
Abstract
Hereditary hyperferritinaemia-cataract syndrome (HHCS) is a rare disorder usually caused by heterozygous mutations in the iron-responsive element (IRE) in the 5′ untranslated region (5′UTR) of the L-ferritin gene (FTL), disturbing the binding of iron regulatory proteins (IRPs) and the post-transcriptional regulation of ferritin expression. Here, the proband of a consanguineous family displayed moderate bilateral cataracts and elevated serum ferritin in the absence of iron overload. The parents and siblings showed variable degrees of mild bilateral cataracts combined with elevated levels of circulating ferritin. Sequencing of FTL identified a novel 5′UTR mutation c.-151A > G, also named “Ghent +49A > G”. The zygosity of the mutation, occurring in homozygous and heterozygous state in the proband and other affected family members respectively, correlated well with severity of ophthalmological and hematological manifestations. The substitution is expected to impair the secondary structure of the upper IRE stem. Functional characterization of +49A > G by electrophoretic mobility shift assays demonstrated a reduced binding affinity for IRP1 compared to the wild-type IRE of FTL. Overall, we have expanded the repertoire of deleterious biallelic FTL IRE mutations in HHCS with this novel +49A > G mutation, the zygosity of which correlated well with the disease expression.
Similar content being viewed by others


Introduction
Hereditary hyperferritinaemia-cataract syndrome (HHCS) (OMIM 600886) is a rare autosomal dominant disease (estimated prevalence of 1 in 200,000), characterized by the combination of elevated serum ferritin in the absence of iron overload or other hematological abnormalities and progressive cataracts of a highly distinctive morphology1. The genetic disorder was first described in 1995 by two independent groups2,3. HHCS might be misdiagnosed as hereditary hemochromatosis, since serum ferritin levels are still widely used to identify hereditary and acquired iron overload conditions4. As a consequence, patients with HHCS could undergo inadequate follow-up with repeated exams in search of iron overload or even an inappropriate phlebotomy treatment that leads to iron deficiency anemia, stressing the importance of a correct clinical diagnosis of HHCS3.
Patients with HHCS present a disease-causing mutation in the FTL gene, located on chromosome 19 (19q13.1). The FTL gene encodes the light subunit, L-ferritin (19 kDa), that together with the heavy subunit, H-ferritin (21 kDa, encoded by the FTH gene located on chromosome 11q12.3) constitutes the 24-subunit heteropolymer ferritin protein5. Ferritin is an ubiquitously expressed protein responsible for the storage and intracellular distribution of iron. The expression of the ferritin subunits is modulated by intracellular iron levels through a tightly regulated negative feedback system based on the interaction between cytoplasmic iron-sensing mRNA-binding proteins, the iron regulatory proteins (IRP1 and IRP2), and a non-coding cis-acting stem-loop structure located in the 5′ untranslated region (5′UTR) of both L- and H-ferritin mRNA, the iron-responsive elements (IREs)6. These IREs comprise four important structural parts: the hexanucleotide apical loop, the upper and lower stem consisting of palindromic sequences and the cytosine bulge, an unpaired cytosine residue (C-bulge) located in between the upper and lower stem7. In conditions of low intracellular iron levels, the high affinity IRP/IRE binding prevents the recruitment of the small ribosomal subunit to the mRNA. As a consequence, the synthesis of the ferritin subunits is repressed at the translational level which limits the storage and utilization of cytoplasmic iron. Conversely, when intracellular iron levels increase the IRP/IRE binding affinity decreases due to conformational changes of IRP1 and the proteasomal degradation of IRP2, resulting in the initiation of ferritin mRNA translation and the consequent upregulation of ferritin synthesis8,9.
Heterozygous mutations in the IRE of FTL mRNA disturbing cellular iron homeostasis are characteristic of HHCS. FTL IRE mutations reduce the IRP/IRE binding affinity due to changes in the IRE secondary structure and/or the stability of the IRE10, abrogating the IRP/IRE interaction and leading to uncontrolled translation of FTL mRNA, independent of the iron status. The constitutive overproduction of L-ferritin gives rise to L-subunit rich ferritin heteropolymers and ferritin homopolymers of 24 L-subunits, resulting in both hyperferritinaemia and intracellular ferritin accumulation11. Although ferritin accumulates in all cell types of HHCS patients, it turns out to be toxic only in the crystallin-containing lens fiber cells. There, crystalline L-ferritin deposits can be found, which may affect the solubility of other lens proteins or induce oxidative lens damage, altogether leading to the formation of cataracts12.
Here, our aim was to molecularly explain the variable expressivity of hyperferritinaemia and bilateral cataracts in different members of a consanguineous family with HHCS, and to functionally characterize a novel mutation in the 5′UTR of FTL.
