
Abstract
Prokinetics for functional dyspepsia (FD) have relatively higher number needed to treat values. Acupuncture and related therapies could be used as add-on or alternative. An overview of systematic reviews (SRs) and network meta-analyses (NMA) were performed to evaluate the comparative effectiveness of different acupuncture and related therapies. We conducted a comprehensive literature search for SRs of randomized controlled trials (RCTs) in eight international and Chinese databases. Data from eligible RCTs were extracted for random effect pairwise meta-analyses. NMA was used to explore the most effective treatment among acupuncture and related therapies used alone or as add-on to prokinetics, compared to prokinetics alone. From five SRs, 22 RCTs assessing various acupuncture and related therapies were included. No serious adverse events were reported. Two pairwise meta-analyses showed manual acupuncture has marginally stronger effect in alleviating global FD symptoms, compared to domperidone or itopride. Results from NMA showed combination of manual acupuncture and clebopride has the highest probability in alleviating patient reported global FD symptom. Combination of manual acupuncture and clebopride has the highest probability of being the most effective treatment for FD symptoms. Patients who are contraindicated for prokinetics may use manual acupuncture or moxibustion as alternative. Future confirmatory comparative effectiveness trials should compare clebopride add-on manual acupuncture with domperidone add-on manual acupuncture and moxibustion.
Similar content being viewed by others

Introduction
Rationale
Functional dyspepsia (FD) is defined as pain or discomfort of the upper digestive tract in the absence of an organic cause that readily explains them1. One or more of the following symptoms are usually observed: postprandial fullness, early satiation, epigastric pain or burning2. FD is classified into two subtypes, postprandial distress syndrome (PDS, characterized by postprandial fullness and early satiation) and epigastric pain syndrome (EPS, characterized by epigastric pain and epigastric burning)2. The prevalence of FD ranged from 12 to 15% in the general population3. FD significantly reduces quality of life of patients, hence contributes to significant disease burden, treatment cost and loss of productivity4.
Current guidelines and expert consensus5,6,7,8,9 recommend the use of prokinetics as one of the routine treatments for FD. Effectiveness of prokinetics is however unsatisfactory, with a number needed to treat (NNT) of 1610. In addition, potential side effects of prokinetics have raised concern on their longer term use. For instance, existing studies suggest association between prokinetics use and increased risk of extra-pyramidal reactions, cardiac arrhythmic side effects including sudden cardiac death and drug-induced neurological disorders11,12,13,14. There is a need for addressing the effectiveness gap of those who are experiencing limited benefits from prokinetics, or those who are contraindicated to them.
In traditional Chinese medicine, acupuncture and related therapies have been used for treating functional gastrointestinal disorders (FGIDs) including FD15, 16. Existing evidence has shown the efficacy of acupuncture beyond sham control. In a Cochrane review of three trials, meta-analyses indicated that manual acupuncture was superior to sham acupuncture, for improving quality of life measured by SF-36 and Nepean Dyspepsia Life Quality Index17. Another meta-analysis performed by Kim and colleagues has shown that manual acupuncture was superior to sham acupuncture in FD symptoms reduction18. In a meta-analysis performed by Zhou and colleagues19, they have also shown that both manual acupuncture and electroacupuncture were superior to sham acupuncture, in the improvement of Nepean Dyspepsia Index.
When acupuncture and related therapies were compared with prokinetics, evidence from existing systematic reviews (SRs) is inconsistent. One SR showed similar effectiveness in FD symptoms reduction between manual acupuncture or electroacupuncture versus domperidone, as well as electroacupuncture versus itopride, in three separate trials17. However, meta-analyses from three other SRs showed that acupuncture and related therapies were more effective than prokinetics for FD symptoms reduction18,19,20.
These heterogeneous results make it difficult to draw conclusions on the effectiveness of acupuncture and related therapies on FD, used as an add-on or alternative to prokinetics. There is a need to perform an overview of SRs to clarify such uncertainty, as well as to assess the comparative effectiveness among different types of acupuncture and related therapies.
Objectives
We conducted an overview of SRs to critically appraise and synthesize all clinical evidence on the comparative effectiveness of different acupuncture and related therapies on the treatment of FD, using a network meta-analysis (NMA) approach21.
Methods
Search methods for identification of studies
Four electronic international (Cochrane Database of Systematic Reviews, Database of Abstracts of Reviews of Effect, MEDLINE, and EMBASE) and four Chinese electronic databases (Wan Fang Digital Journals, China National Knowledge Infrastructure, Taiwan Periodical literature databases and Chinese Biomedical Database) were searched for potential SRs from their inception till November 2015. Validated, sensitivity maximized search filters for systematic reviews were applied in MEDLINE and EMBASE searches22, 23. The searches were limited to human studies and no language restriction was applied. The search strategies are presented in Appendix 1.
Types of studies
To be included in this overview, SRs must include meta-analysis results, and satisfy the participants, interventions, controls and outcomes of interest criteria described below. SRs which only reported data narratively were excluded.
Types of participants
Patients diagnosed with FD according to Rome criteria, or other criteria stated by the authors were considered. There was no restriction on the versions of Rome criteria used.
Types of intervention
In this overview of SR, we only include three specific modalities: manual acupuncture, electroacupuncture, and moxibustion, as defined in Table 1 24. Accordingly, in this overview of SR we defined “acupuncture and related therapies” as single or combined use of manual acupuncture, moxibustion and electroacupuncture.
