
Abstract
Heat shock protein 27 (HSP27) has been found to be related to tumorigenesis. The aim of this study was to investigate the expression pattern and clinical significance of HSP27 in non-small-cell lung cancer (NSCLC). The expression of HSP27 in tissues was examined by immunohistochemistry and serum level of HSP27 mRNA was detected by real-time PCR. The survival analysis was performed by a Kaplan Meier method and the estimation of risk factors was determined by the multiple regression analysis. The expression of HSP27 was increased in lung cancer tissues (p < 0.001) and serum (p < 0.001) of NSCLC patients and higher HSP27 in lung cancer tissues and serum of NSCLC patients was associated with poorly differentiated cancer (p < 0.001; p = 0.035), lymphatic metastasis (p < 0.001; p < 0.001), advanced TNM stage (p < 0.001; p < 0.001). And the levels of HSP27 in tissues and serum of lung cancer patients had a certain positive correlation (p = 0.046). Moreover, increased HSP27 expression correlated with shorter survival of NSCLC patients (p < 0.001). The results suggest that HSP27 may serve as a potential biomarker for diagnosis and prognosis of NSCLC.
Similar content being viewed by others

Introduction
Lung cancer is the leading cause of cancer-related death in men and women in China accounting for approximately 32% of total cancer deaths in 2015 despite comprising only ~25% of new cancer cases1. Especially, morbidity and mortality of non-small-cell lung cancer (NSCLC) are relatively high in China, with a 5-year survival rate of less than 20%, which is often due to lung cancer first presenting at late stages and a lack of curative therapeutic options at these later stages1. Decades of research have contributed to our understanding that NSCLC is a multi-step process involving genetic and protein alterations which transforms normal lung epithelial cells into lung cancer2. It is commonly understood that an early detection of NSCLC leads to a better chance for reducing the mortality and morbidity. The advent of new and emerging molecular, genetic, and imaging technologies has broadened the possible strategies for early detection and prevention of NSCLC3. Molecular markers are being identified that are enhancing our ability to predict and detect NSCLC before it develops and at the earliest signs of impending carcinogenic transformation4. Thus, new biological markers are urgently needed to improve the early detection, diagnosis and treatment of NSCLC.
The heat shock protein 27 (HSP27), a 27 kDa protein, belongs to the heat shock protein family, which is highly expressed in some tumors and is associated with tumor metastasis, poor prognosis and resistance to chemotherapy5. The heat shock protein family are highly conserved molecular chaperones with indispensable roles in protein homeostasis, transport processes and signal transduction6. Research shows that up-regulation of HSP27 in tumor cells increases tumor cell growth, and thus most probably serves as a protective factor to chemical stress7. Previously, we have identified the up-regulation of HSP27 in NSCLC tissues compared with the normal lung tissues using laser capture microdissection combined with liquid chromatography-tandem mass spectrometry. However, compared with cells, investigating on the HSP27 expression in serum and tissues in NSCLC is still lacking. In this research, we tested the expression levels of HSP27 in tissues and serum of patients with NSCLC, disclosed the relationship between HSP27 and clinical parameters of NSCLC and assessed its value in discerning NSCLC.
Results
NSCLC tissues showed a higher expression of HSP27 than normal tissues
The immunohistochemistry (IHC) method was employed to detect the expression of HSP27 in lung cancer tissues and cancer adjacent normal tissues of 76 NSCLC patients. We found that HSP27 was expressed in the cytoplasm of lung cancer cells and normal cells. Cells that appeared to have brown-yellow granules in the nuclei or cytoplasm were considered to be positive expression (Fig. 1A–H). The statistical results showed that lung cancer tissues showed a higher expression of HSP27 (45/76, 59.2%) than the cancer adjacent normal tissues (18/76, 23.7%) (P < 0.001) (Table 1 and Fig. 2A).

Immunohistochemistry analysis of HSP27 in NSCLC tissues and normal lung tissues (×400). (A) No staining of HSP27 in normal tissues. (B) No staining of HSP27 in well differentiated LAC. (C) Moderate staining of HSP27 in moderately differentiated LAC. (D) Intense staining of HSP27 poorly differentiated LAC. (E) No staining of HSP27 in normal tissues. (F) No staining of HSP27 in well differentiated LSCC. (G) Moderate staining of HSP27 in moderately differentiated LSCC; (H) Intense staining of HSP27 in poorly-differentiated LSCC; NSCLC, non-small cell lung cancer; LAC, lung adenocarcinoma; LSCC, lung squamous cell carcinoma.

