
Abstract
This study is intended to find more effective and robust clinical diagnostic indices to characterize muscle strength and coordination alternation following anterior cruciate ligament (ACL) rupture. To evaluate angle-specific moments and hamstring (H)/quadriceps (Q) ratios, 46 male subjects with unilateral chronic ACL-rupture performed isokinetic concentric (c), eccentric (e) quadriceps and hamstring muscle tests respectively at 60°/s. Normalized moments and H/Q ratios were calculated for peak moment (PM) and 30°, 40°, 50°, 60°, 70°, 80° knee flexion angles. Furthermore, we introduced single-to-arithmetic-mean (SAM) and single-to-root-mean-square (SRMS) muscle co-contraction ratios, calculating them for specific angles and different contraction repetitions. Normalized PM and 40° specific concentric quadriceps, concentric hamstring strength in the ACL-deficient knee were reduced significantly (P ≤ 0.05). Concentric angle-specific moments together with Qe/Qc ratios at 40° (d = 0.766 vs. d = 0.654) identify more obvious differences than peak values in ACL ruptured limbs. Furthermore, we found SRMS-QeQc deficits at 40° showed stronger effect than Qe/Qc ratios (d = 0.918 vs. d = 0.766), albeit other ratio differences remained basically the same effect size as the original H/Q ratios. All the newly defined SAM and SRMS indices could decrease variance. Overall, 40° knee moments and SAM/SRMS ratios might be new potential diagnosis indices for ACL rupture detection.
Similar content being viewed by others
Introduction
Muscle strength is important to the health of an individual, critical for optimal performance in sports and for preventing certain serious sport-related injuries. Quadriceps strength deficits may be ubiquitous after anterior cruciate ligament (ACL) rupture and reconstruction1. The quadriceps is important for lower limb control during dynamic activity and quadriceps weakness could alter movement strategies potentiating re-injury, which may be hazardous to the patient2.
Isokinetic dynamometry-based strength evaluations both in healthy individuals and ACL-deficient (ACLD) patients allow establishment of baseline scores and progress of different phases. Most studies of muscle strength related to the ACL injury have used the peak moment as main outcome measure3,4,5. Quadriceps peak moment represents the value during knee extension where the individual could produce the highest force6. ACLD patients have shown about 14–25% quadriceps5, 7 and hamstring strength7, 8 deficits on the injured limb. However, the peak moment may give limited information about the muscle performance throughout the range of motion (ROM)9. The efficiency of muscle strength testing could be improved if the same angle could be used10. Especially, quadriceps contraction would produce a larger anterior tibial shear force when the knee flexion angle is less than 40°. Compared to the commonly used peak moment values, angle of less than 40° specific thigh muscle moment values provided more information on the strength deficits after ACL injury11. And Eitzen et al. revealed that the largest quadriceps deficits could be found at less than 40° knee angle for both potential copers and non-copers5.
The assessment of strength and strength balance about the knee has been used as an objective marker after ACL injury, reconstruction and subsequent rehabilitation. Therefore, a hamstring/quadriceps (H/Q) strength ratio based on peak moment values during a maximal voluntary contraction has traditionally been used to describe the potential for knee joint stabilization12, 13. The Hamstring concentric/Quadriceps concentric (Hc/Qc) ratios and the Hamstring eccentric/Quadriceps eccentric (He/Qe) ratios of peak moments have been studied in ACLD subjects14. Kannus reported that a greater difference of the Hc/Qc ratio between the ACLD and the sound limb was associated with a less successful outcome of rehabilitation15. However, the Hc/Qc ratio is not physiologic, because there is a wide discrepancy between the time and angle of the hamstring peak force and those of quadriceps. The peak moments generated by the knee extensors and flexors occur at about 60° and 20° of knee flexion, respectively16. In contrast to the Hc/Qc, the functional He/Qc ratio is similar to the kicking action, and the increase in the ACLD side may help the patients accomplish low intensity knee extension motion17.
Up to now, there is still few work related to the angle specific H/Q ratios, especially for ACLD patients. Aagaard et al. put forward the concept of “functional H/Q ratio”, and reported 30°, 40°, and 50° He/Qc ratio values12, 13. Coombs et al. have shown angle specific characteristics of He/Qc and Hc/Qc ratios throughout 90° range of motion14, but they did not present the optimal knee angle for analysis. Hiemstra et al. stated that the largest Hc/Qc ratio variations could be found at around 40° knee angle between normal and ACL reconstructed subjects18, yet no concentration was paid on ACLD patients. According to our previous results, the Hc/Qc, He/Qc and Qe/Qc ratios significantly changed on the ACLD side at 30° of knee flexion17. However, the optimal joint angle of the H/Q ratio which demonstrates the most obvious disparities between the healthy and ACLD limb needs to be clarified.
Moreover, muscle co-contraction should also be taken into consideration for ACL injury evaluation, due to that antagonist muscles must contract simultaneously to increase joint stability and protect ligaments during motion19. Numerous forms of indices have been introduced for muscle co-activation assessment of different joints20,21,22,23, and they are compared by Souissi et al. recently24. All of the indices have been based on muscle electromyography activities (EMG) or moments calculated by musculoskeletal models, and as has been pointed out, measurement of muscle co-contraction level based on joint moments might provide more reliable description of muscle actions24. All forms of the H/Q ratio directly compare the strength of two isolated muscle groups, however, they lack proper measurement on the simultaneous contraction strength of agonist and antagonist muscles. So new indices have been introduced in this paper based on quadriceps and hamstring muscle strength from isokinetic tests. They were computed by following the protocol of co-contraction index. Furthermore, nearly all the indices included linear combinations of muscle moments or EMG data, but nonlinear polynomial forms of cost functions have been more frequently used for solving the so-called muscle distribution problem due to the musculoskeletal system redundancy25. Therefore, the root-mean-square (RMS) form of quadriceps and hamstring muscle strength has been finally proposed to describe knee muscle coordination.
