
Abstract
Mean platelet volume (MPV) was recently published as a possible marker of coronary artery disease in patients at high risk for major adverse cardiac events. Because platelets play an important role in atherosclerosis, we examined the relationship between critical limb ischemia (CLI) and MPV in patients with peripheral arterial occlusive disease (PAOD). Our study comprised 2124 PAOD patients. Univariate logistic regression was performed to analyze potential predictors for CLI. Nagelkerke’s R² is reported. Cross validation was performed using the leave-one-out principle. ROC analyses were performed to identify the best cut off value for MPV predicting CLI; to this end, Youden’s index was calculated. For CLI diabetes (p < 0.001, OR 2.44, 95% CI 1.97–3.02), hsCRP (p < 0.001, OR 1.01, 95% CI 1.01–1.01), age (p < 0.001, OR 1.05, 95% CI 1.04–1.06), thrombocytosis (p = 0.025, OR 1.84, 95%CI 1.08–3.14), and MPV (p = 0.003, OR 0.84, 95% CI 0.75–0.94) were significant independent predictors for CLI. ROC analysis (AUC: 0.55, 95% CI 0.52–0.58, p < 0.001) showed ≤10.2 as the best cut off value for MPV to predict CLI. As there is a significant relationship between low MPV and a high risk for CLI in PAOD patients, MPV can be used to identify patients who are likely to develop CLI.
Similar content being viewed by others


Introduction
Peripheral arterial occlusive disease (PAOD), a common disorder, must be diagnosed and treated promptly if progression to critical limb ischemia (CLI), with its high mortality and risk of limb amputation, is to be avoided1,2. Despite new and improved treatment options developed in recent years, CLI still often leads to amputation and/or death3,4.
Platelets play a crucial role in the development of CLI, as there is a high risk for vascular endpoints with a high platelet count. We recently demonstrated that even after adjustment for other well-established vascular risk factors, there was an odds ratio (OR) of 1.9 (95% CI 1.7–2.1) for CLI with a platelet-to-lymphocyte ratio (PLR) of > 1505. Our supposition is an interaction of platelets with endothelial cells and leukocytes6, with release of inflammatory agents and subsequent adhesion and transmigration of monocytes7, whereby the latter are involved in the inflammatory processes that lead to atherosclerosis8.
In recent years MPV has been discussed as a potential marker to identify atherosclerosis patients at high risk for an unfavorable outcome. Coronary artery disease (CAD) patients with high MPV seem to be at an especially high risk of death compared to those with low MPV9. The respective authors attribute their finding mainly to the denser granules found in larger platelets that seem to express more adhesive receptors, so leading to a more thrombotic state10.
As CLI has not yet been included as a vascular endpoint in published studies, and since platelets seem to be substantially involved in vascular disease, we looked into the association of MPV with CLI and other vascular endpoints in our PAOD cohort.
Methods
Our retrospective analysis included 2124 consecutive PAOD patients seen at our angiological service from 2005 to 2010. Our only inclusion criterion was treatment for PAOD at our department during this time period; there were no exclusion criteria.
The International Review Board, Medical University of Graz, Austria, approved the study (IRB Number 24–506 ex 11/12); as performed, the study conformed completely to all relevant guidelines and regulations. The ethics committee deemed that this retrospective analysis of blinded data required neither written nor verbal consent.
Following diagnosis and grading of PAOD on the basis of clinical examination, ankle brachial index (ABI) and duplex scan at our outpatient clinic, patients were scheduled for inpatient treatment of atherosclerotic disease. The Fontaine classification was used to grade PAOD. CLI was present in PAOD patients with ischemic rest pain and/or skin ulceration/gangrene corresponding to Fontaine classes 3 and 411.
After admission, patients’ records were analysed for cardiovascular risk factors and co-morbidities with a standardized questionnaire. Clinical symptoms were assessed with a physical examination. Blood for laboratory studies was drawn after an overnight fast.
