
Abstract
Serum biomarker levels are associated with the risk of complex diseases. Here, we aimed to gain insights into the genetic architecture of biomarker traits which can reflect health status. We performed genome-wide association analyses for twenty serum biomarkers involved in organ function and reproductive health. 9,961 individuals from the UK Household Longitudinal Study were genotyped using the Illumina HumanCoreExome array and variants imputed to the 1000 Genomes Project and UK10K haplotypes. We establish a polygenic heritability for all biomarkers, confirm associations of fifty-four established loci, and identify five novel, replicating associations at genome-wide significance. A low-frequency variant, rs28929474, (beta = 0.04, P = 2 × 10−10) was associated with levels of alanine transaminase, an indicator of liver damage. The variant is located in the gene encoding serine protease inhibitor, low levels of which are associated with alpha-1 antitrypsin deficiency which leads to liver disease. We identified novel associations (rs78900934, beta = 0.05, P = 6 × 10−12; rs2911280, beta = 0.09, P = 6 × 10−10) for dihydroepiandrosterone sulphate, a precursor to major sex-hormones, and for glycated haemoglobin (rs12819124, beta = −0.03, P = 4 × 10−9; rs761772, beta = 0.05, P = 5 × 10−9). rs12819124 is nominally associated with risk of type 2 diabetes. Our study offers insights into the genetic architecture of well-known and less well-studied biomarkers.
Similar content being viewed by others


Introduction
Serum biomarker levels are associated with the risk of complex diseases and are therefore increasingly used in clinical practice to assist with diagnosis, status monitoring and disease management. Well-known examples include the measurement of lipid levels in the context of cardiovascular disease or liver enzymes and albumin to assess liver function.
Serum biomarker levels have a polygenic basis. As demonstrated in the case of lipids, identifying genetic associations can provide new insights into disease aetiology which can in turn guide drug discovery and be useful for diagnosis and risk stratification1,2,3. However, the genetic architecture of most health-related biomarkers has not been studied as extensively as for lipids. Alleles identified to be associated with protein biomarkers to date are predominantly common (minor allele frequency (MAF) >5%). This is primarily driven by genotyping technology and composition of arrays or imputation reference panels used to date4,5,6. Systematically evaluating the association of low frequency and rare variants can provide new insights regarding the genetic architecture of protein biomarkers.
The importance of studying the joint impact of genetic and non-genetic factors on health has been recognised by the UK Household Longitudinal Study (UKHLS, www.understandingsociety.ac.uk), also known as Understanding Society. Involving a total of 40,000 households representative of the UK population, UKHLS is the largest panel survey in the world to support social research. A wide range of social, economic, environment, behavioural, attitudinal, physiological and biomedical variables, including a large panel of the most commonly used clinical biomarkers, have been measured for a representative selection of the sample. This study represents a large sample with very homogenous biomarker measurements, in which recruitment and processing have been carried out consistently and following strict protocols.
Here we describe genome-wide investigation of associations with 20 biomarkers relevant to blood clot formation (fibrinogen), diabetic status (glycated haemoglobin [HbA1c]), insulin-like growth factor 1 [IGF-1]), inflammation (C-reactive protein [CRP]), iron homeostasis (ferritin, haemoglobin), lipid metabolism (HDL-, LDL- and total cholesterol, triglycerides), liver function (alanine and aspartate transaminase, alkaline phosphatase, gamma glutamyl transferase [GGT]), liver and kidney function (albumin, creatinine, eGFR, urea), and reproductive health (dihydroepiandrosterone sulphate [DHEAS], testosterone) in 9,961 individuals from UKHLS. We also leverage the homogeneity of the sample and its size to estimate the narrow sense heritability which has not yet been quantified for many of these biomarkers.
Results
Imputation and genomic coverage
After quality control, genotype data for 525,314 variants were available for 9,961 individuals (Table 1). Following imputation based on the combined reference panel of UK10K and 1000 Genomes Project phase 3, we analysed 23,756,480 variants with imputation accuracy >0.4. Of those, 14,364,872 were rare (MAF <1%, minor allele count (MAC) >10) (2,237,400 of which had imputation accuracy >0.9), 2,732,394 low-frequency (1%≤ MAF <5%) and 6,659,214 common (MAF ≥5%).
