
Abstract
Hypertension and diabetes mellitus (DM) have become major public health issues, and previous studies have shown that there is an association between hypertension and DM. However, there is a lack of detailed information about this association. This study aimed to explore how different blood pressure (BP) levels were associated with fasting blood glucose (FBG) levels. A cross-sectional survey with adults aged 18 to 79 years was conducted in Jilin Province, China in 2012. Lambda-mu-sigma (LMS) was used to preliminarily explore the associations of BP with FBG. Quantile regression (QR) was performed to identify the specific associations by adjusting for confounding factors. The distributions of systolic blood pressure (SBP) (χ2 = 710.76, P < 0.001) and diastolic blood pressure (DBP) (χ2 = 460.20, P < 0.001) were different according to gender. LMS showed that the associations of BP with FBG became stronger when the FBG levels were close to 5.6 mmol/L. QR showed that FBG was positively associated with SBP (P30 to P90) and DBP (P20 to P90) in males. In females, FBG was positively associated with SBP from only P85 to P90. In summary, FBG was positively associated with BP in a gender-dependent manner.
Similar content being viewed by others

Introduction
Currently, both hypertension and diabetes mellitus (DM) are serious global public health issues1,2,3, and previous studies have shown that there is an association between hypertension and DM4,5. On the one hand, patients with DM are at increasing risk of developing hypertension compared to those without DM6,7. On the other hand, the association between hypertension and DM may increase the risk of the co-occurrence of these two diseases, and then the interaction of these two diseases could lead to new public health issues, such as increasing the risk of the development of stroke8. Moreover, among DM patients with hypertension, insulin resistance is an independent risk factor for ischaemic cerebral infarction, especially lacunar infarction9. Furthermore, the combination of hypertension and DM can significantly increase circadian rhythm abnormalities and target organ damage10.
Many studies have focused on the association between hypertension and DM, and most of them have treated blood pressure (BP) and fasting blood glucose (FBG) as categorical variables (transforming the data into “normal” and “abnormal”)4,11. However, the occurrence and development of hypertension is a continuous and long-term process. BP, a sensitive index for diagnosing hypertension, can reflect the progression of hypertension to some extent. Yet no study has fully reflected the whole distribution of BP, and studies on the association of BP with FBG have been inadequate12. There still exists a huge gap in our understanding on the association of BP with FBG.
In view of the above facts, it was a challenge to explore the association of BP with FBG by using the whole distribution of BP rather than the average BP with conventional methods (such as logistic regression). Fortunately, the lambda-mu-sigma (LMS) and quantile regression (QR) methods are well suited to solving this problem. Therefore, in this study we aimed to explore the associations of different levels of BP with FBG by using LMS and QR methods based on a cross-sectional study in Jilin Province, China.
Results
Descriptive characteristics of participants by gender
In total, 11,878 subjects were enrolled in the study, with 5,571 males and 6,307 females. As shown in Table 1, BMI, WC, SBP, DBP and FBG were all significantly higher in males than those in females (P < 0.05), and females were older than males (P < 0.05). There were significant differences between males and females in the distributions of alcohol consumption, smoking status and dyslipidaemia (P < 0.05) as well.
Distribution of BP in males and females
Figure 1 shows the distributions of SBP (χ2 = 710.76, P < 0.001) and DBP (χ2 = 460.20, P < 0.001) by gender, and there were significant differences between males and females (hypotension was merged into normal BP due to the small population). Table 2 shows the quantiles of SBP and DBP, and the levels of BP were different according to gender. Therefore, the following results were analysed separately in males and females.

Distribution of BP in males and females. *Px: percentile x; SBP: systolic blood pressure; and DBP: diastolic blood pressure.
Results of LMS analysis
The smoothed percentile curves of SBP and DBP in males and females are shown separately in Figs 2 and 3. The shapes of the curves were different according to gender, and all the percentiles of BP in males were substantially and consistently higher compared with those in females. Moreover, the associations of BP with FBG became stronger when the FBG levels were close to 5.6 mmol/L.

Smoothed SBP percentile curves for males and females.

Smoothed DBP percentile curves for males and females.