Statistical analyses
Data are presented as mean and standard deviation (SD) or median and interquartile range (IQR) for continuous data and as a frequency for categorical data. To analyze potential predictors for CLI the following variables were analyzed using univariate binary logistic regression using a logit function: clopidogrel treatment (yes/no), acetylsalicylate treatment (yes/no), diabetes (yes/no), thrombocytosis (yes/no), sex (female/male), hsCRP level, age, and MPV. Significant variables in univariate analyses were selected for multivariate logistic regression. Variables in the final model were selected with a backward stepwise procedure. The decision to remove variables was based on a likelihood-ratio test. Nagelkerke’s R² is reported. For the comparision of the impact of the different significant variables the absolute value of standardized estimates. Cross validation was performed using the leave-one-out principle. A p-value of less than 5% was considered significant. ROC analyses were performed to identify the best cut off value to predict CLI for MPV; to this end, Youden’s index was calculated. Further vascular endpoints tested similarly to CLI were myocardial infarction and stroke. For data analysis SPSS 23.0.0.2 (SPSS Inc, Chicago, IL) and SAS 9.4 (2002–2012 by SAS Institute Inc., Cary, NC, USA) were used.
The datasets analyzed during the study are available from the corresponding author on reasonable request.
Results
Patient’s characteristics are given in
Calculations for endpoint CLI: According to univariate analysis, higher age (p < 0.001), higher hsCRP values (p < 0.001), female sex (p < 0.001), presence of diabetes (p < 0.001), no clopidogrel treatment (p = 0.004), no acetylsalicylate treatment (p = 0.003), lower MPV values (p < 0.001), and presence of thrombocytosis (p < 0.001) were associated with an increased risk of CLI Table 1. Multivariate logistic regression analysis (R² = 0.199) revealed that presence of diabetes (p < 0.001, OR: 2.4 95%CI: 2.0–3.0) and thrombocytosis (p = 0.025, OR: 1.84 95%CI: 1.08–3.14), higher hsCRP (p < 0.001, OR: 1.012 95%CI: 1.008–1.014) and age (p < 0.001, OR: 1.05 95%CI: 1.04–1.06) and lower MPV (p = 0.003, OR: 0.84 95%CI: 0.75–0.94) were significant variables associated with CLI (Table 2) with highest absolute values of standardized estimates for age (0.31) hsCRP (0.23) and presence of diabetes (0.23). The area under the ROC curve for the naive prediction model for CLI was 0.746 (95% CI: 0.723–0.769), and 0.742 (95% CI: 0.719–0.765) after cross-validation.
Occurrence of myocardial infarction (MCI) and stroke were investigated in the same cohort as described above. According to univariate analysis, higher age (p = 0.007), higher hsCRP values (p = 0.001), presence of diabetes (p = 0.004) and clopidogrel treatment (p = 0.016) were associated with an increased risk of MCI. Multivariate logistic regression analysis (R² = 0.05) revealed that higher age (p = 0.008, OR: 1.03 95%CI: 1.01–1.05), higher hsCRP values (p = 0.005, OR: 1.005 95%CI: 1.002–1.009), presence of diabetes (p = 0.011, OR: 1.75 95%CI: 1.14–2.69) and clopidogrel treatment (p = 0.002, OR: 1.96 95%CI: 1.27–3.04) were significant predictors for MCI (Table 3) with highest absolute values of standardized estimates for age (0.18) and clopidogrel treatment (0.18). The area under the ROC curve for the naive prediction model for MCI was 0.680 (95% CI: 0.624–0.737) after cross-validation. According to univariate analysis, higher hsCRP values (p = 0.002), clopidogrel treatment (p = 0.016) and no acetylsalicylate treatment (p = 0.001) were associated with an increased risk of stroke. Multivariate logistic regression analysis (R² = 0.02) revealed that higher hsCRP values (p = 0.002, OR: 1.005 95%CI: 1.002–1.008), clopidogrel treatment (p = 0.025, OR: 1.453 95%CI: 1.048–2.014) and no acetylsalicylate treatment (p = 0.010, OR: 0.652 95%CI: 0.47–0.90) were significant predictors for stroke with similar absolute values of standardized estimates for all predictors (hsCRP: 0.10; clopidogrel treatment: 0.10; acetylsalicylate treatment: 0.11) (Table 4). The area under the ROC curve for the naive prediction model for stroke was 0.658 (95% CI: 0.600–0.716) after cross-validation.