Correlation between the expression of HSP27 in tissues and clinicopathologic factors of NSCLC patients. (A) Higher positive expression of HSP27 in NSCLC tissues than in normal tissues. (B) Higher positive expression of HSP27 in LAC tissues than in LSCC tissues. (C) Higher positive expression of HSP27 in poorly differentiated NSCLC tissues than in moderately and well tissues differentiated NSCLC tissues. (D) Higher positive expression of HSP27 in NSCLC tissues at T3-T4 stage than in cancer tissues at T1-T2 stage. (E) NSCLC tissues with lymph node metastasis (N2-N3) revealed higher positive expression of HSP27 than lymph node metastasis (N0-N1). (F) NSCLC tissues at staged IIIB-IV had higher positive expression of HSP27 than those at stages IIA- IIIA; NSCLC, non-small cell lung cancer; LAC, adenocarcinoma of the lung; LSCC, squamous cell carcinoma of the lung; T, the size of the tumor mass; N, node stage (TNM classification).
Increased HSP27 in NSCLC tissues correlated with clinicopathologic factors of NSCLC
As shown in Table 1, HSP27 was highly expressed in lung adenocarcinoma (LAC) (27/38, 71.1%), compared with lung squamous cell carcinoma (LSCC) (18/38, 47.4%) (P = 0.036). Also, poorly differentiated NSCLC tissues (20/25, 80%) showed an elevated HSP27 expression compared with the well differentiated tissues (9/29, 31%) (P < 0.001). In addition, overexpression of HSP27 was observed in NSCLC tissues with T3-T4 (41/53, 77.4%), but not in those of T1-T2 (4/23, 17.4%) (P < 0.001). Moreover, NSCLC tissues with lymph node metastasis (N2-N3) (39/50, 78%) displayed a higher expression of HSP27 than those with lymph node metastasis (N0-N1) (6/26, 23.1%) (P < 0.001). Furthermore, an increase of HSP27 was exhibited in tissues with NSCLC at stage IIIB-IV (33/40, 82.5%), compared with those of stage IIA-IIIA (12/36, 33.3%) (P < 0.001) (Table 1 and Fig. 2B–F). However, the expressions of HSP27 was irrelevant to gender, age and smoking of NSCLC patients.
NSCLC patients presented a higher level of HSP27 mRNA in serum than benign lung disease patients
Serum level of HSP27 mRNA was detected by a method of real-time PCR in a series of 76 NSCLC patients and a series of 38 benign lung disease patients. The results showed that expression level of serum HSP27 mRNA was higher in patients with NSCLC (42.28 ± 14.28, 2−ΔΔCt) than that in benign lung disease patients (23.66 ± 10.93, 2−ΔΔCt) (P < 0.001) (Table 2, Fig. 3A).

Correlation between the serum level of HSP27 mRNA and clinicopathologic factors of lung cancer patients. (A) Increased serum level of HSP27 mRNA in NSCLC patients than in benign lung disease patients. (B) The level of serum HSP27 mRNA did not have a difference between LAC and LSCC patients. (C) Higher level of serum HSP27 mRNA in poorly differentiated NSCLC than in moderately and well tissues differentiated NSCLC. (D) Higher level of serum HSP27 mRNA in NSCLC at T3-T4 stage than at T1-T2 stage. (E) NSCLC patients with lymph node metastasis (N2-N3) revealed a higher level of serum HSP27 mRNA than patients with lymph node metastasis (N0-N1). (F) NSCLC patients at staged IIIB-IV had higher level of serum HSP27 mRNA than those at stages IIA-IIIA; NSCLC, non-small cell lung cancer; LAC, adenocarcinoma of the lung; LSCC, squamous cell carcinoma of the lung; T, the size of the tumor mass; N, node stage (TNM classification).
Increased serum HSP27 mRNA correlated with clinicopathologic factors of NSCLC patients
As shown in Table 2 and Fig. 3B–F, patients with poorly differentiated NSCLC showed an elevated serum level of HSP27 mRNA (45.61 ± 11.30, 2−ΔΔCt) compared with the patients with well differentiated NSCLC (36.94 ± 15.55, 2−ΔΔCt) (P = 0.035). In addition, patients with T3-T4 (46.84 ± 13.5, 2−ΔΔCt) revealed a higher serum level of HSP27 mRNA than those at T1-T2 stage (31.76 ± 9.93, 2−ΔΔCt) (P < 0.001). And patients with N2-N3 of lymph node metastasis (47.36 ± 13.94, 2−ΔΔCt) exhibited an increased serum level of HSP27 mRNA than those with N0-N1 (32.51 ± 8.96, 2−ΔΔCt) (P < 0.001). Furthermore, NSCLC patients at IIIB-IV stage (48.99 ± 14.49, 2−ΔΔCt) displayed a higher serum level of HSP27 mRNA than those at IIA-IIIA stage (34.81 ± 9.72, 2−ΔΔCt) (P < 0.001). But the serum level of HSP27 mRNA did not correlate with gender, age, smoking and histological classification of NSCLC patients.