Accordingly, acupuncture and related therapies including the single or combined use of manual acupuncture, moxibustion, electroacupuncture were considered eligible for this overview. Prokinetics can be used as an add-on or alternative to these interventions. Prokinetics which are available in the market were eligible in the comparison group except cisapride. We chose to exclude cisapride as it has been removed from market due to serious adverse events25. Trials which evaluate combined therapy of proton pump inhibitors (PPIs) and prokinetics was excluded, as substantial side effects of their combined use have been shown in recent meta-analyses26. Combined therapy of H2 histamine receptor antagonist (H2RA) and prokinetics was also excluded, as H2RA has shown to be associated with an increased risk of pneumonia by a meta-analysis27, vitamin B12 deficiency by a case-control study28 and impaired cognitive function among elderlies by a cohort study29.
Outcome measures
Trials results reported from each meta-analysis should include at least one of the following outcomes:
(i) Alleviation of dyspeptic symptoms, measured with either global or individual dyspepsia symptom scores; or (ii) proportion of patients achieving satisfactory alleviation of global or individual symptoms. Choices of these outcomes were based on current expert recommendations on endpoints for FD clinical trials30.
Eligibility Assessment and Data Extraction
Two reviewers (RH and IW) independently screened titles and abstracts of retrieved citations, evaluated potential full texts, and determined eligibility. For each eligible SRs, full texts of each embedded RCTs were obtained. For duplicate citations, the most updated RCTs were selected for data extraction, while the older versions were used as supplementary information, if necessary. Discrepancies were resolved by consensus between two reviewers. A third reviewer (VC) was invited for consensus adjudication if discrepancy were not resolved.
The following were extracted from each embedded RCTs: year of publication, number of patients enrolled, participant characteristics, duration of FD diagnosis, diagnostic criteria used, and features of interventions in treatment and control groups. These features included frequencies of acupuncture sessions and prokinetics dosage intake. Types of outcome assessment, treatment duration, and follow-up duration, as well as any reported adverse events were also extracted.
Methodological quality of included SRs and risk of bias assessment of included RCTs
The validated Methodological Quality of Systematic Reviews (AMSTAR) instrument was used to appraise quality of included SRs31. For each embedded RCTs, their risks of bias were assessed by the Cochrane’s risk of bias tool32. Both appraisals were performed by two reviewers (RH and IW) independently. Discrepancies were resolved by discussion between two reviewers, and consensus adjudication was sought from a third author (VC) if discrepancy persisted.
Data synthesis
We followed established methods of conducting pairwise meta-analysis, followed by network meta-analysis (NMA) in this systematic review, which are considered as standard modelling methodology in the field33.
The first method, pairwise meta-analysis, synthesize results from head to head comparison between acupuncture and related therapies versus prokinetics under random effect model34.
Random effect pairwise meta-analyses were used to synthesize data extracted from embedded RCTs, separately for each type of acupuncture and related therapies using Review Manager Version 5.335. Pooled relative risk (pooled RR) and standardized mean difference (SMD), with their 95% confidence interval (CI) were used to synthesize dichotomous outcome and continuous outcome respectively. I-square (I2) values were calculated for quantifying heterogeneity among RCTs. The I2 value of <25%, 26-50%, >50% were regarded as low, moderate, and high heterogeneity respectively36.
The outcome of global assessment on a Likert scale measures overall symptom improvement or deterioration. This approach allows the individual to integrate all aspects of one’s condition into a single treatment outcome, and is particularly suitable to show deterioration30. All primary outcomes of symptoms improvement were reported on short, 3 or 4 points Likert scales. Following recommendation of the Cochrane Handbook, we lumped these “short” ordinal results into dichotomous data as this resemble clinical decision making process of “to do” or “not to do”37. Provided that the ordinal outcome rating scales used among trials were similar, such combination of short ordinal scale is justified38. Indeed, binary assessment for overall symptom improvement is an accepted approach for outcome measurement in functional dyspepsia trials39.
Accordingly all 3 point Likert scale results were categorized as “marked improvement”, “slight improvement” and “no improvement”, while all 4 point Likert scale cases were categorized as “symptom-free”, “marked improvement”, “slight improvement” and “no improvement”. Then, in the transformation process, the categories of “symptom-free”, “marked improvement” or “slight improvement” cases were combined and labelled as “favourable” cases; while “no improvement” cases were renamed as “unfavourable” cases.
The second method is indirect comparisons of the effectiveness among 11 treatments of acupuncture and related therapies used as add-on or alternative to prokinetics for FD via NMA, a standard modelling methodology for conducting overview of systematic review40. NMA is a preferred approach which offers a set of methods to visualize and interpret wider picture of existing evidence, as well as to understand the comparative effectiveness of these multiple treatments41.
NMA was conducted to explore the highest probability of being the most effective form of acupuncture and related therapies when compared to prokinetics, either alone or as an add-on, by using STATA Version 13.0 (STATA Corporation, College Station, TX)42. Indirect comparisons of dichotomous and continuous outcomes among different treatments were implemented with the mvmeta command43, 44. Assumption of NMA was checked by evaluating inconsistency factor (IF) of direct and various indirect effect estimates, using the loop-specific heterogeneity estimates43 for the same comparison.