Heritability and genetic overlap analyses
For all biomarkers except overall and LDL-cholesterol, alanine transaminase and ferritin there was significant (p < 3.6 × 10−3) evidence for a heritable polygenic component (Table 2). Alkaline phosphatase and testosterone had the highest array heritability estimates with h2 = 27.7% (standard error (SE): 0.040) and h2 = 27.1% (SE: 0.084), respectively. Creatinine, GGT, HbA1c, HDL, IGF1, and triglycerides all had estimates larger than 0.20 while the lowest estimate was observed for ferritin (h2 = 6.1%, SE: 0.037). We found statistically significant (p < 5.5 × 10−4) evidence of genome-wide pleiotropy between different biomarkers (Fig. 1). There was genetic correlation between lipid biomarkers: triglyceride and HDL-cholesterol levels (genetic correlation rg = −0.67, p = 9.9 × 10−18). Triglyceride levels were also inversely genetically linked with DHEAS (rg = −0.53 p = 4.0 × 10−4). The genetic correlation between two markers of inflammation, C-reactive protein and fibrinogen, was also significant (rg = 0.60 p = 3.2 × 10−8). Finally, the genetic factors for creatinine and urea were positively correlated (rg = 0.56 p = 1.2 × 10−5).

Genetic correlations between different biomarker levels. Colour-coding indicates the strength of the correlations. The lower triangle uses only the red color-coding to make it easier to compare the strength of all correlations. Stars indicate statistically significant associations. Albumin: alb, Alkaline Phosphatase: alkp, Alanine Transaminase: alt, Aspartate Transaminase: ast, Fibrinogen: cfib, Total Cholesterol: chol, LDL cholesterol: ldl, Dihydroepiandrosterone Sulphate: dheas, Creatinine: ecre, Gamma Glutamyl Transferase: ggt, Glycated haemoglobin: hba1c, HDL cholesterol: hdl, Haemoglobin: hgb, C-Reactive Protein: hscrp, Insulin-like growth factor 1: igfi, Ferritin: rtin, Testosterone: testo, Triglycerides: trig, Urea: ure.
Genome-wide association analyses
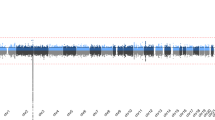
The genome-wide significance threshold of P < 3.56 × 10−9 for this study was derived by taking the conventional genome-wide significance threshold (P < 5 × 10−8) divided by the effective number of independent traits analysed (N = 14.05, details in Methods). Across fifteen biomarkers, we observed associations of 54 previously reported loci at this threshold (Fig. 2). This includes a low frequency variant, rs148685782 at 4q31 in the fibrinogen gamma chain gene (weighted effect allele frequency [WEAF] = 0.4%, beta[SE] = −0.18[0.02], P = 4.0 × 10−21), associated with levels of fibrinogen, a glycoprotein that assists in the blood clot formation. This variant is a missense mutation and has been previously reported to be associated with fibrinogen levels7 as well as with hypofibrinogenemia and haemorrhage8,9,10.

Scatter plot of effect size by frequency of genome-wide significant variants. Effect sizes and 95% confidence intervals (absolute value of beta, expressed in standard deviation units) as a function of minor allele frequencies (MAF), based on the discovery stage of this study. Novel variants (Table 1) are displayed as diamonds, whilst known variants that reach genome-wide significance (P<3.56 × 10-9, two-sided) in the discovery stages are display as circles. Alkaline Phosphatase: alkp, Alanine Transaminase: alt, Fibrinogen: cfib, Total Cholesterol: chol, LDL cholesterol: ldl, Dihydroepiandrosterone Sulphate: dheas, Gamma Glutamyl Transferase: ggt, Glycated haemoglobin: hba1c, HDL cholesterol: hdl, Haemoglobin: hgb, C-Reactive Protein: hscrp, Insulin-like growth factor 1: igfi, Ferritin: rtin, Testosterone: testo_m, Triglycerides: trig.
From the discovery phase we carried forward 573 independent (pairwise r2 < 0.01) variants that were associated with biomarker levels at P < 1 × 10−5 and were located more than 500 kb away from any known index variant for the respective biomarker. Using data from up to 25,897 samples from 4 independent studies (Supplementary Table S1), five loci provided evidence of replication and reached P < 3.6 × 10−9 for the combined analysis of discovery and replication data (Table 3).
rs28929474 at 14q32 (WEAF = 2%, beta[SE] = 0.04[0.01], P = 1.7 × 10−10), a low-frequency variant associated with alanine transaminase (ALT), resides in the serpin family A member 1 (SERPINA1) gene (Figs 3 A and 4). SERPINA1 encodes alpha-1-antitrypsin (AAT), which is a serine protease inhibitor produced in the liver11. Low levels of this protein are the hallmark of a genetic disorder called alpha-1 antitrypsin deficiency (A1AD), which leads to liver disease12.

