
Abstract
The COVID-19 pandemic has sparked unprecedented public health and social measures (PHSM) by national and local governments, including border restrictions, school closures, mandatory facemask use and stay at home orders. Quantifying the effectiveness of these interventions in reducing disease transmission is key to rational policy making in response to the current and future pandemics. In order to estimate the effectiveness of these interventions, detailed descriptions of their timelines, scale and scope are needed. The Health Intervention Tracking for COVID-19 (HIT-COVID) is a curated and standardized global database that catalogues the implementation and relaxation of COVID-19 related PHSM. With a team of over 200 volunteer contributors, we assembled policy timelines for a range of key PHSM aimed at reducing COVID-19 risk for the national and first administrative levels (e.g. provinces and states) globally, including details such as the degree of implementation and targeted populations. We continue to maintain and adapt this database to the changing COVID-19 landscape so it can serve as a resource for researchers and policymakers alike.
Measurement(s) | Public Health • Preventive Intervention |
Technology Type(s) | digital curation |
Factor Type(s) | country • date |
Sample Characteristic - Location | global |
Machine-accessible metadata file describing the reported data: https://doi.org/10.6084/m9.figshare.12724058
Similar content being viewed by others


Background & Summary
Since the first reported cases in December 20191, Coronavirus Disease 2019 (COVID-19) has become a global pandemic and a major cause of morbidity and mortality. Due to high population susceptibility and the lack of effective therapeutics and vaccines to treat or prevent this emerging disease, many healthcare systems have been overwhelmed by a global surge in cases. In an effort to limit the transmission of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and mitigate its impact on public health, national and local governments worldwide have instituted a variety of public health and social measures (PHSM, often also referred to as non-pharmaceutical interventions, NPIs) in different combinations, of varying durations, and at different time points during their epidemic trajectories. This heterogeneity serves as a natural testing bed to characterize the effectiveness and impact of different interventions on SARS-CoV-2 transmission2. As a clearer picture of SARS-CoV-2 transmission dynamics emerges, public health experts and policy makers are now tasked with issuing informed and urgently needed recommendations for the easing of certain restrictions, many of which are associated with significant social and economic costs.
The Health Intervention Tracking for COVID-19 (HIT-COVID) project seeks to fill a critical knowledge gap through systematic collection of PHSM data at national and sub-national levels worldwide, HIT-COVID compliments other intervention tracking efforts that have tended to capture only national policies, focus primarily on middle and/ upper income countries or use less structured approaches to data collection3,4,5,6,7. We aim to provide the resolution required for robust epidemiologic study, which may in turn inform policy makers at a national, sub-national, and local level. The project, which has mobilized an international team of trained data collectors using standardized field definitions and data collection processes, has come with careful curation and internal auditing of policy dates and source documents for optimal transparency. HIT-COVID also collections information on whether missing data truly reflect an absence of policy interventions. As the current pandemic unfolds, HIT-COVID may also provide the data necessary to analyze historical trends in disease transmission, which may be important for current and future policy making, research, and education.
Methods
We collected information on PHSM policies related to COVID-19 worldwide at the national and first administrative (e.g. provinces, states) levels, with finer geographic resolution data for specific countries, including counties in the United States of America. We focused primarily on interventions that may have direct and quantifiable impacts on disease transmission, and limited data collection to government-level policy changes. We collected information on policies using a classification system adapted from the WHO PHSM Database7: (1) restrictions of travel and movement, (2) social and physical distancing measures, (3) surveillance and response measures, and (4) other measures, including military and police deployment, state of emergency declarations, and mandatory mask use (Table 1).
In order to collect these data, we recruited a global network of over 200 volunteer data contributors, primarily through professional and social networks associated with academic institutions of the management team. Upon agreeing to contribute to this project, volunteers were (1) assigned to follow and document policy changes for a specific country or administrative unit, (2) invited to attend an orientation meeting, which we held on a weekly basis for new recruits, (3) provided training materials including videos and written documentation on the expected workflow and nuances of data collection, (4) provided data entry templates and step-by-step instructions via emails, and (5) invited to an online social network for this project (www.slack.com) where they could ask and answer questions and interact with other members of the HIT-COVID team. This on-boarding process is summarized in our Data Entry Manual (Supplementary File 1).
We tracked the implementation of these interventions over time by asking contributors to submit an update each time a policy changed (Fig. 1). For each update, contributors collected the date of the update and the current status of the intervention, including whether the policy was recommended or required, and whether it was applied to the entire population or a subpopulation. In order to improve data quality and auditability, we also required an uploaded source document for each update (e.g., executive order, press release, or website screen capture).