Methods
Clinical assessment of patients
A Belgian family of Moroccan descent with parental consanguinity (second cousins) (Fig. 1A) underwent hematological and ophthalmological assessment following a clinical diagnosis of HHCS in the 8-year-old proband (II:2). In particular, slit-lamp biomicroscopy and the measurement of iron parameters were performed. Normal serum ferritin levels are ranging from 12 to 300 µg/L for males and from 12 to 150 µg/L for females13. An extended pedigree, illustrating the consanguineous relationship in this family, can be found in Supplementary Figure 1.

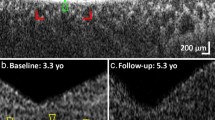
Overview of the HHCS-affected family. (A) Pedigree of the family investigated in this study, with segregation of the Ghent +49A > G mutation. The severity of the phenotype is represented by the darkness of the pedigree symbol. The pedigree shows parental consanguinity between I:1 and I:2. The proband II:2 is indicated by an arrow. (B) Slit-lamp examination of the anterior segment of the proband (II:2) displayed moderate central nuclear bilateral cataracts, in the absence of scattered flecks. The proband’s father (I:1) presented with mild bilateral central nuclear cataracts with typical distinctive peripheral spicules, while the mother (I:2) and siblings (II:1, II:3) demonstrated mild bilateral central nuclear cataracts with less dense opacities. (C) Electropherograms of Sanger sequencing of the IRE located in the 5′UTR of the FTL gene, using genomic DNA of patients. The arrow indicates the nucleotide change +49A > G (c.-151A > G, NM_000146.3). The WT sequence is displayed on top as a reference, the homozygous sequence (II:2) in the middle and the heterozygous sequence (I:1, I:2, II:1, II:3) at the bottom.
FTL analysis
The proband (II:2), the parents (I:1, I:2) and two siblings (II:1, II:3) were referred to the Center for Medical Genetics in the Ghent University Hospital for genetic testing of the FTL 5′UTR. An informed consent was obtained from all subjects or their legal representative. Genomic DNA was extracted from peripheral blood using the QIAamp DNA blood mini kit, according to manufacturer’s instructions (Qiagen). In our standard workflow the coding regions, exon-intron boundaries and UTRs of the FTL gene (NM_000146.3) were PCR amplified starting with 40 ng of genomic DNA using four primer pairs (Supplementary Table 1). Purification of the PCR products by Exonuclease I and Antarctic Phosphatase (New England Biolabs) treatment was followed by bi-directional Sanger sequencing using the BigDye Terminator v3.1 Cycle Sequencing Kit (Applied Biosystems). Sequencing products were purified by CleanDTR magnetic beads (GC Biotech) and analyzed on a ABI PRISM 3730XL Sequencer (Applied Biosystems). Data-analysis and variant calling was performed with the SeqScape Software (Applied Biosystems). Given the clinical diagnosis of HHCS, data analysis was confined to the 5′UTR of FTL. Variants were designated according to the HGVS nomenclature and the classical nomenclature used for HHCS variants. Variant classification was performed following the American College of Medical Genetics (ACMG) guidelines of 201514. The study was conducted in accordance with the tenets of Helsinki and was approved by the Ghent University Hospital Ethics Committee (approval 2004/094).
Confirmation of homozygosity
To exclude false homozygosity of the 5′UTR mutation in the proband due to an FTL deletion in trans with the mutation, three qPCR primer pairs were used, located in the FTL 5′UTR region (Supplementary Table 1). Copy number analysis was performed on the LightCycler 480 real-time PCR instrument (Roche) using the SYBR Green Master Mix (Roche) and 20 ng of genomic DNA of each patient and three positive controls15. Each reaction was run in duplicate. Data analysis was executed using the qBase+ software (Biogazelle) and results were normalized to two reference assays (ZNF80, GPR15).
Genome-wide SNP genotyping and homozygosity mapping
In order to assess the size of the autozygous region and haplotype in which the homozygous FTL 5′UTR mutation is located, genome-wide SNP genotyping was performed using the HumanCytoSNP-12 BeadChip platform (Illumina). Plink software, integrated in ViVar, identified homozygous regions >1 Mb which were ranked according to their length and the number of SNPs, as described16.
FTL RNA fold predictions
RNA folding analysis to predict the IRE structure of wild-type (WT) and mutated FTL was carried out using Mfold (http://unafold.rna.albany.edu/)17 and Sfold web server (http://sfold.wadsworth.org/)18. RNA sequences used for fold predictions are shown in Supplementary Table 2.
