
Abstract
Acute myeloid leukemia (AML) is a heterogeneous disease. One reason for the heterogeneity may originate from inter-individual differences in the responses of leukemic cells to endogenous cytokines. On the basis of mathematical modeling, computer simulations and patient data, we have provided evidence that cytokine-independent leukemic cell proliferation may be linked to early relapses and poor overall survival. Depending whether the model of cytokine-dependent or cytokine-independent leukemic cell proliferation fits to the clinical data, patients can be assigned to two groups that differ significantly with respect to overall survival. The modeling approach further enables us to identify parameter constellations that can explain unexpected responses of some patients to external cytokines such as blast crisis or remission without chemotherapy.
Similar content being viewed by others


Introduction
Acute myeloid leukemias (AML) comprise a heterogeneous group of malignant diseases. Since major clinical symptoms originate from impairment of healthy blood cell production, it is important to understand how leukemic cells interfere with healthy hematopoiesis. Clinical and genetic observations reveal a strong heterogeneity among individual patients. One reason for the observed heterogeneity may be differences in cytokine dependence of leukemic cells, i.e., cells of some patients require cytokines to expand (cytokine-dependent leukemic cells) whereas others exhibit autonomous (cytokine-independent) growth.
The idea that cytokine dependence of leukemic cells differs between patients is supported by experimental results. Xenotransplantation assays reveal that some leukemia samples exclusively engraft in mice transgenic for human cytokines and not in standard NSG mice1,2. Similarly, in vitro studies imply that leukemic cells of some patients exhibit autonomous growth in cell cultures whereas others require cytokines to expand3,4,5. The correlation between cytokine-dependence in cell culture and patient survival suggests that cytokine dependence of leukemic cells may be a clinically meaningful parameter4,5. However, it can depend on the culture conditions whether a leukemia sample exhibits autonomous growth or not3. Clinical trials also suggest that cytokine dependence of leukemic cells differs between patients. In principle, exogenous cytokine administration could recruit cytokine-dependent leukemic cells into cell cycle and thus increase efficacy of S-phase specific cytotoxic drugs3. However, clinical trials show that this approach, also referred to as “priming”, works in some but not in all patients. Some trials report an improved rate of complete remission, disease free survival and rarely also overall survival after priming6, whereas others report no effect7,8,9. A direct measurement of the increase of blasts in S-phase after cytokine administration confirms this heterogeneity10. More detailed studies suggest that the impact of priming may depend on the patient subgroups defined e.g., by risk scores11,12,13,14.
Cytokine administration has become a widely used supportive strategy to prevent chemotherapy-related neutropenia6. In this context the question arises whether cytokines could potentially stimulate leukemic cells that survived therapy and trigger relapse. Although studies in AML patients suggest that leukemic cells can be recruited into cell cycle in response to administered cytokines6,10,15, multiple clinical trials imply that supportive cytokine treatment has no negative effects on relapse free survival6. Nevertheless, there exist trials and case reports stating that in some patients administration of cytokines or their analogues increases leukemic cell load or reduces relapse free survival16,17,18. Different genetic hits accounting for that have been identified so far17,19,20. On the other hand, there exist reports of patients achieving complete remission solely by cytokine administration without chemotherapy21,22,23,24. Both phenomena, negative and positive impact of cytokines on leukemic cell load, are so far not well understood.
The aim of this work is to study if cytokine dependence of leukemic cells has an impact on the clinical course of the disease. For this purpose, we compare disease dynamics in case of cytokine-dependent (i.e. leukemic cells require endogenous cytokines to expand) and cytokine-independent (i.e. leukemic cells can expand in absence of endogenous cytokines) AMLs using mathematical models. We focus on the following questions: (i) How does time evolution of blasts differ in mathematical models of cytokine-dependent and cytokine-independent AML? (ii) Does it have a prognostic impact if patient data fits to the model of cytokine-dependent or to the model of cytokine-independent AML? (iii) Which cell parameters determine whether cytokine administration may have negative, neutral or positive effects on the leukemic cell load?
To approach these questions, we develop new mathematical models of cytokine-dependent and cytokine-independent AML and apply them to patient data showing time changes of bone marrow blast counts between first remission and relapse. Comparing the two models we identify key dynamic features that may help to distinguish between both scenarios. Model-based patient data analysis suggests that the overall survival may depend on the type of regulatory feedback governing cancer stem cell behavior and that it could be significantly worse in case of cytokine-independent AML. Mathematical models provide potential explanations for unexpected responses of patients to cytokines described in literature16,17,18,21,22,23,24.
Mathematical models are a useful tool to understand processes that cannot be manipulated or measured experimentally. They allow rigorous comparison of different hypothetical scenarios and estimation of unknown parameters25,26. Studies from literature demonstrate that mathematical modeling is a suitable approach to investigate the dynamics of cancer cells subjected to regulatory feedbacks or treatment interventions25,26,27,28,29,30. Especially in case of ambiguous experimental results or in systems where the observables strongly depend on experimental conditions, a model-based interpretation of patient data can provide additional insights.
Methods and Model Description
Mathematical models
The interaction of healthy and leukemic cells by cytokine feedbacks and consumption of environmental resources, such as niche spaces, makes it necessary to model both healthy and leukemic cells. To study the potential impact of these interactions on the clinical course of the disease our models incorporate two different modes of feedback, namely cytokine-dependent leukemic cells and cytokine-independent leukemic cells. Cytokine-dependent leukemic cells expand only in presence of cytokines, whereas cytokine-independent (autonomous) leukemic cells have the ability to expand without cytokine stimulation. In this work we develop a new mathematical model for cytokine-independent leukemic cells and compare it to a model of cytokine-dependent leukemic cells proposed by Stiehl et al.31 and applied to data from AML patients25. Both models are an extension of a model of hematopoiesis32, which has been validated on the basis of patient data and applied to clinical questions25,33,34,35.