Results of the QR model in males
The coefficients of FBG in different quantiles of SBP and DBP are shown separately in Tables 3 and 4. Table 3 shows that there were positive associations of SBP with FBG, and the coefficients increased from P10 to P90 (model 1). In addition, FBG was positively associated with SBP from P30 to P90 after adjusting for age, BMI, WC, smoking status, alcohol consumption and dyslipidaemia (model 2). Table 4 shows that FBG was positively associated with DBP from P20 to P90 (model 1). In addition, FBG was still positively associated with DBP from P20 to P90 after adjusting for age, BMI, WC, smoking status, alcohol consumption and dyslipidaemia (model 2).
Results of the QR model in females
The coefficients of FBG in different quantiles of SBP and DBP are shown separately in Tables 5 and 6. As shown in Table 5, FBG was positively associated with SBP from P10 to P90 (model 1), whereas FBG had positive associations with SBP from only P85 to P90 after adjusting for age, BMI, WC, smoking status, alcohol consumption and dyslipidaemia (model 2). As shown in Table 6, there were positive associations of DBP with FBG from P10 to P30 and from P75 to P90 (model 1). Yet the associations of DBP with FBG were not statistically significant after adjusting for age, BMI, WC, smoking status, alcohol consumption and dyslipidaemia (model 2).
Discussion
The findings of this study could be summarized as follows. First, there were positive associations of BP with FBG, and the associations were different according to gender. FBG was associated with BP in almost all quantiles in males, while in females, only SBP in high quantiles had positive associations with FBG. Second, the associations of BP with FBG became stronger when the FBG levels were close to 5.6 mmol/L.
In our study, we found that FBG was positively associated with BP, which was consistent with the results of similar previous studies13,14. The possible mechanism is that as the FBG level increases, hyperglycaemia with insulin resistance, overweight and metabolic disorders could alter the rennin-angiotensin system (RAS), then leading to an effect on BP15,16.
In addition, we found that the associations of BP with FBG were different in males and females; FBG was positively associated with both SBP and DBP in almost all quantiles in males, whereas FBG had positive associations with only SBP in the high quantiles in females. The finding implied that the positive associations of BP with FBG were more notable in males than in females. There are several reasons for these associations. First, the risk of hypertension in females is lower than that in males17. Second, evidence has shown that the lower endogenous oestrogen levels found in males might be related to higher insulin resistance when compared with females18, which means that the same FBG levels in males and females may lead to different physiological effects due to different levels of insulin resistance. Thus, the finding might suggest that control of one’s FBG level should be more emphasized and strengthened among males than females, except females with high SBP.
The cut-off value for the definition of impaired fasting glycaemia (IFG) is still controversial at present; the American Diabetes Association (ADA) Expert Committee reduced the cut-off value of IFG to 5.6 mmol/L in 2003, while the World Health Organization (WHO) retained the previous cut-off value of IFG (6.1 mmol/L)19. Further, IFG has been shown as an independent risk factor for hypertension20,21; however, whether the FBG level begin to become a potential risk factor for hypertension when it is close to 5.6 mmol/L is uncertain. Fortunately, our study showed that the positive associations of BP with FBG became stronger when FBG levels were close to 5.6 mmol/L, which implied that FBG level might begin to become a potential risk factor for hypertension when it was close to 5.6 mmol/L. A possible explanation is that the body may develop hyperinsulinaemia before FBG level reaches 6.1 mmol/L, and the presence of hyperinsulinaemia could directly contribute to an elevation in BP by increasing renal sodium retention22. Therefore, having awareness of controlling FBG levels when they approach 5.6 mmol/L might have potential benefits, such as early control of BP. Furthermore, having awareness of controlling FBG levels might also assist in preventing the development of co-occurrence of hypertension and DM to some extent.
Some limitations should be noted in this study. First, participants in the study were from Jilin Province in Northeast China, and the results may not be generalizable to other areas. Second, some of the subjects were excluded because they did not suit the purpose of the study and/or they were with incomplete data on BP, thus, selection biases might be present. Third, other confounding factors (such as genes) may have impacted the results. Finally, the data were obtained from a cross-sectional survey; therefore, further studies are needed to explore the associations in a longitudinal setting.
