
Abstract
Based on long-term follow-ups, this study was designed to investigate the incidence and risk factors for postoperative adjacent segment degeneration (ASD) after anterior cervical discectomy and fusion (ACDF) or total disc replacement (TDR) in treating cervical degenerative diseases. Between January 2000 and December 2005, 108 cases undergoing ACDF and 78 undergoing TDR, were enrolled into this study. All medical records were retrospectively collected. Every patient was followed up at least 10 years. Outcome assessment included visual analogue scale (VAS) score, Neck Disability Index (NDI) score, Japanese Orthopaedic Association (JOA) score, and radiographic parameters. Consequently, thirty-eight (35.2%) of 108 cases suffered from ASD in ACDF group, and 26 (33.3%) of 78 cases in TDR group. There was no statistical difference between the two groups regarding ASD incidence, VAS/NDI/JOA score, recovery rate. Logistic regression analysis showed that age (OR = 2.86, 95% CI, 1.58–4.14) and preoperative segmental lordosis (OR = 1.90, 95% CI, 1.05–3.20) were risk factors associated with increased odds of ASD regardless of surgical procedures. On the other hand, preoperative overall lordosis (OR = 0.54, 95% CI, 0.26–0.82) was most likely protective. In conclusion, advanced age and preoperative segmental lordosis were identified as risk factors for postoperative ASD, while preoperative overall lordosis proves to be a protective factor.
Similar content being viewed by others
Introduction
Anterior cervical discectomy and fusion (ACDF) which has been considered as the “gold standard” treatment of cervical degenerative diseases was founded by Smith-Robinson and Cloward inthe 1950s1. But in recent years, radiographic and clinical studies have shown that as time went by, the segements adjacent to the fused spinal segments occasionally degenerated or became unstable2,3,4.
ACDF surgery has changed the original mechanical behavior of the spine at the expense of the activity of the fusion segment; and in theory it may lead to the changes of adjacent vertebral stress distribution and the movement patterns, resulting in biomechanical changes including stress concentration of adjacent segments, compensatory increase in activity, and even instability5,6,7. However, the correlation between so-called “adjacent segment degeneration” and ACDF surgery still needs theoretical and experimental data to support. It is unclear whether ASD after ACDF surgery occurs due to segmental fusion, or it is just the normal physiological degeneration of the spine.
Nowadays, cervical total disc replacement (TDR) is a major non-fusion surgical method. Its designed concept is to retain as much as possible the intervertebral disc height and segmental activity, so as to reduce accelerated adjacent segment degeneration (ASD) that may be caused by ACDF surgery. Its short-term clinical results have been well demonstrated3,8,9,10,11,12,13,14,15,16, but the studies reporting long-term curative effect are still few17.
Thus, this study was designed to investigate the incidence and risk factors for postoperative ASD after ACDF or TDR surgery, and compare the clinical effects in treating cervical degenerative diseases, based on a long-term follow-up with a minimum of 10 years.
Patients and Methods
Statement
This study was approved by the local Ethics Committee of The Third Hospital of Hebei Medical University (Approval No. K2017–003–01). Informed consent was obtained from all participants and/or their legal guardian/s. The methods were carried out in accordance with the relevant guidelines and regulations.
Patient selection
Case selection had strict criteria as follows. Inclusion criteria are (1) single-level, radiculopathic; (2) cervical disc herniation; (3) degenerative cervical spinal stenosis; (4) conservative treatment for at least three months; (5) adult patients only; (6) no degeneration existing in the adjacent disc. Exclusion criteria are (1) severe facet joint degeneration (bridging osteophytes, intervertebral disc height loss > 50%, intervertebral activity < 2°); (2) developmental cervical stenosis; (3) ossification of posterior longitudinal ligament; (4) obviously unstable cervical spine with angular displacement > 2° or vertical displacement > 2 mm; (5) osteoporosis, or with spinal compression fractures; (6) cervical abnormalities; (7) cervical cancer; (8) cervical infection; (9) ankylosing spondylitis; (10) a history of cervical spine surgery.
