
Abstract
Although intraocular pressure is the main the risk factor for the development of glaucoma, other risk factors such as vascular dysfunction might play an additional pathogenic role. Hypertriglyceridemia, which may lead to vascular dysfunction, has been implicated in the development of glaucoma. The objective of this meta-analysis was to investigate the association of triglyceride levels with the risk of glaucoma in case-control studies. Seventeen case-control studies were included investigating the difference in triglyceride levels in patients with glaucoma (N = 1 391) compared to subjects without glaucoma (N = 25 575). In random effects meta-analysis, the pooled mean triglyceride level across all studies and patients with and without glaucoma was 132.9 mg/dL (95%CI: 124.0–141.7). Patients with glaucoma had significantly higher mean triglyceride levels than patients without glaucoma (absolute difference = 14.2 mg/dL, 95%CI: 5.8–22.5, p < 0.0001). A considerable amount of heterogeneity of included studies was observed (I2 = 66.2%, heterogeneity χ2 = 47.4 on 16 degrees of freedom, p < 0.0001). In conclusion, this meta-analysis of case-control studies found that patients with glaucoma had higher mean triglyceride levels than patients without glaucoma. This finding is consistent with the concept that hypertriglyceridemia represents an additional risk factor for glaucoma. Whether this association is causal and/or might be modified by glaucoma medications remains to be investigated.
Similar content being viewed by others

Introduction
Elevated intra-ocular pressure (IOP) is the main risk factor for the development of glaucoma. However, many patients develop glaucoma despite an IOP in the normal range, and not all patients with elevated IOP develop glaucoma1. Therefore, other risk factors have been implicated in the pathogenesis of glaucoma including structural abnormalities and functional dysregulation of the vasculature supplying the optic nerve and the surrounding retinal tissue2. The presence of vascular dysfunction in glaucoma patients was recently postulated in a large clinical study, the Leuven Eye Study3.
Hypertriglyceridaemia is often seen in patients with metabolic syndrome and type 2 diabetes4. Based on recent genetic studies, triglycerides are increasingly considered to be a causal cardiovascular risk factor5,6,7. Thus, novel therapies to reduce circulating triglycerides are currently being developed8. The role of triglycerides in the pathogenesis and progression of glaucoma remains unclear. Several case-control studies report a significant association of triglycerides with glaucoma9, 10 and with intraocular pressure11, 12. However, this was not confirmed in all studies13, 14 and a recent study by Ko et al.15 even found a significant inverse relationship between high triglyceride levels and glaucoma. The objective of this meta-analysis was to investigate the association of triglyceride levels with the risk of glaucoma in case-control studies.
Results
Study characteristics
Seventeen studies were included investigating the difference in triglyceride levels in patients with glaucoma (number of patients (N) 1 391) compared to patients without glaucoma (N 25 575) (Table 1).
The largest study included 300 patients with normal tension glaucoma (NTG) and 17940 patients without glaucoma, while the smallest study included 19 patients with pseudoexfoliation glaucoma (PEX glaucoma) and 51 patients without glaucoma. Five studies included patients with primary open angle glaucoma (POAG), five studies patients with NTG, two studies patients with PEX glaucoma, two studies patients with NTG and POAG, one study patients with NTG and PEX glaucoma and two studies included all glaucoma types. Patients without glaucoma were hospital controls in six studies, community controls in four studies and not defined in seven studies (Table 2).
Triglyceride levels in patients with and without glaucoma
In random-effects meta-analysis of all 17 included studies, the mean triglyceride level pooled across studies and patients with and without glaucoma was 132.9 mg/dL (95%CI: 124.0–141.7, Table 1, Supplementary Figure 1). The mean triglyceride level strongly varied between studies (I2 = 91.9%, heterogeneity χ2 = 197.1 on 16 degrees of freedom, p < 0.0001), and ranged from 93.3 mg/dL in the study by Chiba et al. to 223.5 mg/dL in the study by Ogurel et al.