Plasmid construction
Plasmids for generating RNA probes for electrophoretic mobility shift assay (EMSA) experiments were constructed based on the I-12.CAT plasmid19 using annealed synthetic complementary oligonucleotides corresponding to the sequence of interest. Constructs were made for the FLT 5′ IRE +49A > G mutation as well as the WT sequence (FTL 5′ IRE WT, negative control) and a mutant version bearing a C deletion in the apical loop (FTL 5′ IRE +39ΔC, positive control), not interacting with IRP120. After ligation using the Quick Ligation kit (New England Biolabs), 2 μL of the ligation product was heat-shock transformed into 50 µL competent TOP10 bacterial cells (Invitrogen) which were plated on LB plates containing 100 μg/mL ampicillin. Colonies were picked and grown in LB broth. Plasmid DNA was isolated using the Nucleospin plasmid mini DNA purification kit (Macherey-Nagel). Sanger sequencing was performed (GATC Biotech, Konstanz) to verify the presence of the correct insert in each construct. All oligonucleotides used for cloning purposes are listed in Supplementary Table 3. Plasmids were linearized and used as template for T7 in vitro transcription (MEGAscript T7 kit, Life Technologies).
EMSA experiments
Two types of EMSA experiments were performed in this study: direct and competitive EMSA. For direct EMSA experiments, fluorescent-labeled probes corresponding to FTL 5′ IRE WT, +39ΔC and +49A > G were incubated with the recombinant IRP1 protein19 in order to qualitatively assess IRP1/IRE binding. For competitive EMSA experiments, the fluorescent-labeled WT probe was incubated with recombinant IRP1 together with increasing amounts of non-labeled competitor FTL 5′ IRE WT, +39ΔC and +49A > G probes. The extent to which the non-labeled probes competed with the labeled WT probe for binding the IRP1 protein, provided a quantitative insight into IRP1/IRE binding affinity.
The T7 in vitro transcription reaction for the labeled probes was performed in 1X transcription buffer, 0.33 mM rATP, rCTP, rGTP, 3.33 μM rUTP, 20 μM ATTO-680 aminoallyl-rUTP (Jena Bioscience), 240 units T7 RNA polymerase (EMBL Heidelberg core facility), 60 units RNasin Ribonuclease Inhibitor (Promega), and 30 mM DTT in a total reaction volume of 45 µL, using 6 µg of template DNA. After incubation for 4 h at 37 °C, template DNA was degraded by TURBO DNase (Ambion) treatment. The non-labeled competitors were in vitro transcribed using the MEGAscript T7 kit (Life Technologies) according to the manufacturer’s instructions. ATTO-680 labeled probes and unlabeled competitors were purified by phenol/chloroform/isoamyl alcohol extraction and used as probes. Prior to protein binding, 100 ng of labeled probe, and increasing molar excess (1X, 2X, 5X, 10X, 20X, 40X, 80X) of unlabeled competitor probes in case of competitive EMSA, were denatured at 95 °C for 5 min, followed by renaturation at room temperature. Probes were then incubated with 200 ng recombinant IRP1 protein19 in CLB buffer (25 mM Tris/HCl pH 7.4, 40 mM KCl, 1% Triton X-100, 1X cOmplete EDTA-free protease inhibitor cocktail) for 15 min at room temperature. In order to displace non-specific RNA-protein interactions, 50 ng of sodium heparin was added to the reaction mix. After incubation for 10 min at room temperature, 2 μL of 80% glycerol loading buffer was added and reaction mixtures were loaded on a 5% native acrylamide (60:1 acrylamide:bisacrylamide) gel in 1X TBE buffer. Gels were run at 80 V at 4 °C and visualized in the 700 nm channel using the Odyssey Infrared Imaging System (LI-COR Biosciences), at an intensity setting of 7.0, with resolution set to 169 µm and focus offset to 1.0 mm. Adjustment of brightness and contrast levels was applied to the entire images using the ImageJ software. After applying the despeckle and background subtraction tool, absolute band intensities corresponding to IRP1/IRE complexes were calculated with the ImageJ software. For direct EMSA experiments, intensities were normalized relative to the intensity of the shifted band of WT IRE. Normalization of intensities of competitive EMSA experiments was done relative to the intensity of the band in lane N. Direct and competitive EMSA experiments were performed in quadruplicate and triplicate respectively.
Statistical analysis
The results from the direct EMSA experiments were compared using one-way analysis of variance (ANOVA) with a post hoc Bonferroni multiple-comparison test. Differences between groups were considered statistically significant for p values less than 0.05. Statistical analyses were performed with GraphPad Prism 5.0.