In the following we introduce the biological system underlying our models. In a multi-step process, the hematopoietic stem cell (HSC) population gives rise to all types of mature blood cells36. Since acute myeloid leukemia (AML) is a disease of the myeloid lineage, our models focus on the granulopoietic branch of the hematopoietic system. A complex network of cytokine signals adjusts cell production to the need of the organism36. Time evolution of the non-linear cytokine feedback in the models are inspired by G-CSF, the main cytokine of granulopoiesis36, and were proposed by Marciniak-Czochra et al.32. It has been reported that cytokine concentration influences properties of stem cells37 and more mature cells36, we therefore assume in the model that feedback signals act on all mitotic cell compartments.
In case of AML the leukemic cell population shows a similar hierarchical organization as the hematopoietic system with the leukemic stem cell (leukemia stem cell, LSC, leukemia initiating cell, LIC) population at the top of the hierarchy38,39. To investigate the potential impact of leukemic cell cytokine dependence on disease dynamics we consider two models, which are summarized in Fig. 1 and Table 1.

Models of cytokine-dependent and cytokine-independent AML. (A) Model 1: Hematopoietic and leukemic cells depend on the same cytokine. (B) Model 2: The leukemic cells are independent of cytokines. Crowding in marrow space results in increased apoptosis. The fraction of self-renewal assigned to non-stem cells is a measure of the average number of cell divisions performed before a cell becomes post-mitotic under homeostatic conditions33.
In Model 1 (cytokine-dependent AML), it is assumed that leukemic cells depend on the same endogenous cytokines as healthy hematopoietic cells. This assumption is justified by the following biological findings: (1) Leukemic cells express the same cytokine receptors as hematopoietic cells40. (2) Leukemic cells of some patients expand only in the presence of cytokines and engraft only in mice transgenic for human cytokines1,2,4,5. (3) Cytokine administration in some AML patients recruits leukemic cells into S-phase10,15. Since hematopoietic and leukemic cells absorb and degrade cytokine molecules by receptor-mediated endocytosis, the two cell lineages interact through competition for the cytokine36,40.
Model 2 (cytokine-independent AML) is based on the evidence that in some patients malignant cells are autonomous with respect to physiological hematopoietic growth factors4,5,41,42. The cytokine-independent leukemic cell growth is then limited by a competition for the bone marrow space that results in an increased cellular degradation due to overcrowded bone marrow space. It is modeled by a feedback loop in death rates depending on the total immature cell population. A model assuming increased cell differentiation in case of marrow overcrowding leads to similar results. These assumptions are justified by the following evidence: (1) Different mechanisms of cytokine-independent leukemic cell expansion have been identified. One mechanism is autocrine sinalling where leukemic cells express the hematopoietic cytokines required for their survival. The cytokine expression profile of leukemic cells shows high inter-individual variability43,44 and includes multiple growth factors such as GM-CSF45,46, G-CSF43, M-CSF47, and IL-148. Secretion of these factors together with expression of the corresponding receptors leads to activation of the leukemic cells43,47. Another mechanism of factor-independent growth is constitutive activation of key signaling components due to mutations such as JAK/STAT or MAP-Kinase41,42. (2) Markers for cell death such as LDH, are increased in bloodstream of leukemic patients49,50 and enhanced cell death is observed in marrow samples of many patients51. The increased cell death is included in Model 2. Several mechanisms for spatial competition have been described such as (i) physical stress owing to overcrowding leading to extinction of cells52, (ii) competition for a limited niche surface expressing certain receptors (contact molecules) necessary for survival of healthy and leukemic cells and apoptosis or differentiation occurring, if no contacts to these molecules can be established53.
The latter niche competition mechanism is also valid for the cytokine-dependent AML in case of overcrowded bone marrow. Therefore, we include it also in the Model 1. As shown by numerical simulations this mechanism is relevant in Model 1 only under external cytokine stimulation. In absence of external cytokine stimulation, the feedback mechanism prevents significant overcrowding of the bone marrow space in cytokine-dependent AMLs.
Both considered models include one leukemic cell lineage and one healthy cell lineage. Dynamics of the different healthy and leukemic cell types are given by ordinary differential equations. We assume that each lineage can be described by 2 compartments: dividing cells (including stem cells and progenitors) and post-mitotic cells. The resulting four-compartment model architecture is based on a simplified description of the multi-stages differentiation process, which reduces the complexity of the differentiation process to focus on mechanisms and effects of competition between different cell lines. The previous studies showed that reduction of the number of compartments do not change the behavior of the model after the modification of the parameters corresponding to the new interpretation of the compartments25.
Each cell type is characterized by the following cell parameters, which are summarized in Fig. 2:
-
Proliferation rate, describing the number of cell divisions per unit of time.
-
Fraction of self-renewal, describing the fraction of progeny cells returning to the compartment occupied by the parent cells that gave rise to them. On the basis of our earlier work and on compatibility with clinical data25,26,32,33,34,35, we assume that the fraction of self-renewal is regulated by feedback signaling. The fraction of self-renewal assigned to non-stem cells is a measure of the average number of cell divisions performed before a cell differentiates under homeostatic conditions33.