Regional association plots of novel genome-wide significant loci. Panel A–E : Regional association plots for replicating lead variants for alanine transaminase (A), DHEAS (B,C), HbA1c (D,E) respectively. Pairwise LD (r2) with the index variant is indicated following a color-coded scale. Both the p-values for the discovery as well as the combined discovery + replication are plotted for the index variant, results for all other variants were based on discovery-only data.

Power calculations. Power calculations for individual variants selected for replication per trait, number of samples needed to reach 80% power to reach genome-wide significance (P<3.56 × 10−9, two-sided). The size of the circles represents the relative effect size (standardised) compared amongst all traits.
We identified two novel replicating associations for DHEAS (Fig. 3B,C). DHEAS is the sulphated form of DHEA, a precursor to major sex-hormones such as testosterone and oestrogen, and is synthesized in the adrenal glands. It is an important marker of adrenal gland function. rs78900934 at chromosome 1p21 (WEAF = 30.9%, beta[SE] = 0.05[0.01], P = 5.9 × 10−12) is located 1 kb upstream of a pseudogene, peptidylprolyl isomerase A pseudogene 7 (PPIAP7). This gene shows a high degree of similarity to cyclophilin A (PPIA), the product of which is involved in a number of biological processes including signal transduction13, inflammation14 and apoptosis15. At the second novel locus associated with DHEAS the index variant, rs2911280 at 16q13 (WEAF = 7.5%, beta[SE] = 0.09[0.01], P = 6.0 × 10−10), is located in an intron of the gene encoding c-Maf inducing protein (CMIP), thought to play a role in the T-cell signalling pathway.16
Two novel replicating associations with HbA1c levels were identified (Fig. 3D,E). HbA1c represents the three-month average plasma glucose concentration and is used to diagnose as well as manage type 2 diabetes. The index variant at 12q13, rs12819124 (WEAF = 46.7%, beta[SE] = −0.03[0.01], P = 4.2 × 10−9) lies in an intron of RP1-228P16.4, a long non-coding RNA. The index variant of the second novel locus, rs761772 at 17q25 (WEAF = 12.4%, beta[SE] = 0.05[0.01], P = 4.9 × 10−9), lies within a non-coding exon in the transmembrane channel-like 6 (TMC6) gene and has been shown to affect the expression of TMC6, as well as TNRC6C antisense RNA 1 (TNRC6C-AS1) and transmembrane channel like 8 (TMC8), in cardiac, thyroid, and vascular tissue, as well as whole blood in the GTEx database17.
Discussion
We identify five new biomarker loci, across common and low frequency variants, associated with DHEAS, HbA1c and ALT. We demonstrate polygenic heritability of the majority of biomarkers included in this study and observe large differences in their polygenic component. To our knowledge this is the first report of SNP-based heritability estimates for DHEAS, insulin-like growth factor 1, testosterone and urea. The large sample set with homogeneous biomarker measurements afforded by UKHLS enables reliable estimation for this population. We also identify genetic correlations between several of the biomarkers. Genetic correlation between two traits is an indicator of shared genetic factors and consequently genome-wide pleiotropy. The patterns of heritability and genetic correlations we observe for lipid biomarkers are consistent with previous reports in independent samples18. For total and LDL cholesterol, the SNP-based heritability is less than 10% whilst for HDL it is higher at 23.2%. All these estimates represent a lower bound for the narrow sense heritability. Our estimate of the negative genetic correlation between levels of HDL-cholesterol with triglycerides of rg = −0.67 is similar to the estimate derived from an independent study (rg = −0.61)19. High levels of triglycerides are mechanistically related to low levels of HDL20, 21, which could explain the reverse influence of the shared genetic factors on the biomarkers. We show for the first time that polygenic factors for triglyceride are also negatively correlated with DHEAS. There is a statistically significant genetic correlation between CRP and fibrinogen levels, which could be due to shared inflammation pathways. Finally, the genetic correlation we observe between creatinine and urea is a previously unreported and highly biologically plausible finding as both markers are increased in blood when glomerular filtration rate declines, reflecting impaired kidney function. Characterising the genetic architecture of health-related biomarkers in this way is informative with respect to their biology as well as the design of future association studies. While each known locus individually explains only a small proportion of the variance in biomarker levels, these analyses demonstrate that the joint effect of many variants can be much larger.