Conclusions
There were positive associations of BP with FBG, and these associations were different according to gender. FBG was associated with BP in almost all quantiles in males, yet in females, FBG had positive associations with only SBP in the high quantiles. Moreover, the associations of BP with FBG became stronger when the FBG levels were close to 5.6 mmol/L.
Methods
Study population
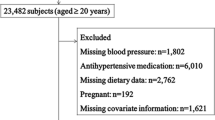
Data was derived from a cross-sectional study of chronic disease conducted by the Jilin University School of Public Health and the Jilin Department of Health in Jilin Province of China in 2012. In this study, a total of 23,050 subjects who had lived in Jilin Province for more than 6 months and were 18–79 years old were selected through multistage stratified random cluster sampling23. First, 1,615 subjects whose questionnaires were invalid were excluded. Second, 9,421 subjects were excluded because they did not suit the purpose of the study (4,993 subjects were not tested for FBG and 4,428 subjects controlled their BP and/or FBG level with medicine). Third, 136 subjects were excluded due to incomplete data on systolic blood pressure (SBP) (75 subjects) and diastolic blood pressure (DBP) (61 subjects). Finally, 11,878 subjects were included in this study (Fig. 4). All participants provided written informed consent, and the study was approved by the Institutional Review Board of the Jilin University School of Public Health. In addition, all analyses were performed in accordance with the relevant guidelines and regulations.

Flow diagram of the study design and participant selection process for this study.
Data Collection and Measurement
The data in this study were collected by investigators who had been uniformly trained. The information included demographics (gender, age), health-related behaviours (smoking status, alcohol consumption), anthropometric measurements (SBP, DBP and waist circumference (WC), etc.) and biochemical tests (FBG, total cholesterol (TC) and triglycerides (TG), etc.). BP was measured using a mercury sphygmomanometer by trained professionals, and the subjects were required to have rested for at least 5 min before BP was measured. Two readings of SBP and DBP were recorded, and the average values were used for the data analysis. If the first two measurements differed by more than 5 mmHg, additional readings were taken. FBG levels were measured by the Bai Ankang fingertip blood glucose monitor (Bayer, Leverkusen, Germany).
Serum lipid levels (TG, TC, low-density lipoprotein cholesterol (LDL-C), high-density lipoprotein cholesterol (HDL-C)) were measured by the MODULE P800 biochemical analysis machine (Roche Co., Ltd., Shanghai, China) in the morning after participants had fasted for 10 or more hours overnight. The participants’ height and weight were measured according to a standardized protocol with the participants wearing clothing but no shoes, and WC was measured at the midpoint between the lowest rib margin and the iliac crest with the participants standing. Body mass index (BMI) was calculated using the following formula: BMI = Weight (kg)/Height (m)2.
Assessment Criteria
Hypertension was defined as resting SBP ≥ 140 mmHg and/or DBP ≥ 90 mmHg; high-normal BP was defined as SBP 120–139 mmHg or DBP 80–89 mmHg; and normal BP was defined as SBP < 120 mmHg and DBP < 80 mmHg, with no antihypertensive treatment24. Smoking status was categorized into never smoker (had never smoked cigarettes or had smoked fewer than 100 cigarettes in one’s lifetime), former smoker (had smoked at least 100 cigarettes in one’s lifetime but was not currently smoking), and current smoker (had smoked at least 100 cigarettes in one’s lifetime and was still smoking)25. Alcohol consumption was defined as consuming any type of purchased or homemade alcohol-containing beverages on average more than once per week26. Regarding serum lipid level, any of the following criteria was defined as dyslipidaemia: high TC: TC ≥ 6.22 mmol/L; high TG: TG ≥ 2.26 mmol/L; low HDL-C < 1.04 mmol/L; and high LDL-C ≥ 4.14 mmol/L27.
