
Abstract
The Japan Gerontological Evaluation Study is a nationwide cohort study of individuals aged 65 years and older established in July 2010. Seven months later, one of the study field sites was directly in the line of the 2011 Great East Japan Earthquake and Tsunami. Despite the 1-hour warning interval between the earthquake and tsunami, many coastal residents lost their lives. We analyzed the risk of all-cause mortality on the day of the disaster as well as in the 38-month interval after the disaster. Among 860 participants, 33 (3.8%) died directly because of the tsunami and an additional 95 people died during the 38-month follow-up period. Individuals with depressive symptoms had elevated risk of mortality on the day of the disaster (odds ratio = 3.90 [95% CI: 1.13, 13.47]). More socially connected people also suffered increased risk of mortality, although these estimates were not statistically significant. In contrast, after the disaster, frequent social interactions reverted back to predicting improved survival (hazard ratio = 0.46 (95% CI: 0.26, 0.82)). Depressive symptoms and stronger social connectedness were associated with increased risk of mortality on the day of the disaster. After the disaster, social interactions were linked to improved survival.
Similar content being viewed by others

Introduction
An estimated 99,700 people have lost their lives annually on average due to global natural disasters in the past decade1. In addition to direct impact, disasters also increase mortality as a result of acute stress, injuries, disruptions in medical care, heart disease, suicide, and other causes2,3,4,5,6,7,8,9,10. Many victims develop posttraumatic stress disorder or other mental disorders11,12,13,14. Acute stress after a disaster is thought to trigger cardiovascular events4,5,10. Victims who are forced to relocate frequently experience worse living conditions as well as disruption of their social networks, and these factors may also adversely affect mental and physical health2,13.
Although a framework for disaster risk reduction was developed by the United Nations Office in 201515, potential risk factors for mortality pre-dating the events are not well understood. An obvious reason is that most studies of disasters are conducted after the fact, and they must rely on retrospective recall among the survivors, limited medical records, or ecological data2,3,4,5,6,7,8,9,16,17,18,19,20,21. A notable exception is the Study of the Tsunami Aftermath and Recovery (STAR) conducted before and after the 2004 Indian Ocean Tsunami that killed more than 130,000 people22. However, because their baseline survey was focused on social and economic conditions, information on health and behavioral risk factors was not collected. Other exceptions to the absence of pre-disaster information include cohort studies from New Zealand and Sweden that were able to take advantage of the fact that disaster struck in the midst of ongoing follow-up23,24; however, these studies did not examine mortality as an outcome.
Despite the about 1-hour warning interval between the earthquake and tsunami triggered by the 2011 Great East Japan Earthquake and Tsunami, 15,894 people lost their lives and 2,546 people remained missing25. The maximum run-up height of the tsunami recorded 40.5 m, and 90% of the deaths were due to drowning26. Pro-social behavior, such as helping others to evacuate, may have increased the risk of mortality during the disaster27,28,29, but epidemiological evidence remains scarce. In addition, more than 60% of fatalities were older adults18,26. Although older people are considered to be a vulnerable group in disaster planning policy30,31,32, specific risk and protective factors for mortality remain poorly understood. For example, depression is quite prevalent in the older population33, and possibly contributes to delayed evacuation in the event of disaster. In the present analysis, we conducted a longitudinal assessment of risk factors for tsunami-related mortality using baseline data collected 7 months before the 2011 earthquake and tsunami.
Results
The mean age of participants was 75.6 (SD = 7.7) years. On the day of the disaster 33 participants died (mortality rate = 3.8%). An additional 95 participants died in the 3.15-year interval (mean follow-up period was 2.96 years) after the disaster. Baseline characteristics and mortality rates on the day of and day after the disaster are shown in Table 1. On the day of the disaster, those living less than 1 km from the coast (Figs 1, 2, and 3a), as well as those with pre-existing severe depressive symptoms had higher mortality rates. Participants co-habiting with others tended to have higher mortality than people living alone on the day of the disaster. However, after the disaster, people living alone experienced higher mortality. After the disaster, participants without any social interactions had higher mortality rates though it was not observed during the disaster.

A heat map of Iwanuma City, the present study field, showing the density of mortality on the day of the Great East Japan Earthquake and Tsunami and the tsunami inundated area (N = 4,873 on March 11, 2011). The area surrounded by red dot-line and inundated by the tsunami is Tamaura district. Respondents living in the Tamaura district (N = 860) were included into the current analysis. The southern part of Tamaura district shown in the white color is the Abukuma River. Hiroyuki Hikichi edited the geographic data using ArcGIS Pro 1.1. (Esri, Redlands, California, USA), which were obtained from City Bureau (http://fukkou.csis.u-tokyo.ac.jp) and National Spatial Planning and Regional Policy Bureau (http://nlftp.mlit.go.jp/ksj/), Ministry of Land, Infrastructure, Transport and Tourism.