Expression level of HSP27 protein in tissues was consistent with the expression level of HSP27 mRNA in serum
To verify whether the HSP27 expression in lung cancer tissues is consistent with serum HSP27 mRNA of patients, we performed a non-parametric rank correlation analysis in matched 76 tissues and serum specimens. We divided the serum detection value of HSP27 mRNA into two zones (low and high), which corresponded to the two grades of tissues detection. The statistical analysis showed that the correlation coefficient (spearman rank test) of expression level of HSP27 protein in tissues and the expression level of HSP27 mRNA in serum is 0.697 (P = 0.046), suggesting that tissues HSP27 and serum mRNA in patients with NSCLC had a certain positive correlation (Fig. 4A).

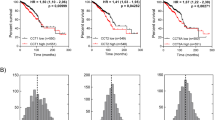
Consistency test of HSP27 expression and Kaplan-Meier survival analysis. (A) HSP27 expression in tissues was consistent with the level of HSP27 mRNA in serum (McNemar test, P = 0.046). (B) Scatter diagram showed that higher expression of HSP27 correlated with early emergence of death in NSCLC; (C) Survival curve showed that positive expression of HSP27 was associated with a shorter post-surgery survival time (P < 0.001).
Higher level of HSP27 expression was related to the shorter survival of NSCLC patients
Through medical follow-up, we got the survival data from the patients. The definition of survival time is as follows: start time = the date of taking tissues samples (the time of surgery); terminating time = the date of patients’ death (or the last date lost to follow-up). A total of 69 out of 76 patients had follow-up records, which were included in survival analysis. The Kaplan-Meier curves analysis showed that patients who displayed a high expression of HSP27 appeared to have a shorter survival after surgery, as compared with patients with low level of HSP27 (P < 0.001) (Fig. 4B and C). In addition, lymph node metastasis (P = 0.037) and advanced TNM stage (P < 0.001) were also shown to be important risk factors which reduced the survival time of NSCLC patients. Cox-Regression analysis provided the final risk function: H(t) = [h0(t)]e(0.922 ×6+1.99 ×8+1.657 ×9) (Table 3).
Threshold value of serum HSP27 mRNA and accuracy analysis for discerning patients with NSCLC
The threshold value of serum HSP27 mRNA for discerning patients with NSCLC from benign lung diseases was determined via ROC curve analysis. The minimum value of HSP27 mRNA was 10 (2−ΔΔCt), which was observed in the benign lung disease group while the maximum was 82.11 (2−ΔΔCt), located in the disease group with NSCLC (Fig. 5A and B). The threshold of serum HSP27 mRNA for distinguishing NSCLC patients from benign lung diseases was defined as 25.4 (2−ΔΔCt), responding a sensitivity of 94.76% and specificity of 81.58% (Table 4). In order to discern NSCLC, the AUC (area under the curve) of serum HSP27 mRNA arrived at 0.884 with 0.0408 of standard error, while 95% CI was from 0.810 to 0.936, and then Z value was 9.401 (P < 0.001) (Fig. 5C).

Diagnostic accuracy of serum HSP27 mRNA for NSCLC. (A) After calculating, the cut-off value (25.4, 2−ΔΔCt) of serum HSP27 mRNA appeared to discern the NSCLC patients from benign lung disease, responding a sensitivity of 94.76% and specificity of 81.58%. (B) The expression of serum HSP27 mRNA in NSCLC group was significantly higher than that in normal group; the minimum value of HSP27 mRNA was 10 (2−ΔΔCt), which was observed in the benign lung disease group while the maximum was 82.11 (2−ΔΔCt), located in the disease group with NSCLC; there were 3 samples in the normal group and 4 samples in the NSCLC group are out of the dispersion. (C) Receiver operating characteristic curves (ROC) of serum HSP27 mRNA for distinguishing NSCLC patients from benign lung disease (AUC = 0.884); ROC, receiver operating characteristic curve; AUC, area under the curve.