-
Death rate, describing the fraction of cells dying per unit of time. For simplicity, we assume that under physiological conditions dividing cells do not die and non-dividing cells die at constant rates.

Important model parameters. (A) The proliferation rate describes the average number of divisions performed by a cell of given type per unit of time. (B) The fraction of self-renewal describes the probability that a progeny cell originating from division adopts the fate of its parent cell, e.g., that a daughter cell of a stem cell is again a stem cell. (C) The effective growth rate describes how many cells enter a given cell fate per unit of time, e.g., the number of stem cells that are generated per unit of time. The effective growth rate depends on the proliferation rate and the fraction of self-renewal.
The effects of cytokines on hematopoietic and leukemic cells are complex. In our models, we assume that cytokines regulate the ratio of self-renewing versus differentiating cells. We neglect the impact of cytokines on the proliferation rates. Our previous quantitative modeling works, see references25,32,33,35, have shown that additional regulation of proliferation rates has little impact on model dynamics. A system with a regulation of proliferation rates but constant self-renewal /differentiation is insufficient to explain hematopoietic reconstitution32,33,35. The simulations depicted in Supplemental Fig. 1 show that additional regulation of proliferation rates has little impact on the blast dynamics. The obtained models are in good qualitative and quantitative agreement with clinical dynamics during hematopoietic stress32,33,35 and in leukemias25.
For analysis of the model dynamics, we define also the effective growth rate of a mitotic cell population. It describes how many mitotic cells are generated per unit of time, see Fig. 2. This quantity depends on the proliferation rate and the fraction of self-renewal of the immature cell population. A high proliferation rate and a low fraction of self-renewal, as long as it is larger than one half, can lead to the same effective growth rate as a combination of high self-renewal and slow proliferation. The supplementary information contains model details (Section 1) together with analytical studies (Section 2) and model parametrization (Section 3).
Simulations
Simulations have been performed using standard ODE-solvers in MATLAB (Version 7.8, The MathWorks, Inc.). We start simulations with equilibrium cell counts in the hematopoietic lineage and a small number of LSC (1 per kg of body weight), mimicking the appearance of LSC due to a mutation or survival of LSC after therapy. Parameters describing the healthy cells (fraction of self-renewal, proliferation rate, death rate) are taken from the previous work34 (based on model fitting to data of hematopoietic reconstitution) and are assumed to be the same for all patients. Leukemic cell properties (fraction of self-renewal, proliferation rate, death rate of post-mitotic cells) and parameters describing interaction of leukemic and healthy cells (death rates due to overcrowding, interaction of the leukemic cells with the feedback signals) are considered to be patient specific. We use the least square method to fit the model to the patient data. The purpose of the parameter fitting is to determine which of the two models are able to capture the individual dynamics of a given patient. During the fitting procedure we restrict patient-specific parameters to biologically plausible ranges: (i) The leukemic cell proliferation rates can vary between one division per two years and one division per day. The latter is considered the upper bound taking into account the DNA replication time of a eukaryotic cell54. (ii) Leukemic cell self-renewal may vary between zero and one. (iii) Blast half-life is chosen between 25% and 100% of leukocyte half-life, motivated by literature55. More details are provided in Section 3.2 of the Supplement.
To decide which of the models fits to the data of a given patient better, we find the best fit for each of the two models and calculate the RMSE (root mean square deviation) for each model. If RMSE for Model 1 is 5% larger than that for Model 2, we conclude that Model 2 fits the data better than Model 1 and vice versa. The results are robust with respect to these choices.
Application to patient data
We use bone marrow aspiration data from patients participating in clinical trials at the University Hospital of Heidelberg (Department of Medicine V; Heidelberg, Germany). Written consent for usage of clinical data for scientific purposes was obtained from each patient. We consider the data of 41 randomly chosen patients. Patients meet the following criteria: (i) at least one documented relapse of the disease in the bone marrow, (ii) achievement of complete hematological remission after treatment of primary diagnosis, (iii) successful bone marrow examination at relapse, and (iv) documented date of death or patients were still alive at the day of data collection. Criterion (iv) limited the number of considered patients.
Statistical analysis
Survival distributions of different patient groups are compared using standard Kaplan-Meier survival analysis56. In all considered cases, the test yields significant results (p < 0.05).
Data availability
All data analyzed in this study are included in this article, its supplementary information and in the cited references.
Results
Cytokine-dependence of leukemic cells has an impact on blast expansion rates
To study how the dependence of leukemic cells on endogenous cytokines can impact on the clinical course of AML, we introduce two different mathematical models. In one model leukemic cells need endogenous cytokines to expand (cytokine-dependent AML) whereas in the other model leukemic cells can expand independently of endogenous cytokines (cytokine-independent AML). The models are summarized in Fig. 1 and in Table 1. They are extensions of previous works and have been parameterized based on patient data25,31,32,33,34,35. For details see section “Methods and Model Description” and Sections 1 and 3 of the Supplement.
We perform numerical simulations to compare blast expansion rates in the models of cytokine-dependent and cytokine-independent (autonomous) leukemic cells. To simulate the fastest possible expansion of leukemic cells, we set their proliferation rate to one division per day, which is an upper bound54. We then measure the time span from origin of one LSC per kg of body weight to a marrow blast fraction of 10% for different LSC self-renewal fractions, see Fig. 3. The simulations show that, for a given leukemic cell self-renewal, leukemic cell expansion is faster for the model of cytokine-independent leukemic cells compared to the model of cytokine-dependent leukemic cells: Whereas for cytokine-dependent leukemic cells a minimum of 200 days is needed to obtain a marrow blast fraction of 10%, 30 days are sufficient in case of cytokine-independent leukemic cell expansion. This observation can serve as a discriminator between both models and suggests that fast relapses can be explained only by autonomous leukemic cell growth or treatment failure. The latter can be excluded based on bone marrow biopsy or aspiration.