Calculation of apparent dissociation constants (KDapp)
The calculation of the KDapp values was performed using a previously reported method for competition assays21. The plot of bound labeled WT probe against the concentration of free unlabeled competitor was best fit to the single independent site model:
with f the ratio of observed intensity relative to the intensity in the absence of competitor, KDapp the apparent dissociation constant for the competitor under investigation, and [C]free the concentration of the free competitor:
with [C]i the initial concentration of competitor, [H]i the initial amount of labeled WT probe. The non-linear leastsquares best fit apparent dissociation constant was then calculated from Equation (1).
Results
Clinical findings
The 8-year-old proband (II:2) was referred because of highly elevated serum ferritin (2784 µg/L) without clinical, biological or radiologic evidence of iron overload. His familial history revealed consanguinity (Fig. 1A), a long follow-up for moderate hyperferritinaemia without iron overload in his mother (I:2) with negative genetic testing for HFE-associated hereditary hemochromatosis and early-onset of bilateral cataracts at age 30 in his father (I:1). Slit-lamp examination of the anterior segment of the proband (II:2) unveiled moderate bilateral cataracts (Fig. 1B) compatible with a clinical diagnosis of HHCS. In the proband’s parents (I:1, I:2) and siblings (II:1, II:3) variable degrees of mild bilateral cataracts (Fig. 1B) were observed, with elevated, but significantly lower levels of circulating ferritin compared to the proband (576 µg/L, 586 µg/L, 460 µg/L, and 661 µg/L respectively), with normal levels of serum iron and transferrin saturation. The father (I:1) was also diagnosed with possible Fuchs’ uveitis, a condition often resulting in secondary cataract22. In this case, however, the cataract morphology showed a different aspect than that usually observed in Fuchs’ uveitis. The biological and clinical findings in this family are summarized in Table 1.
Molecular genetic findings
Subsequent analysis of the 5′UTR of the FTL gene encoding the FTL IRE in the HHCS-affected proband revealed a novel homozygous mutation c.-151A > G (NM_000146.3). In agreement with the traditional nomenclature for FTL IRE mutations, the alternative name for this mutation is the “Ghent +49A > G” mutation (relative to the transcription initiation signal). Segregation analysis showed the presence of the Ghent +49A > G mutation in a heterozygous state in the parents as well as in both siblings (Fig. 1C). This variant was not reported in the consulted public databases (1000 Genomes Project, ExAC, dbSNP, HGMD). No other likely pathogenic variants in the FTL gene were observed in neither the proband nor the family members.
To exclude false homozygosity of the Ghent +49A > G mutation in the proband due to a deletion in trans with the mutation, a qPCR analysis was performed using three amplicons neighbouring the mutation. The corresponding results ruled out false homozygosity and confirmed that the Ghent +49A > G mutation in the proband is present on both alleles (Supplementary Figure 2). Following ACMG guidelines, this mutation was classified as a pathogenic mutation (class 5) (Supplementary Table 4).
Given the parental consanguinity, genome-wide SNP genotyping was performed in the proband, the parents and two siblings, in order to have more insight into the size of the autozygous region and corresponding haplotype containing the homozygous 5′UTR mutation. Homozygosity mapping in the proband revealed seven homozygous regions (>1 Mb) unique to the proband, one of which contains the FTL gene. An overview over the regions of homozygosity can be found in Supplementary Table 5.
The Ghent +49A > G mutation is predicted to impair the IRE structure
RNA secondary structure modeling of WT and mutated FTL 5′ IRE sequences was performed using the Mfold and Sfold web server. Both folding software packages predict that the Ghent +49A > G mutation, which is located at the basis of the upper stem, just above the cytosine bulge, is likely to disturb the WT IRE conformation (Fig. 2). The substitution of adenine by guanine at position +49 is expected to affect base pairing with uracil at position +34, inducing a broader rearrangement of base pairing in the upper stem, an altered secondary structure of the apical loop and loss of the cytosine bulge.

Predicted secondary structure of WT and +49A > G mutated FTL 5′UTR IRE RNA, computed using the Sfold web server18. The +49A > G mutation, indicated with an arrow, is expected to influence base pairing in the upper stem, resulting in an impaired secondary structure of the hexanucleotide loop and loss of the cytosine bulge. Secondary structure modeling by the Mfold web server yields the same result. Nucleotides are numbered from the transcription initiation signal. Green dots represent common base pairs between the ensemble centroid (EC) structure diagram and the minimum free energy (MFE) structure diagram. Blue dots represent base pairs predicted only by the MFE structure diagram.