At 30° of knee flexion, which was important for knee dynamic function, there was a significant reduction in the moment of quadriceps at concentric and eccentric 60°/s produced by the deficient-side compared to the intact side17. According to our clinical experience, the H/Q ratio may demonstrate extremely high values when the quadriceps strength is close to zero. In addition, Ayala et al. determined the absolute reliability of conventional and functional H/Q ratios, and found that angle-specific H/Q ratios showed poor absolute reliability26. On the contrary, Hirai et al. have shown that the variance of muscle synergy indices of upper limbs was sufficiently small for each subject27. Therefore, it seems that new forms of robust hamstring and quadriceps muscle strength indices for decreasing standard deviation can be introduced based on the polynomial combination of hamstring and quadriceps muscle strength.
The purpose of this study was to determine the moments and ratios of the hamstring and quadriceps strength at 30°, 40°, 50°, 60°, 70°, 80° of knee flexion in 60°/s isokinetic contractions, trying to examine the differences of angle specific hamstring and quadriceps moments and muscle strength parameters between the healthy and ACLD limb, and find more robust clinical diagnosis indices to detect altered muscle coordination strategies with lower variance. We hypothesized that 30° and 40° H/Q ratios would show more effective statistical significance than peak moment H/Q values. In addition, we also hypothesized that the newly introduced angle specific muscle co-contraction indices (shown below) would reduce diversity and increase robustness than H/Q ratios.
Methods
Ethics statement and Subjects
The study protocol was approved by the Institutional Research Board of Peking University Third Hospital (IRB00006761–2013070) and the written informed consents were obtained from all subjects. This study was performed in 46 male subjects (30.1 ± 6.6 years, BMI 26.1 ± 4.0 kg/m2) with unilateral and symptomatic ACL deficiency (24 left, 22 right), who reported symptom of giving-way during pivoting or twisting activities while no symptom of pain, swelling or giving-way during straight line and level walking. Subjects were recruited to the study from the Institute of Sports Medicine, Peking University Third Hospital (Beijing, China) between June 2013 and December 2015. ACL deficiency was confirmed through physical examination by an orthopedic surgeon as well as through MRI examination. In addition, the status of each injured ACL was verified by an arthroscopic ACL reconstruction procedure. All patients had unilateral ACL rupture with minimal other tissue injuries that did not need surgical intervention. There was no history of injury, surgery or disease in the contralateral knees of the patients.
Testing Procedure
Subjective evaluation included subjective International Knee Documentation Committee (IKDC)28, Lysholm and Tegner scores29 (IKDC 66.6 ± 15.1; Lysholm score 77.5 ± 15.6; Tegner score 4.1 ± 1.6). Those evaluations were single blinded and performed by the same experimenter. Objective evaluation included isokinetic quadriceps and hamstring muscle tests.
Isokinetic muscle strength testing
Before each test, there was a 5-minute warmup cycling session (SCIFIT, American). Subjects were also asked to complete practice repetitions once or twice prior to each test series, separated by 90 seconds rest intervals. All isokinetic measurements were recorded by the same experimenter to avoid intertester variability. Isokinetic concentric and eccentric quadriceps and hamstring muscle tests in both the sound and ACLD knees were performed at 60°/s respectively, which were frequently referred to as a relevant and valid measurement for muscle performance in ACLD individuals2, 30. The reliability for isokinetic muscle testing of knee was previously reported to be adequate both for healthy subjects and for subjects with ACL deficiency31, 32.
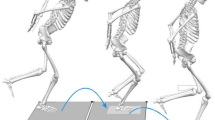
The thigh muscles of the uninvolved limbs were tested first by using an isokinetic dynamometer (Con-Trex MJ; Germany), as shown in Fig. 1. Subjects were comfortably seated on the dynamometer chair, with the hip joint at about 85° (0° = full extension). The distal shin pad of the dynamometer was attached proximal to the medial malleolus by using a strap. To minimize extraneous body movements during thigh muscle contractions, straps were applied across the chest, pelvis and mid-thigh. The alignment between the dynamometer rotational axis and the knee joint rotation axis (lateral femoral epicondyle) was checked at the beginning of each trial. Gravity effect moment was recorded on each subject throughout the range of motion and this was used to correct moment measurements during all tests. The participants were given standardized encouragement by the investigator, and were asked to position their hands on the bilateral handles on the side of the chair during the testing procedure. The ROM for the isokinetic trials was 70°, from 20° to 90° of knee flexion (0°corresponding to knee fully extended). Knee flexor and extensor trials were performed as discrete movements in both directions at a velocity of 60°/s. For both concentric and eccentric repetitions, subjects were exhorted to push/pull five continuous, reciprocal knee extensions and flexions as hard and fast as possible and to complete the full ROM.

Illustrations of isokinetic test protocol. (a) An example of the isokinetic test by a subject and (b) an illustration of knee motion and the limb muscle contraction in the isokinetic test.