Statistical Analysis
Continuous variables were presented as medians (inter-quartile range) because they did not have normal distributions. Wilcoxon rank sum tests were used to make comparisons according to gender. Categorical variables were presented as counts or percentages and compared with the Rao-Scott Chi-square test. Sex-specific percentile curves of BP with FBG were constructed by LMS method developed by Cole and Green28. The 3rd, 5th, 10th, 25th, 50th, 75th, 90th, 95th and 97th29 percentile BP curves were constructed to explore the associations of BP with FBG and to determine the general trend of those associations. QR, which is very flexible, especially for data with a heterogeneous conditional distribution, was performed to establish 2 models to explore how different BP levels were associated with FBG levels according to gender (model 2 was adjusted for age, BMI, WC, smoking status, alcohol consumption and dyslipidaemia). Meanwhile, QR was applied to build a series of regression equations in all quantiles of BP, and thus, the extreme data, such as the high BP quantiles, could be analysed30. R version 3.3.3 (University of Auckland, Oakland, New Zealand) was used to perform the statistical analyses. Statistical significance was set at P-value < 0.05.
Data Availability
The survey was implemented by School of Public Health, Jilin University and Jilin Center for Disease Control and Prevention in Jilin Province in 2012. According to the relevant regulations, we were sorry that the data can’t be shared.
References
Wang, C. et al. Prevalence of type 2 diabetes among high-risk adults in Shanghai from 2002 to 2012. Plos One 9, e102926 (2014).
NCD Risk Factor Collaboration (NCD-RisC). Effects of diabetes definition on global surveillance of diabetes prevalence and diagnosis: a pooled analysis of 96 population-based studies with 331,288 participants. Lancet Diabetes Endocrinol 3, 624 (2015).
Lim, S. S. et al. A comparative risk assessment of burden of disease and injury attributable to 67 risk factors and risk factor clusters in 21 regions, 1990–2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380, 2224 (2012).
Mancia, G. The association of hypertension and diabetes: prevalence, cardiovascular risk and protection by blood pressure reduction. Acta Diabetol 42(Suppl 1), S17 (2005).
Zhao, H., Zeng, F., Wang, X. & Wang, L. Prevalence, risk factors, and prognostic significance of masked hypertension in diabetic patients. Medicine (Baltimore) 96, e8363 (2017).
Adler, A. I. et al. Association of systolic blood pressure with macrovascular and microvascular complications of type 2 diabetes (UKPDS 36): prospective observational study. Bmj 321, 412 (2000).
Hypertension in Diabetes Study (HDS): II. Increased risk of cardiovascular complications in hypertensive type 2 diabetic patients. J Hypertens 11 319 (1993).
Ohishi, M. Hypertension with diabetes mellitus: physiology and pathology. Hypertens Res (2018).
Lee, J. E. et al. Insulin Resistance Is a Risk Factor for Silent Lacunar Infarction. Stroke 47, 2938 (2016).
Osawa, H. et al. Diabetes and hypertension markedly increased the risk of ischemic stroke associated with high serum resistin concentration in a general Japanese population: the Hisayama Study. Cardiovasc Diabetol 8, 60 (2009).
Yan, Q. et al. Association of blood glucose level and hypertension in Elderly Chinese Subjects: a community based study. Bmc Endocr Disord 16, 40 (2016).
Conen, D., Ridker, P. M., Mora, S., Buring, J. E. & Glynn, R. J. Blood pressure and risk of developing type 2 diabetes mellitus: the Women’s Health Study. Eur Heart J 28, 2937 (2007).
Di Bonito, P. et al. Fasting plasma glucose and clustering of cardiometabolic risk factors in normoglycemic outpatient children and adolescents. Diabetes Care 34, 1412 (2011).
Heianza, Y. et al. Fasting glucose and HbA1c levels as risk factors for the development of hypertension in Japanese individuals: Toranomon hospital health management center study 16 (TOPICS 16). J Hum Hypertens 29, 254 (2015).
Jia, G., DeMarco, V. G. & Sowers, J. R. Insulin resistance and hyperinsulinaemia in diabetic cardiomyopathy. Nat Rev Endocrinol 12, 144 (2016).
Zhou, M. S., Liu, C., Tian, R., Nishiyama, A. & Raij, L. Skeletal muscle insulin resistance in salt-sensitive hypertension: role of angiotensin II activation of NFkappaB. Cardiovasc Diabetol 14, 45 (2015).