When summarizing comparative effectiveness ranking results from NMA, we calculated the probability of an intervention being the most effective treatment, the second best treatment, the third best treatment and so on by calculating the RR (dichotomous outcome) and mean difference (continuous outcome) for each possible pair of comparisons. The probability for a treatment of being at a particular rank was interpreted by the surface under the cumulative ranking curve (SUCRA) and mean ranks were used to obtain the effectiveness hierarchy. The more surface of SUCRA curve, the higher probability of the treatment will be43, 44. All statistical tests were 2-tailed with significance level of 0.05.
Results
Literature search
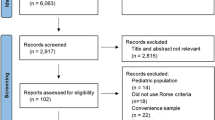
The search strategies yielded 192 records, and 23 duplicates were identified and excluded. We excluded 157 citations after screening titles and abstracts, and full texts of the remaining 12 citations were retrieved for further assessment. Seven publications were excluded for the following reasons: six were narrative reviews, and one SR involved head to head comparison of acupuncture and related therapies with cisapride. A total of 5 SRs were included in this overview. Details of the literature search and SR selection can be found in Fig. 1. These 5 SRs (Appendix 2) included a total of 78 RCTs. Among these RCTs, fifty-six were excluded due to the following reasons:
-
duplicate publications (n = 24);
-
ineligible control groups (n = 29), of which 4 groups were PPIs plus prokinetics, 3 groups were Chinese herbal medicine, 1 group was homeopathy, 1 group was antacid, 1 group was H2 histamine receptor antagonist plus prokinetics, 7 groups were head to head comparison between acupuncture and related therapies with cisapride and 12 used sham acupuncture;
-
ineligible experimental groups (n = 2) of vitamin injection and finger acupressure;
-
one did not report outcome on FD symptom changes (n = 1).

Flowchart of literature selection on systematic reviews on acupuncture and related therapies for functional dyspepsia.
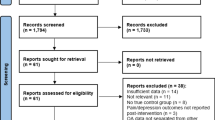
After applying eligibility criteria, 22 unique RCTs were extracted from the SRs for inclusion in this overview. Details on the RCTs literature selection were presented in Fig. 2. A list of these eligible RCTs was presented in Appendix 3.

Flowchart for randomized controlled trials selection for acupuncture and related therapies for functional dyspepsia.
Characteristics of included RCTs
Participants
Characteristics of included RCTs were summarized in Table 2. The 22 RCTs included a total of 1,727 FD patients. Age of participants ranged from 17 to 70 years. Average sample size of the RCTs was 79 participants (ranging from 46 to 260). Duration of diagnosis ranged from 1.2 to 120 months.
Diagnostic criteria
Respectively eleven, six and three RCTs applied the Rome III, Rome II and Rome I criteria. Two RCTs followed criteria determined by the authors.
Interventions
Amongst the 22 included RCTs, all RCTs were two arm trials, except one which has three arms. Twenty-three comparisons were therefore included in this review. Four different forms of acupuncture and related therapies were evaluated: manual acupuncture (10 comparisons), manual acupuncture plus moxibustion (4 comparisons), moxibustion (3 comparisons), electroacupuncture (3 comparisons). Three types of combination therapies were evaluated: one each for clebopride or mosapride being an add-on to manual acupuncture (2 comparisons) and domperidone being an add-on to manual acupuncture plus moxibustion (1 comparison). Four types of oral prokinetics were evaluated as comparison: domperidone (13 comparisons), itopride (6 comparisons), mosapride (2 comparisons), and clebopride (1 comparison). Fifteen out of 22 RCTs offered 20 to 30 sessions of acupuncture and related therapies. Detailed descriptions of the included acupuncture and related therapies procedures are reported in Table 3 according to the revised standards for reporting interventions in clinical trials of acupuncture (STRICTA)45. Information including the style of acupuncture, names of acupuncture points used, depth of needle insertion or moxa distance away from skin, response sought, retention time, needle or moxa type, length and diameter of needle or moxa, frequency and duration of acupuncture sessions were shown in detailed in Table 3.
Treatment duration for acupuncture or related therapies as well as prokinetics ranged from four weeks (17 RCTs) to three weeks (1 RCT) and two weeks (4 RCTs). Follow-up duration for outcome assessment ranged from 2 weeks to 12 weeks.
Critical appraisal of SRs and RCTs
Methodological quality of the five SRs, including one Cochrane SR and four non-Cochrane SRs, was mediocre. All included SRs performed duplicate study selection and data extraction, conducted comprehensive literature search, formulated conclusions appropriately regarding to scientific quality of the included studies, and provided characteristics and assessed the scientific quality of included studies. Four SRs used appropriate statistical methods for combining findings. However, none of the SRs explicitly stated conflicts of interests for both the SR and included studies. Except one Cochrane SR, the remaining four did not fulfill the following three AMSTAR criteria: providing a protocol of the SR, searching unpublished literature, providing lists of both included and excluded studies. Only two SRs assessed publication bias. Details on methodological quality of the five SRs are presented in Table 4.