Criterion measures
For concentric and eccentric strength trials, we retained two sets of parameters for each individual contraction repetition of the knee: average peak moment (PM), which referred to the average peak moment of five trials and would be less affected by the artifact than the peak moment33; the moment of quadriceps and hamstring at specific 30°, 40°, 50°, 60°, 70°, 80° of flexion. And then H/Q ratios and 6 newly introduced indices of quadriceps and hamstring muscle co-contraction strength (the detailed mathematical forms are shown in Table 1) were calculated for the PM and 30°, 40°, 50°, 60°, 70°, 80° respectively.
Data Processing
Gravity-correct measurement data from the dynamometer was slightly smoothed by fifth-order Savitzky-Golay filter with the frame size 51. This type of filter was chosen so that possible essential differences could be recorded, and at the same time the time-velocity curve could be smoothed for further use. All repetitions were used in subsequent analysis, for not all the participants performed the strongest peak moment value for the first repetition, and the majority of participants did not perform fatigue for the last one. Hamstring and quadriceps moment data of concentric and eccentric motion was respectively normalized by weight and height of each participant5, that is
and the normalized moment values (m/s2) versus knee extension-flexion angle (°) curves were then obtained from the smoothed experimental data. Several participants did not manage to move their limbs within the predefined ROM for fatigue in one or two repetitions, and these data would be moved out for further analysis. All the remained curves were normalized by the ROM of corresponding participants and projected to the predefined ROM (20°–90°) so that they can be compared with each other. The knee moments of each repetition were assumed to be linear with joint angle, and they were evenly distributed by 100 points using cubic spline interpolation. Only the data between 26°–84° was taken into consideration for average peak normalized moment (m/s2) per participant to neglect inertia effect.
Statistical Analysis
Custom-written Matlab (MathWorks, Natick, MA) programs were used to perform statistical analyses. Nonparametric statistics were calculated for the average peak knee moments, ratios of hamstring strength between ACLD side and the healthy side (HHR)/ratios of quadriceps strength between ACLD side and the healthy side (QQR), H/Q ratios, the newly introduced SAM indices and the SRMS indices at 30°, 40°, 50°, 60°, 70°, 80° of knee flexion34. Firstly, the experimental data and computed ratios were checked for homogeneity of variance using Bartlett’s test. Then, a Friedman ANOVA by Ranks was chosen to assess whether there were significant differences in average peak knee moments, HHR/QQR ratios, H/Q ratios, SAM indices and SRMS indices35. It was also applied to detect differences among the values of the above variables by angle. When Friedman’s test was significant, the next step was to perform Wilcoxon signed Rank-test as post hoc analyses. The significance level was set as P < 0.05. Furthermore, Cohen’s d (d) was used as a measure of effect size.
Results
Average normalized moment-angle characteristics
In the case of concentric motion (Table 2), there was a significant difference in the mean normalized moment values between ACLD and the uninvolved limb for both extension and flexion motion. Post hoc analysis revealed that the extension normalized moment in ACLD knees decreased remarkably at all the angles (P < 0.010, QQR < 0.85). Normalized moment differences of knee flexion were smaller by angle (HHR < 0.85 for above 60°), and no significant differences were identified for 30° (P = 0.092, HHR = 0.92). In eccentric contraction mode (Table 2), no significant differences were identified for knee extension (P > 0.050), and the ACLD side was 13%-19% lower than the healthy side (QQR ≥ 0.85). There were statistically significant differences of normalized mean moment between the two sides at 80° knee flexion (P = 0.040), yet at other angles there was no significant difference (HHR ≥ 0.85, P ≥ 0.179) (see Supplementary Fig. S1).
H/Q ratio values
The difference in Qe/Qc ratios between the healthy and ACLD knees was obviously discernible at 30°, 40°, 50° and 60° (P ≤ 0.032, Table 3), and the effect size at 40° (d = 0.766) and 50° (d = 0.739) was larger than the average peak moment Qe/Qc ratios (d = 0.654). A clear increase of the Hc/Qc ratios in the ACLD limbs (Table 3) can be observed in the average peak value (P = 0.032, d = 0.698), yet a fairly less remarkable change of the Hc/Qc ratios was observed at 30° and 40°knee angle (P ≤ 0.021, d ≥ 0.646), essentially consistent with the previously presented characteristics of H/Q ratios. The ACLD He/Qc deficit was significant at 30° and 40° (P ≤ 0.032, d ≥ 0.529), but the difference of the average peak moment He/Qc ratios was not significant (P = 0.080, Table 3). Regardless of the knee angle, one can observe high diversity of the H/Q ratio values (Fig. 2).

Mean values and standard error (s.e.m.) plot of H/Q ratio, SAM and SRMS indices. (a) The Qe/Qc, SAM-QeQc and SRMS-QeQc indices; (b) the Hc/Qc, SAM-HcQc and SRMS-HcQc indices; (c) the He/Qc, SAM-HeQc and SRMS-HeQc indices. SAM, single-to-arithmetic-mean form indices; SRMS, single-to-root-mean-square form indices; h, healthy limb (in solid lines); d, ACLD limb (in dashed lines).