Patients with glaucoma had higher mean levels of triglycerides than patients without glaucoma. In detail, the pooled mean absolute difference in triglycerides between patients with and without glaucoma was 14.2 mg/dL in random-effects analysis (95%CI: 5.8–22.5, p < 0.0001, Fig. 1), and 13.0 mg/dL in fixed-effects analysis (95%CI: 8.9–17.0, p < 0.0001, Fig. 1). Upon inspection of study weights (gray boxes in Fig. 1), we observed that only 2 studies (Kim et al. #2. 2014, and Yilmaz et al. 2016) contributed half of the information to the pooled difference in triglycerides. On a standardized mean difference (SMD) scale, patients with glaucoma had a 0.21 standard deviations (SD) higher triglyceride level than patients without glaucoma (95%CI: 0.09–0.34, p < 0.0001, Supplementary Figure 2). The corresponding fixed-effects estimate was 0.15 SD (95%CI: 0.08–0.22, p < 0.0001). In cumulative meta-analysis, we found that significantly higher mean triglyceride levels were consistently found after the study of Lee et al., which appeared in 2012 (Fig. 2).

Random-effects meta-analysis of triglyceride level differences between patients with glaucoma and controls. The differences are expressed on an absolute scale, i.e. they represent differences in mg/dL. “I-V Overall” represents the fixed effects pooled estimate, and “D+L Overall” the random-effects pooled estimate. Grey boxed surrounding the individual study estimates are proportional to the fixed effects weight of the study. Diamonds surrounding the pooled estimates represent 95% confidence intervals. Abbreviations: 95%CI - 95% confidence interval, SD - Standard Deviation.

Cumulative meta-analysis of triglyceride level differences between patients with glaucoma and controls. Studies are sorted by calendar time. The estimates represent cumulative mean absolute differences in triglyceride levels (in mg/dL) between patients with glaucoma and controls. After the study of Lee et al., which appeared in 2012, all cumulative difference estimates indicate a statistically significantly higher average triglyceride level in glaucoma patients.
In both meta-analyses of absolute and standardized mean triglyceride differences between patients with glaucoma and controls, we observed statistically significant evidence for heterogeneity (I2 for the absolute difference analysis = 66.2%, heterogeneity χ2 = 47.4 on 16 degrees of freedom, p < 0.0001). This finding suggests that random effects estimates may be more appropriate than fixed effects estimates. Further, this relative large heterogeneity estimate is consistent with the assumption that other between-study differences may at least partly explain the overall difference in triglyceride levels between glaucoma patients and controls. To explore these potential factors, we performed a meta-regression (Table 3). In detail, we investigated the covariables age, sex, diabetes, BMI, LDL cholesterol, HDL cholesterol, total cholesterol, systolic blood pressure, diastolic blood pressure, and mean within-study triglyceride levels. None of these variables were significantly associated with the difference in triglycerides between patients with and without glaucoma, except for HDL, which was “borderline statistically significantly” associated with the triglyceride difference. However, considering that (1) meta regression has a comparably low power, (2) some covariables (e.g. diabetes, n = 5 studies) were not completely observed for all 17 studies (Tables 1, 2 and 3), and (3) the use of lipid-lowering medications was not documented in most studies (Table 2), we focussed our interpretation of meta-regression results on reductions in I2 upon adding the covariables. Here, our analysis suggested that study-level HDL cholesterol was an important modifier of the glaucoma-triglyceride-association. In detail, a 10 mg/dL increase in HDL cholesterol was associated with a 6 mg/dL reduction in the triglyceride difference between patients with and without glaucoma (Difference = −5.92, 95%CI: −12.55–0.71, p = 0.075, Fig. 3), which implies that studies with higher mean HDL cholesterol levels generally showed smaller difference in triglycerides between patients with and without glaucoma. Further evidence for this hypothesis comes from I2 estimates. In detail, addition of HDL cholesterol reduced the amount of unexplained variation in the triglyceride-glaucoma association from 30.4% to 4.2%. Diabetes may be another modifier of the triglyceride-glaucoma association, with meta-regression suggesting a higher contribution of triglycerides to glaucoma in patients that were diabetic. However, due to the small number of studies with observed diabetes data (n = 5), these results remain hypothesis-generating. In terms of within-study average triglyceride levels, we did not observe evidence for an association with triglyceride difference between glaucoma patients and controls. Studies with higher mean triglyceride levels did not appear to have a greater difference between glaucoma patients and controls than studies with lower mean triglyceride levels. Otherwise, the difference in triglycerides between patients with and without glaucoma prevailed in almost all meta-regressions (Table 3), which is consistent with the concept that elevated triglycerides may be associated with glaucoma independent of covariables such as age, sex, BMI and total cholesterol.