Schematic of data collection for an example administrative unit. Each point represents a date of policy change. Colors represent the degree or intensity of policy implementation. The time arrow goes from left to right. Dashed lines indicate the period over which data were collected.
We considered several sources of information for documenting policy changes, with a strong preference for official sources, including releases from national governments, ministries of public health, embassies and consular services. However, as these are not always available online, secondary sources such as media reports, technical and scientific reports were also deemed acceptable. Social media accounts (e.g., Facebook and Twitter) that are verifiably linked to national and subnational government entities (e.g., ministries of health) were also allowed if no better source could be found. When non-official sources were used, we asked contributors to corroborate information with more than one source where possible. In most cases, contributors were assigned to collect information based on their proficiency with the language(s) used in their particular administrative unit.
To ensure consistency and reproducibility, we developed a uniform data entry protocol (see Supplementary File 1, Data Entry Manual). First, by following a suggested search strategy, contributors were encouraged to conduct an overall review on public health intervention policies in their assigned geographic areas, which included national and first administrative units (Fig. 2). Second, contributors were asked to construct a historical timeline of all public health intervention policy changes starting from January 1, 2020, and complete historical data entry within one week. Third, contributors were asked to track their assigned locations and submit weekly updates either noting new policy changes (new policies or modifications of those previously implemented) or the absence of any changes (Fig. 1).

Spatial resolution of the data reported in each country. This figure shows the percentage of interventions reported at the national level for data reported from January 1, 2020 to July 10, 2020. As of July 10, there have been 10,129 records logged into our database covering 137 countries. A graduated color scale is used to show the percentage of national data available for each country, with the darkest shades representing the highest proportions of such data available. Countries in grey are those where no data have been recorded.
Data were entered into a survey designed on the Research Electronic Data Capture (REDCap) platform hosted at Johns Hopkins University8. If contributors discovered an error with their entries after submitting, they were asked to complete an online change request where they could log the details of the error. The management team reviewed all reported errors and updated the database as appropriate, reaching out to the contributor for clarifications via email or Slack when necessary. Further data validation was completed through weekly audit reports, which are described in detail in the Technical Validation section below.
As a living database, the HIT-COVID team modified the REDCap survey questions to capture nuances in re-opening policy as PHSMs have shifted from closings to openings over time. We disseminated standard information on what constitutes “open,” “partially closed,” and “fully closed,” and added questions about symptom screening and limits on opening capacity in different survey sections as appropriate. These changes are documented in the Data Entry Manual, and are also noted in the change log of our Github repository.
Data Records
The latest version of data (V6.0 at the time of writing) and REDCap survey codebook are available on Github (https://github.com/HopkinsIDD/hit-covid) with the current release available through Zenodo (https://doi.org/10.5281/zenodo.3939075)9. Data visualizations and a description of the project are available online at https://akuko.io/post/covid-intervention-tracking. In the database, each row represents a single policy update with a description of each of the fields below.
Main Dataset
unique_id: unique id for the row combining the record_id and the intervention
record_id: unique id of the REDCap record (note that a single record is generated each time a set of data are entered, so these may be shared across interventions)
entry_time: time and date when data were entered by the contributor
national entry: flag for whether this is a national-level policy
country: ISO 3166-1 alpha-3 country code
country_name: country name
admin1: first administrative unit code (following GADM10 unless otherwise noted)
admin1_name: level 1 administrative unit name
locality: specified geographic areas below level 1
usa_county: name of county for USA county-level data
usa_county_code: FIPS code of the USA county
intervention_group: code that groups interventions by type
intervention: name of the specific intervention
date_of_update: date of updated status to policy implementation for a particular intervention
status: updated status of intervention policy
status_simp: simplified updated status of policy (partially implemented, strongly implemented, implementation suspended)
subpopulation: sub-population that the status of the specific intervention applies to
required: is the specific intervention required or recommended?
enforcement: are police/military enforcing the specific intervention?
size: what is the size of groups allowed for social gatherings or in restaurants?
duration: what is the duration of quarantine or self-isolation?
testing_population: sub-populations of symptomatic or asymptomatic populations tested
details: any specific details about the policy update
source_document_url: URL for the source document(s) stored in the online document repository
url: URL(s) provided by the contributors for the policy update
entry_quality: have these interventions been confirmed by the contributors (Verified, Changes pending, or Unverified)
Completeness dataset
country: ISO 3166-1 alpha-3 country code
admin1: first administrative unit code (following GADM10 unless otherwise noted)
usa_county_data: does this completeness information refer to USA county-level data
intervention_group: code that groups interventions by type
date: date the contributor logged this completeness information
completeness: is this intervention information considered complete and up to date (Complete, Incomplete, Unsure)
Technical Validation
Working with a large team of data collectors with diverse backgrounds presented unique challenges in assuring data quality. To continually clarify the intent behind the survey questions, we held online office hours twice per week to answer questions from contributors, and updated an online list of frequently asked questions that could be easily referenced by contributors. Contributors were encouraged to ask questions or raise concerns either through private correspondence or on our online social media community, within which contributors were organized into sub-communities by their assigned administrative units or themes (e.g., fragile states).