Survival rate (%) by distance living from the coast since the baseline survey for all districts in Iwanuma city (N = 4,937 on August 1, 2010).

(a) Mortality rate (%) on the day of the Great East Japan Earthquake and Tsunami by distance living from the coast in Tamaura districts (N = 860). (b) Prevalence of the participants with severe depressive symptoms (%) before the day of the Great East Japan Earthquake and Tsunami by distance living from the coast in Tamaura districts (N = 860).
Table 2 presents the main risk factors for mortality on the day of and the day after the disaster (Supplementary Tables 1 and 2 show the results of other variables, univariate analysis, and sensitivity analysis). On the day of the disaster, compared to residents living 2000 m or more from the coast, participants living 0–499 m (odds ratio [OR] = 22.66 (95% confidence interval [CI]: 5.78, 88.84)) and 500–999 m (OR = 16.88 (95% CI: 4.33, 65.84)) had elevated risks of mortality (Table 2a). However, after the disaster, there was no significant association between distance and mortality after controlling for other characteristics.
Although statistically non-significant, physical strength (taller body height served as proxy) tended to be protectively associated with mortality on the day of the disaster (compared to taller people, participants with a height of less than 150 cm had a 2.98 times increased mortality rate (95% CI: 0.75, 11.84), but men had higher mortality (OR = 2.74 (95% CI: 0.77, 9.68)) compared to women (Table 2b).
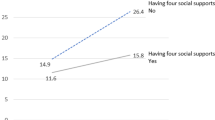
Those with greater social connectedness paradoxically appeared to have higher mortality risk on the day of the disaster (Table 2c). Those living with others had relatively higher risk of mortality than those living alone, although these estimates were not significant due to the small number of events. Although social interactions with friends and neighbors were not protectively associated with death on the day of the disaster, in the 3-year extended follow-up interval, the association between social interactions and mortality reverted back to a protective pattern, which has normally been observed in epidemiological studies (Table 2c).
Severe depressive symptoms pre-dating the disaster were associated with elevated risk of death on the day of the disaster (OR = 3.90 (95% CI: 1.13, 13.47), Table 2d), although participants with severe depressive symptoms lived, not only in coastal areas, but also in inland areas (Fig. 3b). The mortality rates among disabled participants were lower on the day of the disaster, but higher after the disaster.
Discussion
On the day of the March 11, 2011 disaster, 92.4% of deaths were due to drowning26. This situation differed from that noted during previous inland earthquakes in which many people died due to the collapse of their homes31,34,35. In this study field, the earthquake occurred at 2:46 p.m., and the tsunami reached the Iwanuma coastline at 3:56 p.m.36. Although there was a 1-hour warning interval between the earthquake and the tsunami, some residents in the coastal areas still failed to evacuate. Our study examined pre-existing risk factors for mortality among older people. In addition to residential distance from the coastline, we found that presence of depressive symptoms before the disaster was a major risk factor for mortality on the day of the disaster. This new finding was made possible only as a result of our unique study design. In addition, people with stronger social relationships tended to be at increased risk of mortality on the day of the disaster, possibly because they tried to help others. However, in the months and years following the disaster, a protective impact of social interactions was observed. Other risks of mortality after the disaster were also primarily driven by conventional risk factors (such as older age). These findings contribute to deepening our understanding of the life-threatening impact of disasters.
The present study has several strengths. Explanatory variables were available pre-dating the disaster. This “natural experiment” design enabled us to avoid recall bias in the aftermath of the disaster, and to produce robust evidence for the creation of disaster preparedness policies.
This study also has several limitations. First, the response rate was only 59.0% at the baseline (pre-disaster) survey. However, as a whole, comparison to census data in Iwanuma supported the representativeness of the present data37, and the follow-up rate for the mortality outcome was high (99.6%). In addition, the response rate was comparable to that in other surveys involving community-dwelling residents38. For example, response rates of community-dwelling resident surveys in 10 European countries varied from 37.6% to 73.6%38. Second, although the GDS-15 has been validated as a measure of depressive symptoms, most of the variables in our survey were self-reported.