Leukemic cell dynamics in Model 1 and Model 2. At t = 0 one leukemic cell per kg of body weight is added to the healthy equilibrium. The number of days elapsing until a marrow blast fraction of 10% is depicted depending on leukemic cell self-renewal. The simulations imply that leukemic cell expansion is faster in Model 2 (dashed line) compared to Model 1 (solid line).
Cytokine-dependence of leukemic cells contributes to inter-individual heterogeneity of clinical courses
To check whether the observed clinical courses are covered by our models, we fit both models to patient blast counts between complete remission (CR) and relapse, see Fig. 4. Time evolution of blast counts of 22 of the considered 41 patients are compatible with both models (Fig. 4A). Evolution of blast counts of 17 patients are compatible only with the model of cytokine-independent AML (Fig. 4B) and blast counts of 2 patients are compatible only with the model of cytokine-dependent AML (Fig. 4C). The fitting results demonstrate that our models capture clinical data and that cytokine dependence of leukemic cells can contribute to the observed clinical heterogeneity of acute myeloid leukemias.

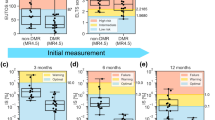
Fit of models to patient data. Models are fitted to marrow blast fractions of AML patients between remission and relapse (solid line: Model 1; dashed line: Model 2). Bone marrow blast fractions are marked by “x” if exact values were reported, if intervals, such as “less than 5% blasts” have been reported, the data is shown as a bar. Panels: Examples for patient data compatible with Models 1 and 2 (A), Model 2 but not Model 1 (B), or Model 1 but not Model 2 (C).
Prognostic significance of autonomous leukemic cell growth
We ask whether cytokine-dependence of leukemic cells can have impacts on patient prognosis. For this purpose, we compared overall survival of patients compatible only with the model of cytokine-independent AML (group 2, n = 17) to patients compatible with the model of cytokine-dependent AML (group 1, n = 24). Survival analysis yields a significantly longer overall survival for group 1 (p = 7 × 10−3, Fig. 5, median overall survival 700 days) compared to group 2 (median overall survival 350 days). The survival after the first relapse is also significantly increased for group 1 (p = 0.03). These results are in line with reports from literature stating that autonomous leukemic cell growth has a negative impact on patient prognosis4,5 and also with the finding that in some trials patient subgroups with unfavorable risk do not respond to cytokine priming before chemotherapy11,12.

Patient data compatible only with model of cytokine independent AML correlates with poor overall survival. Overall survival of two patient groups is compared. Group 1: Patients compatible with model of cytokine dependent AML, group 2: Patients compatible with model of cytokine independent AML and incompatible with model of cytokine dependent AML. Survival of both groups differs significantly (p = 7 × 10−3). Similar results are obtained if survival after first relapse is compared (p = 0.03).
Potential effects of supportive cytokine administration
Depending on the underlying leukemic cell properties and feedbacks, external cytokine administration may have divergent effects. In some patients, external cytokines stimulate blast expansion at the expense of healthy cells16, whereas in other patients leukemic cells are out-competed by stimulated healthy cells which results in a reduction of blast counts21. To understand which cell parameters are crucial for the observed dynamics we run model simulations for multiple parameter combinations. Representative results are depicted in Fig. 6. All parameters used for the simulations shown in Fig. 6 are within the parameter distributions obtained from fitting of patient data. The results can be classified using the effective growth rate of mitotic healthy and leukemic cells. It describes how many mitotic cells of the respective type are produced per unit of time (Fig. 2). In the model of cytokine-dependent AML, cytokine administration is beneficial if the effective growth rate of stimulated leukemic cells is smaller than the corresponding rate for the stimulated healthy cells (Fig. 6A) and harmful otherwise (Fig. 6B). Note that in the model of cytokine-dependent AML a higher self-renewal of leukemic cells compared to hematopoietic cells is sufficient for leukemic cell expansion, independent of the relation between the corresponding effective growth rates. If the effective growth rates of healthy and leukemic cells are similar, cytokine administration has no relevant effect. The simulation depicted in Fig. 6A is in line with the observation that in some patients one cycle of cytokine administration can result in complete remissions that are stable for time intervals between several months and more than one year21,22,24. The simulation depicted in Fig. 6B is in line with the observation that cytokine stimulation can result in blast crisis11. A fit of our models to the data from Duval et al.11 is depicted in Fig. 7.

Effect of cytokine stimulation on leukemic cell burden. When mature cell counts are reduced by 50% due to leukemic cell load we simulate cytokine stimulation for 30 days. Dotted lines show dynamics in absence of cytokine stimulation, solid lines show dynamics during and after cytokine stimulation. (A) Cytokine dependent AML, the self-renewal of leukemic cells is higher than the self-renewal of hematopoietic cells and the effective growth rate of leukemic cells is smaller than the effective growth rate of hematopoietic cells. Cytokine administration reduces the leukemic cell burden. (B) Cytokine dependent AML, the self-renewal of leukemic cells is higher than the self-renewal of hematopoietic cells and the effective growth rate of leukemic cells is higher than the effective growth rate of hematopoietic cells. Cytokine administration increases the leukemic cell burden. (C) Cytokine independent AML, the effective growth rate of leukemic cells is larger than the effective growth rate of hematopoietic cells, leukemic cell self-renewal can be larger or smaller than hematopoietic cell self-renewal. Cytokines cannot reduce the leukemic cell burden. (D) Cytokine independent AML, the effective growth rate of leukemic cells is smaller than the effective growth rate of hematopoietic cells, leukemic cell self-renewal can be larger or smaller than hematopoietic cell self-renewal. In this case leukemic cell counts can be reduced by cytokine administration. Simulation details are provided in the Supplement (Section 3.5). All parameters are listed in Supplemental Table 2.