Random-effects meta-regression of triglyceride level differences between patients with glaucoma and controls according to within-study mean high-density-lipoprotein (HDL) levels. The red line represents a line of best fit from meta-regression. The diameter of the hollow circles reflects the weight of the individual studies in the random-effects meta-regression. The slope of the line of best fit declines with increasing HDL levels, which suggests that differences in triglyeride levels between glaucoma patients and controls are strongest in patient populations with low average HDL levels.
Discussion
In this meta-analysis of 1 391 patients with glaucoma compared to 25 575 without glaucoma included in 17 cross-sectional studies, we found higher mean triglyceride levels in patients with glaucoma as compared to controls. The pooled mean absolute difference in triglycerides between patients with and without glaucoma was 14.2 mg/dL.
The association of triglycerides and glaucoma has so far been a matter of ongoing debate. Some studies found a significant association9, 10, while other studies could not confirm this association (Table 1)13, 14. These different results are reflected by the considerable amount of heterogeneity found in this meta-analysis. One reason for this heterogeneity may be that different types of glaucoma were included in this meta-analysis (Table 2). Furthermore, inclusion criteria were different among the included studies. For example visual field defects had to be present in some but not all studies. Three studies had no definition for who was considered to be a patient with glaucoma16,17,18 and in one study patients were simply surveyed on whether they had a glaucoma19. The control groups were equally dissimilar. Six studies included hospital controls, four community controls and seven did not report on control group recruitment. Nine studies gave no definition of the inclusion criteria for the control group. Likewise, exclusion criteria were different in the included studies. This may be particularly relevant for a modifying influence of co-medications on triglyceride levels. For example, patients using lipid-lowering medication were excluded in six of the seventeen studies and included in one study, while the other ten studies did not report any data on the use of lipid-lowering medication. Moreover, diabetes mellitus, smoking and cardiovascular disease was included in some studies, excluded in others, or not reported on (Table 2).
However, not only co-medications may modify the association of triglycerides and glaucoma, but also medications used for glaucoma treatment. Importantly, topical beta-blockers, which are a cornerstone treatment for glaucoma, have been shown to increase systemic triglyceride levels in a study on 28 healthy volunteers taking topical timolol20. Given the fact that it is very likely that the patients in this meta-analysis had a high prevalence of topical beta-blocker use, this may have increased the difference in triglyceride levels between patients and controls. Therefore, future studies should address this potential bias.
In meta-regression, we found that HDL cholesterol was a modifier of the glaucoma-triglyceride-association. Specifically, studies including patients with lower average HDL cholesterol levels showed larger differences in triglyceride levels between patients with and without glaucoma. As HDL levels are known to inversely correlate with triglyceride levels suggesting a dynamic interaction4, 21, it seems rather unlikely that HDL itself is a modifier of the glaucoma-triglyceride-association. We hypothesize that lipid-lowering interventions may cause this surprising result. In a recent meta-analysis, statin use was associated with a reduced incidence of glaucoma22. Life-style interventions influencing the metabolism of HDL such as smoking, weight loss and physical activity, and the use of lipid-lowering medications are poorly reported in most studies. For example the percentage of patients using lipid-lowering medications was given in only one study23. Therefore we could not account for lipid-lowering interventions in this meta-regression.