The Ghent +49A > G mutation shows reduced IRP1 binding
To assess the functional effect of the Ghent +49A > G mutation, the relative binding of recombinant IRP1 to the mutated IRE was evaluated in vitro by EMSA experiments. Qualitative results obtained by direct EMSA experiments indicate a 75% decrease (mean of four experiments) for binding of the Ghent +49A > G mutation to IRP1, relative to the WT FTL IRE sequence (Fig. 3A). As expected, the positive control +39ΔC mutation showed only minimal binding to IRP1, with a reduction of almost 95%. The full-length gel image is included in Supplementary Figure 3. One-way ANOVA showed that differences in the mean of intensities for the Ghent +49A > G mutation, negative and positive control are statistically significant (Fig. 3B). Post hoc analysis indicated that the mean of all three groups are statistically different from each other. The effect of the Ghent +49A > G mutation on IRP1 binding was evaluated quantitatively using a more stringent assay, a competitive EMSA. Using this assay, it was demonstrated that the +49A > G mutant competitor is less efficient in displacing the labeled probe than the WT competitor, as observed by a more gradual disappearance of the shifted band on the gel in the presence of increasing amounts of +49A > G mutant competitor when compared to the WT competitor (Fig. 4A). In particular, the competitor containing the Ghent +49A > G mutation starts to compete effectively at concentrations between 10- and 20-fold excess, which is significantly later than the negative control WT competitor that begins to show significant competition between 2- and 5-fold excess. In contrast, the +39ΔC competitor, used as a positive control, is inefficient in displacing the labeled probe, since the IRE containing this mutation does not show significant competition even at 80-fold excess. Full-length gel images are included in Supplementary Figure 4. A plot of the quantified band intensities in function of the molar excess of the competitor is given by Fig. 4B.

Direct EMSA experiments to qualitatively evaluate the effect of the Ghent +49A > G mutation on IRP/IRE binding affinity. Therefore, fluorescent-labeled probes of the +49A > G mutant IRE were incubated with IRP1 protein and loaded on a 5% native acrylamide gel. Fluorescent-labeled probes of the WT and +39ΔC mutant IRE were used as negative and positive controls respectively. (A) Representative gel image showing the intensities of the shifted IRP1/IRE complex. Lane 1 contains the labeled WT probes in absence of IRP1. Lane 2, 3 and 4 respectively contain labeled WT, +39ΔC mutant and +49A > G mutant probes in the presence of IRP1. (B) Band intensities of the two mutant groups were normalized relative to the intensity of the shifted band of WT IRE (lane 2) and presented as the mean of four experiments ± standard error of the mean. Statistical analysis was done by one-way ANOVA, followed by post hoc Bonferroni multiple comparison test (*p < 0.05, **p < 0.01, ***p < 0.001).

Competitive EMSA experiments to quantitatively evaluate the effect of the Ghent +49A > G mutation on IRP/IRE binding affinity. Fluorescent-labeled probes of the WT IRE were incubated with IRP1 protein and increasing molar excess (1X, 2X, 5X, 10X, 20X, 40X, 80X) of unlabeled +49A > G mutant competitor probes. Unlabeled competitor probes of the WT and +39ΔC mutant IRE were used as negative and positive controls respectively. Reactions were loaded on a 5% native acrylamide gel. (A) Representative gel images showing the intensities of the shifted IRP1/IRE complex. Lane N contains the labeled WT probe with IRP1 in the absence of unlabeled competitor. The following lanes contain labeled WT probe with IRP1 and increasing amounts of WT, +39ΔC mutant and +49A > G mutant competitor. (B) Band intensities of the WT and two mutant groups were normalized relative to the intensity of the shifted band in the absence of competitor (lane N) and presented on a logarithmic scale in function of the molar excess of the competitor. Means ± standard error of the mean of three independent experiments are shown.
Quantification of the apparent dissociation constant (KDapp) of the WT and +49A > G mutant IRE using a single independent site model21 indicates that the WT IRE has an KDapp of 0.50 nM, while the +49A > G mutant IRE demonstrates a more than 5-fold lower affinity for IRP1, with an KDapp of 2.70 nM. Since the +39ΔC mutant IRE is ineffective at binding IRP1, no single independent site model could be fitted to the values of this mutant IRE, therefore no KDapp could be calculated. In summary, in vitro EMSA experiments support a decreased binding affinity of the +49A > G mutant IRE for IRP1.
Discussion
In this study a novel mutation in the IRE of FTL, Ghent +49A > G, was found in a homozygous and heterozygous state in different members of a consanguineous family with HHCS. Another mutation at the same nucleotide position (+49A > C) has been reported once in a family with HHCS, however, no clinical data were provided23. So far, more than thirty point mutations and six deletions in the FTL IRE have been identified in patients with HHCS24,25. The Ghent +49A > G mutation adds to the repertoire of HHCS causing mutations.