Blast crisis after pegfilgrastim. Blast crisis after pegfilgrastim administration can only be explained by cytokine sensitive leukemic cells. The figure shows the best fits of the models of cytokine-dependent (A) and cytokine independent (B) AML to the data from Duval16.
Also in the model of cytokine-independent AML the effect of cytokine administration depends on the effective growth rate of mitotic leukemic and hematopoietic cells. If the effective growth rate of leukemic cells is larger than that of stimulated hematopoietic cells, cytokine administration cannot reduce leukemic cell load, it only leads to a negligible reduction of the speed of leukemic cell expansion (Fig. 6C). In the opposite scenario cytokine administration can temporarily reduce the leukemic cell burden but remission, if achieved at all, lasts shorter than in the case of cytokine-dependent AML. The scenario depicted in Fig. 6D fits to the clinical observations reported by Xavier et al.23. Repeated cytokine administration can be used in this case to control the leukemic cell burden23.
The mechanism behind the observed dynamics is as follows: In Fig. 6A healthy and leukemic cells depend on cytokines and thus effective growth rates increase under cytokine stimulation. However, for the chosen parameters, the effective growth rate of stimulated healthy cells is larger than that of stimulated leukemic cells. Since overcrowding of the bone marrow space leads to increased healthy and leukemic cell clearance, the cell population with a higher effective growth rate (healthy cells) out-competes the population with a smaller effective growth rate (leukemic cells). The scenario in Fig. 6B is similar, with the only difference that leukemic cells have a higher effective growth rate compared to healthy cells. In Fig. 6C,D only healthy but not leukemic cells respond to cytokines. Cytokine administration, therefore, results in an increased effective growth rate of healthy cells only. If the stimulated healthy cells have a higher effective growth rate than the leukemic cells, the competition will lead to a reduced leukemic cell count and to an increased healthy cell count, as shown in Fig. 6D. If the stimulated healthy cells have a smaller growth rate than the leukemic cells, cytokine stimulation cannot reduce the leukemic cell load, as shown in Fig. 6C.
Discussion
In this work we propose mathematical models to investigate a possible impact of cytokine-dependence of leukemic cells on the course of the disease. We focus on two scenarios. In Scenario 1 (cytokine-dependent AML) leukemic and healthy cells compete for endogenous cytokines, which they require for expansion. In Scenario 2 (cytokine-independent AML) leukemic cells expand independently of cytokines but cells compete for the bone marrow space and die in case of overcrowding. Both scenarios are supported by experimental evidence3,4,5,41,42.
Unlike many previous models, the models considered in this work explicitly include dynamics of healthy cells. Animal experiments show that hematopoietic stem cells isolated from leukemic organisms can lead to normal hematopoiesis if transplanted to a non-leukemic host57. This finding suggests that a better understanding of the disease mechanisms could allow to derive clinical strategies that support healthy hematopoiesis and reduce expansion of leukemic cells.
The proposed mathematical models provide criteria that might allow discrimination between cytokine-dependent and cytokine-independent AMLs. Our results suggest that rapid leukemic cell expansion and early relapses may be typical for cytokine-independent AML. The models suggest that if time between complete remission and 10% marrow blasts at relapse is shorter than 200 days, only the model of cytokine-independent AML is able to explain the dynamics.
Fitting of the developed models to patient blast counts between complete remission and relapse demonstrates that patients compatible only with the model of cytokine-independent AML have a significantly poorer overall survival compared to patients compatible with the model of cytokine-dependent AML. This observation is in line with data from cell culture studies showing that autonomous cell growth is correlated with a poor prognosis4,5.
Another important difference between the models lies in the reaction of the patient to external cytokine administration. Cytokine administration is a commonly used treatment strategy to increase healthy cell counts and to reduce complications of chemotherapy6. Although considered safe in general, there exist multiple reports of patients showing unexpected increase or reduction of the leukemic cell burden after cytokine administration. Increasing leukemic cell counts can be explained by cytokine-mediated blast expansion16, whereas decreasing leukemic cell counts result from stimulation of hematopoiesis and out-competition of leukemic clones21. Our modeling approach suggests the effective growth rate of leukemic and hematopoietic mitotic/stem cells as a crucial parameter to understand divergent reaction of patients to cytokine administration. The effective growth rate of a cell population describes how many cells of that population are produced per unit of time. It can potentially be estimated based on mathematical models. In our model simulations cytokine stimulation can induce complete remissions even in cytokine-dependent AML provided the effective growth rate of mitotic leukemic cells is smaller than that of mitotic hematopoietic cells (note that an effective growth rate of leukemic cells larger than zero is necessary and sufficient for their expansion). This scenario is in line with multiple clinical observations21,22,24. If the effective growth rate of leukemic cells is higher compared to hematopoietic cells, cytokine administration can result in blast expansion as it has been clinically observed16.
