
Abstract
Gemcitabine-cisplatin (GP) chemotherapy is the standard first-line systemic treatment for recurrent or metastatic nasopharyngeal carcinoma (RM-NPC). In this international, double-blind, phase 3 trial (ClinicalTrials.gov identifier: NCT03581786), 289 patients with RM-NPC and no previous chemotherapy for recurrent or metastatic disease were randomized (1/1) to receive either toripalimab, a monoclonal antibody against human programmed death-1 (PD-1), or placebo in combination with GP every 3 weeks for up to six cycles, followed by monotherapy with toripalimab or placebo. The primary endpoint was progression-free survival (PFS) as assessed by a blinded independent review committee according to RECIST v.1.1. At the prespecified interim PFS analysis, a significant improvement in PFS was detected in the toripalimab arm compared to the placebo arm: median PFS of 11.7 versus 8.0 months, hazard ratio (HR) = 0.52 (95% confidence interval (CI): 0.36–0.74), P = 0.0003. An improvement in PFS was observed across key subgroups, including PD-L1 expression. As of 18 February 2021, a 40% reduction in risk of death was observed in the toripalimab arm compared to the placebo arm (HR = 0.603 (95% CI: 0.364–0.997)). The incidence of grade ≥3 adverse events (AEs) (89.0 versus 89.5%), AEs leading to discontinuation of toripalimab/placebo (7.5 versus 4.9%) and fatal AEs (2.7 versus 2.8%) was similar between the two arms; however, immune-related AEs (irAEs) (39.7 versus 18.9%) and grade ≥3 irAEs (7.5 versus 0.7%) were more frequent in the toripalimab arm. In conclusion, the addition of toripalimab to GP chemotherapy as a first-line treatment for patients with RM-NPC provided superior PFS compared to GP alone, and with a manageable safety profile.
This is a preview of subscription content, access via your institution
Access options
Access Nature and 54 other Nature Portfolio journals
Get Nature+, our best-value online-access subscription
$29.99 / 30 days
cancel any time
Subscribe to this journal
Receive 12 print issues and online access
$209.00 per year
only $17.42 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

Data availability
All requests for data will be reviewed by the leading clinical site, Sun Yat-Sen University Cancer Center, and the study sponsor, Shanghai Junshi Biosciences, to verify whether the request is subject to any intellectual property or confidentiality obligations. Requests for access to the patient-level data from this study can be submitted via email to xurh@sysucc.org.cn with detailed proposals for approval. A signed data access agreement with the sponsor is required before accessing shared data. Source data are provided with this paper.
Code availability
No custom code was used for statistical analysis in this study.
Change history
13 January 2022
A Correction to this paper has been published: https://doi.org/10.1038/s41591-021-01673-3
References
Chen, Y. P. et al. Nasopharyngeal carcinoma. Lancet 394, 64–80 (2019).
Ngan, H. L., Wang, L., Lo, K. W. & Lui, V. W. Y. Genomic landscapes of EBV-associated nasopharyngeal carcinoma vs. HPV-associated head and neck cancer. Cancers (Basel) 10, 210 (2018).
Ou, S. I., Zell, J. A., Ziogas, A. & Anton-Culver, H. Epidemiology of nasopharyngeal carcinoma in the United States: improved survival of Chinese patients within the keratinizing squamous cell carcinoma histology. Ann. Oncol. 18, 29–35 (2007).
Chin, Y. et al. HLA-A SNPs and amino acid variants are associated with nasopharyngeal carcinoma in Malaysian Chinese. Int. J. Cancer 136, 678–687 (2015).
Tian, W. et al. Sequence-based typing of HLA-A gene in 930 patients with nasopharyngeal carcinoma in Hunan province, southern China. Tissue Antigens 86, 15–20 (2015).
Ferris, R. L. et al. Nivolumab for recurrent squamous-cell carcinoma of the head and neck. N. Engl. J. Med. 375, 1856–1867 (2016).
Chow, L. Q. M. et al. Antitumor activity of pembrolizumab in biomarker-unselected patients with recurrent and/or metastatic head and neck squamous cell carcinoma: results from the phase Ib KEYNOTE-012 expansion cohort. J. Clin. Oncol. 34, 3838–3845 (2016).
Zhang, L. et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma: a multicentre, randomised, open-label, phase 3 trial. Lancet 388, 1883–1892 (2016).
Huang, Z. L. et al. The prognostic significance of PD-L1 and PD-1 expression in patients with nasopharyngeal carcinoma: a systematic review and meta-analysis. Cancer Cell Int. 19, 141 (2019).
Wang, F. H. et al. Efficacy, safety, and correlative biomarkers of toripalimab in previously treated recurrent or metastatic nasopharyngeal carcinoma: a phase II clinical trial (POLARIS-02). J. Clin. Oncol. 39, 704–712 (2021).