We examined less-well studied health-related biomarkers in addition to routine blood measures used in clinical practice. This made it possible to identify novel associations of common and low frequency variants with DHEAS, HbA1c and ALT. These associations could provide novel biological insights. rs2911280, which we found to be associated with DHEAS, is located in an intron of the gene encoding c-Maf inducing protein (CMIP). CMIP is a highly pleiotropic gene, and is associated with several metabolic traits such as adiponectin and HDL cholesterol levels. Cholesterol is a precursor of DHEA in its synthesis process22.
rs28929474 at 14q32 is associated with levels of ALT, which is used in clinical practice to assess liver damage. This variant is located in SERPINA1, encoding the serine protease inhibitor alpha-1-antitrypsin (AAT), which is largely produced in the liver. Associations of variants in this gene were previously found for cortisol23 and height24. Mutations of this gene can cause alpha-1 antitrypsin deficiency (A1AD) which can lead to an accumulation of aberrant proteins in hepatocytes causing liver damage25. This in turn may elevate levels of ALT, warranting future assessment of the association between this signal and liver-related clinical endpoints.
We identify two novel associations with HbA1c levels. In a lookup using published data from an independent large-scale meta-analysis by the MAGIC consortium26, rs12819124 was associated with HbA1c levels with P = 1.8 × 10−6. The direction of effect was consistent with our findings. rs12819124 was also nominally associated with risk of type 2 diabetes at P = 0.025 using data from the DIAGRAM study27. Moreover, association results from published cohorts suggest a possible pleiotropic association with mental disorders and wellbeing (P = 9.0 × 10−6 for bipolar disorder and schizophrenia28, P = 6.4 × 10−5 for subjective wellbeing29). No HbA1c association results were available for rs761772 in MAGIC. For a proxy SNP, rs429216 (r2 = 0.75), the p-value for the association with HbA1c was in the same direction and reached P = 2.7 × 10−3.
The UKHLS sample size is modest compared to some of the previous large-scale GWAS meta-analysis efforts (e.g., >45,000 individuals for HbA1c levels26). The relative gain in power leading to novel locus identification in this study can be attributed to several factors. Two of the newly reported signals have relatively low allele frequency (2% and 7.5%, respectively). These were captured here through use of the Illumina HumanCoreExome array and imputation to a comprehensive reference panel consisting of 1000 Genomes combined with the UK10K haplotypes30. A further power advantage was afforded by the homogeneous measurement of biomarkers in UKHLS and in two of the replication studies. Each biomarker was measured using the same assay for each sample, and processed on the same machine, avoiding loss of information due to diverse biomarker assays with different sensitivity, dynamic range and detection limit, potentially leading to power reductions31.
Larger-scale homogeneous studies and synthesis in massive-scale meta-analyses will help further elucidate the genetic architecture of medically-relevant biomarker traits. Insights into the genetic determinants of population variation in biomarker levels can help us to understand basic processes involved in maintaining health.
Methods
Ethics
Participants gave informed written consent for their blood to be taken and stored for future scientific analysis. The UKHLS has been approved by the University of Essex Ethics Committee and the nurse data collection by the National Research Ethics Service (10/H0604/2).
Study population
The United Kingdom Household Longitudinal Study, also known as Understanding Society (https://www.understandingsociety.ac.uk) is a longitudinal panel survey of 40,000 UK households from England, Scotland, Wales and Northern Ireland). Participants are surveyed annually since 2009 and contribute information relating to their socioeconomic circumstances, attitudes, and behaviours via a computer assisted interview. As recruitment was household based, the study contains related individuals. The study includes phenotypical data for a representative sample of participants for a wide range of social and economic indicators as well as a biological sample collection encompassing biometric, physiological, biochemical, and haematological measurements and self-reported medical history and medication use (https://www.understandingsociety.ac.uk/d/100/7251_User_Guide_Health_Assmt_w2_w3.pdf?1392855567). For each participant non-fasting blood samples were collected through venepuncture, were centrifuged to separate plasma and serum, aliquoted and frozen at −80 °C. DNA has been extracted and stored for genetic analyses.
For replication, data were available for 5533 individuals from ELSA32, 9888 from Fenland33 (Supplemental Table 1), 7621 from HRS (http://hrsonline.isr.umich.edu)34, 2859 from NCDS35. These studies have been described in detail elsewhere. Sample collection were carried out consistently and analysed by the same laboratories for UKHLS, ELSA and NCDS.