SAM/SRMS muscle strength indices
The generalized SAM/SRMS form QeQc indices showed marked increase in the ACLD limb at 30°–60° knee angle, extremely significant for SRMS-QeQc at 40° and 50°(P < 0.01, d ≥ 0.892). And the effect size of the corresponding average peak value ratios (d ≤ 0.813) was lower than that at 40° and 50° (d ≥ 0.867). As for SAM-HeQc and SRMS-HeQc ratio, significant differences were noticeable at 30°, 40° and 50°(P < 0.031, d ≥ 0.552), whereas no discernable decrease could be observed of the corresponding average peak moment ratios (P ≥ 0.053). Furthermore, the SAM-HcQc and SRMS-HcQc ratios presented a significant increase at ACLD side at 30° and 40° (P ≤ 0.029). And the effect size of the average peak moment ratio (d = 0.706) was still lower than the indices at the 30° of knee flexion (d = 0.723). Of note is that the variance of SAM and SRMS ratios was obviously decreased in the whole ROM (shown in Fig. 2), meaning a marked increase of robustness (Table 4).
Discussion
The objective of this study was to investigate the angle-specific moments, H/Q ratios and newly introduced muscle strength indices, which were important for knee dynamic function following unilateral ACL rupture17. Our hypotheses were basically supported by the results. At concentric mode, ACLD individuals revealed the largest quadriceps strength deficits for the injured limbs at less than 40° knee angle. Compared with related peak values, the Qe/Qc ratio change of ACL ruptured limbs was more obvious at 40° knee angle, while He/Qc ratios remained the same effect size. Moreover, the most evident diagnostic ratios among all the muscle co-contraction strength indices listed would be SRMS-QeQc ratios at 40° knee angle (d = 0.918) in statistical sense.
Contrary to common belief, the average quadriceps peak moment of concentric motion was almost the same as the eccentric average peak moment values, yet similar phenomenon had been reported as a special case in literature36. Comparing relative muscle strength values between the injured and the uninjured limb, the largest deficits of concentric quadriceps strength were established for less than 40° of knee flexion, in consistent with the literature17. The validity of the widespread use of the peak moment as the only measurement criterion was called into question by such an outcome. During isokinetic or isometric extension exercises, the peak ACL forces occurred at knee angles of around 35°37. And the peak anterior tibial shear force, referring to the maximal value of the resultant joint shear force in the anterior direction38, occurred at about 37° knee flexion during the jump landing task which is a common functional activity inherent to many sports and has been identified as a mechanism for non-contact ACL injury39. The contraction force of the quadriceps muscle during knee extension produced substantial anterior directed shear of the tibia relative to the femur at extended joint angles40. This shear can be counteracted not only by the ACL but also by hamstring coactivation40. Thus, low muscle strength of the hamstring relative to quadriceps has been proposed to increase the risk of noncontact knee joint injuries12, which was the original intention of introducing the H/Q ratio.
The H/Q ratio has been used as a guideline for managing strength training or injury rehabilitation by assessing changes in the ratios after training or injury41. The average peak moment Hc/Qc ratio and He/Qe ratio have been studied in ACLD subjects15. A greater difference between the peak moment Hc/Qc ratio of the injured and sound knee was associated with a less successful outcome of rehabilitation. A peak moment Hc/Qc ratio of 0.6 has been usually regarded as normative data33. But in our study, the average value of this ratio for the healthy limb was 0.69, partly because ACL injury could also affect its opposite side, resulting in bilateral quadriceps activation deficits after ACL injury40. Quadriceps contraction would probably increase tibial translation in the sagittal unstable knee, but hamstring contraction could reduce tibial translation42. An elevated H/Q ratio resulting from diminished quadriceps strength may indicate better H/Q strength balance. However, quadriceps weakness has been proven to be strongly associated with altered biomechanics in gait43 and may be linked to the pathogenesis of posttraumatic osteoarthritis44.
It has recently been suggested that the agonist-antagonist strength relationship for knee extension and flexion may be better described by a functional He/Qc or Hc/Qe ratio compared to conventional ratios (e.g. Hc/Qc or He/Qe)12. However, peak moment may give limited information about the muscle performance during the full selected range of motion9. While Qe peak moment generated for testing at 60°/s was attained at 73°, Hc peak moment was attained at 31°38. These findings illustrated the limitations of using peak moment to predict loading during functional activities38, although the peak moment He/Qc increase was fairly higher than angle-specific values. Therefore, our research focused on functional He/Qc ratios at 30°–50° of knee flexion which could be important for knee dynamic function. Functional He/Qc ratio deficit of the ACLD limb was only noticeable at 30° and 40°, yet the decrease in the peak moment He/Qc only showed marginally significant difference (P = 0.080), in consistence with the findings of Gibson et al.45. Moreover, Aagaard et al. only examined the He/Qc ratio below 50° of knee flexion, and hold the view that its value should be always above 1.012, while our findings have shown that the He/Qc ratios for both the uninvolved and the ACLD limb were all below 1.0 at flexed knee joint position (≥60°). It was due to elongated force-length conditions for the quadriceps and shortened one for hamstring at flexed knee joint angles. These values may well reflect the real contraction force-length properties for the knee muscles, and may elucidate the change of the hamstring and quadriceps biomechanical profiles following ACL rupture.
Moreover, the Qe/Qc, Hc/Qc, and He/Qc indices of both average peak moment and the 30°, 40°, and 50° angle-specific moments were at least marginally significantly increased (P ≤ 0.080) on the ACLD side. These findings agree with numerous previous studies7, 8, 17, 43, 46 but disagree with others45. Differences in patient characteristics, especially different isokinetic dynamometers, confound direct comparisons among studies. For example, gravity correction was not used on the Kin-Com dynamometer, but in our study, gravity effect was corrected throughout the range of motion during all tests. Furthermore, there still have been debates about the menstrual cycle effects on the biomechanical profiles of women with ACL injury. Bell et al.47 highlighted gender difference on ACL reconstruction, yet Chaudhari et al.48 reported that hormone cycling in women did not affect knee joint biomechanics. Therefore, our study was confined to the use of male subjects to avoid any potential variability associated with gender effects.