Everett, B. & Zajacova, A. Gender differences in hypertension and hypertension awareness among young adults. Biodemography Soc Biol 61, 1 (2015).
Meyer, M. R., Clegg, D. J., Prossnitz, E. R. & Barton, M. Obesity, insulin resistance and diabetes: sex differences and role of oestrogen receptors. Acta Physiol (Oxf) 203, 259 (2011).
American Diabetes Association, Standards of Medical Care in Diabetes–2013. Diabetes CarE 36 S11 (2012).
Hayashi, T. et al. High normal blood pressure, hypertension, and the risk of type 2 diabetes in Japanese men. The Osaka Health Survey. Diabetes Care 22, 1683 (1999).
Vaidya, A. et al. A prospective study of impaired fasting glucose and type 2 diabetes in China: The Kailuan study. Medicine (Baltimore) 95, e5350 (2016).
Chavez-Canales, M. et al. Insulin increases the functional activity of the renal NaCl cotransporter. J Hypertens 31, 303 (2013).
Wang, C. et al. Awareness, treatment, control of diabetes mellitus and the risk factors: survey results from northeast China. Plos One 9, e103594 (2014).
Yip, G. W. et al. Oscillometric 24-h ambulatory blood pressure reference values in Hong Kong Chinese children and adolescents. J Hypertens 32, 606 (2014).
Schoenborn, C. A. & Adams, P. E. Health behaviors of adults: UnitedStates, 2005–2007. Vital Health Stat 10, 1 (2010).
He, H. et al. Dyslipidemia awareness, treatment, control and influence factors among adults in the Jilin province in China: a cross-sectional study. Lipids Health Dis 13, 122 (2014).
Ge, H. et al. The association between serum 25-hydroxyvitamin D3 concentration and serum lipids in the rural population of China. Lipids Health Dis 16, 215 (2017).
Cole, T. J. & Green, P. J. Smoothing reference centile curves: the LMS method and penalized likelihood. Stat Med 11, 1305 (1992).
Ma, J., Wang, Z., Song, Y., Hu, P. & Zhang, B. BMI percentile curves for Chinese children aged 7–18 years, in comparison with the WHO and the US Centers for Disease Control and Prevention references. Public Health Nutr 13, 1990 (2010).
Wei, Y., Pere, A., Koenker, R. & He, X. Quantile regression methods for reference growth charts. Stat Med 25, 1369 (2006).
Acknowledgements
This work was supported by the Natural Science Foundation of Science and Technology Department of Jilin Province, China (grant number: 20180101129JC); the Outstanding Youth Foundation of Science and Technology Department of Jilin Province, China (grant number: 20170520049JH); the National Natural Science Foundation of China (grant number: 11301213 and 11571068); the National Key Research and Development Program of China (grant number: 2016YFC1303800); and the Scientific Research Foundation of the Health Bureau of Jilin Province, China (grant number: 2011Z116).
Author information
Authors and Affiliations
Contributions
Yaogai Lv, Lina Jin and Yan Yao conceived the original idea for the study and designed the work. Lina Jin and Yan Yao provided valuable insight regarding the methodological approach and organization of the manuscript. Yaogai Lv, Junsen Ye, Xin Guo, Jing Dou and Li Shen carried out the statistical analyses and reviewed the consistency of data included in the paper. Yaogai Lv and Yan Yao drafted the manuscript. Anning Zhang, Zhiqiang Xue and Yaqin Yu revised the manuscript. All authors read and approved the final manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lv, Y., Yao, Y., Ye, J. et al. Association of Blood Pressure with Fasting Blood Glucose Levels in Northeast China: A Cross-Sectional Study. Sci Rep 8, 7917 (2018). https://doi.org/10.1038/s41598-018-26323-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-26323-6
This article is cited by
-
Association of blood pressure with fasting blood glucose in Indian adults: a secondary data analysis of a clinical, anthropometric, and biochemical survey
Journal of Public Health (2023)
-
Effect of fasting blood glucose on risk of new‐onset hypertension in rural Chinese population: a 15-year follow-up cohort
BMC Cardiovascular Disorders (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