Likewise, triglycerides appeared to have a higher contribution to glaucoma in patients with diabetes mellitus, a known risk factor for glaucoma24, 25. Ko et al.15 found that diabetes was significantly associated with glaucoma only if triglycerides were excluded from the multivariable regression model. High triglyceride levels seem to be associated with worse glycaemic control26. Zhao et al.19 could show that HbA1c levels are associated with glaucoma. Our findings of diabetes mellitus as a modifier may therefore reflect the association of glaucoma with worse glycaemic control.
In this meta-analysis triglyceride levels were significantly higher in patients with glaucoma in the random-effects analysis. A recent study by Ko15 et al. found a significant inverse correlation between high triglyceride levels and glaucoma. As no actual triglyceride levels are given by Ko15 et al., it was not included in this meta-analysis. They used a rather high cut-off at ≥200 mg/dL. As the difference in triglyceride levels in this meta-analysis was 14.2 mg/dL, differences in the percentage of high triglycerides levels using a cut-off at ≥200 mg/dL would probably not be found and this may explain this discrepancy. Further no information on the use of lipid-lowering drugs, especially fibrates, is given, which might also explain the inverse correlation.
Elevated IOP does not seem sufficient to solely explain the pathogenesis of glaucoma1. Other risk factors, especially the dysfunction of the vasculature supplying the optic nerve and the surrounding tissue, have therefore been implicated3. Triglycerides are an independent risk factor for cardiovascular disease27, although their role in the pathogenesis of atherosclerosis is controversial28. Patients diagnosed with glaucoma have been shown to have an increased risk of cardiovascular mortality29, 30, which is primarily explained by common risk factors such as hypertriglyceridemia31, 32. Glaucoma medication has also been suggested to influence lipid levels, however evidence is very limited33, 34.
Finally, we want to mention three limitations of the study. First, the current analysis only incorporates observational data. Therefore, we want to stress that although our study provides strong statistical evidence that triglycerides are associated with glaucoma, we cannot prove causality. Specifically, we cannot answer whether hypertriglyceridemia leads to glaucoma via a potential effect on intraocular pressure, or whether triglycerides may have a pathogenic impact on glaucoma independently of intraocular pressure. Second, the observational nature of the included studies does not allow us to evaluate whether interventions that lower triglyceride levels can modify glaucoma development and/or outcomes. Randomised clinical studies are needed to investigate whether the use of triglyceride-lowering drugs may be useful in the prevention or treatment of glaucoma. Preliminary evidence supporting a role for lipid-lowering drugs towards glaucoma outcomes stems from a large British registry study, in which statin use was associated with lower IOP35. This is relevant also for our meta-analysis, given the fact that statins not only lower LDL cholesterol but also triglyceride levels, which may in turn ameliorate the adverse association of triglycerides with glaucoma. Although the impact of statins on IOP did not prevail after adjusting for beta-blockers in the aforementioned study, future studies should clearly explore how lipid-lowering drugs affect triglyceride levels and their role on glaucoma development and progression. Third, we obtained convincing statistical evidence that patients with glaucoma have higher average triglyceride levels than controls. However, it remains to be investigated whether this statistically significant absolute difference of approximately 14 mg/dL is not only statistically significant but also clinically relevant. This question could be addressed by future studies, which employ a prospective design looking at clinical outcomes of glaucoma pathogenesis or glaucoma progression.
In conclusion, our meta-analysis summarizes a large body of evidence from case-control studies on the glaucoma-triglyceride association. The observed results are consistent with the concept that hypertriglyceridemia may contribute to glaucoma pathogenesis, and support the future conduct of randomized trials on triglyceride-lowering interventions for prevention or treatment of glaucoma.
Methods
Search history
From July 12th, 2014, until August 2nd, 2016, we used an Ovid Interface to search for the following medical subject headings in the databases PubMed, EMBASE, and The Cochrane Library: “glaucoma” AND “triglycerides”; “intraocular pressure” AND “triglycerides”; “glaucoma” AND “dyslipidemia”; and “intraocular pressure” AND “dyslipidemia”. The reference lists of included studies were additionally scanned to identify potentially relevant reports. Two investigators (LP & FP) performed the literature search and study selection.