Overall, risk of bias amongst included RCTs is moderate. Amongst these 22 RCTs, nine were of low risk of bias for random sequence generation, while seven did not report sequence generation procedures used and six were of high risk of bias. Except one RCT, all did not state details on allocation concealment. In all trials, patient blinding was not applied, and blinding of investigators was not reported. Outcome assessment was based on subjective outcome reported by patients themselves. Thus these 2 domains were subjected to high risk of bias. All included RCTs had low risk of bias for incomplete data, with 21 out of 22 RCTs achieved 100% follow up rate. Selective outcome reporting was unclear in all included RCTs as none of them provided published protocols. Risk of bias assessment results of the 22 RCTs were presented in Table 5.
Results of pairwise meta-analyses on binary outcome
Five pairwise meta-analyses were performed to compare the effectiveness between acupuncture and related therapies versus prokinetics. Detailed results were shown in Fig. 3.

Five pairwise meta-analyses on the comparative effectiveness of acupuncture and related therapies versus prokinetics.
When compared to domperidone, manual acupuncture showed a marginally stronger effect in alleviating global FD symptoms (6 RCTs, pooled RR: 1.21, 95%CI: 1.10, 1.33, p = 0.0001, I2 = 21%). Manual acupuncture were also found to be marginally superior to itopride (3 RCTs, pooled RR: 1.30, 95%CI: 1.11, 1.52, p = 0.001, I2 = 33%).
There was no statistically significant difference between moxibustion and domperidone in their effectiveness in alleviating global FD symptoms (3 RCTs, pooled RR: 1.14, 95%CI: 0.97, 1.33, p = 0.12, I2 = 54%), but moderate level of heterogeneity exists. No significant difference were observed for the following 2 comparisons as well: manual acupuncture plus moxibustion versus domperidone (2 RCTs, pooled RR: 1.10, 95%CI: 0.92, 1.33, p = 0.30, I2 = 0%); and electroacupuncture alone versus itopride alone (2 RCTs, pooled RR: 1.12, 95%CI: 1.00, 1.26, p = 0.05, I2 = 0%).
Results of network meta-analysis
A network was devised to illustrate the comparative effectiveness among 11 interventions for patient reported global FD symptom. These 11 interventions were different forms of acupuncture and related therapies, used alone or as an add-on to prokinetics. The common comparator among all RCTs in the network was prokinetics (Fig. 4). Indirect comparison on the dichotomous outcome of patient reported global FD symptom alleviation among these 11 treatments is shown in Fig. 5.

Network of comparison on patient reported global functional dyspepsia symptoms. Width of the lines represents the proportion of the number of trials for each comparison to the number of trials. Size of the nodes represents the proportion of the number of randomized patients (sample sizes).

Comparative effectiveness of 11 interventions for alleviating patient reported global functional dyspepsia symptom: Results of indirect comparisons. Results are the relative risks (RRs) and related 95% credibility intervals in the row-defining treatment compared with the RRs in the column-defining treatment. RRs higher than 1 favour the column-defining treatment, and vice versa. Significant result is in bold and underlined.
Five interventions including (i) manual acupuncture, (ii) moxibustion, (iii) clebopride, (iv) combination of manual acupuncture, moxibustion and domperidone, and (v) combination of manual acupuncture and clebopride, were significantly more effective than domperidone alone (first column of Fig. 5).
Five interventions including (i) manual acupuncture, (ii) moxibustion, (iii) electroacupuncture, (iv) combination of manual acupuncture and moxibustion, and (v) combination of manual acupuncture, moxibustion and domperidone showed superiority over itopride alone (seventh row of Fig. 5).
Four treatments including (i) manual acupuncture, (ii) moxibustion, and (iii) combination of manual acupuncture, moxibustion and domperidone, and (iv) combination of manual acupuncture and mosapride were significantly more effective than mosapride alone (eighth row of Fig. 5, third last row of Fig. 5).
The combination of manual acupuncture and clebopride was significantly more effective than 4 other treatments, including (i) domperidone, (ii) itopride, (iii) mosapride, and (iv) combination of manual acupuncture and moxibustion (second last row of Fig. 5). Lastly, clebopride was more effective than 3 other prokinetics including domperidone, itopride and mosapride (last row of Fig. 5).
Figure 6 showed the cumulative probabilities (SUCRA results) of being the best option for alleviating patient reported global FD symptom, when the 11 treatments are compared simultaneously. The combination of manual acupuncture and clebopride has the highest probability being the best (95.0%), followed by the combination of manual acupuncture, moxibustion and domperidone (76.1%), clebopride (74.5%), manual acupuncture (62.6%), moxibustion (62.3%), combination of manual acupuncture and mosapride (61.9%), electroacupuncture (48.6%), combination of manual acupuncture and moxibustion (35.9%), and domperidone (18.4%). Mosapride (7.6%) and itopride (7.1%) have the lowest probabilities.

Surface under the cumulative ranking curves (SUCRA) for patient reported global symptom in functional dyspepsia patients. The x-axis represents the possible rank of each treatment (from the first best rank to the worst according to the alleviation of patient reported global functional dyspepsia symptom). The y-axis indicated the cumulative probability for each treatment to be the best treatment, the second best treatment, the third best treatment, and so on.
In this NMA, inconsistency of direct and various indirect effect estimates was insignificant. IF was found to be small (z test for three loops = 0.27, 0.54 and 0.52, all p values > 0.05).