Discussion
Lung cancer is the leading cause of cancer death worldwide. Approximately 80% of lung cancers are grouped as NSCLC, which are clinically and pathologically different from small cell lung carcinoma (SCLC)8. Recent advances in lung cancer research have enabled significant progress in our understanding of the molecular pathogenesis and treatment for lung cancer9. These discoveries graphically illustrate that molecular biological findings are directly linked to the development of clinical oncology and contribute to improve the survival rates of patients with lung cancer10. Heat shock protein 27 (HSP27) also known as heat shock protein beta-1 (HSPB1), which is encoded by the HSPB1 gene. HSP27 is an ATP-independent molecular chaperone, is induced by the heat shock associated with physical and chemical stresses, including radiation, oxidative stress, and various chemotherapies. HSP27 has been appeared to be constitutively expressed at high levels in various tumors, including gastric, prostate, and pancreatic cancer11. Study shows that elevated expression of HSP27 in cancers has been associated with poor clinical prognosis and therapeutic resistance and has been suggested as a diagnostic, predictive or prognostic marker in various tumors12. In the current study, we identified the expressions of HSP27 in NSCLC tissues and serum of patients, and analyzed the clinical significance of it expression and the potential use of HSP27 as clinical markers for the diagnosis and prognosis of NSCLC.
We found that whether in lung cancer tissues or in serum of patients, the expression of HSP27 was up-regulated in NSCLC, particularly in poorly differentiated lung cancer. In clinical practice, poorly differentiated lung cancers tend to progress faster and have a poor prognosis than moderately and well differentiated tumors4. Thus, we can infer that high expression of HSP27 is involved in tumorigenesis of NSCLC and potentially promotes NSCLC development. Previous research suggest that over-expression of HSP27 is associated with promoting drug resistance, aggressive cancers, metastasis, and poor patient outcomes and influence cellular processes such as apoptosis, DNA repair, recombination, and formation of metastases13. In the study of NSCLC tissue level, we found that HSP27 expression was significantly higher in lung adenocarcinoma than in squamous cell carcinoma. But, this phenomenon was not verified in the subsequent serological studies. However, this conclusion still has a specific clinical indication that the high expression of HSP27 in NSCLC may be more relevant to lung adenocarcinoma. Some previous studies have shown that HSP27 expression was significantly increased in some different tumors of adenocarcinoma14,15,16. In addition, we found that NSCLC tissues with the lymph node metastasis showed a high expression of HSP27 and the up-regulation of HSP27 intimately correlated with the tumor size positively, which means that overexpression of HSP27 was likely to facilitate the lymphatic metastasis of lung cancer and disease progression. Our studying conclusion is consistent with previous some studies, in which overexpression of HSP27 usually leads to a poor prognosis of patients and is intimately related to the malignant biological characteristics of cancers5,6,7,12,13,14,15. Previous studies also suggest that there is a significant correlation between serum Hsp70 levels and the gross tumor volume of NSCLC17 and serum levels of HSP27 are elevated in patients with NSCLC diagnosed at an early or advanced stage when compared with healthy control groups18. These conclusions suggest that both in lung cancer and in patients with serum, HSP27 expression levels are upregulated, indicating that HSP27 is closely related to the occurrence and development of lung cancer. Invasion and metastasis are the main characteristics during the progression of malignant tumors, which is responsible for the majority of cancer mortalities. Lymph node metastasis is an important prognostic indicator in a number of cancer types. More than half of NSCLC patients have lymph node metastasis when they are initially diagnosed or underwent surgical resection, which results in poor prognosis19,20. Similarly, research reports that tumor size is an independent prognostic factor, for early stage as well as node positive and locally invasive disease, and tumor size had significantly better predictive accuracy than alternative model without tumor size21. Our subsequent serological study also confirmed that increased HSP27 mRNA in serum of NSCLC patients were significantly associated with lymph node metastasis and advanced T stage. The another discovery from our study is also in accordance with previously published investigations, where an up-regulated level of HSP27 in malignant tumors is associated with advanced TNM classification, suggesting that increased expression of HSP27 contributes to the progression and deterioration of NSCLC5,12,16. And it is a clear conclusion that advanced TNM classification predicts a poor outcome and a shorter survival of malignant tumors21. Previous studies find that HSP27 plays an important role in the development of NSCLC through complex upstream and downstream signal control. The tyrosine kinase encoded by the MET oncogene is activated by gene mutation or amplification in tumors. MET kinase inhibition resulted in a 3- to 4-fold increased expression of HSP27. HSP27 increase depended on the inhibition of the MEK/ERK pathway and on heat-shock factor 1 (HSF1) and hypoxia-inducible factor-1α (HIF-1α) regulation22. Transforming growth factor β (TGF-β) signal pathway abnormality is widely observed in drug resistance during lung cancer chemotherapy. TGF-β induces the mRNA and protein expression of HSP27 in human lung cancer cell (A549) and the knockdown of HSP27 blocks TGF-β-induced cisplatin resistance via decreasing cell viability and increasing cell apoptosis in A549 cell23. It is reported that HSP27 is highly expressed in lung cancer tissues from mice, as well as in a lung cancer cell line. In the in vitro model, the overexpression of HSP27 promotes cell proliferation by upregulating specific target genes, which requires the activation of the activator protein-1 (AP-1) signaling pathway following the phosphorylation of c-Jun24. Epithelial to mesenchymal transition (EMT) is induced by transforming growth factor-β1 (TGF-β1) and is a crucial event for cancer cells to acquire invasive and metastatic phenotypes. The silencing of HSP27 enhances an additive effect with TGF-β1-induced EMT and the TGF-β1-induced HSP27 increase is not affected by the suppression of Smad2 and Smad3 in A549 cells, which suggests that HSP27 is involved in TGF-β1-induced EMT in a Smad-independent manner in lung cancer cells25.