The zygosity of +49A > G was found to correlate with disease expression, with the most severe phenotype observed in the index case harbouring the mutation in homozygous state. In particular, the serum ferritin level of the proband displays a roughly 5-fold increase in comparison with the heterozygous family members and is almost 10-fold higher than the normal reference values. Moreover, despite the young age of the proband, he shows the most severe clinical manifestations of cataracts among the affected individuals. Despite the fact that genotype-phenotype correlations between serum ferritin levels and HHCS severity are difficult to obtain, mainly due to age and gender variability of serum ferritin, our observation is in line with a more severe clinical phenotype in subjects with a homozygous mutation in comparison with heterozygous patients, as reported for multiple other diseases26.
So far, three HHCS families with rare homozygous mutations in the IRE of FTL have been reported25,27,28. In a first homozygous case serum ferritin levels were more than 2-fold higher than in heterozygous patients. The severity of cataracts however showed no correlation with mutation dose27. For the second case, no correlation between the state of zygosity and the severity of the clinical phenotype was found in the two homozygous and four heterozygous patients25. In the third case, only the proband was investigated, so no comparison could be made with heterozygous cases28. As noted previously, HHCS patients with the same mutation can demonstrate phenotypic diversity due to other genetic or environmental factors, concomitant pathologies or age-related penetrance6. Indeed, serum ferritin levels show inter- and intra-individual differences since they are affected by age and sex, while the age of cataract onset and its severity can be influenced by differences in diet, exposure to UV light, or substance abuse10. There have been, for instance, reports of young children with elevated serum ferritin levels but without cataracts, having the same mutation as their affected relatives with cataract12. In the proband reported here, the early-onset cataract formation could be explained by the unusual high levels of serum ferritin, causing a rapid accumulation of crystalline deposits in the lens. Interestingly, it has been demonstrated that endogenous FTL transcription is significantly higher in the lens compared to other eye tissues, which is likely to contribute to the pathogenic levels of FTL deposits found in HHCS lenses29. Several authors have also attempted to establish a relationship between the severity of the clinical features and the location of the mutation in the IRE structure10,25,30. In general, heterozygous mutations disturbing the hexanucleotide loop or the cytosine bulge give rise to strongly increased serum ferritin levels and early-onset bilateral cataract, while mutations affecting the base pairing of the upper or lower stem generally present a more moderate phenotype. The +49A > G mutation is located at the basis of the upper stem, right above the cytosine bulge. In the heterozygous patients, the mutation gives rise to a moderate increase of serum ferritin and mild cataract, supporting the abovementioned genotype-phenotype correlation.
Sanchez et al.31 performed a series of competitive EMSA experiments to determine IRP1 binding motifs in the IRE of H-ferritin (FTH)31. The FTH 5′ IRE probe containing the adenine to guanine change at the position corresponding to position +49 of the FTL 5′ IRE, showed IRP1 binding characteristics comparable to those of the WT probe. This implies that this change in FTH causes no loss of IRP1 binding affinity, as opposed to the +49A > G mutation in FTL, shown to effectively reduce IRP1 binding. This difference could be explained by the hypothesis the authors derived from additional experiments. Specifically, it was shown that the presence of three or more G-U or U-G wobble base pairs in the FTH 5′ IRE motif severely impairs its ability to compete with the WT probe. The WT FTL 5′ IRE has two U-G base pairs, compared to only one in the WT FTH 5′ IRE. Since +49A > G induces an additional U-G base pair, the threshold of three U-G base pairs is exceeded in mutant FLT, but not in mutant FTH. The results of the EMSA experiments in our study therefore illustrate that the hypothesis, allowing a maximum of two G-U or U-G wobble base pairs in order to preserve proper binding characteristics, can be broadened from FTH to FTL.
Bioinformatics tools show that the substitution of adenine by guanine at position +49 in the upper stem of the IRE is predicted to change the secondary structure of the FTL IRE, thereby affecting the apical loop as well as causing a loss of the cytosine bulge, elements that are critical for IRP/IRE recognition9. Furthermore, previous studies suggest that proper base pairings at the basis (+34/+49) and the top (+38/+45) of the upper stem of the IRE are crucial for obtaining the correct arrangement of nucleotides composing the upper stem and hexanucleotide apical loop31.
The functional effect of the +49A > G mutation in the FTL IRE on IRP1 binding affinity was evaluated by means of EMSA experiments. The direct as well as competitive EMSA experiments show that +49A > G reduces, but not completely abolishes, the binding with recombinant IRP1. From the EMSA data, we have calculated KDapp values for the WT and +49A > G IRE. The KDapp value of the mutant IRE is more than 5-fold lower than WT IRE, which also corresponds with the outcome of the direct EMSA experiment. The observations from both types of EMSA experiments thus suggest that the FTL 5′ IRE with +49 A > G is capable of binding IRP1 in vitro, albeit with a significantly reduced binding affinity. It seems, however, that the manifestation of the HHCS phenotype is independent of the strength of the mutation in terms of reduction of binding affinity. In particular, mutations that only mildly impair IRP/IRE binding in vitro, can also induce biochemical and clinical symptoms10,25, illustrating the high sensitivity of the IRP/IRE complex to minor perturbations in affinity.