Another interesting finding of this study was two new versions of muscle co-contraction indices with less variance and more clinical accuracy, compared with the H/Q ratio. The H/Q ratio depended on many factors35, and the values of this ratio therefore had a fairly wide range (shown in Fig. 2), especially when some participants had severe muscle weakness in one of their limbs. Such numerical fluctuation could lead to clinical unreliability of the indices. Therefore, this led to our research of novel indices of hamstring and quadriceps co-activation. The geometric meanings of the novel indices were shown in Fig. 3. The H/Q ratio was a tangent function of the triangle ∠A′ CC′, which would become singularity when α approximates to 90°. At this time, the quadriceps strength tested by isokinetic concentric motion would come close to zero. In order to avoid similar circumstances, another tangent function, tanα′ of the triangle ∠ABC′, was introduced to replace the original one. Taking SAM-HeQc as an example, the denominator of the He/Qc ratio was replaced by the arithmetic mean of the hamstring and quadriceps strength, preventing possible singularity. Another method of eliminating singularity was to change the mathematical form of trigonometric function by using sinusoidal function. The SAM/SRMS form QeQc, HcQc, and HeQc indices of both average peak moment and the 30°, 40°, and 50° angle-specific moments were at least marginally significantly increased (P ≤ 0.10) on the ACLD side, consistent with the conventional one, and this procedure could decrease the ranges evidently, supporting such an approach.

Relationship among different knee muscle strength indices. (a) Geometric description of the H/Q ratio and the SAM/SRMS ratios. He, hamstring eccentric contraction; Qc, quadriceps concentric contraction. (b) Illustration of knee flexion and extension motion. Flx, knee flexion; Ext, knee extension; H, healthy limb; I, ACLD limb; Qe, quadriceps eccentric contraction; Hc, hamstring concentric contraction. (c) Illustration of quadriceps and hamstring strength in concentric and eccentric modes. Quad, quadriceps; Hams, hamstring.
In the computational biomechanics field, muscle recruitment of the musculo-skeletal system can be determined by an optimization problem, where the “polynomial criteria” was often used as the cost function49. The polynomial criteria can be interpreted as minimizing weighted average of muscle forces, and the mathematical form is
where n (M) is the number of muscles, \({f}_{i}^{(M)}\) are the muscle forces, N i are the normalization factors, and p is the power exponent. This criterion has important implications for rehabilitation and surgical planning. Quadriceps and hamstring are the main agonist-antagonist muscle groups that coexist in knee extension motion. According to equation (2), the arithmetic mean (AM) and the root mean square (RMS) values of hamstring eccentric and quadriceps concentric muscle strength (He + Qc or He2 + Qc2) might be two acceptable muscle cost functions. They both predict synergistic muscle behavior, for the linear combination (p = 1) is a measurement of the limb endpoint stiffness23, 50, and the quadratic cost function (p = 2) tends to minimize endpoint positional errors25. After ACL injury, the constraints of knee mechanical system are diminished especially at extended knee joint motion36, resulting in the decrease of knee cost function and changed muscle co-activation strategies. Similarly, from our aspect of view, such a cost function can be extended to assess a single muscle group function. For example, quadriceps has two fundamental functions: concentric contraction for voluntary extension and eccentric contraction for flexion stability. According to the literature, ACL rupture could evoke neurophysiological abnormality in quadriceps, leading to its atrophy and activation failure43. Muscle strength deficit may lead to quadriceps strength rebalance between such two functions, similar to the muscle residual force enhancement phenomenon, which has been regarded as a combination between an active and a passive component51, 52. Therefore, the AM and RMS average of concentric and eccentric quadriceps strength (Qe + Qc or Qe2 + Qc2) could be a reasonable evaluating indicator for muscle biomechanical dysfunction. In fact, Qe/Qc ratio has already been proved a more valid index of muscular imbalance than Hc/Qc53. Compared with the H/Q ratio, SAM and SRMS formed ratios measured voluntary/passive muscle captivity in related single muscle (QeQc) or muscle group function (HeQc) cost, directly associated with the rehabilitation16.
The relationship among various angle-specific indices of quadriceps and hamstring strength was shown in Fig. 3. Figure 3(a) illustrated the knee muscle functional differences between healthy limbs and ACLD limbs, in which quadriceps strength was used as abscissa against hamstring strength as ordinate. As for knee extension, the slope of Qc-He curve He/Qc (tanα) was above 1 at below 40° knee angle for healthy limbs, yet the threshold knee angle value was up to 52° for ACLD limbs. The more even change of He/Qc ratios for ACLD limbs (Table 3) resulted in the relatively smoothness of the ACLD Qc-He curve (Fig. 3), similar to the phenomenon of ACL reconstructed subjects shown in literature19. The same analysis method was also applicable to knee flexion motion, but at this time Qe-Hc curves for both healthy and ACLD limbs were geometrically more similar. Figure 3(b) was an illustration of quadriceps and hamstring muscle strength abilities. In this case, muscle strength in concentric mode was used as abscissa, and eccentric strength as ordinate. Both Qc-Qe and Hc-He curves have shown a sharp turning point, almost coincident with the maximum Qe2 + Qc2 and He2 + Hc2 points. We found that the maximum Qe2 + Qc2 strength occurred at 63° knee angle for healthy limbs, albeit 62° for ACLD ones. However, the maximum He2 + Hc2 strength was found at 43° knee angle for both healthy and ACLD limbs. The turning points were in consistent with the optimal knee angles with maximum quadriceps and hamstring strength respectively (Table 3), which meant that this criteria was a good combination of isokinetic concentric and eccentric muscle strength. In a word, the protocol shown in Fig. 3(b,c) could be an auxiliary method of qualitatively measuring muscle dysfunction of ACLD patients.