Results from continuous outcome
We have extracted continuous data on patient reported individual symptoms in continuous data including postprandial fullness, early satiety, epigastric pain and epigastric burning comparing (i) manual acupuncture, (ii) moxibustion, and (iii) combination of manual acupuncture and moxibustion with domperidone. However, due to the scarcity of comparisons in the network, consistency assumption cannot be met and thus we chose not to perform NMA. When compared to domperidone, manual acupuncture showed stronger effect in alleviating postprandial fullness (SMD: −0.79, 95%CI: −1.30, −0.28, p = 0.002)46, moxibustion was found to be superior in alleviating both early satiety (SMD: −0.77, 95%CI: −1.37, −0.17, p = 0.01) and epigastric pain (SMD: −0.87, 95%CI: −1.47, −0.26, p = 0.005)47, and combination of manual acupuncture and moxibustion was shown to be more favourable in alleviating epigastric pain (SMD: −0.66, 95%CI: −1.18, −0.14, p = 0.01)48. However, no statistically significant difference were observed for the following comparisons when compared with domperidone: manual acupuncture in alleviating early satiety (SMD: −0.31, 95%CI: −0.80, 0.18, p = 0.21) and epigastric pain (SMD: −0.13, 95%CI: −0.62, 0.35, p = 0.59)46; moxibustion in alleviating postprandial fullness (SMD: −0.11, 95%CI: −0.69, 0.47, p = 0.71) and epigastric burning (SMD: −0.58, 95%CI: −1.17, 0.01, p = 0.06)47; and combination of manual acupuncture and moxibustion in alleviating postprandial fullness (SMD: −0.20, 95%CI: −0.71, 0.31, p = 0.43), early satiety (SMD: 0.12, 95%CI: −0.38, 0.63, p = 0.63) and epigastric burning (SMD: −0.21, 95%CI: −0.72, 0.30, p = 0.41)48. Detailed results are shown in Appendix 4.
Adverse events
No serious adverse events were reported in all included RCTs. All reported adverse events were of minor and transient nature. In one included RCT48 reported 4 cases of ecchymosis at acupuncture points after manual acupuncture plus moxibustion, while rash (n = 1) and constipation (n = 2) were reported in the domperidone group. In another RCT49, there were six patients reporting minor nausea, five cases of increased defecation frequency, and five stomach rumble cases reported as adverse events in the combined manual acupuncture and mosapride group. While in the mosapride group, there were respectively five, four and five cases of minor nausea, increased frequency of defecation and stomach rumble reported as adverse events.
Discussion
Implications for practice
From our results, the combination of clebopride plus manual acupuncture and the combination of domperidone plus manual acupuncture and moxibustion are ranked to have the highest probability of being the best treatment options. Taking into account potential adverse effects of these prokinetics, including Parkinsonism syndrome and hemifacial dystonia from clebopride13, 14; and extra-pyramidal reactions and cardiac arrhythmic effects from domperidone, manual acupuncture or moxibustion could be alternatives to these medications.
Physiologically, bidirectional brain-gut interactions involve the regulation of digestive processes, including the control of appetite, food in-take, as well as coordination of the gastrointestinal (GI) tract activities50. Central and peripheral alterations of brain-gut interactions are proposed to cause symptoms of chronic abdominal pain and associated GI dysfunction51. A recent systematic review has shown associations of FD with functional abnormalities in brain-gut interactions, including the aspects of sensory and pain modulation, emotion, saliency and homeostatic processing52. A cross-sectional study performed by Zeng and colleagues has compared resting brain activity between FD patients and healthy subjects. Higher glycometabolism was observed among FD patients than healthy subjects in the key regions of the homeostatic afferent processing network, including the insula, hypothalamus, brainstem and the anterior cingulate cortex (ACC). The abnormalities of these regions were significantly related to the severity of FD symptoms53.
Increased sensory signal from the gut, as well as impaired central modulation of pain and gut functions were considered to be the key pathogenic features among FD patients. These would subsequently cause central changes like functional brain abnormalities and peripheral changes including visceral hypersensitivity, abnormal gastric motility and accommodation52. These mechanisms are found to be associated with FD symptoms53.
With regards to the potential therapeutic mechanisms of acupuncture, a RCT comparing brain responses between FD patients receiving acupuncture and sham acupuncture may offer some insights. It is observed that deactivations of glycometabolism in cerebral regions including the insula, ACC, prefrontal cortex, putamen, hypothalamus, hippocampus, parahippocampal gyrus and temporal pole were observed only in patients receiving acupuncture, but not amongst those with sham acupuncture. Since the majority of these deactivated regions in the acupuncture group belonged to the homeostatic sensory processing network, acupuncture is suggested to have an effect in modulating the activity of the homeostatic afferent processing network and hence restoring the balance of homeostatic mechanism. This is a potential mechanism that explain the effectiveness of acupuncture for managing FD54.
Since all participants of the included trials were Chinese, applicability of our results to other ethnicity is limited. Also, external validity of our results is limited by the use of heterogeneous diagnostic criteria for inclusion amongst trials. It is noteworthy that the Rome III criteria has been adopted in 11 out of 22 included RCTs, and it is acknowledged that its use may lead to exclusion of a substantial number of patients with endoscopically verified FD55. The application of such a strict inclusion criteria implies that trial patients are likely to differ from average patient seen in clinical practice55. In the newly announced Rome IV criteria, only minor modifications were made with regards to symptom description56. In the future, a more flexible diagnostic criteria might be used in recruiting patients in FD clinical trials57.