Ma, B. B. Y. et al. Antitumor activity of nivolumab in recurrent and metastatic nasopharyngeal carcinoma: an international, multicenter study of the Mayo Clinic Phase 2 Consortium (NCI-9742). J. Clin. Oncol. 36, 1412–1418 (2018).
Hsu, C. et al. Safety and antitumor activity of pembrolizumab in patients with programmed death-ligand 1-positive nasopharyngeal carcinoma: results of the KEYNOTE-028 study. J. Clin. Oncol. 35, 4050–4056 (2017).
Fang, W. et al. Camrelizumab (SHR-1210) alone or in combination with gemcitabine plus cisplatin for nasopharyngeal carcinoma: results from two single-arm, phase 1 trials. Lancet Oncol. 19, 1338–1350 (2018).
Wei, X. L. et al. A phase I study of toripalimab, an anti-PD-1 antibody, in patients with refractory malignant solid tumors. Cancer Commun. (Lond.) 40, 345–354 (2020).
Ren, C. et al. Clinical response and biomarker analysis of a phase II basket trial of toripalimab, a PD-1 mAb in combination with standard chemotherapy as a first-line treatment for patients with solid tumors. J. Clin. Oncol. 38, Suppl. abstract e15083 (2020).
Tang, B. et al. Safety, efficacy and biomarker analysis of toripalimab in previously treated advanced melanoma: results of the POLARIS-01 multicenter phase II trial. Clin. Cancer Res. 26, 4250–4259 (2020).
Chen, Y. P. et al. Surrogate endpoints for overall survival in combined chemotherapy and radiotherapy trials in nasopharyngeal carcinoma: meta-analysis of randomised controlled trials. Radiother. Oncol. 116, 157–166 (2015).
Hui, E. P. et al. Efficacy, safety, and pharmacokinetics of axitinib in nasopharyngeal carcinoma: a preclinical and phase II correlative study. Clin. Cancer Res. 24, 1030–1037 (2018).
Zhao, C. et al. Anti-epidermal growth factor receptor (EGFR) monoclonal antibody combined with cisplatin and 5-fluorouracil in patients with metastatic nasopharyngeal carcinoma after radical radiotherapy: a multicentre, open-label, phase II clinical trial. Ann. Oncol. 30, 637–643 (2019).
Brahmer, J. et al. Nivolumab versus docetaxel in advanced squamous-cell non-small-cell lung cancer. N. Engl. J. Med. 373, 123–135 (2015).
Rizvi, N. A. et al. Activity and safety of nivolumab, an anti-PD-1 immune checkpoint inhibitor, for patients with advanced, refractory squamous non-small-cell lung cancer (CheckMate 063): a phase 2, single-arm trial. Lancet Oncol. 16, 257–265 (2015).
Wang, Z. et al. Safety, antitumor activity, and pharmacokinetics of toripalimab, a programmed cell death 1 inhibitor, in patients with advanced non-small cell lung cancer: a phase 1 Trial. JAMA Netw. Open 3, e2013770 (2020).
Corry, J., Fisher, R., Rischin, D. & Peters, L. J. Relapse patterns in WHO 2/3 nasopharyngeal cancer: is there a difference between ethnic Asian vs. non-Asian patients? Int. J. Radiat. Oncol. Biol. Phys. 64, 63–71 (2006).
Sun, L. M., Li, C. I., Huang, E. Y. & Vaughan, T. L. Survival differences by race in nasopharyngeal carcinoma. Am. J. Epidemiol. 165, 271–278 (2007).
Chen, Y. P. et al. Chemotherapy in combination with radiotherapy for definitive-intent treatment of stage II-IVA nasopharyngeal carcinoma: CSCO and ASCO guideline. J. Clin. Oncol. 39, 840–859 (2021).
Tang, L. Q. et al. Prospective study of tailoring whole-body dual-modality [18F]fluorodeoxyglucose positron emission tomography/computed tomography with plasma Epstein–Barr virus DNA for detecting distant metastasis in endemic nasopharyngeal carcinoma at initial staging. J. Clin. Oncol. 31, 2861–2869 (2013).
Acknowledgements
This study is sponsored by Shanghai Junshi Biosciences. The authors thank the patients who participated in this study and their families. This work was supported by National Major Science & Technology Major Projects (no. 2017ZX09302009) awarded to H.F., and a Shanghai Science and Technology Committee Technology Grant awarded to H.F. (no. 17431900700).