To minimize the variance which could confound the results, our patients were male and recruited from the same department. However, several limitations should be considered when interpreting our results. First, the small sample size (N = 46) was acknowledged, and it was recognized that this may have impacted the large variability in the test results. Second, no control group of healthy subjects was included in this study. Even though the sound leg as control has been an established approach when evaluating deficits after ACL injury34, 54. Other studies suggested that neuromuscular dysfunction and quadriceps strength loss after ACL injury also affect the sound side55. Furthermore, ACL injury occurs at a higher rate in females than males due to neuromechanical characteristics between sexes. Including a sound control group of both sexes would therefore enhance our understanding of the isokinetic quadriceps strength profiles of the ACL injury.
Conclusion
In conclusion, concentric angle-specific quadriceps muscle moments and the Qe/Qc ratios at 40° knee angle demonstrated more significant deficits at ACLD side than the conventional used peak moment values. In addition, the newly defined SAM and SRMS muscle co-contraction strength indices could evidently enhance statistical robustness than the ordinary H/Q ratios by eliminating numerical singularity. Furthermore, among all indices, SRMS QeQc ratios have shown the strongest differences between the healthy and ACLD limbs with the largest effect size. These results suggested that, in isokinetic 60 °/s mode, thigh muscle strength deficits and change of SRMS QeQc indices at 40° of knee flexion might be used in documenting muscle function of ACLD patients.
References
Urbach, D., Nebelung, W., Weiler, H. T. & Awiszus, F. Bilateral deficit of voluntary quadriceps muscle activation after unilateral ACL tear. Med. Sci. Sports Exerc. 31, 1691–1696 (1999).
Keays, S. L., Bullock-Saxton, J. E., Newcombe, P. & Keays, A. C. The relationship between knee strength and functional stability before and after anterior cruciate ligament reconstruction. J. Orthop. Res. 21, 231–237 (2003).
Almosnino, S. et al. Principal component modeling of isokinetic moment curves for discriminating between the injured and healthy knees of unilateral ACL deficient patients. J. Electromyogr. Kinesiol. 24, 134–143 (2014).
Piontek, T. et al. Arthroscopically assisted combined anterior and posterior cruciate ligament reconstruction with autologous hamstring grafts-isokinetic assessment with control group. PLoS One 8, e82462 (2013).
Eitzen, I., Eitzen, T. J., Holm, I., Snyder-Mackler, L. & Risberg, M. A. Anterior cruciate ligament-deficient potential copers and noncopers reveal different isokinetic quadriceps strength profiles in the early stage after injury. Am. J. Sports Med. 38, 586–593 (2010).
Tsepis, E., Giakas, G., Vagenas, G. & Georgoulis, A. Frequency content asymmetry of the isokinetic curve between ACL deficient and healthy knee. J. Biomech. 37, 857–864 (2004).
Tsepis, E., Vagenas, G., Ristanis, S. & Georgoulis, A. D. Thigh muscle weakness in ACL-deficient knees persists without structured rehabilitation. Clin. Orthop. Relat. Res. 450, 211–218 (2006).
Tsepis, E., Vagenas, G., Giakas, G. & Georgoulis, A. Hamstring weakness as an indicator of poor knee function in ACL-deficient patients. Knee Surg. Sports Traumatol. Arthrosc. 12, 22–29 (2004).
Wilk, K. E., Romaniello, W. T., Soscia, S. M., Arrigo, C. A. & Andrews, J. R. The relationship between subjective knee scores, isokinetic testing, and functional testing in the ACL-reconstructed knee. J. Orthop. Sports Phys. Ther. 20, 60–73 (1994).
Krishnan, C. & Williams, G. N. Effect of knee joint angle on side-to-side strength ratios. J Strength Cond Res 28, 2981–2987 (2014).
Patel, R. R., Hurwitz, D. E., Bush-Joseph, C. A., Bach, B. R. Jr & Andriacchi, T. P. Comparison of clinical and dynamic knee function in patients with anterior cruciate ligament deficiency. Am. J. Sports Med. 31, 68–74 (2003).
Aagaard, P., Simonsen, E. B., Magnusson, S. P., Larsson, B. & Dyhre-Poulsen, P. A new concept for isokinetic hamstring: quadriceps muscle strength ratio. Am. J. Sports Med. 26, 231–237 (1998).
Aagaard, P., Simonsen, E. B., Trolle, M., Bangsbo, J. & Klausen, K. Isokinetic hamstring/quadriceps strength ratio: influence from joint angular velocity, gravity correction and contraction mode. Acta Physiol. Scand. 154, 421–427 (1995).
Coombs, R. & Garbutt, G. Developments in the use of the hamstring/quadriceps ratio for the assessment of muscle balance. J Sports Sci Med 1, 56–62 (2002).
Kannus, P. Ratio of hamstring to quadriceps femoris muscles’ strength in the anterior cruciate ligament insufficient knee. Relationship to long-term recovery. Phys. Ther. 68, 961–965 (1988).