Some residents in the coastal areas failed to evacuate in spite of the 1-hour interval between the earthquake and the tsunami. There were several reasons for this. First, the earthquake damaged the electric power supply and impeded communications, which contributed to delays in evacuation. In addition, past tsunami experiences may have lulled some people into a false sense of security and they did not feel evacuation was necessary39. In the year prior to the disaster (February 28, 2010), the highest level tsunami alert was issued in the same area followed by evacuation of residents; however, the tsunami did not even reach the land on that occasion. In addition, two days prior to the March 11 event, a lower level tsunami alert was issued, but again the waves did not reach the land. These past tsunami experiences are believed to have contributed to a false sense of security among some local residents and delayed their evacuation. Third, there was a possibility that some heuristic-based biases distorted evacuation decision making28. Normality bias, which is the human’s propensity to consider abnormalities as normal, may have contributed to delaying evacuation27. This cognitive bias can be potentiated by groupthink28. These heuristic-based biases can delay evacuation, for example, waiting for others to be able to evacuate together. In the present study, people living with other family members tended to have higher mortality rates on the day of the disaster, even though social isolation is an established risk factor for death in normal situations40,41. In particular, people living with parents who were more vulnerable because of higher age30,31,32 had higher risk of mortality. This finding might be explained by pro-social behavior, i.e. helping others to evacuate, that may have increased the risk of being caught in the tsunami27. In the Indian Ocean tsunami, family members helping each other is also believed to have paradoxically decreased the chances of survival22. Therefore, higher mortality among men on the day of the disaster might also be explained by altruistic behavior. There is a possibility that an older adult with disability would be more likely to live with other family members. In fact, however, in the Japan Gerontological Evaluation Study (JAGES) cohort, people living alone tended to be older and to report lower activities of daily living (ADLs) compared to those co-habiting with others (Supplementary Table 4). In the analysis, we adjusted for pre-disaster disability status and other covariates. It is also possible that social connectedness was correlated with death due to delayed evacuation while waiting for others’ help to arrive.
A novel finding of the present study is that severe depressive symptoms also delayed evacuation ahead of the tsunami. There are possible explanations to account for the correlation between depressive symptoms and delayed evacuation. Delayed response is observed among depressed individuals because of the changes in brain function in the reward-related regions42,43. Because of decreased reward processing, it is difficult for depressed individuals to modify unhealthy behavior to improve health44. In addition, depressed older people tend to have cognitive impairment and dementia45. Psychomotor retardation, which includes motor and cognitive impairment, is a major feature of depression46. Feelings of hopelessness – i.e. negative expectation bias about the outcome of any attempt to save themselves - may have also reduced the motivation to evacuate47. These mechanisms may explain delayed evacuation among participants with severe depressive symptoms.
There are some possible reasons why distance from the coast, the proxy of personal experiences of disaster damage, did not have a clear effect on mortality after the disaster. In relocating the displaced survivors of the disaster, Iwanuma City officials consciously strove to maintain the social networks of residents. Most survivors were moved to shelters and temporary housing together with their neighbors; thus, even after the disaster, they successfully kept their “community” that existed before the disaster. Therefore, many survivors were able to maintain the same social networks as before the disaster and this seemed to be beneficial to their mental health48,49. The residences to house the displaced survivors were also built within one block of a large local hospital, so that geographical barriers to health care access were minimized.
There are also some notable similarities between the present study and previously reported findings from the Indian Ocean tsunami22. In both studies, living closer to the coast, shorter body height, and living with older people were associated with higher mortality, while socioeconomic status did not have a strong impact. In the Indonesia study, physical strength, which is related to swimming and running ability, was a key factor for survival during the tsunami (male sex and body height were the proxies for these characteristics), whereas being female, being a child or an older adult, having a shorter height, and living with an older woman were each associated with higher tsunami mortality22. Therefore, the present results relating to these risk factors could be generalized to other populations. In contrast, in our study, physical strength was not necessarily associated with survival, though shorter height and older age tended to be associated with heightened mortality risk. In fact, mortality risks were lower among women, the disabled, and those reporting less physical activity prior to the disaster. One possible reason for this is that older people living in nursing homes were assisted by the staff to evacuate in Iwanuma City50. In addition, the discrepant results between the Indian Ocean tsunami and the current study may be partly ascribed to differences in water temperature since Sumatra is located at a latitude of 5°N and Iwanuma City at a latitude of 38°N. The water temperature around the study area at the time was lower than 0 °C51. Cold-shock and hypothermia52 would have been major causes of mortality in the Japan tsunami, even if people, especially men, could swim.
Aldrich and Sawada20 conducted an ecological study of the determinants of mortality in the 2011 Great East Japan Earthquake and Tsunami. They reported that municipal levels of social capital – the lower level of local crime rate served as proxy – were associated with lower mortality. Because our study focused on individual mortality risk (as well as individual measures of social connectedness), we cannot directly compare our results to those of the previous study. Similar to our study, Weil, et al.53 reported longitudinal effects of social capital following exposure to disaster. Immediately following Hurricane Katrina in the U.S., people with higher social capital experienced increased stress because they helped displaced victims, but thereafter they were found to quickly recover.
Social connectedness was beneficial for longer term survival, which is consistent with previous studies41. Social connectedness is thought to reduce mortality among disaster survivors by acting as a buffer against stress41. Social support relating to altruistic behavior from neighbors could have helped to reduce emotional stress, and served as a source of instrumental assistance in daily life. Previous studies reported favorable association of social capital and recovery after disaster53,54,55,56,57,58. According to Aldrich58 the mechanisms by which local social capital enhance disaster recovery include mutual assistance between residents, collective action, and stronger linkage between victims and government services.