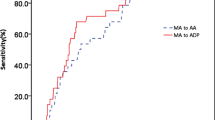
ROC analysis (AUC: 0.55, 95%CI: 0.52–0.58; p < 0.001) revealed a cut-off of ≤10.2 fL for MPV to best predict CLI (sensitivity: 65%, specificity: 42%, positive predictive value: 71%, negative predictive value: 36%). As MPV was not associated with MI and stroke, ROC analyses were not performed for these endpoints.
Discussion
Our study demonstrates a significant association of low MPV with higher occurrence of CLI in a large number of PAOD patients
Our findings are partly in contrast to the literature published in the field of atherosclerosis, mainly evaluating death, MI, and stroke as endpoints. We therefore calculated not only CLI as an endpoint in our data; we also evaluated our PAOD patients for MI and stroke as well. In our cohort neither endpoint, high nor low, was associated with MPV. We know, however, that stroke and MI patients differ from PAOD patients. Usually PAOD patients are older than CAD patients; however, when age was included in our regression analysis, low MPV was still associated with elevated CLI rates.
Recently high MPV was only investigated for mortality in a hemodialysis cohort. In nearly 150 000 patients, high MPV was associated with a higher risk for death and low MPV was associated with a lower death risk, even in multivariate analyses12. Possible reasons for the association of high MPV with cardiovascular endpoints were found in the Gutenberg Health Study. MPV was published in this study as a possible marker for platelet activation and arterial stiffness13. In this context, recently the white blood cell-to-mean platelet volume ratio (WMR) was found to be associated with a poorer outcome in over 3000 patients with ST-segment elevation myocardial infarction, so that low MPV was associated with a poorer outcome in CAD patients14.
Platelets are importantly involved in the progression of atherosclerosis. Current research suggests an interaction between platelets and endothelial cells and leukocytes6, with release of inflammatory agents and subsequent adhesion and transmigration of monocytes7, whereby the latter are involved in the inflammatory processes that lead to atherosclerosis8.
Thrombus formation in PAOD is mainly aggravated after plaque rupture by thrombogenic plaque components that set in motion an avalanche of aggregating platelets and fibrin strand formation, critically triggered by platelet-derived tissue factor (TF) based thrombin generation via feedback activation of coagulation loops15.
Recent studies have suggested an association not only of platelets but also of platelet-derived microparticles with arterial thrombi that form and progress when there is frank atherosclerosis or vascular injury16. The procoagulant activity of TF, whether bloodborne or derived from plaque, is an important feature of these MP, which accordingly play a major part in hemostasis and thrombosis17. This may strongly support our finding since platelets with MPV < 10.2 fL can be considered as “MP” themselves providing enormous enlargement of surface activity and allowing for higher cross-reactivity with TF and receptors for platelet aggregation and subsequent thrombus formation.
Our study has two main drawbacks: the retrospective design and elevated MPV calculated from a single blood sample, as this does not allow assessment of MPV over time.
In a large number of PAOD patients we were, however, able to show for the first time that low MPV is associated with CLI but not with MI and stroke. One possible explanation might be an MP-like pathway initiated by small platelets.
References
Bertomeu, V. et al. Prevalence and prognostic influence of peripheral arterial disease in patients or = 40 years old admitted into hospital following an acute coronary event. Eur. J. Vasc. Endovasc. Surg. 36, 189–196 (2008).
Norgren, L. et al. Inter-Society Consensus for the Management of Peripheral Arterial Disease (TASC II). J. Vasc. Surg. 45, Suppl: S5–67 (2007).
Novo, S., Coppola, G. & Milio, G. Critical limb ischemia: definition and natural history, current drug targets. Cardiovasc. Hematol. Disord. Drug Targets 4, 219–225 (2004).
