L. I., McBride, G., Bland, J. M. & Altman, D. G. A proposal for strength-of-agreement criteria for Lin’s Concordance Correlation Coefficient. NIWA Client Rep. 45, 307–310 (2005).
Martinez-Tellez, B., Sanchez-Delgado, G., Boon, M. R., Rensen, P. C. N. & Ruiz, J. R. Activation and quantification of human brown adipose tissue: Methodological considerations for between studies comparisons. Eur. J. Intern. Med. 6–8, https://doi.org/10.1016/j.ejim.2017.02.006 (2017).
Vijgen, G. H. E. J. et al. Brown adipose tissue in morbidly obese subjects. PLoS One 6, 2–7 (2011).
Gerngroß, C., Schretter, J., Klingenspor, M., Schwaiger, M. & Fromme, T. Active brown fat during 18 FDG-PET/CT imaging defines a patient group with characteristic traits and an increased probability of brown fat redetection. J. Nucl. Med. jnumed. 116, 183988, https://doi.org/10.2967/jnumed.116.183988 (2017).
Yoneshiro, T. et al. Age-related decrease in cold-activated brown adipose tissue and accumulation of body fat in healthy humans. Obesity (Silver Spring). 19, 1755–60 (2011).
Baba, S., Jacene, H. A., Engles, J. M., Honda, H. & Wahl, R. L. CT Hounsfield Units of Brown Adipose Tissue Increase with Activation: Preclinical and Clinical. Studies. 51, 246–250 (2010).
Din, U. M. et al. Human Brown Fat Radiodensity Indicates Underlying Tissue Composition and Systemic Metabolic Health. J. Clin. Endocrinol. Metab. 102, 2258–2267 (2017).
Hu, H. H. & Gilsanz, V. Developments in the imaging of brown adipose tissue and its associations with muscle, puberty, and health in children. Front. Endocrinol. (Lausanne). 2, 33 (2011).
Blondin, D. P. et al. Selective Impairment of Glucose but Not Fatty Acid or Oxidative Metabolism in Brown Adipose Tissue of Subjects With Type 2 Diabetes. Diabetes 64, 2388–97 (2015).
Ouellet, V. et al. Outdoor temperature, age, sex, body mass index, and diabetic status determine the prevalence, mass, and glucose-uptake activity of 18F-FDG-detected BAT in humans. J. Clin. Endocrinol. Metab. 96, 192–199 (2011).
Kooijman, S. et al. Prolonged daily light exposure increases body fat mass through attenuation of brown adipose tissue activity. Proc. Natl. Acad. Sci. USA 112, 6748–53 (2015).
Boellaard, R. et al. FDG PET/CT: EANM procedure guidelines for tumour imaging: version 2. 0. 328–354, https://doi.org/10.1007/s00259-014-2961-x (2015).
Acknowledgements
The authors would like to thank all the participants who volunteered for this investigation. We are grateful to Ms. Carmen Sainz Quinn for assistance with the English language. This study is part of a Ph.D. Thesis conducted in the Biomedicine Doctoral Studies of the University of Granada, Spain. The study was supported by the Spanish Ministry of Economy and Competitiveness, Fondo de Investigación Sanitaria del Instituto de Salud Carlos III (PI13/01393), and Retos de la Sociedad (DEP2016-79512-R), Fondos Estructurales de la Unión Europea (FEDER), by the Spanish Ministry of Education (FPU 13/04365), by the Fundación Iberoamericana de Nutrición (FINUT), by the Redes temáticas de investigación cooperativa RETIC (Red SAMID RD16/0022), by AstraZeneca HealthCare Foundation and by the University of Granada, Plan Propio de Investigación 2016, Excellence actions: Units of Excellence; Unit of Excellence on Exercise and Health (UCEES). Mariëtte R. Boon is supported by the Dutch DiabetesFoundation (grant 2015.81.1808). Patrick C.N. Rensen is an Established Investigator of the Dutch Heart Foundation (grant 2009T038). We also acknowledge the support from the Netherlands Cardiovascular Research Initiative: an initiative with support of the Dutch Heart Foundation for the GENIUS project ‘Generating the best evidence-based pharmaceutical targets for atherosclerosis’ (CVON2011-9).
Author information
Authors and Affiliations
Contributions
Conception and design of the experiments: B.M.T., K.J.N., GSD., G.A.V., F.H.V., L.P.A.B., P.C.N.R., M.R.B., and J.R.R. Collection, analysis, and interpretation of data: B.M.T., K.J.N., G.S.D., G.A.V., J.M.L., F.H.V., L.P.A.B., P.C.N.R., M.R.B and J.R.R. Drafting the article or critical revision for intellectual content: B.M.T., K.J.N., G.S.D., G.A.V., J.M.L., F.H.V., L.P.A.B., P.C.N.R., M.R.B and J.R.R.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Martinez-Tellez, B., Nahon, K.J., Sanchez-Delgado, G. et al. The impact of using BARCIST 1.0 criteria on quantification of BAT volume and activity in three independent cohorts of adults. Sci Rep 8, 8567 (2018). https://doi.org/10.1038/s41598-018-26878-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-26878-4
This article is cited by
-
Association of apolipoprotein M and sphingosine-1-phosphate with brown adipose tissue after cold exposure in humans
Scientific Reports (2022)
-
Fecal microbiota composition is related to brown adipose tissue 18F-fluorodeoxyglucose uptake in young adults
Journal of Endocrinological Investigation (2022)
-
No evidence of brown adipose tissue activation after 24 weeks of supervised exercise training in young sedentary adults in the ACTIBATE randomized controlled trial
Nature Communications (2022)
-
Low-dose 18F-FDG TOF-PET/MR for accurate quantification of brown adipose tissue in healthy volunteers
EJNMMI Research (2020)
-
Distribution of Brown Adipose Tissue Radiodensity in Young Adults: Implications for Cold [18F]FDG-PET/CT Analyses
Molecular Imaging and Biology (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