Biomarker measurements
In total, biomarker data were successfully obtained from 13,107 eligible individuals who gave consent to give blood samples to be stored for future analysis (https://www.understandingsociety.ac.uk/d/154/7251-UnderstandingSociety-Biomarker-UserGuide-2014.pdf?1418057881). All biomarkers were measured from serum (non-fasting), using a variety of suitable assays, and the majority analysed on a single Roche P module analyser36. On each machine Internal Quality Controls (IQC) were at regular intervals per day. External Quality Assurance (EQA) systems were in place to monitor all tests.
Phenotype transformations and exclusions
The measurements for biomarkers used in the association analyses were prepared according to protocols from the largest genetic association study published for each specific trait at the time when analyses commenced, details for which are available in Supplementary Table S2.
Genotyping
In total, 10,484 UKHLS samples have been typed using the Illumina Infinium HumanCoreExome BeadChip Kit® (12v1-0). This array contains a set of >250,000 highly informative genome-wide tagging single nucleotide polymorphisms as well as a panel of functional (protein-altering) exonic markers, including a large proportion of low-frequency (MAF 1–5%) and rare (MAF <1%) variants. Genotype calling was performed with the gencall algorithm using GenomeStudio (Illumina Inc.). For quality control (QC) we excluded individuals based on the following criteria: sample call rate <98%, autosomal heterozygosity outliers (>3SD), gender mismatches, duplicates as established by identity by descent (IBD) analysis (PI_HAT > 0.9). Individuals with non-European ancestry were also excluded. For this we estimated the genomic kinship between all pairs of individuals along with 1000 Genomes Project data. These were converted to distances and subjected to multidimensional scaling. Prior to variant QC, we first mapped all 538,448 variants to the human reference genome build 37. Variants with Hardy-Weinberg equilibrium p-value < 1 × 10−4, call rate below 98% or poor genotype clustering values (<0.4) were excluded, leaving 525,314 variants passing QC. For typed variants in our GWAS analyses that were brought forward for replication we inspected cluster plots manually using Scattershot 0.75 beta (Supplementary Fig. S1). All QC procedures were carried out using PLINK (v1.07) and R.
Imputation
We imputed our genotype data using a combined reference panel consisting of 7,562 haplotypes from the UK10K project and 2,184 haplotypes from 1000 Genomes phase 3. Details regarding the creation of this combined imputation panel are described elsewhere37. Prior to imputation, we first pre-phased using SHAPEIT (v2.r). Data were then imputed using IMPUTE2 (v2.3.0), resulting in an initial set of 38,310,212 variants. Variants with an IMPUTE info score <0.4, and variants with a Hardy-Weinberg p-value < 1 × 10−4 were excluded, leaving 26,851,013 variants for analysis.
Data availability
The UKHLS EGA accession number is EGAD00010000918. ELSA EGA accession number is EGAC00001000270. NCDS accession number is EGAC00000000001. HRS is available through dbGAP, Study Accession number phs000428.v1.p1. Genotype-phenotype data access for UKHLS, ELSA and NCDS is available by application to Metadac (www.metadac.ac.uk).
Statistical analysesh
Heritability analyses and genetic correlations
The proportion of trait variance explained by the genotyped and imputed variants was estimated using the GREML method as implemented in the GCTA software38, 39 (v1.26). We included all variants with minor allele frequency (MAF) > 0.01. We excluded variants with imputation accuracy less than 0.4. We computed the genetic relationship matrix (GRM) for each autosome and then used GCTA to combine them into one matrix. We excluded relatives from the estimation by filtering based on the GRM using a threshold of 0.1 after inspecting the distribution. This led to the exclusion of 672 individuals for this analysis. We also performed bivariate REML analysis in order to estimate genetic correlations between different biomarkers40. We applied a Bonferroni adjusted significance threshold using the effective number of traits for the heritability analyses and using the number of pairs based on the effective number of traits for the genetic correlation analyses.
Association analyses
The association analyses were carried out using a multivariate linear mixed model to account for relatedness as implemented in GEMMA (v0.95). QQ plots and genomic inflation factors, as well as Manhattan plots for traits where we identified novel associations are displayed in Supplementary Fig. S2. Replication analyses were carried out in R and PLINK, following the same trait preparation protocols as used in the discovery stage. The association summary statistics from the replication analyses, as well as the combined discovery and replication stage were meta-analysed using a fixed-effects inverse variance weighted approach implemented in METAL (v2011-03-25). We calculated an adjusted genome-wide significance threshold, for the effective number of traits, as several of our biomarkers have correlated levels. The effective number of traits was derived by computing the eigenvalues for the correlation matrix of the 20 biomarkers (effective number: 14.05). The routinely used GWAS threshold of p < 5 × 10−8 was then adjusted for this using the Bonferroni approach: 5 × 10−8/14.05 = 3.56 × 10−9.