The present results include a public health implication: disaster evacuation planning should take into account that those with depressive symptoms have greater difficulty in evacuation situations than those who are not depressed. In addition, since it is difficult to behave as disaster experts wish when disaster occurs59, sharing understanding about human’s pro-social behavior and cognitive bias should be included in emergency public health education. Although our study examined the risks of tsunami-related mortality, further evidence is needed for other types of disasters, which may differ with respect to factors that predict survival.
In conclusion, this natural experiment study produced robust evidence for the creation of disaster preparedness policies. Pre-existing individual, social, and health characteristics affect mortality risk during and after a major disaster, and the effects of social connectedness may differ during versus after a disaster.
Methods
Cohort study design
This study is part of a larger ongoing, nationwide prospective cohort study, called the Japan Gerontological Evaluation Study (JAGES)37,60,61,62. In August 2010, a census of all residents aged 65 years or older was conducted in Iwanuma City, Miyagi Prefecture, for studying the determinants of healthy aging and functional disability. At that time, Iwanuma had a population of 44,187 living over an area of 60.71 km2. A census was taken of all the city’s residents aged over 65 years. Questionnaires were sent to 8,576 residents and 5,058 were returned. The response rate was 59.0%, which is comparable to other surveys of community-dwelling residents in European countries38. Seven months following the establishment of the cohort baseline, the east coast of Japan (including Iwanuma) was struck by a magnitude 9.0 earthquake and tsunami. On March 11, 2011, the earthquake occurred at 2:46 p.m., and the first wave of the tsunami reached the Sendai Airport (Fig. 1) located in Iwanuma at 3:56 p.m.36, though the time the tsunami arrived varied between municipalities. The height of the tsunami around the Sendai Airport was 5.6 to 12.3 m63. Figure 1 depicts the heat map of mortality in relation to the tsunami-inundated areas of Iwanuma city. The tsunami swept 48% of the municipality’s land area, and 187 residents including younger people lost their lives. This study is therefore a unique “natural experiment” in which we had information about the residents of a disaster-affected area that pre-dated the event. To determine the risk factors for mortality on the day of the disaster, we restricted our analysis to residents of Tamaura-district where all of the land area was inundated (N = 860). A flow chart of the participants is shown in Fig. 4. ArcGIS Pro version 1.1.1. (Esri, Redlands, CA) was used for drawing the map.

Japan Gerontological Evaluation Study/Iwanuma Project cohort composition.
Mortality assessment
Our outcome was all-cause mortality. Mortality data of the participants up to May 5, 2014 were obtained from the national long-term care insurance database. Local physicians are required to report all deaths to the local municipal government. The insurance database enabled us to link 99.6% of cohort participants.
Social and demographic predictors
We measured each resident’s distance from the coast as an indicator of tsunami damage. We used years of educational attainment as an indicator of socioeconomic status. Social connectedness was measured by household living arrangement: living alone, living with parent(s), or co-habiting with others (e.g. spouse, adult children), but not parent(s), and by social interactions (frequency of informal socializing with friends-not meeting any friends or meeting some friends). If participants lived with parent(s) and others, they were categorized as “living with parent(s)”.
Health status and health behavior
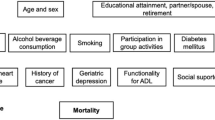
Comorbidity was determined by inquiring about current medical treatment for the following conditions related to major causes of death in Japan: cancer, heart disease, stroke, and respiratory diseases64. We also inquired about body height, since this had been previously reported to be associated with tsunami-related mortality22,65. Depressive symptoms were assessed by the Japanese version66 of the Geriatric Depression Scale (GDS-15)67. Total scores of GDS were categorized as follows: 0–4, normal; 5–8, mild; 9–11, moderate; and 12–15, severe68. ADLs were determined by asking whether participants could walk, take a bath, or use the toilet independently. We also inquired about the following health behaviors: smoking, alcohol consumption, and physical exercise (i.e. walking time per day in min). Body mass index (BMI) was also calculated from self-reported height and weight.
Statistical analyses
The Kaplan-Meier survival curves from the day of the disaster up to three years of follow-up among all survey participants (N = 4,937) are shown in Fig. 2. The mortality rates on the day of the disaster according to distance of residents from the coastline (Tamaura district, N = 860) are shown in Fig. 3a. The prevalence of the participants with severe depressive symptoms at the baseline by distance living from the coast in Tamaura districts (N = 860) are shown in Fig. 3b.
We separately analyzed risk factors for mortality on the day of the disaster versus up to 38 months after the disaster. We applied logistic regression models to determine the risk of mortality on March 11, 2011, the day of the disaster. Because of the small number of events (N = 33 deaths) relative to the number of predictor variables, we applied logistic regression with penalized maximum likelihood estimation for rare events analysis69. Next we used Cox proportional hazards models to examine mortality risk from one day after the disaster up to 3.15 years (38 months) after the disaster (March 12, 2011 to May 5, 2014).