A previous meta-analysis suggests that HSP27 expression is significantly associated with the unfavorable conditions for differentiation degree, lymphatic metastasis, clinical stage and tumor size. Meanwhile, HSP27 expression seems to be a predictor for a lower 5-year overall survival (OS) rate but not for 1-year OS of NSCLC26. Our findings are consistent with the conclusion of the meta-analysis. To analyze the prognostic impact of HSP27 overexpression on the survival of NSCLC patients, we also performed a multifactor retrospective analysis. We found that the overexpression of HSP27 appeared to be an important independent risk factor correlated with poor prognosis of NSCLC patients, which suggests that the NSCLC patients with higher expression of HSP27 (24.3± 5.7 months) have a shorter survival time compared with patients with the low expression of HSP27 (42.4 ± 9.3 months) (risk coefficient = 1.657). In addition to HSP27, the other two variables were also introduced into the regression equation: lymph node metastasis and advanced TNM stage. The final risk function was H(t) = [h0(t)]e(0.922 ×6+1.99 ×8+1.657 ×9), suggesting that these factors all affect the outcome of NSCLC patients and their risk coefficients were reached at 0.922 and 1.99 respectively. As we all know, once lymph node metastasis and distant metastasis take place, the survival time of patient with malignant tumors will be remarkably shortened, and will also lead to a great adverse to the treatment27. Through our results, it is suggested that HSP27 can be used as a new tumor marker to evaluate the prognosis of NSCLC. Many studies have shown that HSP27 overexpression correlates with cell proliferation, motility and metastasis of malignant tumors; however, anti-HSP27 treatment has shown to be effective in suppressing the growth and migration of cancer cells6,12,13,28. These results indicate that HSP27 may serve as a valid prognostic marker and therapeutic target for NSCLC. And the characterization of HSP27 expression in NSCLC will conduce to clarify a new molecular pathway on the tumourigenesis and progression of NSCLC and may lead to the development of molecular diagnostic tool and target-specific therapy for NSCLC.
Because this study also involved serological test of HSP27, we analyzed whether serum HSP27 mRNA can discern NSCLC patients from normal individuals. The results showed that the serum HSP27 mRNA had an ideal ability for discerning NSCLC with a sensitivity of 94.76% and specificity of 81.58%, indicating that it can be a useful biomarker for NSCLC diagnosis. We calculated the threshold value of serum HSP27 mRNA through drawing the ROC curve, which showed HSP27 mRNA is conduce to discern the NSCLC. Using an univariate logistic regression models including healthy subjects and patients with NSCLC, previous study finds that HSP27 shows an AUC of 0.870 (P < 0.0001) and suggests that serum HSP27 levels might serve as a possible tool to discriminate between early and advanced stages NSCLC18. So far, a number of studies are concordant with the notion that HSP27 expression is up-regulated in a variety of human cancers, and may be served as effective prognostic and diagnostic indicators for cancer patients5,6,7,12,13,14,15. However, multi-center and large sample of clinical studies still need to be done before serum HSP27 could be used to conduct the diagnosis and treatment of lung cancer in clinical practice.
Yet, there are some deficiencies in this study. Firstly, because experimental specimens on tissue levels were mainly gotten from the surgical resection, this may lead to a selection bias of patients. Secondly, the number of study samples was relatively small, thus a larger number of samples should be required to get a more definitive conclusion. Thirdly, we did not study the molecular signal mechanism on the relationship between the HSP27 and NSCLC. Hence, mechanism research via RNA interference and HSP27 antibody neutralization need to be done for elucidating the role of HSP27 in NSCLC.