It should be noted here that both the two groups of patients were not randomly selected; all included patients were suitable for TDR surgery or ACDF surgery. But taking account of the ethical issues and economic capacity of the patients, the final choice of selecting an operation was made by the patients themselves after a complete explanation to them before surgery.
Surgical procedures
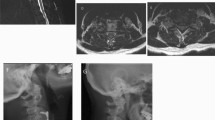
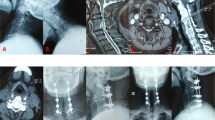
Surgery was performed with conventional technique as follows. Briefly, a standard right-sided anterior approach was performed. The symptomatic disc was removed, and then the posterior longitudinal ligament (PLL) was removed. The Syncage-C (Synthes company) or PEEK-Cage (Depuy company) with local bone was implanted into intervertebral space in ACDF group, as shown in Fig. 1A,B. For TDR group, the Bryan Cervical Disc Prosthesis (Medtronic Sofamor Danek, Inc, Memphis, TN) was implanted after accurate measurement, as shown in Fig. 1C,D.

X-ray images of ACDF and TDR surgery in treating cervical degenerative diseases. (A,B) The Syncage-C (Synthes company) or PEEK-Cage (Depuy company) with local bone was implanted into intervertebral space in ACDF group. (C,D) For TDR group, the Bryan Cervical Disc Prosthesis (Medtronic Sofamor Danek, Inc, Memphis, TN) was implanted into intervertebral space after accurate measurement. ACDF, anterior cervical discectomy and fusion; TDR, total disc replacement.
Radiographic measurements
Radiographic parameters were collected by screening neutral and dynamic flexion-extension lateral radiographs, including cervical lordosis, operated segmental height, C2-7 range of motion (ROM), operated segmental ROM, upper segmental ROM and lower segmental ROM, upper segmental height and lower segmental height. Neutral-position and dynamic flexion-extension lateral radiographs during each follow-up examination were evaluated with the PACS software and a PACS workstation (Centricity 2.0, General Electrics Medical Systems, Milwaukee, WI).
ASD was assessed through lateral X-ray film and MRI T2-weighted images. The Kellgren X-ray cervical vertebra degeneration system was a method considering the cervical degeneration just like the anterior vertebral osteophyte, disc height collapse, endplate sclerosis and anterior or posterior slip. The MRI manifestation of ASD was newly formation of intervertebral disc herniation and decreased signal intensity on MRI images using Miyazaki classification18. All radiological outcomes were reviewed by an independent spine surgeon and a radiologist, who were unaware of the treatment details. At last follow-up, the cases whose X-ray and (or) MRI appear ASD performance were included in ASD group, otherwise, included in non-ASD group.
Outcome assessment
All patients were required to return for follow-up. Clinical and radiological evaluation were performed at 1 week, 3 months, 1 year, postoperatively, and last follow-up (more than 10 years). Clinical effectiveness was evaluated by visual analogue scale (VAS) score, Japanese Orthopaedic Association (JOA) score (17 points system, 1994 revised edition)19,20 and Neck Disability Index (NDI) score. The recovery rate (RR) of JOA score was calculated according to the following formula: RR = (postoperative scores – preoperative scores)/(17 - preoperative scores) *100%.
Statistical analysis
Statistical analyses were performed using SPSS for Windows, version 18.0 (IBM SPSS Inc., New York, USA). Data are presented as Mean ± SD (standard deviation) for measurement data. Comparisons of VAS, JOA, NDI score, and preoperative radiographic parameters between ACDF group and TDR group were determined by Student t-test. For count data, it was presented as percentage, and chi-square test was used for data analysis. Non-conditional binary logistic regression model was used to explore the associated risk factors of ASD in patients after surgery. P values less than 0.05 were regarded as significant with two-tailed tests.
Results
Baseline data
This study was carried out between January 2000 and December 2005. As shown in Table 1, a total of 186 patients underwent ACDF surgery (108 cases), or Bryan (Medtronic Sofamor DanekInc, USA) TDR surgery (78 cases). The age is 50 ± 18 years in ACDF group, and 52 ± 19 years in TDR group. All cases have completed regular follow-ups of at least 10 years. The baseline data from two groups showed no significant difference regarding age, sex, and history of chronic diseases including diabetes mellitus, heart diseases, and high blood pressure. All operations were performed by the same surgeon (WYD).