Bertele, V., Roncaglioni, M. C., Pangrazzi, J., Terzian, E. & Tognoni, E. G. Clinical outcome and its predictors in 1560 patients with critical leg ischaemia. Eur. J. Vasc. Endovasc. Surg. 18, 401–410 (1999).
Gary, T. et al. Platelet-to-lymphocyte ratio: a novel marker for critical limb ischemia in peripheral arterial occlusive disease patients. PloS One 8, e67688 (2013).
Gawaz, M., Langer, H. & May, A. E. Platelets in inflammation and atherogenesis. J. Clin. Invest. 115, 3378–3384 (2005).
Lindemann, S., Kramer, B., Seizer, P. & Gawaz, M. Platelets, inflammation and atherosclerosis. J. Thromb. Haemost. 5(Suppl), 203–211 (2007).
Huo, Y. et al. Circulating activated platelets exacerbate atherosclerosis in mice deficient in apolipoprotein E. Nat. Med. 9, 61–67 (2003).
Sansanayudh, N. et al. Prognostic effect of mean platelet volume in patients with coronary artery disease. A systematic review and meta-analysis. Thromb. Haemost. 114, 1299–1309 (2015).
Bath, P. M. & Butterworth, R. J. Platelet size: measurement, physiology and vascular disease. Blood Coagul. Fibrinolysis 7, 157–161 (1996).
Hirsch, A. T. et al. ACC/AHA 2005 guidelines for the management of patients with peripheral arterial disease (lower extremity, renal, mesenteric, and abdominal aortic): executive summary a collaborative report from the American Association for Vascular Surgery/Society for Vascular Surgery, Society for Cardiovascular Angiography and Interventions, Society for Vascular Medicine and Biology, Society of Interventional Radiology, and the ACC/AHA Task Force on Practice Guidelines (Writing Committee to Develop Guidelines for the Management of Patients With Peripheral Arterial Disease) endorsed by the American Association of Cardiovascular and Pulmonary Rehabilitation; National Heart, Lung, and Blood Institute; Society for Vascular Nursing; TransAtlantic Inter-Society Consensus; and Vascular Disease Foundation. J. Am. Coll. Cardiol. 47, 1239–1312 (2006).
Kim, S. et al. Mean platelet volume and mortality risk in a national incident hemodialysis cohort. Int. J. Cardiol. 220, 862–870 (2016).
Panova-Noeva, M. et al. Mean platelet volume and arterial stiffness - clinical relationship and common genetic variability. Sci. Rep. 7, 40229 (2017).
Cicek, G., Acikgoz, S. K., Yayla, C., Kundi, H. & Ileri, M. White blood cell count to mean platelet volume ratio: A novel and promising prognostic marker for ST-segment elevation myocardial infarction. Cardiol. J. 23, 225–235 (2016).
Bernlochner, I. et al. A 2-step mechanism of arterial thrombus formation induced by human atherosclerotic plaques. J. Am. Coll. Cardiol. 55, 1147–58 (2010).
Suades, R., Padro, T., Vilahur, G. & Badimon, L. Circulating and platelet-derived microparticles in human blood enhance thrombosis on atherosclerotic plaques. Thromb. Haemost. 108, 1208–1219 (2012).
Mackman, N. Role of tissue factor in hemostasis, thrombosis, and vascular development. Arterioscler. Thromb. Vasc. Biol. 24, 1015–22 (2004).
Acknowledgements
We want to thank Eugenia Lamont for her English language editing service.
Author information
Authors and Affiliations
Contributions
P.R., T.G., R.B.R., F.H., M.S., M.W. and M.B. wrote the main manuscript text; A.A. performed the statistical analysis and prepared Tables 1–4. All authors reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rief, P., Raggam, R.B., Avian, A. et al. Low mean platelet volume is associated with critical limb ischemia in peripheral arterial occlusive disease. Sci Rep 8, 6718 (2018). https://doi.org/10.1038/s41598-018-25058-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-25058-8
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