In conclusion, we identified a novel non-coding mutation,“Ghent +49A > G”, in the IRE of FTL causing variable degrees of HHCS in a consanguineous family. The zygosity of the mutation correlated with the severity of the phenotypes in this family. The mutation was predicted to disrupt the secondary structure of the IRE. Functional characterization of the mutation revealed that +49A > G reduces, but does not completely abolishes, the binding to IRP1.
References
Craig, J. E. et al. Hereditary Hyperferritinemia-Cataract Syndrome: Prevalence, Lens Morphology, Spectrum of Mutations, and Clinical Presentations. Arch Ophthalmol 121, 1753–1761 (2003).
Beaumont, C. et al. Mutation in the iron responsive element of the L ferritin mRNA in a family with dominant hyperferritinaemia and cataract. Nat Genet 11, 444–446 (1995).
Girelli, D. et al. A linkage between hereditary hyperferritinaemia not related to iron overload and autosomal dominant congenital cataract. Br J Haematol 90, 931–934 (1995).
Platteau, E., Hoornaert, K., Moens, K. & Leroy, B. P. Age-dependent ocular phenotype in hereditary hyperferritinaemia cataract syndrome (HHCS). Acta Ophthalmol 90, e239–e240, https://doi.org/10.1111/j.1755-3768.2011.02142.x (2012).
Ghosh, S., Hevi, S. & Chuck, S. L. Regulated secretion of glycosylated human ferritin from hepatocytes. Blood 103, 2369–2376, https://doi.org/10.1182/blood2003-09-3050 (2004).
Girelli, D. et al. Clinical, biochemical and molecular findings in a series of families with hereditary hyperferritinaemia-cataract syndrome. Br J Haematol 115, 334–340 (2001).
Lachlan, K. L., Temple, I. K. & Mumford, A. D. Clinical features and molecular analysis of seven British kindreds with hereditary hyperferritinaemia cataract syndrome. Eur J Hum Genet 12, 790–796, https://doi.org/10.1038/sj.ejhg.5201252 (2004).
Muckenthaler, M., Gray, N. K. & Hentze, M. W. IRP-1 binding to ferritin mRNA prevents the recruitment of the small ribosomal subunit by the cap-binding complex eIF4F. Mol Cell 2, 383–388 (1998).
Joshi, R. S., Moran, E. & Sanchez, M. The IRP/IRE Regulatory Network, Iron Metabolism in Cellular Iron Metabolism (ed. Arora, S.) 25–58 (InTech, 2012).
Allerson, C. R., Cazzola, M. & Rouault, T. A. Clinical Severity and Thermodynamic Effects of Iron-responsive Element Mutations in Hereditary Hyperferritinemia-Cataract Syndrome. The Journal of biological chemistry 274, 26439–26447 (1999).
Mumford, A. et al. The lens in hereditary hyperferritinaemia cataract syndrome contains crystalline deposits of L-ferritin. Br J Ophthalmol 84, 697–700 (2000).
Campagnoli, M. F. et al. Onset of cataract in early infancy associated with a 32G–>C transition in the iron responsive element of L-ferritin. European journal of pediatrics 161, 499–502, https://doi.org/10.1007/s00431-002-1019-4 (2002).
National Institutes of Health (NIH). Ferritin blood test https://medlineplus.gov/ency/article/003490.htm (2017).
Richards, S. et al. Standards and guidelines for the interpretation of sequence variants: a joint consensus recommendation of the American College of Medical Genetics and Genomics and the Association for Molecular Pathology. Genet Med 17, 405–424, https://doi.org/10.1038/gim.2015.30 (2015).
D’Haene, B., Vandesompele, J. & Hellemans, J. Accurate and objective copy number profiling using real-time quantitative PCR. Methods 50, 262–270, https://doi.org/10.1016/j.ymeth.2009.12.007 (2010).
Coppieters, F. et al. Identity-by-descent-guided mutation analysis and exome sequencing in consanguineous families reveals unusual clinical and molecular findings in retinal dystrophy. Genet Med 16, 671–680, https://doi.org/10.1038/gim.2014.24 (2014).
Zuker, M. Mfold web server for nucleic acid folding and hybridization prediction. Nucleic Acids Res 31, 3406–3415, https://doi.org/10.1093/nar/gkg595 (2003).
Ding, Y., Chan, C. Y. & Lawrence, C. E. Sfold web server for statistical folding and rational design of nucleic acids. Nucleic acids research 32, W135–W141, https://doi.org/10.1093/nar/gkh449 (2004).