ASD incidence
Two groups of patients successfully completed surgery without major complications. At last follow-up, it was found that 38 (35.2%) of 108 cases suffered from ASD in ACDF group, and 26 (33.3%) of 78 cases in TDR group. There was no statistical difference between the two groups regarding ASD incidence. We compared ASD group with non-ASD group and found that sex, disease duration, surgical approach and follow-up period had no significant differences (all P > 0.05). But the patients in ASD group (56 ± 12 years) are older than those in non-ASD group (50 ± 11 years) (P < 0.001).
VAS/JOA/NDI scores and RR
At last follow-up, VAS/JOA/NDI scores both in ACDF and TDR groups achieved significant improvement compared with the preoperative scores, as shown in Tables 2–4. However, there were no significant differences regarding VAS/NDI/JOA scores between ACDF group and TDR group. As well, there was no statistical difference regarding RR between ACDF group (RR = 75.56%) and TDR group (RR = 81.58%).
Preoperative radiographic parameters
As shown in Table 5, preoperative overall lordosis is 12.6 ± 1.1 in ASD group while it is 15.3 ± 1.4 in Non-ASD group. Thus, preoperative overall lordosis in ASD group is smaller than that in Non-ASD group (P < 0.001). Preoperative segmental lordosis is 2.8 ± 4.0 in ASD group while it is 1.1 ± 3.8 in Non-ASD group, with significant difference (P = 0.047). There were no statistical differences regarding ROM, segment height, or segmental activity between ASD group and Non-ASD group (all P > 0.05).
Logistic regression analysis
All patients were divided into three age groups according to WHO classification (~44; 45~59; 60~). As shown in Table 6, logistic regression analysis showed that the regression equation was presented as follows, logit P = −3.28 + 1.05*X1 − 0.62*X3 + 0.64*X4 (X1 = age, OR = 2.86, 95% CI, 1.58–4.14; × 3 = preoperative overall lordosis, OR = 0.54, 95% CI, 0.26–0.82; × 4 = preoperative segmental lordosis, OR = 1.90, 95% CI, 1.05–3.20). Herein, ‘logit P’ is the likelihood of developing an ASD after a surgery, regardless of the technical procedures used.
Discussion
In our study, postoperative neurological function scores of both ACDF group and TDR group were significantly different from preoperative scores respectively, and there was no significant difference between the two groups at different timepoints. It showed that the postoperative clinical results, involving significant improvement in neurological function and quality of life were satisfactory when compared with preoperative status, regardless of surgical procedures, ACDF or TDR. Reported literature (randomized controlled clinical studies) had shown that the short-term effect of TDR surgery was not inferior to ACDF surgery21,22,23. These results were similar to those of our study. The same surgery point of the two surgical ways above was the operation of thoroughly complete decompression in the pathological level. It might indicate that recovery of neurological function was primarily related to whether intraoperative decompression was thorough or not, not the selection of surgical methods.
Some reported literature indicated that cervical sagittal curvature had an important impact on neck pain, spinal cord compression and ASD24,25. Pickett et al.26 and Johnson et al.27 reported that Bryan TDR surgery might bring about deformity of segmental kyphosis. In this study, we found that the ROM recovered to the preoperative value during the follow-up period after Bryan TDR surgery. Meanwhile, the treated segment ultimately showed preservation of movement when compared with the preoperative levels. Postoperative overall lordosis angle after ACDF surgery was basically consistent with the preoperative status. As compared with ACDF, Bryan TDR surgery had a better effect on recovery and reconstruction of overall lordosis angle. However, the Bryan TDR surgery was non-fusion surgery without titanium plate fixation. How to avoid the kyphosis that the above scholars reported, and how to achieve overall lordosis improvement? We should pay more attention to the following aspects: (1) to keep neutral position and avoid hyper-extension during operation; (2) to thoroughly remove the osteophytes at anterior lower edge of the upper vertebral body, and to avoid improper intervertebral height resulting in excessive lordosis; (3) to determine the exact prosthesis model through accurately measuring the size of vertebral body in X-ray images; (4) to be sure that insertion direction of prosthesis was parallel to the intervertebral space; (5) excessive scraping on cartilage endplate should be avoided, especially near to the dorsal side.