Implications for research
With regards to internal validity, our assessment suggested that risk of bias among included RCTs is often unclear due to poor reporting, especially in allocation concealment and selective outcome reporting domains. Indeed, poor reporting is a prevalent problem in Chinese medicine publications58 and we cannot draw any solid conclusion on their methodological rigor. Also, end points are subjective patient reported outcomes, but blinding of patients and investigators were not applied among Included RCTs. These risks of bias may lead to an exaggeration of treatment effects for acupuncture and related therapies59.
On top of improving rigor, future trialists should adhere to the CONSORT reporting statement60 for improving the usefulness of study results, as well as in methodological transparency. All adverse events should also be well reported. With regards to outcome selection, while patient reported symptoms alleviation can remain as one of the endpoint, depending on such dichotomous assessment is not sufficient. Both objective as well as detailed patient centered outcome should be reported in future trials, including (i) individual symptom assessment; (ii) disease specific quality of life questionnaire; (iii) nutrient drink test; and (iv) gastric emptying test61. Also, follow-up duration of 16 out of 22 included RCTs was only 4 weeks. Longer term benefits of acupuncture and related therapies should be evaluated by following the recommended follow-up duration of at least 12 weeks61.
Current guideline recommends PPIs as one of the first line treatment for FD62, but in this systematic review we did not locate any RCTs which provide evidence on the comparative effectiveness of acupuncture and related therapies and PPIs, or their combined use. Acupuncture and related therapies could also be an alternative to patient responding poorly to PPIs, or when patients are contraindicated for its adverse effects of increased risk of dementia63, chronic and acute kidney disease, hypomagnesemia, Clostridium difficile infection, and osteoporotic fractures64. Future trials should investigate this research question.
Our assessment indicated rooms for improvement on rigor of included SRs. There are several methodological areas that require attention from future SR authors. These include assessment of publication bias, reporting of conflict of interest, searching for unpublished studies, providing a list of included and excluded studies, and publishing protocols of SRs. Methodological and reporting standards of SR should follow the AMSTAR tool and PRISMA statement65 respectively. Finally, although mechanism of acupuncture’s effect on FD has been studied, therapeutic mechanism of moxibustion has not been studied and is subjected to further research.
Conclusion
With clinical evidence summarized by this overview of SRs and NMA, it is observed that the combination of manual acupuncture and clebopride has the highest probability of being the most effective therapy for alleviating FD symptoms. FD patients who are intolerant or unresponsive to prokinetics, manual acupuncture or moxibustion may be used as alternative. The potential synergistic effect of PPIs plus acupuncture and related therapies should also be explored in future trials. Future trialists should pay attention to choice of diagnostic criteria, outcome assessment, as well as methodological rigor in trial design.
References
Tack, J. & Talley, N. J. Functional dyspepsia–symptoms, definitions and validity of the Rome III criteria. Nat Rev Gastroenterol Hepatol. 10, 134–41 (2013).
Drossman, D. A. The functional gastrointestinal disorders and the Rome III process. Gastroenterology. 130, 1377–90 (2006).
El-Serag, H. B. & Talley, N. J. Systemic review: the prevalence and clinical course of functional dyspepsia. Aliment Pharmacol Ther. 19, 643–54 (2004).
Brun, R. & Kuo, B. Review: functional dyspepsia. Therapeutic advances in gastroenterology. 3, 145–64 (2010).
Moshiree, B., Barboza, J. & Talley, N. An update on current pharmacotherapy options for dyspepsia. Expert opinion on pharmacotherapy. 14, 1737–53 (2013).
Camilleri, M. & Stanghellini, V. Current management strategies and emerging treatments for functional dyspepsia. Nature Reviews Gastroenterology and Hepatology. 10, 187–94 (2013).
Lacy, B. E. et al. Review article: current treatment options and management of functional dyspepsia. Alimentary pharmacology & therapeutics. 36, 3–15 (2012).
Talley, N. J. & Vakil, N. Guidelines for the management of dyspepsia. The American journal of gastroenterology. 100, 2324–37 (2005).
Loyd, R. A. & McClellan, D. A. Update on the evaluation and management of functional dyspepsia. American family physician. 83, 547 (2011).
Hojo, M., Nagahara, A., Asaoka, D. & Watanabe, S. Emerging pharmacological therapy for functional dyspepsia. Clinical journal of gastroenterology. 6, 352–6 (2013).
Quigley, E. M. Prokinetics in the management of functional gastrointestinal disorders. Journal of neurogastroenterology and motility. 21, 330 (2015).
Leelakanok, N., Holcombe, A. & Schweizer, M. L. Domperidone and risk of ventricular arrhythmia and cardiac death: a systematic review and meta-analysis. Clinical drug investigation. 36, 97–107 (2016).
Shin, H. W. & Chung, S. J. Drug-induced parkinsonism. Journal of clinical neurology. 8, 15–21 (2012).
Bosco, D., Plastino, M., Marcello, M. G., Mungari, P. & Fava, A. Acute Hemifacial Dystonia Possibly Induced by Clebopride. Clinical neuropharmacology. 32, 107–8 (2009).
Chen, J. D., Yin, J., Takahashi, T. & Hou, X. Complementary and alternative therapies for functional gastrointestinal diseases. Evidence-Based Complementary and Alternative Medicine. 2015, 138645 (2015).