Power calculations
We carried out power calculations using Quanto (v1.2.4), for discrete per-variant frequency and (standardised) effect sizes combinations, representative of variants identified in the discovery. Per-trait and per selected variant power analyses showed that we would minimally need 5,000 to 15,000 samples to replicate our variants with P < 3.56 × 10−9, two-sided, for testosterone levels, whereas the largest replication sample of 25,000 to 60,000 would be needed for eGFR (Fig. 4).
Selection of replication SNPs, and criteria for novel loci
For replication we selected independent SNPs (LD r2 < 0.1), with MAF > 0.01 and a discovery p-value of P < 1 × 10−5 and at least > 500 Kb away from the nearest known reported index SNP for a given trait. We also took forward independent rare variants with a MAF ≤ 0.01 that were typed and reached P < 1 × 10−5, regardless whether they represented known associations for a given trait. Known index SNPs for all biomarkers analysed in this study were obtained through the GWAS catalog41 (accessed August 4, 2016) > , supplemented by manual searches in PubMed.
Annotation
For annotation of our lead variants we used an in-house annotation script that automatically retrieves variant annotations from ENSEMBL42, including variant function, the nearest gene IDs within < 500Kb from a given variant, transcript and protein IDs for these genes, as well as conservation scores. It also calculates GWAVA43 scores for non-genic variants amongst other annotations.
All methods were performed in accordance with the relevant guidelines and regulations.
References
Teslovich, T. M. et al. Biological, clinical and population relevance of 95 loci for blood lipids. Nature 466, 707–713 (2010).
Cohen, J. C., Boerwinkle, E., Mosley, T. H. & Hobbs, H. H. Sequence variations in PCSK9, low LDL, and protection against coronary heart disease. N. Engl. J. Med. 354, 1264–1272 (2006).
Timpson, N. J. et al. A rare variant in APOC3 is associated with plasma triglyceride and VLDL levels in Europeans. Nat. Commun. 5, 4871 (2014).
Manolio, T. A. Bringing genome-wide association findings into clinical use. Nat. Rev. Genet. 14, 549–558 (2013).
Voight, B. F. et al. The metabochip, a custom genotyping array for genetic studies of metabolic, cardiovascular, and anthropometric traits. PLoS Genet. 8, e1002793 (2012).
Cortes, A. & Brown, M. A. Promise and pitfalls of the Immunochip. Arthritis Res. Ther. 13, 101 (2011).
Huffman, J. E. et al. Rare and low-frequency variants and their association with plasma levels of fibrinogen, FVII, FVIII, and vWF. Blood 126, e19–29 (2015).
Brennan, S. O., Fellowes, A. P., Faed, J. M. & George, P. M. Hypofibrinogenemia in an individual with 2 coding (gamma82 A– > G and Bbeta235 P– > L) and 2 noncoding mutations. Blood 95, 1709–1713 (2000).
Wyatt, J., Brennan, S. O., May, S. & George, P. M. Hypofibrinogenaemia with compound heterozygosity for two gamma chain mutations - gamma 82 Ala– > Gly and an intron two GT– > AT splice site mutation. Thromb. Haemost. 84, 449–452 (2000).
Ivaskevicius, V. et al. gammaAla82Gly represents a common fibrinogen gamma-chain variant in Caucasians. Blood Coagul. Fibrinolysis Int. J. Haemost. Thromb. 16, 205–208 (2005).
Stoller, J. K. & Aboussouan, L. S. A review of α1-antitrypsin deficiency. Am. J. Respir. Crit. Care Med. 185, 246–259 (2012).
de Serres, F. J., Blanco, I. & Fernández-Bustillo, E. Genetic epidemiology of alpha-1 antitrypsin deficiency in North America and Australia/New Zealand: Australia, Canada, New Zealand and the United States of America. Clin. Genet. 64, 382–397 (2003).
Walsh, C. T., Zydowsky, L. D. & McKeon, F. D. Cyclosporin A, the cyclophilin class of peptidylprolyl isomerases, and blockade of T cell signal transduction. J. Biol. Chem. 267, 13115–13118 (1992).
Jin, Z.-G. et al. Cyclophilin A is a proinflammatory cytokine that activates endothelial cells. Arterioscler. Thromb. Vasc. Biol. 24, 1186–1191 (2004).