We employed a multi-faceted data validation process after data were reported. We emailed weekly audit reports to contributors for each sub-national administrative unit and country. These reports listed and visualized all intervention updates that had been logged up to that point, organized by intervention type. The reports also highlighted entries with potential errors including possible duplicated entries, potentially inaccurate dates (e.g. dates in the future), and field omissions. Contributors were asked to review their audit reports and either confirm that the entries were all correct, or log errors using an online form. The management team reviewed all logged errors and manually updated the information within REDCap. The study team maintains a record of all database changes, which can be made available upon request.
The database includes an “entry_quality” field that captures the results of this self-audit process. As a living database, this field will continue to change as more data are entered and validated, and as errors are found and resolved. All the records in an audit report for an administrative unit or country are considered “Verified” if the contributor who logged those entries (or in some circumstances someone else assigned to the same administrative unit) has confirmed that all of the information is correct or all reported errors have already been resolved by the management team. If the contributor logged an error for an audit report and the management team has not yet resolved the error, all entries associated with the report will state “Pending changes” in the “entry_quality” field. If a contributor has not submitted an audit report, these entries are considered “Unverified”.
When verifying their data through the audit reports, contributors were also asked to report whether the data for each intervention domain (Table 1) was “Complete”, “Incomplete”, or “Unsure”. Marking an intervention domain as “Complete” means either: 1) the policy is entered and up to date, 2) there is no policy, or 3) the level 1 administrative unit follows the national policy which is already captured in the database. This field provides information on whether the lack of data related to an intervention for a given spatial scale is likely due to the lack of a policy or simply missing data.
In addition to the weekly audits for contributor review, the management team continues to perform periodic internal audits to address repeated misunderstandings in the data entry process. Finally, on the public website visualizing these data (https://akuko.io/post/covid-intervention-tracking), we provide a form for viewers to flag potential errors which the management team will review, clarify, and change as necessary.
Usage Notes
As a public database, HIT-COVID provides a unique opportunity for researchers and policy makers to unravel the potential impacts of PHSM on COVID-19 transmission worldwide. While there are many global databases collecting data for PHSM3,4,5,6,7, HIT-COVID’s particular strengths include the geographic scale of interventions captured across both national and first administrative units, a strong focus on underserved regions of the world (including Africa, South America, and South Asia, see Fig. 2), and standardized field definitions with items aimed at capturing the intensity and nuances of PHSM implementation and relaxation. Furthermore, HIT-COVID maintains a unique requirement for contributors to upload source documents to a centralized server. This archiving system will allow for accurate historical review of PHSM data that may otherwise be lost as government and media sources are updated. Finally, our multifaceted auditing process, based on continuous and scheduled exchanges between data contributors and the data management team, provides a way of verifying both the accuracy and completion of captured data. It is important for users of our data to ascertain whether the absence of data truly reflects the absence of policy implementation within the given PHSM category. HIT-COVID therefore represents a powerful complement to the strengths of other global databases, and has recently been aggregated to the WHO PHSM Database7.
Despite the global efforts made by all HIT-COVID contributors, there are still data missing from a number of countries (Fig. 2). Over the course of this pandemic, we will continue to address coverage gaps by recruiting more contributors, and are collaborating with other COVID-19 related health intervention databases (including the WHO PHSM database7). Furthermore, the scale and complexity of interventions that have been implemented are heterogeneous across regions. Although every effort was made to standardize intervention categories, there may be some discrepancies regarding how our pre-specified intervention categories were interpreted by contributors. While we continue to conduct internal audits to reconcile entries that may not have been coded correctly, further data validation and cleaning will be needed for country and region-specific analysis. Finally, as the pandemic progresses, we anticipate the need to modify or expand the fields of data collection in order to accurately reflect changes in the implementation of PHSMs, though this may make reconciliation of interventions over time more challenging. We provide an example of how our data may be eventually visualized to inform epidemiologic analyses (Fig. 3).