Takahashi, T. Acupuncture for functional gastrointestinal disorders. Journal of gastroenterology. 41, 408–17 (2006).
Lan, L. et al. Acupuncture for functional dyspepsia. Cochrane Database of Systematic Reviews. (2014).
Kim, K. N., Chung, S. Y. & Cho, S. H. Efficacy of acupuncture treatment for functional dyspepsia: A systematic review and meta-analysis. Complementary therapies in medicine. 23, 759–66 (2015).
Zhou, W., Su, J. & Zhang, H. Efficacy and Safety of Acupuncture for the Treatment of Functional Dyspepsia: Meta-Analysis. The Journal of Alternative and Complementary Medicine. 22, 380–89 (2016).
Wu, X. W., Ji, H. Z., Xu, L. E. & Wang, F. Y. The effect of acupuncture and moxibustion on functional dyspepsia compared with prokinetic agents: a meta-analysis. Chin J Integr Trad West Med Dig. 23, 100–04 (2015).
Mills, E. J., Thorlund, K. & Ioannidis, J. P. Demystifying trial networks and network meta-analysis. BMJ. 346, f2914 (2013).
Haynes, R. B., Wilczynski, N., McKibbon, K. A., Walker, C. J. & Sinclair, J. C. Developing optimal search strategies for detecting clinically sound studies in MEDLINE. Journal of the American Medical Informatics Association. 1, 447–58 (1994).
Wong, S. S., Wilczynski, N. L. & Haynes, R. B. Developing optimal search strategies for detecting clinically sound treatment studies in EMBASE. Journal of the Medical Library Association. 94, 41–47 (2006).
Lao, L. X. Acupuncture techniques and devices. The Journal of Alternative and Complementary Medicine. 2, 23–25 (1996).
Wysowski, D. K., Corken, A., Gallo-Torres, H., Talarico, L. & Rodriguez, E. M. Postmarketing reports of QT prolongation and ventricular arrhythmia in association with cisapride and Food and Drug Administration regulatory actions. The American journal of gastroenterology. 96, 1698–703 (2001).
Ren, L. H. et al. Addition of prokinetics to PPI therapy in gastroesophageal reflux disease: a meta-analysis. World J Gastroenterol. 20, 2412–9 (2014).
Eom, C. S. et al. Use of acid-suppressive drugs and risk of pneumonia: a systematic review and meta-analysis. Canadian Medical Association Journal. 183, 310–9 (2011).
Lam, J. R., Schneider, J. L., Zhao, W. & Corley, D. A. Proton pump inhibitor and histamine 2 receptor antagonist use and vitamin B12 deficiency. JAMA. 310, 2435–42 (2013).
Hanlon, J. T. et al. Histamine2 receptor antagonist use and decline in cognitive function among community dwelling elderly. Pharmacoepidemiology and drug safety. 13, 781–87 (2004).
Ang, D. et al. Review article: endpoints used in functional dyspepsia drug therapy trials. Alimentary pharmacology & therapeutics. 33, 634–49 (2011).
Shea, B. J. et al. AMSTAR is a reliable and valid measurement tool to assess the methodological quality of systematic reviews. Journal of clinical epidemiology. 62, 1013–20 (2009).
Higgins, J. P. et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trial. s. BMJ. 343, d5928 (2011).
Salanti, G. Indirect and mixed‐treatment comparison, network, or multiple‐treatments meta‐analysis: many names, many benefits, many concerns for the next generation evidence synthesis tool. Research synthesis methods. 3, 80–97 (2012).
Borenstein, M., Hedges, L. V., Higgins, J. & Rothstein, H. R. A basic introduction to fixed‐effect and random‐effects models for meta‐analysis. Research Synthesis Methods. 1, 97–111 (2010).
Review Manager 5. Available from: http://community.cochrane.org/tools/review-production-tools/revman-5. Accessed date: 20 December, 2016.
Higgins, J. P., Thompson, S. G., Deeks, J. J. & Altman, D. G. Measuring inconsistency in meta-analyses. BMJ. 327, 557–60 (2003).
Higgins, J.P.T & Green, S. (editors). Section 9.2.4., Effect Measures for Ordinal Outcomes and Measurement Scales. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org.
Higgins, J.P.T & Green, S. (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. Available from www.handbook.cochrane.org. Accessed date: 20 December, 2016.
Talley, N. J. et al. Effect of amitriptyline and escitalopram on functional dyspepsia: a multicenter, randomized controlled study. Gastroenterology. 149, 340–349 (2015).
Caldwell, D. M. An overview of conducting systematic reviews with network meta-analysis. Systematic reviews. 3, 109 (2014).
Lu, G. & Ades, A. E. Combination of direct and indirect evidence in mixed treatment comparisons. Statistics in medicine. 23, 3105–3124 (2004).
STATA 13- Data Analysis and Statistical Software. Available from: https://www.stata.com/support/updates/stata13.html. Accessed date: 20 December, 2016.
Chaimani, A., Higgins, J. P., Mavridis, D., Spyridonos, P. & Salanti, G. Graphical tools for network meta-analysis in STATA. PloS one. 8, e76654 (2013).
Salanti, G., Ades, A. & Ioannidis, J. P. Graphical methods and numerical summaries for presenting results from multiple-treatment meta-analysis: an overview and tutorial. Journal of clinical epidemiology. 64, 163–71 (2011).