Yazdanbakhsh, K., Choi, J. W., Li, Y., Lau, L. F. & Choi, Y. Cyclosporin A blocks apoptosis by inhibiting the DNA binding activity of the transcription factor Nur77. Proc. Natl. Acad. Sci. USA 92, 437–441 (1995).
Grimbert, P. et al. The Filamin-A is a partner of Tc-mip, a new adapter protein involved in c-maf-dependent Th2 signaling pathway. Mol. Immunol. 40, 1257–1261 (2004).
Carithers, L. J. et al. A Novel Approach to High-Quality Postmortem Tissue Procurement: The GTEx Project. Biopreservation Biobanking 13, 311–319 (2015).
The UK10K Consortium. The UK10K project identifies rare variants in health and disease. Nature 526, 82–90 (2015).
Bulik-Sullivan, B. et al. An atlas of genetic correlations across human diseases and traits. Nat. Genet. 47, 1236–1241 (2015).
Pownall, H. J. et al. Correlation of serum triglyceride and its reduction by omega-3 fatty acids with lipid transfer activity and the neutral lipid compositions of high-density and low-density lipoproteins. Atherosclerosis 143, 285–297 (1999).
Tall, A. R. Plasma cholesteryl ester transfer protein. J. Lipid Res. 34, 1255–1274 (1993).
Miller, W. L. Androgen biosynthesis from cholesterol to DHEA. Mol. Cell. Endocrinol. 198, 7–14 (2002).
Bolton, J. L. et al. Genome Wide Association Identifies Common Variants at the SERPINA6/SERPINA1 Locus Influencing Plasma Cortisol and Corticosteroid Binding Globulin. PLOS Genet. 10, e1004474 (2014).
North, T.-L. et al. A study of common Mendelian disease carriers across ageing British cohorts: meta-analyses reveal heterozygosity for alpha 1-antitrypsin deficiency increases respiratory capacity and height. J. Med. Genet. 53, 280–288 (2016).
Lomas, D. A., Evans, D. L., Finch, J. T. & Carrell, R. W. The mechanism of Z alpha 1-antitrypsin accumulation in the liver. Nature 357, 605–607 (1992).
Soranzo, N. et al. Common variants at 10 genomic loci influence hemoglobin A1(C) levels via glycemic and nonglycemic pathways. Diabetes 59, 3229–3239 (2010).
Fuchsberger, C. et al. The genetic architecture of type 2 diabetes. Nature 536, 41–47 (2016).
Wang, K.-S., Liu, X.-F. & Aragam, N. A genome-wide meta-analysis identifies novel loci associated with schizophrenia and bipolar disorder. Schizophr. Res. 124, 192–199 (2010).
Okbay, A. et al. Genetic variants associated with subjective well-being, depressive symptoms, and neuroticism identified through genome-wide analyses. Nat. Genet. 48, 624–633 (2016).
Kim, Y. J. et al. Large-scale genome-wide association studies in east Asians identify new genetic loci influencing metabolic traits. Nat. Genet. 43, 990–995 (2011).
Sluis, S., van der, Verhage, M., Posthuma, D. & Dolan, C. V. Phenotypic Complexity, Measurement Bias, and Poor Phenotypic Resolution Contribute to the Missing Heritability Problem in Genetic Association Studies. PLOS ONE 5, e13929 (2010).
Steptoe, A., Breeze, E., Banks, J. & Nazroo, J. Cohort profile: the English longitudinal study of ageing. Int. J. Epidemiol. 42, 1640–1648 (2013).
Lotta, L. A. et al. Integrative genomic analysis implicates limited peripheral adipose storage capacity in the pathogenesis of human insulin resistance. Nat. Genet., doi:10.1038/ng.3714 (2016).
Sonnega, A. et al. Cohort Profile: the Health and Retirement Study (HRS). Int. J. Epidemiol. 43, 576–585 (2014).
Power, C. & Elliott, J. Cohort profile: 1958 British birth cohort (National Child Development Study). Int. J. Epidemiol. 35, 34–41 (2006).
M Benzeval, A Davillas, M Kumari, P Lynn Understanding Society: the UK Household Longitudinal Study Biomarker User Guide and Glossary, ISER, University of Essex - Google Search. Available at: https://www.google.co.uk/search?q=M+Benzeval, +A+Davillas, +M+Kumari, +P+Lynn+ (2014)+Understanding+Society: +the+UK+Household+Longitudinal+Study+Biomarker+User+Guide+ and +Glossary, +ISER,+University+of+Essex&ie=utf-8&oe=utf-8&gws_rd=cr&ei=XfRSWOjVGdetgAa3qIKoDg. (Accessed: 15th December 2016) (2014).