Cervical local and overall activity was critical for both ACDF surgery and TDR surgery. In this study, the difference of preoperative overall activity between the two groups was not statistically significant. At last follow-up, overall activity in TDR group decreased average 1.8° compared with preoperative data, while that in ACDF group decreased average 4.0° compared with preoperative data. It indicated that TDR surgery had significant effect of maintaining cervical overall activity. The surgery has been widely used in clinical practice since 2000 and has received good clinical efficacy. Quan et al.28 followed up the patients who had underwent Bryan TDR surgery for more than 8 years, 78% of the patients still maintained a good activity. In the present study, we have found that TDR has the role of maintaining overall and segmental activity significantly, which is consistent with the previous report.
In this study, we measured intervertebral disc height and mobility of adjacent segments both before and after surgery in ACDF and TDR group. Intervertebral disc height and ROM were currently the standard evaluation method in ASD applied by the majority of authors. The results showed that intervertebral disc height and ROM of adjacent segments had no significant differences before and after surgery, regardless of TDR group or ACDF group. Sasso et al.29 followed up 22 patients who underwent TDR surgery and found that the upper adjacent vertebral activity was about 10° and the lower was about 15° two years after the surgery. They concluded with prolonged follow-up period that the vertebral activity of adjacent segments increased after ACDF surgery, which was consistent with the findings in our study.
Long-term follow-up interview after ACDF surgery indicated that there were many complications, such as subsequent instability, loss of physical activity, ASD and so on. ASD pathological changes mainly included cervical spondylosis changes, such as cervical osteophyte formation around the vertebral body, disc space narrowing, vertebral slippage, disc herniation, hypertrophy and ossification of the yellow ligament in X-ray and/or CT/MRI images. All of the proliferative and degenerative performance will inevitably lead to degenerative cervical stenosis of the fused and adjacent segments, resulting in spinal cord injury and a corresponding neurological symptoms30. ASD has an adverse impact on the long-term effect on the recovery for patients undergoing ACDF surgery, which has become a major anterior cervical complication.
In the prior univariate analysis, it was found that the patients in ASD group (56 ± 12 years) are older than those in non-ASD group (50 ± 11 years) (P < 0.001). In the logistic regression analysis, all patients in this study were divided into three age groups according to WHO classification (~44; 45~59; 60~), and advanced age was identified as a risk factor of postoperative ASD. We can identify advanced age as a risk factor, but we cannot set the range of age. Cervical lordosis is the biomechanically ideal alignment, but it refers to the overall lordosis. In this study, high-level segmental lordosis was identified as a risk factor of postoperative ASD, whereas high-level overall lordosis was observed to act as a protective factor.
This study goes along with some limitations. First, ACDF surgery and TDR surgery were not randomly selected for the patients, because both two procedures were suitable for patients and the final surgical option was determined by the patients mainly depending on their medical expense. Second, the non-randomized character of the study design was bound to cause some selection bias, even though the baseline and demographic data in the two groups had no statistically significant differences. In addition, the small sample size was also a limitation in this study. This study only looked at radiographic ASD, which is another limitation.
Osteoporosis may lead to the deformation of the cervical vertebra and cause the stenosis of the vertebral canal, which is a potential risk factor for promoting the degeneration of cervical vertebra and developing into cervical spondylosis31. As a retrospective study, osteoporosis cannot be checked for in all patients; thus, only some patients were checked for osteoporosis after being admitted to our hospital. We only can judge the osteoporosis of the rest patients by screening the existed X-ray photographs. It is really another limitation in this study. At last, no recording of other complications including reoperation, symptom recurrence, is also a limitation in this study.