We applied the missing at random assumption, and created 10 datasets using the multivariate normal imputation method70. Results of univariate analyses, results of sensitivity analyses, and information on the missing responses are shown (Supplementary Table 1, 2, and 3). STATA SE version 14.1 (Stata Corp, College Station, TX) was used for all analyses.
Ethics statement
The study was reviewed and approved by the Human Subjects Committee of the Harvard T. H. Chan School of Public Health, the Ethics Committee of the Tohoku University Graduate School of Medicine, the Research Ethics Committee of the Graduate School of Medicine, Chiba University, and the Research Ethics Committee involving Human Participants of the Nihon Fukushi University. Explanations of the study and the self-reported questionnaire were sent by mail to the residents. They were informed that participation was voluntary and that returning the self-administered questionnaire would be interpreted as implying consent.
We followed the STROBE Statement to report our observational study.
Data availability statement
All data used are from the JAGES study. The JAGES data used in this study will be made available upon request, as per NIH data access policies. All enquiries are to be addressed to the data management committee via e-mail: dataadmin.ml@jages.net. All JAGES datasets have ethical or legal restrictions for public deposition due to inclusion of sensitive information from the human participants.
References
Center for Research on the Epidemiology of Disasters. The human cost of natural disasters2015: a global perspective. (Université Catholique de Louvain, 2015).
Nomura, S. et al. Mortality risk amongst nursing home residents evacuated after the Fukushima nuclear accident: a retrospective cohort study. PLoS One 8, e60192, https://doi.org/10.1371/journal.pone.0060192 (2013).
Kelman, J. et al. Dialysis care and death following Hurricane Sandy. Am J Kidney Dis 65, 109–115, https://doi.org/10.1053/j.ajkd.2014.07.005 (2015).
Hayman, K. G., Sharma, D., Wardlow, R. D. & Singh, S. Burden of cardiovascular morbidity and mortality following humanitarian emergencies: a systematic literature review. Prehosp Disaster Med 30, 80–88, https://doi.org/10.1017/s1049023x14001356 (2015).
Edmondson, D. et al. Association of posttraumatic stress disorder and depression with all-cause and cardiovascular disease mortality and hospitalization among Hurricane Katrina survivors with end-stage renal disease. Am J Public Health 103, e130–137, https://doi.org/10.2105/ajph.2012.301146 (2013).
Kolves, K., Kolves, K. E. & De Leo, D. Natural disasters and suicidal behaviours: a systematic literature review. J Affect Disord 146, 1–14, https://doi.org/10.1016/j.jad.2012.07.037 (2013).
Uchimura, M., Kizuki, M., Takano, T., Morita, A. & Seino, K. Impact of the 2011 Great East Japan Earthquake on community health: ecological time series on transient increase in indirect mortality and recovery of health and long-term-care system. J Epidemiol Community Health 68, 874–882, https://doi.org/10.1136/jech-2014-204063 (2014).
Niiyama, M. et al. Population-based incidence of sudden cardiac and unexpected death before and after the 2011 earthquake and tsunami in Iwate, northeast Japan. J Am Heart Assoc 3, e000798, https://doi.org/10.1161/jaha.114.000798 (2014).
Orui, M. et al. Delayed increase in male suicide rates in tsunami disaster-stricken areas following the Great East Japan Earthquake: a three-year follow-up study in Miyagi Prefecture. Tohoku J Exp Med 235, 215–222, https://doi.org/10.1620/tjem.235.215 (2015).
Armenian, H. K., Melkonian, A. K. & Hovanesian, A. P. Long term mortality and morbidity related to degree of damage following the 1998 earthquake in Armenia. Am J Epidemiol 148, 1077–1084 (1998).
North, C. S. & Pfefferbaum, B. Mental health response to community disasters: a systematic review. JAMA 310, 507–518, https://doi.org/10.1001/jama.2013.107799 (2013).
Le, F., Tracy, M., Norris, F. H. & Galea, S. Displacement, county social cohesion, and depression after a large-scale traumatic event. Soc Psychiatry Psychiatr Epidemiol 48, 1729–1741, https://doi.org/10.1007/s00127-013-0698-7 (2013).
Uscher-Pines, L. Health effects of relocation following disaster: a systematic review of the literature. Disasters 33, 1–22, https://doi.org/10.1111/j.1467-7717.2008.01059.x (2009).
Frankenberg, E., Nobles, J. & Sumantri, C. Community Destruction and Traumatic Stress in Post-Tsunami Indonesia. J Health Soc Behav, https://doi.org/10.1177/0022146512456207 (2012).
The United Nations Office for Disaster Risk Reduction. Sendai Framework for Disaster Risk Reduction 2015–2030, http://www.wcdrr.org/preparatory/post2015 (2015).
Chou, Y. J. et al. Who is at risk of death in an earthquake? Am J Epidemiol 160, 688–695, https://doi.org/10.1093/aje/kwh270 (2004).