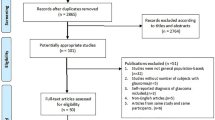
Studies were included if they reported the triglyceride levels in patients with glaucoma and compared to control patients. Only studies in English language were included. All abstracts and conference proceedings that are not published in peer-reviewed journals were excluded. If original data or exact numbers were not available, they were not included in the quantitative analysis (Fig. 4).

Prisma Flow Diagram of the study selection process. Adapted from: Moher D, Liberati A, Tetzlaff J, Altman DG, The PRISMA Group (2009). Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement.PLoS Med 6(7): e1000097. doi:10.1371/journal.pmed1000097. For more information, visit http://www.prisma-statement.org.
Statistical methods
All statistical analyses were performed using Stata (Windows version 14.0, Stata Corp., Houston, TX, USA). Differences in mean triglyceride levels between patients with and without glaucoma were analysed using random- and fixed-effects meta-analysis (Stata routine metan). Differences were analysed both on an absolute scale (i.e. difference in triglycerides between patients with and without glaucoma in mg/dL) and on a standardized scale (i.e. difference in triglycerides between the two groups in units of standard deviation (so-called standardized mean differences)). The I2 statistic was evaluated for quantifying the extent of unexplained variation in the triglyceride-glaucoma association (i.e. heterogeneity). The user-contributed suite metacum was applied for cumulative meta-analysis of absolute differences in triglyceride levels between patients with and without glaucoma. Meta-regressions were performed on the absolute scale with Stata’s user-contributed routine metareg in order to explore potential modifiers of the triglyceride-glaucoma association. The full analysis code is available on request from FP.
References
Huck, A. et al. Vascular considerations in glaucoma patients of African and European descent. Acta Ophthalmol. 92, e336–40 (2014).
Venkataraman, S. T., Flanagan, J. G. & Hudson, C. Vascular reactivity of optic nerve head and retinal blood vessels in glaucoma–a review. Microcirculation 17, 568–581 (2010).
Abegao Pinto, L. et al. Ocular blood flow in glaucoma - the Leuven Eye Study. Acta Ophthalmol. 94, 592–598 (2016).
Chapman, M. J. et al. Triglyceride-rich lipoproteins and high-density lipoprotein cholesterol in patients at high risk of cardiovascular disease: evidence and guidance for management. Eur. Heart J. 32, 1345–1361 (2011).
Do, R. et al. Exome sequencing identifies rare LDLR and APOA5 alleles conferring risk for myocardial infarction. Nature 518, 102–106 (2015).
Stitziel, N. O. et al. Coding Variation in ANGPTL4, LPL, and SVEP1 and the Risk of Coronary Disease. N. Engl. J. Med. 374, 1134–1144 (2016).
Dewey, F. E. et al. Inactivating Variants in ANGPTL4 and Risk of Coronary Artery Disease. N. Engl. J. Med. 374, 1123–1133 (2016).
Gaudet, D. et al. Antisense Inhibition of Apolipoprotein C-III in Patients with Hypertriglyceridemia. N. Engl. J. Med. 373, 438–447 (2015).
Sahinoglu-Keskek, N. et al. Metabolic syndrome as a risk factor for elevated intraocular pressure. Pakistan J. Med. Sci. 30, 477–482 (2014).
Aptel, F. et al. Short- and long-term effects on the ciliary body and the aqueous outflow pathways of high-intensity focused ultrasound cyclocoagulation. Ultrasound Med. Biol. 40, 2096–2106 (2014).
Ye, S. et al. Intraocular pressure and coronary artery calcification in asymptomatic men and women. Br. J. Ophthalmol. 99, 932–936 (2015).
Kim, Y.-H. et al. High intraocular pressure is associated with cardiometabolic risk factors in South Korean men: Korean National Health and Nutrition Examination Survey, 2008–2010. Eye (Lond). 28, 672–679 (2014).
Elisaf, M. et al. Metabolic abnormalities in patients with primary open-angle glaucoma. Acta Ophthalmol. Scand. 79, 129–132 (2001).