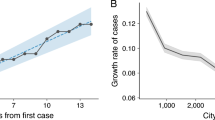
Illustrative example of implemented PHSM for data collected from New Zealand and India at the national and sub-national level to date. Each point represents an intervention. To illustrate interventions of the same type that occurred on the same date, the points are jittered vertically. Dashed line indicates when the first case of COVID-19 was reported in each country (February 28, 2020 and January 30, 2020, respectively).
Code availability
Codes for pulling the standardized dataset from HIT-COVID database and reproducing the figures on HIT-COVID website (https://akuko.io/post/covid-intervention-tracking) are available on Github repository (https://github.com/HopkinsIDD/hit-covid).
References
Huang, C. et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 395, 497–506 (2020).
Imai, N. et al. Adoption and impact of non-pharmaceutical interventions for COVID-19. Wellcome Open Research https://wellcomeopenresearch.org/articles/5-59 (2020).
Porcher, S. Governments’ Responses to COVID-19. openICPSR https://www.openicpsr.org/openicpsr/project/119061/version/V4/view (2020).
ACAPS COVID-19: Government Measures Dataset. Humanitarian Data Exchange(HDX) https://data.humdata.org/dataset/acaps-covid19-government-measures-dataset (2020).
Hale, T., Webster, S., Petherick, A., Phillips,T. & Kira, B. Oxford COVID-19 Government Response Tracker (OxCGRT). Github, https://github.com/OxCGRT/covid-policy-tracker (2020).
Desvars-Larrive A. et al. A structured open dataset of government interventions in response to COVID-19. Sci Data https://doi.org/10.1038/s41597-020-00609-9 (2020).
World Health Organization. Tracking Public Health and Social Measures A Global Dataset. World Health Organization, https://www.who.int/emergencies/diseases/novel-coronavirus-2019/phsm (2020).
Harris, P. A. et al. Research electronic data capture (REDCap) - A metadata-driven methodology and workflow process for providing translational research informatics support. J. Biomed. Inform. 42, 377–81 (2009).
Zheng, Q. et al. HIT-COVID, a global database tracking public health interventions for COVID-19. Zenodo https://doi.org/10.5281/zenodo.3939075 (2020).
Hijmans, R., Garcia, N. & Wieczorek, J. GADM: database of global administrative areas, version 3.6. GADM Maps and Data https://gadm.org/ (2010).
Acknowledgements
We thank all volunteer contributors who have been willing to join our efforts and contribute to this project (see Supplementary File 2). We thank Matt Berg and Dan McCarey from Ona for developing the HIT-COVID website and its data visualizations, Justin Lessler for on-going guidance for this project, Slack Technologies for providing an online workspace for this project, and Andre Hackman for assistance with RedCap. We acknowledge funding from the Johns Hopkins University Modeling & Policy Hub, and the Johnson and Johnson Foundation for some of the activities related to this project.
Author information
Authors and Affiliations
Consortia
Contributions
F.K.J., E.C.L, D.H.P. and A.S.A. developed the survey and codebook. All authors contributed to data collection. Q.Z., F.K.J., S.V.L., L.U., E.C.L. and A.S.A. established and conducted the internal data audit process (technical validation) and are responsible for the daily management of volunteers. Q.Z., F.K.J., S.V.L. and L.U. wrote the first draft of the manuscript. F.K.J. and Q.Z. generated the figures in the manuscript. The members of the HIT-COVID Collaboration contributed to data collection and the internal data auditing process. All authors reviewed and approved the final version of this manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
The Creative Commons Public Domain Dedication waiver http://creativecommons.org/publicdomain/zero/1.0/ applies to the metadata files associated with this article.
About this article

Cite this article
Zheng, Q., Jones, F.K., Leavitt, S.V. et al. HIT-COVID, a global database tracking public health interventions to COVID-19. Sci Data 7, 286 (2020). https://doi.org/10.1038/s41597-020-00610-2
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41597-020-00610-2
This article is cited by
-
The Israeli health system’s rapid responses during the COVID-19 pandemic
Israel Journal of Health Policy Research (2024)
-
Harmonizing government responses to the COVID-19 pandemic
Scientific Data (2024)
-
Standardising policy and technology responses in the immediate aftermath of a pandemic: a comparative and conceptual framework
Health Research Policy and Systems (2023)
-
Timing, extent and outcomes of public health measures in the first wave of the COVID-19 pandemic in Israel and a comparative analysis by socioeconomic indices
Israel Journal of Health Policy Research (2023)
-
Patients’ rights in physicians’ practice during Covid-19 pandemic: a cross-sectional study in Romania
BMC Medical Ethics (2023)