Hiemstra, L. A., Webber, S., MacDonald, P. B. & Kriellaars, D. J. Knee strength deficits after hamstring tendon and patellar tendon anterior cruciate ligament reconstruction. Med. Sci. Sports Exerc. 32, 1472–1479 (2000).
Hong-shi, H. et al. Effect of anterior cruciate ligament rupture on hamstring:quadriceps ratio during isokinetic knee extension and flexion at 30 degrees of flexion. Journal of Peking University (Health Sciences) 47, 787–790 (2015).
Hiemstra, L. A., Webber, S., MacDonald, P. B. & Kriellaars, D. J. Hamstring and quadriceps strength balance in normal and hamstring anterior cruciate ligament-reconstructed subjects. Clin. J. Sport Med. 14, 274–280 (2004).
O’Connor, J. J. Can muscle co-contraction protect knee ligaments after injury or repair. J. Bone Joint Surg. Br. 75, 41–48 (1993).
Falconer, K. & Winter, D. A. Quantitative assessment of co-contraction at the ankle joint in walking. Electromyogr. Clin. Neurophysiol. 25, 135–149 (1985).
Hesse, S., Brandl-Hesse, B., Seidel, U., Doll, B. & Gregoric, M. Lower limb muscle activity in ambulatory children with cerebral palsy before and after the treatment with Botulinum toxin A. Restor. Neurol. Neurosci. 17, 1–8 (2000).
Unnithan, V. B., Dowling, J. J., Frost, G., Volpe, A. B. & Bar-Or, O. Cocontraction and phasic activity during GAIT in children with cerebral palsy. Electromyogr. Clin. Neurophysiol. 36, 487–494 (1996).
Latash, M. L. Evolution of Motor Control: From Reflexes and Motor Programs to the Equilibrium-Point Hypothesis. J Hum Kinet 19, 3–24 (2008).
Souissi, H., Zory, R., Bredin, J. & Gerus, P. Comparison of methodologies to assess muscle co-contraction during gait. J. Biomech. 57, 141–145 (2017).
Prilutsky, Z. V. M. Biomechanics of Skeletal Muscles. Human Kinetics Publishers (2012).
Ayala, F., De Ste Croix, M., de Baranda P., S. & Santonja, F. Absolute reliability of hamstring to quadriceps strength imbalance ratios calculated using peak torque, joint angle-specific torque and joint ROM-specific torque values. Int. J. Sports Med. 33, 909–916 (2012).
Hirai, H. et al. On the Origin of Muscle Synergies: Invariant Balance in the Co-activation of Agonist and Antagonist Muscle Pairs. Front Bioeng Biotechnol 3, 192 (2015).
Fu, S. N. & Chan, Y. H. Translation and validation of Chinese version of International Knee Documentation Committee Subjective Knee Form. Disabil. Rehabil. 33, 1186–1189 (2011).
Huang, H. et al. Translation, Validation and Cross-Cultural Adaptation of a Simplified-Chinese Version of the Tegner Activity Score in Chinese Patients with Anterior Cruciate Ligament Injury. PLoS One 11, e0155463 (2016).
Probst, M. M., Fletcher, R. & Seelig, D. S. A comparison of lower-body flexibility, strength, and knee stability between karate athletes and active controls. J Strength Cond Res 21, 451–455 (2007).
Ross, M. D., Irrgang, J. J., Denegar, C. R., McCloy, C. M. & Unangst, E. T. The relationship between participation restrictions and selected clinical measures following anterior cruciate ligament reconstruction. Knee Surg. Sports Traumatol. Arthrosc. 10, 10–19 (2002).
Sole, G., Hamren, J., Milosavljevic, S., Nicholson, H. & Sullivan, S. J. Test-retest reliability of isokinetic knee extension and flexion. Arch. Phys. Med. Rehabil. 88, 626–631 (2007).
Dvir, Z. Isokinetics: Muscle Testing, Interpretation and Clinical Applications. 2e ed. Churchill Livingstone, p.39 (2004).
Hole, C. D. et al. Dynamic control and conventional strength ratios of the quadriceps and hamstrings in subjects with anterior cruciate ligament deficiency. Ergonomics 43, 1603–1609 (2000).
Czaplicki, A., Jarocka, M. & Walawski, J. Isokinetic Identification of Knee Joint Torques before and after Anterior Cruciate Ligament Reconstruction. PLoS One 10, e0144283 (2015).
Trudelle-Jackson, E., Meske, N. B., Highgenboten, C. & Jackson, A. W. Eccentric/Concentric torque deficits in the quadriceps muscle. J. Orthop. Sports Phys. Ther. 11, 142–145 (1989).
Toutoungi, D. E., Lu, T. W., Leardini, A., Catani, F. & O’Connor, J. J. Cruciate ligament forces in the human knee during rehabilitation exercises. Clin Biomech (Bristol, Avon) 15, 176–187 (2000).
Bennett, D. R. et al. The relationship between anterior tibial shear force during a jump landing task and quadriceps and hamstring strength. Clin Biomech (Bristol, Avon) 23, 1165–1171 (2008).
Griffin, L. Y. et al. Understanding and preventing noncontact anterior cruciate ligament injuries: a review of the Hunt Valley II meeting, January 2005. Am. J. Sports Med. 34, 1512–1532 (2006).
More, R. C. et al. Hamstrings–an anterior cruciate ligament protagonist. An in vitro study. Am. J. Sports Med. 21, 231–237 (1993).