Huang, J. et al. Improved imputation of low-frequency and rare variants using the UK10K haplotype reference panel. Nat. Commun. 6, 8111 (2015).
Yang, J. et al. Common SNPs explain a large proportion of the heritability for human height. Nat. Genet. 42, 565–569 (2010).
Yang, J., Lee, S. H., Goddard, M. E. & Visscher, P. M. GCTA: a tool for genome-wide complex trait analysis. Am. J. Hum. Genet. 88, 76–82 (2011).
Lee, S. H., Yang, J., Goddard, M. E., Visscher, P. M. & Wray, N. R. Estimation of pleiotropy between complex diseases using single-nucleotide polymorphism-derived genomic relationships and restricted maximum likelihood. Bioinforma. Oxf. Engl. 28, 2540–2542 (2012).
Welter, D. et al. The NHGRI GWAS Catalog, a curated resource of SNP-trait associations. Nucleic Acids Res. 42, D1001–1006 (2014).
Yates, A. et al. Ensembl 2016. Nucleic Acids Res. 44, D710–716 (2016).
Ritchie, G. R. S., Dunham, I., Zeggini, E. & Flicek, P. Functional annotation of noncoding sequence variants. Nat. Methods 11, 294–296 (2014).
Acknowledgements
We would like to acknowledge the Understanding Society Scientific Group which includes the following members: Michaela Benzeval, Jonathan Burton, Nicholas Buck, Annette Jäckle, Meena Kumari, Heather Laurie, Peter Lynn, Stephen Pudney, Birgitta Rabe, Dieter Wolke; The UK Household Longitudinal Study is led by the Institute for Social and Economic Research at the University of Essex. The UK Household Longitudinal Study is funded by the Economic and Social Research Council (ES/H029745/1). The survey was conducted by NatCen and the genome-wide scan data were analysed and deposited by the Wellcome Trust Sanger Institute (WT098051). Information on how to access the data can be found on the Understanding Society website https://www.understandingsociety.ac.uk/. Genetic analysis in The English Longitudinal Study of Ageing is sponsored by the Economic and Social Research council (ES/K005774/1). The Health and Retirement Study genetic data project was conducted by the University of Michigan and sponsored by the National Institute on Aging (grant numbers U01AG009740, RC2AG036495, and RC4AG039029). The Fenland Study is funded by the Wellcome Trust and the Medical Research Council (MC_U106179471). We further acknowledge support from the Medical research council (MC_UU_12015/1). We are grateful to all the volunteers for their time and help, and to the General Practitioners and practice staff for assistance with recruitment. Biochemical assays were performed by the National Institute for Health Research, Cambridge Biomedical Research Centre, Core Biochemistry Assay Laboratory and the Cambridge University Hospitals NHS Foundation Trust, Department of Clinical Biochemistry.
Author information
Authors and Affiliations
Contributions
B.P.P., K.B.K. and E.Z. drafted the initial manuscript. B.P.P. and K.B.K. performed the statistical analyses. E.Z. designed and supervised the study. Y.B., M.S., D.Z., G.F., J.L. carried out the replication analyses. N.J.W., R.A.S., J.R.B.P. and C.L. contributed data for the replication. M.B. is the principal investigator of UKHLS. M.K. is the genetics lead of UKHLS. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Prins, B.P., Kuchenbaecker, K.B., Bao, Y. et al. Genome-wide analysis of health-related biomarkers in the UK Household Longitudinal Study reveals novel associations. Sci Rep 7, 11008 (2017). https://doi.org/10.1038/s41598-017-10812-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-10812-1
This article is cited by
-
Identifying the potential causal role of insomnia symptoms on 11,409 health-related outcomes: a phenome-wide Mendelian randomisation analysis in UK Biobank
BMC Medicine (2023)
-
A previously uncharacterized Factor Associated with Metabolism and Energy (FAME/C14orf105/CCDC198/1700011H14Rik) is related to evolutionary adaptation, energy balance, and kidney physiology
Nature Communications (2023)
-
Sex steroid hormones and risk of breast cancer: a two-sample Mendelian randomization study
Breast Cancer Research (2022)
-
The combined impact of persistent infections and human genetic variation on C-reactive protein levels
BMC Medicine (2022)
-
Identifying molecular mediators of the relationship between body mass index and endometrial cancer risk: a Mendelian randomization analysis
BMC Medicine (2022)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