Conclusions
We found that the expression of HSP27 was increased in lung cancer tissues and serum of NSCLC patients and that elevated HSP27 in NSCLC was associated with poorly differentiated cancer, lymphatic metastasis and advanced TNM stage. In addition, higher expression of HSP27 correlated with the shorter survival of patients with NSCLC. These results indicated that overexpression of HSP27 was potentially involved in the aggression and prognosis of lung cancer and that HSP27 may serve as a potential biomarker for diagnosis and prognosis of NSCLC.
Methods and Materials
Patient population
From January 2011 to December 2012, a total 76 confirmed patients with NSCLC were recruited in the study (Jining NO.1 People’s Hospital, Jining City, Shandong Province), including 38 patients with LSCC and 38 patients with LAC. We collected the matched fresh lung cancer tissues and normal adjacent tissues in surgery operation. The serum specimens of patients were gathered before receiving chemotherapy and surgery. Over the same period, the serum samples of 38 benign lung disease patients were gathered as control (59 ± 6.5 years) from the hospital mentioned above, including acute infectious diseases, chronic obstructive pulmonary disease, tuberculosis and interstitial diseases. Table 5 lists the clinical features of patients.
All samples were collected in accordance with the ethical guidelines, written informed consent was received. All patients were approached based on approved ethical guidelines, and those who agreed to participate in this study were required to sign consent forms. All the patients signed the informed consent before including the study. The study was approved by Research Ethics Committee of Jining NO.1 People’s Hospital (Jining City, Shandong Province). We confirmed that all methods were performed in accordance with the relevant guidelines and regulations.
Pathological studies and tissue microarray (TMA) construction
Tissue microarray (TMA) blocks were prepared using lung cancer tissue and adjacent normal tissue from 76 lung cancer patients according to the method published previously23. The TMAs were constructed with a tissue array instrument (Beecher Instruments, Manual Tissue Arrayer, USA) by removal of a tissue core from the donor block using a thin-walled needle with an inner diameter of approximately 2.0 mm. Two core samples of each tumor were precisely placed into a recipient block at specifically assigned locations. Adjacent normal tissues were used as the control, which were also placed into the same recipient block. The array block was sectioned and leveled on the microscope slide and then baked in an oven and finally tested with routine H&E staining and IHC.
Immunohistochemistry (IHC)
The expression of HSP27 in lung cancer tissues and adjacent normal tissues was tested by IHC method (Kit of Ultra-sensitive S-P; Fuzhou Maixin biotechnology company, China) according to a previous method that was described in published article23. The best dilution of anti-human HSP27 antibody is 1:100. The positive staining slice of pancreatic cancer served as a positive control; PBS was used instead of the primary antibody as the negative control. We evaluated the immunostaining of HSP27 according to a previous method described2. Cells that appeared to have brown-yellow granules in the nuclei or cytoplasm were considered to be positive cells. The staining was scored separately as follows: 0 for no staining in tumour cells; 1 for moderate staining; and 2 for intense staining of more than 75% of tumour cells; >1 was considered to be a positive result. Upon differences in scoring, the sections were evaluated in conjunction with the two pathologists.
Real-time PCR
The vein blood of 2 mL was collected from each patient. The blood was centrifugated at 1,000 rpm at 4 °C for 5 min for three times. The serum was extracted and stored in ultra low temperature refrigerator at −80 °C. We used the silica gel column, ordinary trizol and strengthened silica gel column method to extract total RNA of serum, and evaluated the extraction efficiency. Then, we detected the target gene by reverse transcription and real-time PCR method. The conditions of amplification: pre-incubation at 94 °C for 6 min; 38 cycles at 95 °C for 5 s; 7 °C for 45 s; and 72 °C for 30 s. We analysed the quantity of mRNA using the 2−ΔΔCt method. The GAPDH gene was served as the internal control. We designed the primer sequences of mRNA for detection molecular targets, housekeeper gene GAPDH: forward 5′-AACATCATCCCTGCCTCTACTG-3′; reverse 5′-CTCCGACGCCTGCTTCACC-3′; target gene HSP27: forward 5′-AAGGATGGCGTGGTGGAGATC-3′; reverse 5′-TCGTTGGACTGCGTGGCTAG-3′. We drew the dissolution curve by Bio-Rad iQ5, export dissolution curve and the Ct values (threshold value). Finally, we calculated the 2−ΔΔCt values and analyzed the real time quantitative results.