Bennell, K. et al. Isokinetic strength testing does not predict hamstring injury in Australian Rules footballers. Br. J. Sports Med. 32, 309–314 (1998).
Anderson, J. L. et al. Changes in muscle torque following anterior cruciate ligament reconstruction: a comparison between hamstrings and patella tendon graft procedures on 45 patients. Acta Orthop. Scand. 73, 546–552 (2002).
Williams, G. N., Buchanan, T. S., Barrance, P. J., Axe, M. J. & Snyder-Mackler, L. Quadriceps weakness, atrophy, and activation failure in predicted noncopers after anterior cruciate ligament injury. Am. J. Sports Med. 33, 402–407 (2005).
Segal, N. A. et al. Quadriceps weakness predicts risk for knee joint space narrowing in women in the MOST cohort. Osteoarthr. Cartil. 18, 769–775 (2010).
St, C. G. A., Lambert, M. I., Durandt, J. J., Scales, N. & Noakes, T. D. Quadriceps and hamstrings peak torque ratio changes in persons with chronic anterior cruciate ligament deficiency. J. Orthop. Sports Phys. Ther. 30, 418–427 (2000).
Eastlack, M. E., Axe, M. J. & Snyder-Mackler, L. Laxity, instability, and functional outcome after ACL injury: copers versus noncopers. Med. Sci. Sports Exerc. 31, 210–215 (1999).
Bell, D. R. et al. Jump-landing biomechanics and knee-laxity change across the menstrual cycle in women with anterior cruciate ligament reconstruction. J Athl Train 49, 154–162 (2014).
Chaudhari, A. M. et al. Knee and hip loading patterns at different phases in the menstrual cycle: implications for the gender difference in anterior cruciate ligament injury rates. Am. J. Sports Med. 35, 793–800 (2007).
Rasmussen, J., Damsgaard, M. & Voigt, M. Muscle recruitment by the min/max criterion–a comparative numerical study. J. Biomech. 34, 409–415 (2001).
Hang, P., Ariga, Y., Tominaga, K., Oku, T. & Nakayama, K. Extraction and implementation of muscle synergies in neuro-mechanical control of upper limb movement. Advanced Robotics 28, 745–757 (2014).
Herzog, W., Lee, E. J. & Rassier, D. E. Residual force enhancement in skeletal muscle. J. Physiol. (Lond.) 574, 635–642 (2006).
Seiberl, W., Hahn, D. & Paternoster, F. K. Reduced activation in isometric muscle action after lengthening contractions is not accompanied by reduced performance fatigability. Sci Rep 6, 39052 (2016).
Kellis, E. & Baltzopoulos, V. Isokinetic eccentric exercise. Sports Med. 19, 202–222 (1995).
Petschnig, R., Baron, R. & Albrecht, M. The relationship between isokinetic quadriceps strength test and hop tests for distance and one-legged vertical jump test following anterior cruciate ligament reconstruction. J. Orthop. Sports Phys. Ther. 28, 23–31 (1998).
Konishi, Y. et al. Relationship between quadriceps femoris muscle volume and muscle torque after anterior cruciate ligament repair. Scand. J. Med. Sci. Sports 17, 656–661 (2007).
Acknowledgements
The authors thank Professor Yajun Yin, Yan Xu, Qinwei Guo for their fruitful discussions and suggestions. The work in this manuscript was supported by Beijing Nova Program Interdisciplinary Cooperation Project (xxjc201705) and the Seeding Grant for Medicine and Information Sciences of Peking University (BMU20160590).
Author information
Authors and Affiliations
Contributions
Conceived and designed the experiments: Hongshi Huang, Yingfang Ao. Performed the experiments: Hongshi Huang, Jianqiao Guo, Jie Yang. Analyzed the data: Hongshi Huang, Jianqiao Guo, Yanfang Jiang. Contributed reagents/materials/analysis tools: Hongshi Huang, Jianqiao Guo, Yanfang Jiang, Yuanyuan Yu. Wrote the paper: Hongshi Huang, Jianqiao Guo, Yanfang Jiang, Steffen Müller, Gexue Ren,Yingfang Ao. Designed the software used in analysis: Hongshi Huang, Jianqiao Guo, Gexue Ren.
Corresponding authors
Ethics declarations
Competing Interests
The authors declare that they have no competing interests.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Huang, H., Guo, J., Yang, J. et al. Isokinetic angle-specific moments and ratios characterizing hamstring and quadriceps strength in anterior cruciate ligament deficient knees. Sci Rep 7, 7269 (2017). https://doi.org/10.1038/s41598-017-06601-5
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41598-017-06601-5
This article is cited by
-
Hamstrings force-length relationships and their implications for angle-specific joint torques: a narrative review
BMC Sports Science, Medicine and Rehabilitation (2022)
-
Strength and Power Training in Rehabilitation: Underpinning Principles and Practical Strategies to Return Athletes to High Performance
Sports Medicine (2020)
-
Detecting the presence of anterior cruciate ligament injury based on gait dynamics disparity and neural networks
Artificial Intelligence Review (2020)
-
Modeling muscle wrapping and mass flow using a mass-variable multibody formulation
Multibody System Dynamics (2020)
-
Alternative Methods of Determining Hamstrings-to-Quadriceps Ratios: a Comprehensive Review
Sports Medicine - Open (2019)
Comments
By submitting a comment you agree to abide by our Terms and Community Guidelines. If you find something abusive or that does not comply with our terms or guidelines please flag it as inappropriate.