Kim, M. J., Kim, M. J., Kim, H. S., Jeoung, J. W. & Park, K. H. Risk factors for open-angle glaucoma with normal baseline intraocular pressure in a young population: the Korea National Health and Nutrition Examination Survey. Clin. Experiment. Ophthalmol. 42, 825–832 (2014).
Ko, F. et al. Diabetes, Triglyceride Levels, and Other Risk Factors for Glaucoma in the National Health and Nutrition Examination Survey 2005-2008. Invest. Ophthalmol. Vis. Sci. 57, 2152–2157 (2016).
Pavljasevic, S. & Asceric, M. Primary open-angle glaucoma and serum lipids. Bosn. J. Basic Med. Sci. 9, 85–88 (2009).
Chiba, T., Chiba, N. & Kashiwagi, K. Systemic arterial stiffness in glaucoma patients. J. Glaucoma 17, 15–18 (2008).
Davari, M. H., Gheitasi, H., Yaghobi, G. & Heydari, B. Correlation between serum lipids and age-related macular degeneration: a case-control study. J. Res. Health Sci. 13, 98–101 (2013).
Zhao, D., Cho, J., Kim, M. H., Friedman, D. & Guallar, E. Diabetes, glucose metabolism, and glaucoma: the 2005-2008 National Health and Nutrition Examination Survey. PLoS One 9, e112460 (2014).
Coleman, A. L., Diehl, D. L., Jampel, H. D., Bachorik, P. S. & Quigley, H. A. Topical timolol decreases plasma high-density lipoprotein cholesterol level. Arch. Ophthalmol. (Chicago, Ill. 1960) 108, 1260–1263 (1990).
Quispe, R. et al. Relationship of the triglyceride to high-density lipoprotein cholesterol (TG/HDL-C) ratio to the remainder of the lipid profile: The Very Large Database of Lipids-4 (VLDL-4) study. Atherosclerosis 242, 243–250 (2015).
McCann, P., Hogg, R. E., Fallis, R. & Azuara-Blanco, A. The Effect of Statins on Intraocular Pressure and on the Incidence and Progression of Glaucoma: A Systematic Review and Meta-Analysis. Invest. Ophthalmol. Vis. Sci. 57, 2729–2748 (2016).
Bossuyt, J. et al. Vascular dysregulation in normal-tension glaucoma is not affected by structure and function of the microcirculation or macrocirculation at rest: a case-control study. Medicine (Baltimore). 94, e425 (2015).
Song, B. J., Aiello, L. P. & Pasquale, L. R. Presence and Risk Factors for Glaucoma in Patients with Diabetes. Curr. Diab. Rep. 16, 124 (2016).
Zhou, M., Wang, W., Huang, W. & Zhang, X. Diabetes mellitus as a risk factor for open-angle glaucoma: a systematic review and meta-analysis. PLoS One 9, e102972 (2014).
Quispe, R., Martin, S. S. & Jones, S. R. Triglycerides to high-density lipoprotein-cholesterol ratio, glycemic control and cardiovascular risk in obese patients with type 2 diabetes. Curr. Opin. Endocrinol. Diabetes. Obes. 23, 150–156 (2016).
Boullart, A. C. I., de Graaf, J. & Stalenhoef, A. F. Serum triglycerides and risk of cardiovascular disease. Biochim. Biophys. Acta 1821, 867–875 (2012).
Tziomalos, K., Athyros, V. G., Karagiannis, A., Kolovou, G. D. & Mikhailidis, D. P. Triglycerides and vascular risk: insights from epidemiological data and interventional studies. Curr. Drug Targets 10, 320–327 (2009).
Yanagi, M. et al. Vascular risk factors in glaucoma: a review. Clin. Experiment. Ophthalmol. 39, 252–258 (2011).
Orzalesi, N., Rossetti, L. & Omboni, S. Vascular risk factors in glaucoma: the results of a national survey. Graefes Arch. Clin. Exp. Ophthalmol. 245, 795–802 (2007).