Nishikiori, N. et al. Who died as a result of the tsunami? Risk factors of mortality among internally displaced persons in Sri Lanka: a retrospective cohort analysis. BMC Public Health 6, https://doi.org/10.1186/1471-2458-6-73 (2006).
Nagata, S. et al. The tsunami’s impact on mortality in a town severely damaged by the 2011 Great East Japan Earthquake. Disasters 38(Suppl 2), S111–122, https://doi.org/10.1111/disa.12072 (2014).
Obrova, J., Sovova, E., Ivanova, K., Taborsky, M. & Loyka, S. Effects of the July 1997 floods in the Czech Republic on cardiac mortality. Disaster Med Public Health Prep 8, 492–496, https://doi.org/10.1017/dmp.2014.111 (2014).
Aldrich, D. P. & Sawada, Y. The physical and social determinants of mortality in the 3.11 tsunami. Soc Sci Med 124, 66–75, https://doi.org/10.1016/j.socscimed.2014.11.025 (2015).
Nateghi, R., Bricker, J. D., Guikema, S. D. & Bessho, A. Statistical Analysis of the Effectiveness of Seawalls and Coastal Forests in Mitigating Tsunami Impacts in Iwate and Miyagi Prefectures. PLoS One 11, e0158375, https://doi.org/10.1371/journal.pone.0158375 (2016).
Frankenberg, E., Gillespie, T., Preston, S., Sikoki, B. & Thomas, D. Mortality, the Family and the Indian Ocean Tsunami. Econ J 121, F162–F182, https://doi.org/10.1111/j.1468-0297.2011.02446.x (2011).
Fergusson, D. M., Horwood, L. J., Boden, J. M. & Mulder, R. T. Impact of a major disaster on the mental health of a well-studied cohort. JAMA Psychiatry 71, 1025–1031, https://doi.org/10.1001/jamapsychiatry.2014.652 (2014).
Arnberg, F. K. et al. Psychiatric disorders and suicide attempts in Swedish survivors of the 2004 southeast Asia tsunami: a 5 year matched cohort study. Lancet Psychiatry, https://doi.org/10.1016/S2215-0366(15)00124-8 (2015).
National Police Agency. Damage of 2011 Great East Japan earthquake and tsunami and police response (in Japanese), https://www.npa.go.jp/news/other/earthquake2011/pdf/higaijokyo.pdf (2017).
Cabinet Office Government of Japan. White Paper on Disaster Management 2011, http://www.bousai.go.jp/kaigirep/hakusho/pdf/WPDM2011_Summary.pdf (2011).
Iwanaga, S. & Matsuura, Y. In Information processing and management of uncertainty: 15th International Conference on Information Processing and Management of Uncertainty in Knowledge-Based Systems, IPMU 2014, Montpellier, France, July 15-19, 2014, Proceedings, part 1 Communications in computer and information science (eds Anne. Laurent, Olivier. Strauss, Bernadette. Bouchon-Meunier, & Ronald R. Yager) 437–446 (Springer, 2014).
Murata, A., Nakamura, T. & Karwowski, W. Influence of Cognitive Biases in Distorting Decision Making and Leading to Critical Unfavorable Incidents. safety 1, 44–58, https://doi.org/10.3390/safety1010044 (2015).
United Nations, Department of Economic and Social Affairs, Statistics Division. in The World’s Women 2015: Trends and Statistics Ch. 7, 163–178 (United Nations, 2015).
Benson, W. F. & Aldrich, N. CDC’s disaster planning goal: Protect vulnerable older adults. (2007).
Tanida, N. What happened to elderly people in the great Hanshin earthquake. BMJ 313, 1133–1135 (1996).
Arnold, J. L. Disaster medicine in the 21st century: future hazards, vulnerabilities, and risk. Prehosp Disaster Med 17, 3–11 (2002).
Rodda, J., Walker, Z. & Carter, J. Depression in older adults. BMJ 343, d5219, https://doi.org/10.1136/bmj.d5219 (2011).
Yamazaki, F., Nishimura, A. & Ueno, Y. Estimation of human casualties due to urban earthquakes. Eleventh World Conference on Earthquake Engineering, 443 (1996). http://www.iitk.ac.in/nicee/wcee/article/11_443.PDF.
Baba, S. et al. The Great Hanshin earthquake. Lancet 347, 307–309 (1996).
Iwaida, K. Recovery of Sendai Airport (in Japanese). Public works management journal 10, 43–48 (2011).
Hikichi, H., Aida, J., Tsuboya, T., Kondo, K. & Kawachi, I. Can Community Social Cohesion Prevent Posttraumatic Stress Disorder in the Aftermath of a Disaster? A Natural Experiment From the 2011 Tohoku Earthquake and Tsunami. Am J Epidemiol 183, 902–910, https://doi.org/10.1093/aje/kwv335 (2016).
Santos-Eggimann, B., Cuenoud, P., Spagnoli, J. & Junod, J. Prevalence of frailty in middle-aged and older community-dwelling Europeans living in 10 countries. J Gerontol A Biol Sci Med Sci 64, 675–681, https://doi.org/10.1093/gerona/glp012 (2009).