Similarly, leukemic cell load can be temporarily reduced in the model of cytokine-independent AML if the effective growth rate of hematopoietic cells is larger than that of leukemic cells. Nevertheless, this reduction is less efficient compared to the case of cytokine-dependent AML, since remaining leukemic cells expand fast. Model dynamics in this case also fit to clinical reports23. The observation that a given treatment can be beneficial in some patients and harmful in others demonstrates the need to distinguish between the regulation modes present in different patients. The criteria developed in this work can be helpful for this task.
The models considered in this manuscript describe two opposite extremes of a continuum, namely cytokine-dependence and cytokine-independence. However, more complex dynamics may emerge in more complex scenarios, e.g., in scenarios where leukemic cells are not fully independent of cytokines but they need less stimulation than their benign counterparts or leukemic cells are less sensitive to cytokine stimulation than healthy cells. These scenarios can be included in future versions of the presented modeling framework.
From an experimental point of view, it is challenging to decide if leukemic cells depend on cytokines or not. One possibility is to study if leukemic cells show autonomous growth in cell cultures. However, the readout can depend on the culture conditions3. Another possibility is assessment of cell surface receptors, however experimental data suggest that presence of growth factor receptors not automatically implies response of cells to these factors58. Further complications arise from evidence suggesting that hematopoietic growth factors can interact with their receptors inside the cell, which would imply that autocrine loops not necessarily depend on surface receptor expression59.
As previously shown our models can be generalized to a multi-clonal setting, see refs34,60. A multi-clonal version of the model of cytokine-dependent leukemia with stochastic mutation acquisition can be found in reference60. These extensions allow to study the impact of leukemic cell parameters on clonal evolution in absence and presence of therapy34,60. If the frequencies of different leukemic clones at multiple time-points are available for individual patients, the analysis presented in this work can be applied to compare cell properties of different clones. However, such data is not available in clinical routine so far.
Our mathematical modeling approach allows to assign patients to different risk groups based on time evolution of their individual blast counts. This strategy is complementary to the clinically used risk stratifications which rely mostly on genetic hits. In the future this approach could be used to identify patients with adverse and beneficial response to exogenous cytokines and to improve risk stratification approaches.
Our results support the hypothesis that cytokine-dependence of leukemic cells impacts on the course of the disease. Fitting the models to data of individual patients suggests differences in the response of AML cells to cytokines. The models propose a distinction between patients with cytokine-dependent and cytokine-independent AML cell dynamics which leads to significant differences in patients’ prognosis. The modeling insights suggest that this topic may be of clinical relevance and merits further investigation.
References
Feuring-Buske, M. et al. Improved engraftment of human acute myeloid leukemia progenitor cells in beta 2-microglobulin-defficient NOD/SCID mice and in NOD/SCID mice transgenic for human growth factors. Leukemia. 17, 760–763 (2003).
Theocharides, A., Rongvaux, A., Fritsch, K., Flavell, R. & Manz, M. Humanized hemato-lymphoid system mice. Haematologica. 101, 5–19 (2016).
Van der Lely, N. et al. In vitro response of blasts to IL-3, GM-CSF, and G-CSF is different for individual AML patients: factors that stimulate leukemic clonogenic cells also enhance ARA-C cytotoxicity. Ann. Hematol. 68, 225–232 (1994).
Hunter, A., Rogers, S., Roberts, I., Barrett, A. & Russell, N. Autonomous growth of blast cells is associated with reduced survival in acute myeloblastic leukemia. Blood. 82, 899–903 (1993).
Löwenberg, B., van Putten, W. L., Touw, I. P., Delwel, R. & Santini, V. Autonomous proliferation of leukemic cells in vitro as a determinant of prognosis in adult acute myeloid leukemia. N Engl J Med. 328, 614–619 (1993).
Ravandi, F. Role of cytokines in the treatment of acute leukemias: a review. Leukemia. 20, 563–571 (2006).
Löwenberg, B. et al. Use of recombinant GM-CSF during and after remission induction chemotherapy in patients aged 61 years and older with acute myeloid leukemia: final report of AML-11, a phase III randomized study of the Leukemia Cooperative Group of European Organisation for the Research and Treatment of Cancer and the Dutch Belgian Hemato-Oncology Cooperative Group. Blood. 90, 2952–2961 (1997).
Löwenberg, B. et al. Value of different modalities of granulocyte-macrophage colony-stimulating factor applied during or after induction therapy of acute myeloid leukemia. J Clin Oncol. 15, 3496–3506 (1997).
Heil, G. et al. GM-CSF in a double-blind randomized, placebo controlled trial in therapy of adult patients with de novo acute myeloid leukemia (AML). Leukemia. 9, 3–9 (1995).
Schiller, G., Emmanoulides, C., Iastrebner, M. C., Lee, M. & Naeim, F. High-dose cytarabine and recombinant human granulocyte colony-stimulating factor for the treatment of resistant acute myelogenous leukemia. Leuk Lymphoma. 20, 427–434 (1996).
Löwenberg, B. et al. Effect of priming with granulocyte colony-stimulating factor on the outcome of chemotherapy for acute myeloid leukemia. N Engl J Med. 349, 743–52 (2003).
Bug, G. et al. Long-term results of a prospective randomized trial evaluating G-CSF priming in intensive induction chemotherapy followed by autologous stem cell transplantation in elderly patients with acute myeloid leukemia. Ann Hematol. 93, 193–202 (2014).
Thomas, X. et al. Which AML subsets benefit from leukemic cell priming during chemotherapy? Long-term analysis of the ALFA-9802 GM-CSF study. Cancer. 116, 1725–1732 (2010).
Thomas, X. et al. Effect of priming with granulocyte-macrophage colony-stimulating factor in younger adults with newly diagnosed acute myeloid leukemia: a trial by the Acute Leukemia French Association (ALFA) Group. Leukemia. 21, 453–461 (2007).