In summary, both ACDF surgery and TDR surgery for cervical single-level degenerative diseases have achieved satisfying clinical results. Postoperative ASD incidence in the two groups has no significant difference. Advanced age and high-level preoperative segmental lordosis were identified as risk factors for postoperative ASD, while high-level preoperative overall lordosis may act as a protective factor.
References
Whitecloud, T. S. Anterior surgery for cervical spondylotic myelopathy. Smith-Robinson, Cloward, and vertebrectomy. Spine (Phila Pa 1976) 13, 861–863 (1988).
Matsumoto, M. et al. Anterior cervical decompression and fusion accelerates adjacent segment degeneration: comparison with asymptomatic volunteers in a ten-year magnetic resonance imaging follow-up study. Spine (Phila Pa 1976) 35, 36–43 (2010).
Hisey, M. S. et al. Prospective, Randomized Comparison of One-level Mobi-C Cervical Total Disc Replacement vs. Anterior Cervical Discectomy and Fusion: Results at 5-year Follow-up. Int J Spine Surg 10, 10 (2016).
Rajakumar, D. V., Hari, A., Krishna, M., Konar, S. & Sharma, A. Adjacent-level arthroplasty following cervical fusion. Neurosurg Focus 42, E5 (2017).
Ding, F. et al. Fusion-nonfusion hybrid construct versus anterior cervical hybrid decompression and fusion: a comparative study for 3-level cervical degenerative disc diseases. Spine (Phila Pa 1976) 39, 1934–1942 (2014).
Hou, Y. et al. Cervical kinematics and radiological changes after Discover artificial disc replacement versus fusion. Spine J 14, 867–877 (2014).
Jawahar, A. & Nunley, P. Total disc arthroplasty and anterior cervical discectomy and fusion in cervical spine: competitive or complimentary? Review of the literature. Global Spine J 2, 183–186 (2012).
McAfee, P. C., Reah, C., Gilder, K., Eisermann, L. & Cunningham, B. A meta-analysis of comparative outcomes following cervical arthroplasty or anterior cervical fusion: results from 4 prospective multicenter randomized clinical trials and up to 1226 patients. Spine (Phila Pa 1976) 37, 943–952 (2012).
Alvin, M. D. & Mroz, T. E. The Mobi-C cervical disc for one-level and two-level cervical disc replacement: a review of the literature. Med Devices (Auckl) 7, 397–403 (2014).
Hisey, M. S. et al. Multi-center, prospective, randomized, controlled investigational device exemption clinical trial comparing Mobi-C Cervical Artificial Disc to anterior discectomy and fusion in the treatment of symptomatic degenerative disc disease in the cervical spine. Int J Spine Surg 8, (2014).
Davis, R. J. et al. Two-level total disc replacement with Mobi-C cervical artificial disc versus anterior discectomy and fusion: a prospective, randomized, controlled multicenter clinical trial with 4-year follow-up results. J Neurosurg Spine 22, 15–25 (2015).
Hisey, M. S. et al. Prospective, Randomized Comparison of Cervical Total Disk Replacement Versus Anterior Cervical Fusion: Results at 48 Months Follow-up. J Spinal Disord Tech 28, E237–243 (2015).
Luo, J., Gong, M., Huang, S., Yu, T. & Zou, X. Incidence of adjacent segment degeneration in cervical disc arthroplasty versus anterior cervical decompression and fusion meta-analysis of prospective studies. Arch Orthop Trauma Surg 135, 155–160 (2015).
Meisel, H. J. et al. Four-year results of a prospective single-arm study on 200 semi-constrained total cervical disc prostheses: clinical and radiographic outcome. J Neurosurg Spine 25, 556–565 (2016).
Tian, W. et al. Comparison of the Clinical and Radiographic Results Between Cervical Artificial Disk Replacement and Anterior CervicalFusion: A 6-Year Prospective Nonrandomized Comparative Study. Clin Spine Surg 30, E578–578E586 (2017).
Laxer, E. B. et al. Adjacent segment degeneration following ProDisc-C total disc replacement (TDR) and anterior cervical discectomy and fusion (ACDF): does surgeon bias effect radiographic interpretation. Eur Spine J 26, 1199–1204 (2017).