Hasegawa, R. Disaster Evacuation from Japan’s 2011 Tsunami Disaster and the Fukushima Nuclear Accident. IDDRI, Study No05 (2013).
Steptoe, A., Shankar, A., Demakakos, P. & Wardle, J. Social isolation, loneliness, and all-cause mortality in older men and women. Proc Natl Acad Sci USA 110, 5797–5801, https://doi.org/10.1073/pnas.1219686110 (2013).
Holt-Lunstad, J., Smith, T. B. & Layton, J. B. Social relationships and mortality risk: a meta-analytic review. PLoS Med 7, e1000316, https://doi.org/10.1371/journal.pmed.1000316 (2010).
Forbes, E. E. fMRI studies of reward processing in adolescent depression. Neuropsychopharmacology 36, 372–373, https://doi.org/10.1038/npp.2010.164 (2011).
Naranjo, C. A., Tremblay, L. K. & Busto, U. E. The role of the brain reward system in depression. Prog Neuropsychopharmacol Biol Psychiatry 25, 781–823 (2001).
Janes, A. C. et al. Reward Responsiveness Varies by Smoking Status in Women with a History of Major Depressive Disorder. Neuropsychopharmacology 40, 1940–1946, https://doi.org/10.1038/npp.2015.43 (2015).
Richard, E. et al. Late-life depression, mild cognitive impairment, and dementia. JAMA Neurol 70, 374–382, https://doi.org/10.1001/jamaneurol.2013.603 (2013).
Bennabi, D., Vandel, P., Papaxanthis, C., Pozzo, T. & Haffen, E. Psychomotor retardation in depression: a systematic review of diagnostic, pathophysiologic, and therapeutic implications. Biomed Res Int 2013, 158746, https://doi.org/10.1155/2013/158746 (2013).
De Raedt, R. & Hooley, J. M. The role of expectancy and proactive control in stress regulation: A neurocognitive framework for regulation expectation. Clin Psychol Rev 45, 45–55, https://doi.org/10.1016/j.cpr.2016.03.005 (2016).
Koyama, S. et al. Social Support Improves Mental Health among the Victims Relocated to Temporary Housing following the Great East Japan Earthquake and Tsunami. Tohoku J Exp Med 234, 241–247, https://doi.org/10.1620/tjem.234.241 (2014).
Hikichi, H. et al. Residential relocation and change in social capital: A natural experiment from the 2011 Great East Japan Earthquake and Tsunami. Sci Adv 3, e1700426, https://doi.org/10.1126/sciadv.1700426 (2017).
Shibui, T. All residents evacuated from the disaster. Why do miracles in ‘Akaikou Marine Home’, nursing home 250 meters from the sea? (in Japanese), http://www.jprime.jp/articles/-/8034 (2016).
Japan Meteorological Agency. Meteorological statistical information (in Japanese), http://www.data.jma.go.jp/kaiyou/data/db/kaikyo/archive/c_1/kaikyo_monthly/2011/03/kaikyo_monthly.html (2011).
Ducharme, M. B. & Lounsbury, D. S. Self-rescue swimming in cold water: the latest advice. Appl Physiol Nutr Metab 32, 799–807, https://doi.org/10.1139/H07-042 (2007).
Weil, F., Lee, M. R. & Shihadeh, E. S. The burdens of social capital: How socially-involved people dealt with stress after Hurricane Katrina. Soc Sci Res 41, 110–119 (2012).
Chamlee-Wright, E. & Storr, V. H. Social capital as collective narratives and post-disaster community recovery. Soc Rev 59, 266–282 (2011).
Aldrich, D. P. The power of people: social capital’s role in recovery from the 1995 Kobe earthquake. Natural Hazards 56, 595–611 (2011).
Aldrich, D. P. & Meyer, M. A. Social Capital and Community Resilience. Am Behav Sci 59, 254–269, https://doi.org/10.1177/0002764214550299 (2015).
Aida, J., Kawachi, I., Subramanian, S. V. & Katsunori, K. In Global Perspectives on Social Capital and Health (eds I. Kawachi, S. Takao, & S. V. Subramanian) Ch. 7, 167–187 (Springer, 2013).
Aldrich, D. P. In Building resilience: social capital in post-disaster recovery 24–53 (The University of Chicago Press, 2012).
Witze, A. Tsunami alerts fall short. Nature 516, 151–152, https://doi.org/10.1038/516151a (2014).
Tsuboya, T. et al. Predictors of depressive symptoms following the Great East Japan earthquake: A prospective study. Soc Sci Med 161, 47–54, https://doi.org/10.1016/j.socscimed.2016.05.026 (2016).
Tani, Y. et al. Childhood socioeconomic disadvantage is associated with lower mortality in older Japanese men: the JAGES cohort study. Int J Epidemiol, https://doi.org/10.1093/ije/dyw146 (2016).