MacPherson, H. et al. Revised standards for reporting interventions in clinical trials of acupuncture (STRICTA): extending the CONSORT statement. Journal of Evidence‐Based Medicine. 3, 140–155 (2010).
Feng, G.X., Zhu, Y. & Jiang, G.F. Observation on therapeutic effect of 35 cases of functional dyspepsia treated by acupuncture. New Journal of Traditional Chinese Medicine. 36, 48–9 (2004). (Citation translated from Chinese to English).
Yang, J.M., Zhang, T.F. & Huang, G.F. Treatment 23 cases functional dyspepsia by moxibustion treatment. Journal of Jiangxi Chinese Medicine. 42, 43–5 (2011). (Citation translated from Chinese to English).
Zheng, X., Song, X., Jiang, X., ZHANG, G. Z. & CHEN, J. Q. Clinical observation of acupuncture for treatment of Pi Wei Qi deficiency functional dyspepsia. J Trop Med. 13, 232–4 (2013).
He, C. L. Clinical efficacy of mosapride and acupuncture used in the treatment of FD. Journal of Qiqihar University of Medicine. 33, 2906–7 (2012).
Mayer, E. A. & Saper, C. B., editors. The Biological Basis for Mind Body Interactions. Elsevier. 122 (2000).
Mayer, E. A. & Tillisch, K. The brain-gut axis in abdominal pain syndromes. Annual review of medicine. 62, 381–96 (2011).
Lee, I. S., Wang, H., Chae, Y., Preissl, H. & Enck, P. Functional neuroimaging studies in functional dyspepsia patients: a systematic review. Neurogastroenterology & Motility. 28, 793–805 (2016).
Zeng, F. et al. Abnormal resting brain activity in patients with functional dyspepsia is related to symptom severity. Gastroenterology. 141, 499–506 (2011).
Zeng, F. et al. Influence of acupuncture treatment on cerebral activity in functional dyspepsia patients and its relationship with efficacy. Am J Gastroenterol. 107, 1236–47 (2012).
van Kerkhoven, L. A. et al. Functional dyspepsia: not all roads seem to lead to Rome. Journal of clinical gastroenterology. 43, 118–22 (2009).
Sood, R. & Ford, A. C. Diagnosis: Rome IV criteria for FGIDs - an improvement or more of the same? Nature Reviews Gastroenterology & Hepatology. 13, 501–2 (2016).
Shuldiner, S. R. et al. Methodological challenges in mapping chinese medicine syndrome with conventional diagnosis: Implications for multi-centre trials in integrative medicine. European Journal of Integrative Medicine. 7, 358–64 (2015).
Li, J. et al. The quality of reports of randomized clinical trials on traditional Chinese medicine treatments: a systematic review of articles indexed in the China National Knowledge Infrastructure database from 2005 to 2012. BMC complementary and alternative medicine. 14, 1 (2014).
Page, M. J. et al. Empirical evidence of study design biases in randomized trials: systematic review of meta-epidemiological studies. PLoS One. 11, e0159267 (2016).
Moher, D. et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. Journal of clinical epidemiology. 63, e1–e37 (2010).
Lacy, B. E., Talley, N. J. & Camilleri, M. Functional dyspepsia: time to change clinical trial design? The American journal of gastroenterology. 105, 2525–29 (2010).
Talley, N. J. American Gastroenterological Association medical position statement: evaluation of dyspepsia. Gastroenterology. 129, 1753–55 (2005).
Gomm, W. et al. Association of proton pump inhibitors with risk of dementia: a pharmacoepidemiological claims data analysis. JAMA neurology. 73, 410–16 (2016).
Schoenfeld, A. J. & Grady, D. Adverse effects associated with proton pump inhibitors. JAMA internal medicine. 176, 172–74 (2016).
Moher, D., Liberati, A., Tetzlaff, J. & Altman, D. G. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Annals of internal medicine. 151, 264–69 (2009).
Author information
Authors and Affiliations
Contributions
Study concept and design: R.H. and V.C. Acquisition of data: R.H. and I.W. Interpretation of data: R.H., V.C. Figures 1–6 preparation: R.H. Tables 1–5 preparation: R.H. Appendix 1–4 preparation: R.H. Drafting of the manuscript: R.H. Critical revision of the manuscript for important intellectual content: V.C., J.W., S.W. and I.W. Administrative, technical, or material support: C.W. All authors reviewed the manuscript, agreed to all the contents and agreed the submission.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Ho, R.S.T., Chung, V.C.H., Wong, C.H.L. et al. Acupuncture and related therapies used as add-on or alternative to prokinetics for functional dyspepsia: overview of systematic reviews and network meta-analysis. Sci Rep 7, 10320 (2017). https://doi.org/10.1038/s41598-017-09856-0
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-09856-0
This article is cited by
-
Management of Abdominal Pain in Patients with Gastroparesis and Gastroparesis-Like Syndromes
Current Treatment Options in Gastroenterology (2023)
-
Efficacy of compatible acupoints and single acupoint versus sham acupuncture for functional dyspepsia: study protocol for a randomized controlled trial
Trials (2020)
-
Meridian study on the response current affected by electrical pulse and acupuncture
Nanoscale Research Letters (2020)
-
A scoping review of network meta-analyses assessing the efficacy and safety of complementary and alternative medicine interventions
Systematic Reviews (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