Lanman, T. H. et al. Long-term clinical and radiographic outcomes of the Prestige LP artificial cervical disc replacement at 2 levels: results from a prospective randomized controlled clinical trial. J Neurosurg Spine 27, 7–19 (2017).
Miyazaki, M., Hong, S. W., Yoon, S. H., Morishita, Y. & Wang, J. C. Reliability of a magnetic resonance imaging-based grading system for cervical intervertebral disc degeneration. J Spinal Disord Tech 21, 288–292 (2008).
Yukawa, Y. et al. Laminoplasty and skip laminectomy for cervical compressive myelopathy: range of motion, postoperative neck pain, and surgical outcomes in a randomized prospective study. Spine (Phila Pa 1976) 32, 1980–1985 (2007).
Yang, S. et al. Early and intermediate follow-up results after treatment of degenerative disc disease with the Bryan cervical disc prosthesis: single- and multiple-level. Spine (Phila Pa 1976) 33, E371–377 (2008).
Heller, J. G. et al. Comparison of BRYAN cervical disc arthroplasty with anterior cervical decompression and fusion: clinical and radiographic results of a randomized, controlled, clinical trial. Spine (Phila Pa 1976) 34, 101–107 (2009).
Murrey, D. et al. Results of the prospective, randomized, controlled multicenter Food and Drug Administration investigational device exemption study of the ProDisc-C total disc replacement versus anterior discectomy and fusion for the treatment of 1-level symptomatic cervical disc disease. Spine J 9, 275–286 (2009).
Sasso, R. C., Anderson, P. A., Riew, K. D. & Heller, J. G. Results of cervical arthroplasty compared with anterior discectomy and fusion: four-year clinical outcomes in a prospective, randomized controlled trial. J Bone Joint Surg Am 93, 1684–1692 (2011).
Katsuura, A., Hukuda, S., Saruhashi, Y. & Mori, K. Kyphotic malalignment after anterior cervical fusion is one of the factors promoting the degenerative process in adjacent intervertebral levels. Eur Spine J 10, 320–324 (2001).
Ferch, R. D., Shad, A., Cadoux-Hudson, T. A. & Teddy, P. J. Anterior correction of cervical kyphotic deformity: effects on myelopathy, neck pain, and sagittal alignment. J Neurosurg 100, 13–19 (2004).
Pickett, G. E., Mitsis, D. K., Sekhon, L. H., Sears, W. R. & Duggal, N. Effects of a cervical disc prosthesis on segmental and cervical spine alignment. Neurosurg Focus 17, E5 (2004).
Johnson, J. P. et al. Sagittal alignment and the Bryan cervical artificial disc. Neurosurg Focus 17, E14 (2004).
Quan, G. M., Vital, J. M., Hansen, S. & Pointillart, V. Eight-year clinical and radiological follow-up of the Bryan cervical disc arthroplasty. Spine (Phila Pa 1976) 36, 639–646 (2011).
Sasso, R. C., Smucker, J. D., Hacker, R. J. & Heller, J. G. Artificial disc versus fusion: a prospective, randomized study with 2-year follow-up on 99 patients. Spine (Phila Pa 1976) 32, 2933–2940; discussion2941–2942 (2007).
Teramoto, T. et al. Long-term results of the anterior cervical spondylodesis. Neurosurgery 35, 64–68 (1994).
Ding, Y. et al. The effects of osteoporosis and disc degeneration on vertebral cartilage endplate lesions in rats. Eur Spine J 23, 1848–1855 (2014).
Author information
Authors and Affiliations
Contributions
Conceived and designed the study: W.Y.D. Collected data: S.D.Y., S.Z.Y. and D.L.Y. Analyzed the data: S.D.Y. and J.D. Wrote the paper: S.D.Y. and Y.B.Z.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Yang, SD., Zhu, YB., Yan, SZ. et al. Anterior cervical discectomy and fusion surgery versus total disc replacement: A comparative study with minimum of 10-year follow-up. Sci Rep 7, 16443 (2017). https://doi.org/10.1038/s41598-017-16670-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-16670-1
This article is cited by
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