Statistical analysis
We used the Chi-square test, Fisher’s exact, and McNemar test to determine the association between the HSP27 expression and clinicopathological parameters of NSCLC. The expression level of serum HSP27 in different groups was compared using the Student’s T-test (matched samples), One-WAY ANOVA (single factor analysis), Kruskal Wallis Test (nonparametric analysis) and non-parametric rank correlation analysis. Survival curves derived from the Kaplan-Meier method were employed to disclose the risk of HSP27 expression to the survival of lung cancer patients. Cox proportional hazard regression model was utilized to determine the influence of each variable on the survival of lung cancer patients. We used the SPSS 17.0 software (SPSS, Chicago, IL, USA) to implement the statistical analyses. To assess the diagnostic potential of HSP27 in serum for lung cancer, we performed the receiver operator characteristic curve (ROC) analysis. All tests of statistical significance were two-sided, and a P-value < 0.05 was considered as statistically significant.
References
Siegel, R. L., Miller, K. D. & Jemal, A. Cancer statistics, 2016. CA Cancer J Clin 66, 7–30, https://doi.org/10.3322/caac.21332 (2016).
Biaoxue, R. et al. Decreased expression of decorin andp57(KIP2) correlates with poor survival and lymphatic metastasis in lung cancer patients. Int J Biol Markers 26, 9–21 (2011).
Fong, K. M. & Minna, J. D. Molecular biology of lung cancer: clinical implications. Clin Chest Med 23, 83–101 (2002).
Biaoxue, R., Hua, L., Tian, F. & Wenlong, G. Increased stathmin in serum as a potential tumor marker for lung adenocarcinoma. Jpn J Clin Oncol, 1–8, https://doi.org/10.1093/jjco/hyx005 (2017).
Konda, J. D., Olivero, M., Musiani, D., Lamba, S. & Di Renzo, M. F. Heat Shock protein 27 (HSP27, HSPB1) is synthetic lethal to cells with oncogenic activation of MET, EGFR and BRAF. Mol Oncol, https://doi.org/10.1002/1878-0261.12042 (2017).
Vahid, S., Thaper, D., Gibson, K. F., Bishop, J. L. & Zoubeidi, A. Molecular chaperone Hsp27 regulates the Hippo tumor suppressor pathway in cancer. Sci Rep 6, 31842, https://doi.org/10.1038/srep31842 (2016).
Owen, S. et al. Heat shock protein 27 is a potential indicator for response to YangZheng XiaoJi and chemotherapy agents in cancer cells. Int J Oncol 49, 1839–1847, https://doi.org/10.3892/ijo.2016.3685 (2016).
Inamura, K. & Ishikawa, Y. Lung cancer progression and metastasis from the prognostic point of view. Clin Exp Metastasis 27, 389–397, https://doi.org/10.1007/s10585-010-9313-4 (2010).
Yatabe, Y. & Shibata, N. Molecular diagnosis of lung cancer in association with treatment of choice. Rinsho Byori 60, 786–795 (2012).
Toyooka, S. et al. Molecular oncology of lung cancer. Gen Thorac Cardiovasc Surg 59, 527–537, https://doi.org/10.1007/s11748-010-0743-3 (2011).
Okuno, M., Adachi, S., Kozawa, O., Shimizu, M. & Yasuda, I. The Clinical Significance of Phosphorylated Heat Shock Protein 27 (HSPB1) in Pancreatic Cancer. Int J Mol Sci 17, https://doi.org/10.3390/ijms17010137 (2016).
Hayashi, N. et al. Hsp27 silencing coordinately inhibits proliferation and promotes Fas-induced apoptosis by regulating the PEA-15 molecular switch. Cell Death Differ 19, 990–1002, https://doi.org/10.1038/cdd.2011.184 (2012).
Heinrich, J. C. et al. New HSP27 inhibitors efficiently suppress drug resistance development in cancer cells. Oncotarget 7, 68156–68169, https://doi.org/10.18632/oncotarget.11905 (2016).
Tsiaousidou, A. et al. B7H4, HSP27 and DJ-1 molecular markers as prognostic factors in pancreatic cancer. Pancreatology 13, 564–569, https://doi.org/10.1016/j.pan.2013.10.005 (2013).
Slotta-Huspenina, J. et al. Evidence of prognostic relevant expression profiles of heat-shock proteins and glucose-regulated proteins in oesophageal adenocarcinomas. PLoS One 7, e41420, https://doi.org/10.1371/journal.pone.0041420 (2012).
Stope, M. B. et al. Effect of the heat shock protein HSP27 on androgen receptor expression and function in prostate cancer cells. World J Urol 30, 327–331, https://doi.org/10.1007/s00345-012-0843-z (2012).