Gray, N. K. et al. Recombinant iron-regulatory factor functions as an iron-responsive-elementbinding protein, a translational repressor and an aconitase. Eur J Biochem 218, 657–667 (1993).
Gray, N. K., Pantopoulos, K., Dandekar, T., Ackrell, B. A. & Hentze, M. W. Translational regulation of mammalian and Drosophila citric acid cycle enzymes via iron-responsive elements. Proc Natl Acad Sci 93, 4925–4930 (1996).
Drake, S. K., Lee, K. L. & Falke, J. J. Tuning the Equilibrium Ion Affinity and Selectivity of the EF-Hand Calcium Binding Motif: Substitutions at the Gateway Position. Biochemistry 35, 6697–6705 (1996).
Zamir, E. Fuchs’ Heterochromic Uveitis. The American Uveitis Societ y http://www.uveitissociety.org/Resources/Documents/Patient%20Education/fhu.pdf (2003).
Castiglioni, E. et al. High resolution melting for the identification of mutations in the iron responsive element of the ferritin light chain gene. Clin Chem Lab Med 48, 1415–1418, https://doi.org/10.1515/CCLM.2010.281 (2010).
Mattila, R. M., Sainio, A., Jarvelainen, M., Pursiheimo, J. & Jarvelainen, H. A novel double nucleotide variant in the ferritin-L iron-responsive element in a Finnish patient with hereditary hyperferritinaemia-cataract syndrome. Acta Ophthalmol, https://doi.org/10.1111/aos.13492 (2017).
Luscieti, S. et al. Novel mutations in the ferritin-L iron-responsive element that only mildly impair IRP binding cause hereditary hyperferritinaemia cataract syndrome. Orphanet J Rare Dis 8, https://doi.org/10.1186/1750-1172-8-30 (2013).
Wilkie, O. A. The molecular basis of genetic dominance. J Med Genet 31, 89–98 (1994).
Alvarez-Coca-Gonzalez, J. et al. The hereditary hyperferritinemia-cataract syndrome: a family study. Eur J Pediatr 169, 1553–1555, https://doi.org/10.1007/s00431-010-1251-2 (2010).
Giansily-Blaizot, M., Cunat, S., Moulis, G., Schved, J. F. & Aguilar-Martinez, P. Homozygous mutation of the 5′UTR region of the L-Ferritin gene in the hereditary hyperferritinemia cataract syndrome and its impact on the phenotype. Haematologica 98, e42–e43, https://doi.org/10.3324/haematol.2012.077198 (2013).
Bennett, T. M. et al. Noncoding variation of the gene for ferritin light chain in hereditary and age-related cataract. Mol Vis 19, 835–844 (2013).
Cazzola, M. et al. Hereditary Hyperferritinemia-Cataract Syndrome: Relationship Between Phenotypes and Specific Mutations in the Iron-Responsive Element of Ferritin Light-Chain mRNA. Blood 90, 814–821 (1997).
Sanchez, M. et al. Iron regulatory protein-1 and -2: transcriptome-wide definition of binding mRNAs and shaping of the cellular proteome by iron regulatory proteins. Blood 118, e168–e179, https://doi.org/10.1182/blood-2011-04-343541 (2011).
Acknowledgements
This study was supported by the Ghent University Special Research Fund (BOF15/GOA/011) to E.D.B. and grant SAF2015-70412-R from Spanish Secretary of Research, Development and Innovation (MINECO), grant 2014 SGR225 (GRE, Grup Rercerca Emergent) from Generalitat de Catalunya and economical support from Fundació Internacional Josep Carreras and from Obra Social “la Caixa” Spain to M.S. S.V.d.S. is PhD fellow of the BOF (01D04716). E.D.B. is Senior Clinical Investigator of the FWO (1802215N). The authors gratefully acknowledge the family who participated in this study.
Author information
Authors and Affiliations
Contributions
S.V.d.S. designed research, performed the genetic analyses, the experimental studies and data analysis, and drafted the initial manuscript. M.S. and J.C. designed research, supervised the experimental studies and data analysis, and critically reviewed and revised the manuscript. L.P. and A.M. managed patients, provided and interpreted clinical data, and critically reviewed and revised the manuscript. E.D.B. designed research, supervised the genetic analyses and data analysis, and critically reviewed and revised the manuscript.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Van de Sompele, S., Pécheux, L., Couso, J. et al. Functional characterization of a novel non-coding mutation “Ghent +49A > G” in the iron-responsive element of L-ferritin causing hereditary hyperferritinaemia-cataract syndrome. Sci Rep 7, 18025 (2017). https://doi.org/10.1038/s41598-017-18326-6
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-18326-6
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