Tsai, J. C. Influencing ocular blood flow in glaucoma patients: the cardiovascular system and healthy lifestyle choices. Can. J. Ophthalmol. 43, 347–350 (2008).
Leske, M. C. et al. Predictors of long-term progression in the early manifest glaucoma trial. Ophthalmology 114, 1965–1972 (2007).
Stewart, W. C. & Osterman, J. Serum lipid physiology and the influence of glaucoma medications. Surv. Ophthalmol. 43, 233–244 (1998).
Mitchell, P., Wang, J. J., Cumming, R. G., House, P. & England, J. D. Long-term topical timolol and blood lipids: the Blue Mountains Eye Study. J. Glaucoma 9, 174–178 (2000).
Khawaja, A. P. et al. Systemic medication and intraocular pressure in a British population: the EPIC-Norfolk Eye Study. Ophthalmology 121, 1501–1507 (2014).
Yilmaz, N. et al. Higher serum lipids and oxidative stress in patients with normal tension glaucoma, but not pseudoexfoliative glaucoma. Bosn. J. Basic Med. Sci. 16, 21–27 (2016).
Ogurel, T., Ogurel, R., Topuz, M., Ornek, N. & Ornek, K. Plasma adropin level in patients with pseudoexfoliation. Int. Ophthalmol., doi:10.1007/s10792-016-0185-8 (2016).
Shim, S. H. et al. The Role of Systemic Arterial Stiffness in Open-Angle Glaucoma with Diabetes Mellitus. Biomed Res. Int. 2015, 425835 (2015).
Modrzejewska, M., Grzesiak, W., Zaborski, D. & Modrzejewska, A. The role of lipid dysregulation and vascular risk factors in glaucomatous retrobulbar circulation. Bosn. J. Basic Med. Sci. 15, 50–56 (2015).
Kurtul, B. E., Kurtul, A., Altiaylik Ozer, P., Kabatas, E. U. & Ertugrul, G. T. Serum Lipid Levels in Pseudoexfoliation Syndrome. Semin. Ophthalmol, 1–4, doi:10.3109/08820538.2015.1068341 (2015).
Kim, M. et al. Metabolic syndrome as a risk factor in normal-tension glaucoma. Acta Ophthalmol. 92, e637–43 (2014).
Lee, N. Y., Park, H.-Y. L., Park, C. K. & Ahn, M. D. Analysis of systemic endothelin-1, matrix metalloproteinase-9, macrophage chemoattractant protein-1, and high-sensitivity C-reactive protein in normal-tension glaucoma. Curr. Eye Res. 37, 1121–1126 (2012).
Yuki, K., Murat, D., Kimura, I. & Tsubota, K. Increased serum total antioxidant status and decreased urinary 8-hydroxy-2′-deoxyguanosine levels in patients with normal-tension glaucoma. Acta Ophthalmol. 88, e259–64 (2010).
Engin, K. N., Yemisci, B., Yigit, U., Agachan, A. & Coskun, C. Variability of serum oxidative stress biomarkers relative to biochemical data and clinical parameters of glaucoma patients. Mol. Vis. 16, 1260–1271 (2010).
Choi, J. et al. C-reactive protein and lipid profiles in Korean patients with normal tension glaucoma. Korean J. Ophthalmol. 23, 193–197 (2009).
Author information
Authors and Affiliations
Contributions
L.P. and F.P. performed the literature search and wrote the main manuscript. F.P. performed the statistical analysis. G.M., A.W., M.W., O.K. and G.S. reviewed the manuscript.
Corresponding author
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Pertl, L., Mossböck, G., Wedrich, A. et al. Triglycerides and Open Angle Glaucoma – A Meta-analysis with meta-regression. Sci Rep 7, 7829 (2017). https://doi.org/10.1038/s41598-017-08295-1
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-08295-1
This article is cited by
-
Plasma metabolite profile for primary open-angle glaucoma in three US cohorts and the UK Biobank
Nature Communications (2023)
-
Identification of critical genetic variants associated with metabolic phenotypes of the Japanese population
Communications Biology (2020)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