Gunther, S. et al. Correlation of Hsp70 Serum Levels with Gross Tumor Volume and Composition of Lymphocyte Subpopulations in Patients with Squamous Cell and Adeno Non-Small Cell Lung Cancer. Front Immunol 6, 556, https://doi.org/10.3389/fimmu.2015.00556 (2015).
Zimmermann, M. et al. Discrimination of clinical stages in non-small cell lung cancer patients by serum HSP27 and HSP70: a multi-institutional case-control study. Clin Chim Acta 413, 1115–1120, https://doi.org/10.1016/j.cca.2012.03.008 (2012).
Li, J. et al. Association between VEGFR-3 expression and lymph node metastasis in non-small-cell lung cancer. Exp Ther Med 9, 389–394, https://doi.org/10.3892/etm.2014.2091 (2015).
Biaoxue, R. et al. Increased level of Hsp90-beta in bronchoalveolar lavage fluid correlates with lymphatic invasion and advanced stage of lung cancer patients. Am J Transl Res 8, 4147–4159 (2016).
Zhang, J. et al. Relationship between tumor size and survival in non-small-cell lung cancer (NSCLC): an analysis of the surveillance, epidemiology, and end results (SEER) registry. J Thorac Oncol 10, 682–690, https://doi.org/10.1097/jto.0000000000000456 (2015).
Musiani, D. et al. Heat-shock protein 27 (HSP27, HSPB1) is up-regulated by MET kinase inhibitors and confers resistance to MET-targeted therapy. FASEB J 28, 4055–4067, https://doi.org/10.1096/fj.13-247924 (2014).
Huang, Z. et al. Heat Shock Protein 27, a Novel Regulator of Transforming Growth Factor beta Induced Resistance to Cisplatin in A549 Cell. Pharmacology 100, 283–291, https://doi.org/10.1159/000479320 (2017).
Zhang, S. et al. Heat shock protein 27 promotes cell proliferation through activator protein-1 in lung cancer. Oncol Lett 9, 2572–2576, https://doi.org/10.3892/ol.2015.3073 (2015).
Mizutani, H. et al. HSP27 modulates epithelial to mesenchymal transition of lung cancer cells in a Smad-independent manner. Oncol Lett 1, 1011–1016, https://doi.org/10.3892/ol.2010.190 (2010).
Li, S., Zhang, W., Fan, J., Lai, Y. & Che, G. Clinicopathological and prognostic significance of heat shock protein 27 (HSP27) expression in non-small cell lung cancer: a systematic review and meta-analysis. Springerplus 5, 1165, https://doi.org/10.1186/s40064-016-2827-8 (2016).
Baiocchi, G. L. et al. Distant nodal metastasis: is it always an unresectable disease? Transl Gastroenterol Hepatol 2, 1, https://doi.org/10.21037/tgh.2016.12.01 (2017).
Hendriks, L. E. & Dingemans, A. C. Heat shock protein antagonists in early stage clinical trials for NSCLC. Expert Opin Investig Drugs, 1–10, https://doi.org/10.1080/13543784.2017.1302428 (2017).
Acknowledgements
This work was supported by Jining science and Technology Bureau of Shandong Province Funded Projects (No. JN1211). We wish to thank Dr. Wenlong Gao for their helpful discussions and statistical assistance provided during the preparation of this manuscript and also wish to thank all authors of references.
Author information
Authors and Affiliations
Contributions
BW Sheng, CC Qi, B. Liu participated in the design and coordination of the study, carried out the critical experiments, Y. Lin, T. Fu & QD Zeng performed the statistical analysis of studies and wrote the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Sheng, B., Qi, C., Liu, B. et al. Increased HSP27 correlates with malignant biological behavior of non-small cell lung cancer and predicts patient’s survival. Sci Rep 7, 13807 (2017). https://doi.org/10.1038/s41598-017-13956-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-13956-2
This article is cited by
-
Comparative proteomics analysis in different stages of urothelial bladder cancer for identification of potential biomarkers: highlighted role for antioxidant activity
Clinical Proteomics (2023)
-
DHA inhibits invasion and metastasis in NSCLC cells by interfering with CCL18/STAT3 signaling pathway
Clinical and Experimental Medicine (2022)
-
Roles of ferroptosis in urologic malignancies
Cancer Cell International (2021)
-
Targets for protection and mitigation of radiation injury
Cellular and Molecular Life Sciences (2020)
-
Global profiling of O-GlcNAcylated and/or phosphorylated proteins in hepatoblastoma
Signal Transduction and Targeted Therapy (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