Hikichi, H. et al. Increased risk of dementia in the aftermath of the 2011 Great East Japan Earthquake and Tsunami. Proc Natl Acad Sci USA, https://doi.org/10.1073/pnas.1607793113 (2016).
Takahashi, S. et al. Urgent Survey for 2011 Great East Japan Earthquake and Tsunami Disaster in Ports and Coasts. Technical note of the Port and Airport Research Institute 1231 (2011).
Ministry of Health, Labour and Welfare. Vital statistics of Japan, http://www.mhlw.go.jp/english/database/db-hw/index.html (2015).
Yeh, H. Gender and Age Factors in Tsunami Casualties. Nat Hazards Rev 11, 29–34, https://doi.org/10.1061/(Asce)1527-6988(2010)11:1(29) (2010).
Niino, N., Imaizumi, T. & N, K. A Japanese translation of the Geriatric Depression Scale. Clin Gerontol 10, 85–87 (1991).
Sheikh, J. I. & Yesavage, J. A. In Clinical Gerontology: A Guide to Assessment and Intervention (ed. T. L. Brink) 165–173 (The Haworth Press, Inc., 1986).
Greenberg, S. A. How to try this: the Geriatric Depression Scale: Short Form. Am J Nurs 107, 60–69; quiz 69–70, doi:https://doi.org/10.1097/01.NAJ.0000292204.52313.f3 (2007).
Williams, R. Analyzing Rare Events with Logistic Regression, https://www3.nd.edu/~rwilliam/stats3/RareEvents.pdf (2016).
Lee, K. J. & Carlin, J. B. Multiple imputation for missing data: fully conditional specification versus multivariate normal imputation. Am J Epidemiol 171, 624–632, https://doi.org/10.1093/aje/kwp425 (2010).
Acknowledgements
We appreciate the support and cooperation of the Iwanuma Mayor’s office, and staff of the Department of Health and Welfare, Iwanuma City. This study was supported by a grant of the National Institutes of Health (R01 AG042463), the Strategic Research Foundation Grant-aided Project for Private Universities from the Ministry of Education, Culture, Sport, Science, and Technology, Japan (MEXT), 2009–2013, for the Center for Well-being and Society, Nihon Fukushi University, Grants-in-Aid for Scientific Research (22330172, 22390400, 22390400, 22592327, 23243070, 23590786, 23790710, 24390469, 24530698, 24653150, 24683018, 25253052, 25870573, 25870881, 26285138, 26882010, 15H04781, 15H01972, 16H05556, 16K19267) from the Japan Society for the Promotion of Science. The study was also supported by a Health and Labour Sciences Research Grant, and grants for Comprehensive Research on Aging and Health (H22-Choju-Shitei-008, H24-Junkankitou-Ippan-007, H24-Chikyukibo-Ippan-009, H24-Choju-Wakate-009, H25-Kenki-Wakate-015, H25-Irryo-Shitei-003 (Fukkou), H26-Choju-Ippan-006, H27-Ninchisyou-Ippan-001, H28-Choju-Ippan-002) from the Ministry of Health, Labour and Welfare, Japan, the Research and Development Grants for Longevity Science from AMED (Japan Agency for Medical Research and development), the Personal Health Record (PHR) Utilization Project from AMED, World Health Organization Centre for Health Development (WHO Kobe Centre) (WHO APW 2017/713981), Japan Foundation for Aging and Health Research Support Grant, a grant from The Health Care Science Institute, and also grants from National Center for Geriatrics and Gerontology. The funders had no role in the study design, data collection, and analysis. The views and opinions expressed in this article are those of the authors and do not necessarily reflect the official policy or position of the respective funding organizations.
Author information
Authors and Affiliations
Contributions
J.A. created the analysis plan, analyzed the data, and drafted the manuscript. H.H., T. Ts., Y.M., Y.S., T.Ta., K.O., S.K., S.V.S., and K.K. supervised data collection for the whole study. T. Ta., Y.M., and Y.S. helped the analyses. I.K. conceived the study design and participated in the interpretation of data and manuscript preparation. All of the authors discussed the data and results and critically revised the manuscript. J.A. is the guarantor.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Aida, J., Hikichi, H., Matsuyama, Y. et al. Risk of mortality during and after the 2011 Great East Japan Earthquake and Tsunami among older coastal residents. Sci Rep 7, 16591 (2017). https://doi.org/10.1038/s41598-017-16636-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-16636-3
This article is cited by
-
Impact of Socioeconomic Status and Demographic Composition on Disaster Mortality: Community-Level Analysis for the 2011 Tohoku Tsunami
International Journal of Disaster Risk Science (2022)
-
Preliminary tsunami hazard map for Africa
Arabian Journal of Geosciences (2020)
-
Pre-disaster social support is protective for onset of post-disaster depression: Prospective study from the Great East Japan Earthquake & Tsunami
Scientific Reports (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