Baer, M. et al. Biological effects of recombinant human granulocyte colony-stimulating factor in patients with untreated acute myeloid leukemia. Blood. 87, 1484–1494 (1996).
Duval, C. et al. Fatal stimulation of acute myeloid leukemia blasts by pegfilgrastim. Anticancer Res. 34, 6747–6748 (2014).
Ehlers, S. et al. Granulocyte colonystimulating factor (G-CSF) treatment of childhood acute myeloid leukemias that overexpress the differentiation-defective G-CSF receptor isoform iv is associated with a higher incidence of relapse. J. Clin. Oncol. 28, 2591–2597 (2010).
Zittoun, R. et al. Granulocyte-macrophage colony stimulating factor associated with induction treatment of acute myelogenous leukemia: a randomized trial by the european organization for research and treatment of cancer leukemia cooperative group. J. Clin. Oncol. 14, 2150–2159 (1996).
Pebusque, M., Lafage, M., Lopez, M. & Mannoni, P. Preferential response of acute myeloid leukemias with translocation involving chromosome 17 to human recombinant granulocyte colony-stimulating factor. Blood. 72, 257–265 (1988).
Sloand, E. et al. Granulocyte colony-stimulating factor preferentially stimulates proliferation of monosomy 7 cells bearing the isoform iv receptor. PNAS. 103, 14483–14488 (2006).
Vadhan-Raj, S. et al. Stimulation of nonclonal hematopoiesis and suppression of the neoplastic clone after treatment with recombinant human granulocyte-macrophage colony-stimulating factor in a patient with therapy-related myelodysplastic syndrome. Blood. 74, 1491–1498 (1989).
Takahashi, M. et al. Complete remission in three patients with acute myeloblastic leukemia by administration of G-CSF without antileukemic agents. Am. J. Hematol. 56, 42–44 (1997).
Xavier, L. et al. Hematological remission and long term hematological control of acute myeloblastic leukemia induced and maintained by granulocyte-colony stimulating factor (G-CSF) therapy. Leuk. Lymphoma. 44, 2137–2142 (2003).
Bassan, R., Rambaldi, A., Amaru, R., Motta, T. & Barbui, T. Unexpected remission of acute myeloid leukaemia after GM-CSF. Br. J. Haematol. 87, 835–838 (1994).
Stiehl, T., Baran, N., Ho, A. D. & Marciniak-Czochra, A. Cell division patterns in acute myeloid leukemia stem-like cells determine clinical course: a model to predict patient survival. Cancer Res. 75, 940–949 (2015).
Stiehl, T. & Marciniak-Czochra, A. Stem cell self-renewal in regeneration and cancer: Insights from mathematical modeling. Curr Opin Systems Biology. 5, 112–120 (2017).
Komarova, N. Principles of regulation of self-renewing cell lineages. PLoS One. 8, e72847 (2013).
Komarova, N. & Wodarz, D. Evolutionary dynamics of mutator phenotypes in cancer: implications for chemotherapy. Cancer Res. 63, 6635–6642 (2003).
Wodarz, D. et al. Kinetics of cll cells in tissues and blood during therapy with the btk inhibitor ibrutinib. Blood. 123, 4132–4135 (2014).
Yang, J., Axelrod, D. & Komarova, N. Determining the control networks regulating stem cell lineages in colonic crypts. J. Theor. Biol. 429, 190–203 (2017).
Stiehl, T. & Marciniak-Czochra, A. Mathematical modelling of leukemogenesis and cancer stem cell dynamics. Math. Model. Natural Phenomena. 7, 166–202 (2012).
Marciniak-Czochra, A., Stiehl, T., Jäger, W., Ho, A. D. & Wagner, W. Modeling of asymmetric cell division in hematopoietic stem cells - regulation of self-renewal is essential for efficient repopulation. Stem Cells Dev. 18, 377–385 (2009).
Stiehl, T., Ho, A. D. & Marciniak-Czochra, A. The impact of CD34+ cell dose on engraftment after SCTs: personalized estimates based on mathematical modeling. Bone Marrow Transplant. 49, 30–37 (2014).
Stiehl, T., Baran, N., Ho, A. D. & Marciniak-Czochra, A. Clonal selection and therapy resistance in acute leukaemias: mathematical modelling explains different proliferation patterns at diagnosis and relapse. J. R. Soc. Interface. 11, 20140079 (2014).
Stiehl, T., Ho, A. D. & Marciniak-Czochra, A. Assessing hematopoietic (stem-) cell behavior during regenerative pressure. Adv Exp Med Biol. 844, 347–367 (2014).
Metcalf, D. Hematopoietic cytokines. Blood. 111, 485–491 (2008).
Manko, J. et al. A clinical comparison of the efficacy and safety of biosimilar G-CSF and originator G-CSF in haematopoietic stem cell mobilization. Pharmacol. Rep. 66, 239–242 (2014).
Bonnet, D. & Dick, J. Human acute myeloid leukemia is organized as a hierarchy that originates from a primitive hematopoietic cell. Nat. Med. 3, 730–737 (1997).
Hope, K., Jin, L. & Dick, J. Acute myeloid leukemia originates from a hierarchy of leukemic stem cell classes that differ in self-renewal capacity. Nat. Immunology 5, 738–743 (2004).
Shinjo, K., Takeshita, A., Ohnishi, K. & Ohno, R. Granulocyte colony stimulating factor receptor at various stages of normal and leukemic hematopoietic cells. Leuk. Lymphoma. 25, 37–46 (1997).
Hayakawa, F. et al. Tandem-duplicated Flt3 constitutively activates STAT5 and MAP kinase and introduces autonomous cell growth in IL-3-dependent cell lines. Oncogene. 19, 624–631 (2000).
Liu, R., Fan, C., Garcia, R., Jove, R. & Zuckerman, K. Constitutive activation of the JAK2/STAT5 signal transduction pathway correlates with growth factor independence of megakaryocytic leukemic cell lines. Blood. 93, 2369–2379 (1999).
Murohashi, I. et al. Autocrine growth mechanisms of the progenitors of blast cells in acute myeloblastic leukemia. Blood. 74, 35–41 (1989).
Young, D. C., Demetri, G. D., Ernst, T. J., Cannistra, S. A. & Griffin, J. D. In vitro expression of colony-stimulating factor genes by human acute myeloblastic leukemia cells. Exp Hematol. 16, 378–382 (1988).
Young, D. C. & Griffin, J. D. Autocrine secretion of GM-CSF in acute myeloblastic leukemia. Blood. 68, 1178–1181 (1986).
Young, D. C., Wagner, K. & Griffin, J. D. Constitutive expression of the granulocyte-macrophage colony-stimulating factor gene in acute myeloblastic leukemia. J Clin Invest. 79, 100–106 (1987).
Rambaldi, A. et al. Expression of the macrophage colony-stimulating factor and c-fms genes in human acute myeloblastic leukemia cells. J Clin Invest. 81, 1030–1035 (1988).
Nakamura, M., Kanakura, Y., Furukawa, Y., Ernst, T. J. & Griffin, J. D. Demonstration of interleukin-1 beta transcripts in acute myeloblastic leukemic cells by in situ hybridization. Leukemia. 4, 466–470 (1990).
Buechner, T. & Heinecke, A. The role of prognostic factors in acute myeloid leukemia. Leukemia. 10(Suppl. 1), S28–S29 (1996).
Yamauchi, T. et al. A high serum uric acid level is associated with poor prognosis in patients with acute myeloid leukemia. Anticancer Res. 33, 3947–3951 (2013).
Irvine, A., Magill, M., Somerville, L. & McMullin, M. Spontaneous intramedullary apoptosis is present in disorders other than myelodysplasia. Exp. Hematol. 26, 435–439 (1998).
Griffin, J. & Loewenberg, B. Clonogenic cells in acute myeloblastic leukemia. Blood. 68, 1185–1195 (1986).
Zhang, J. et al. Identification of the hematopoietic stem cell niche and control of the niche size. Nature. 425, 836–841 (2003).
Morgan, D. et al. The Cell Cycle In Molecular Biology of the Cell, 5th ed (eds Alberts, B. et al.) 1053–1114 (Garland Science, 2007).
Savitskiy, V., Shman, T. & Potapnev, M. Comparative measurement of spontaneous apoptosis in pediatric acute leukemia by different techniques. Cytometry B Clin. Cytom. 56, 16–22 (2003).
Armitage, P., Berry, G. & Matthews, J. Survival analysis in Statistical methods in medical research, 4th ed (eds Armitage, P., Berry, G. & Matthews, J.) 568–590 (Blackwell Science Ltd, 2002).
Hoang, V. et al. The rarity of ALDH(+) cells is the key to separation of normal versus leukemia stem cells by ALDH activity in AML patients. Int. J. Cancer. 137, 525–536 (2015).
Smith, M. A., Smith, J. G., Pallister, C. J. & Singer, C. R. Kinetic characteristics of de novo and secondary AML cells influence their response to haemopoietic growth factor (HGF) priming and correlate with clinical outcome. Leuk Res. 23, 987–994 (1999).
Dunbar, C. E., Browder, T. M., Abrams, J. S. & Nienhuis, A. W. COOH-terminal-modified interleukin-3 is retained intracellularly and stimulates autocrine growth. Science. 245, 1493–1496 (1989).
Stiehl, T., Lutz, C. & Marciniak-Czochra, A. Emergence of heterogeneity in acute leukemias. Biology Direct. 11, 51 (2016).
Acknowledgements
This work was funded by research funding from the German Research Foundation DFG (Collaborative Research Center SFB 873, Maintenance and Differentiation of Stem Cells in Development and Disease, subproject B08).
Author information
Authors and Affiliations
Contributions
T.S., A.M.C., A.D.H. designed the research, A.D.H. contributed patient data, T.S. performed modeling and simulations, T.S., A.M.C., A.D.H. interpreted the results, T.S. and A.M.C. wrote the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Stiehl, T., Ho, A.D. & Marciniak-Czochra, A. Mathematical modeling of the impact of cytokine response of acute myeloid leukemia cells on patient prognosis. Sci Rep 8, 2809 (2018). https://doi.org/10.1038/s41598-018-21115-4
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-018-21115-4
This article is cited by
-
Understanding Hematopoietic Stem Cell Dynamics—Insights from Mathematical Modelling
Current Stem Cell Reports (2023)
-
AML consolidation therapy: timing matters
Journal of Cancer Research and Clinical Oncology (2023)
-
Local asymptotic stability of a system of integro-differential equations describing clonal evolution of a self-renewing cell population under mutation
Journal of Mathematical Biology (2022)
-
Mathematical models of leukaemia and its treatment: a review
SeMA Journal (2022)
-
Understanding Normal and Pathological Hematopoietic Stem Cell Biology Using Mathematical Modelling
Current Stem Cell Reports (2021)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