Author information
Authors and Affiliations
Contributions
R.-H.X., H.-Q.M., H.F. and S.Y. conceived and designed the study. Provision of study materials and patients was conducted by H.-Q.M., Q.-Y.C., D.C., Chaosu Hu, K.Y., J.W., J.L., Y.-R.S., F.J., R.X., J.P., S.Q., P.L., Chunhong Hu, Y.-C.L., Y.J., X.H., H.-M.W., W.-T.L., W.L., X.H., X.C., Z.L., X.Y., Q.L., X.L., S.J., Y.C., Y.L., C.-Y.H., M.-H.Y., C.-J.Y., J.S., H.F., S.Y., P.K. and R.-H.X. Data analysis and interpretation were carried out by R.-H.X., H.-Q.M., Q.-Y.C., S.Y. and P.K. All authors were involved in writing the manuscript and final approval.
Corresponding author
Ethics declarations
Competing interests
H.F. and S.Y. are employed by Shanghai Junshi Bioscience and TopAlliance Biosciences. P.K. is employed by TopAlliance Biosciences. R.-H.X. has served in consulting or advisory roles for Bristol-Myers Squibb, Merck Serono, Roche, Astellas and AstraZeneca. The remaining authors have no competing interests.
Additional information
Peer review information Nature Medicine thanks J. Jack Lee, Anthony Chan and Douglas Adkins for their contribution to the peer review of this work. Javier Carmona was the primary editor on this article and managed its editorial process and peer review in collaboration with the rest of the editorial team.
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Extended data
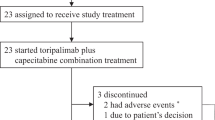
Extended Data Fig. 1 CONSORT diagram for the JUPITER-02 Phase III study.
Between Nov 10, 2018, and Oct 20, 2019, 408 NPC patients were screened for eligibility at 35 sites from mainland China, Taiwan and Singapore. A total of 289 eligible patients were randomized 1:1 to the toripalimab combination arm (n = 146) or the placebo combination arm (n = 143). After completion of chemotherapy, 231 patients continued to receive maintenance treatment (115 in the toripalimab arm and 118 in the placebo arm).
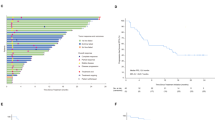
Extended Data Fig. 2 Progression-free Survival by PD-L1 expression subgroups.
Kaplan-Meier estimates of PFS as assessed by a blinded independent review committee according to RECIST v1.1 are shown to compare the toripalimab plus chemotherapy arm with the placebo plus chemotherapy arm in PD-L1 + and PD-L1- subgroups. PD-L1 positive status was defined as the presence of membrane staining of any intensity in ≥1% of tumor cells or immune cells by JS311 IHC staining. Censored patients are marked with “┃” in the graph. Numbers of patients at risk at indicated time points are shown below the x-axis. Number of events and median PFS rates are shown to the right of Kaplan-Meier curves.
Extended Data Fig. 3 Progression-free Survival in PD-L1 + patients.
Kaplan-Meier estimates of PFS as assessed by a blinded independent review committee according to RECIST v1.1 are shown to compare the toripalimab plus chemotherapy arm with the placebo plus chemotherapy arm in PD-L1 + patients. PD-L1 positive status was defined as the presence of membrane staining of any intensity in ≥1% of tumor cells or immune cells by JS311 IHC staining. Censored patients are marked with “┃” in the graph. Numbers of patients at risk at indicated time points are shown below the x-axis. Number of events, median PFS and stratified hazard ratio for disease progression or death are shown to the right of Kaplan-Meier curves. The hazard ratio was computed using the Cox proportional hazards model. The p-value was two-sided with no adjustment of multiplicity and computed using the unstratified log-rank test.
Extended Data Fig. 4 Progression-free Survival in PD-L1- patients.
Kaplan-Meier estimates of PFS as assessed by a blinded independent review committee according to RECIST v1.1 are shown to compare the toripalimab plus chemotherapy arm with the placebo plus chemotherapy arm in PD-L1- patients. PD-L1 negative status was defined as the presence of membrane staining of any intensity in <1% of tumor cells and <1% immune cells by JS311 IHC staining. Censored patients are marked with “┃” in the graph. Numbers of patients at risk at indicated time points are shown below the x-axis. Number of events, median PFS and stratified hazard ratio for disease progression or death are shown to the right of Kaplan-Meier curves. The hazard ratio was computed using the Cox proportional hazards model. The p-value was two-sided with no adjustment of multiplicity and computed using the unstratified log-rank test.
Supplementary information
Supplementary Information
Supplementary Tables 1–24.
Source data
Source Data Fig. 1
PFS by BICR and investigator source data.
Source Data Fig. 2
OS source data.
Source Data Fig. 3
Source data for exposure and clinical events in the ITT population and DoR in patients with confirmed objective responses.
Source Data Extended Data Fig. 2
PFS by BICR in PD-L1 expression subgroups source data.
Rights and permissions
About this article

Cite this article
Mai, HQ., Chen, QY., Chen, D. et al. Toripalimab or placebo plus chemotherapy as first-line treatment in advanced nasopharyngeal carcinoma: a multicenter randomized phase 3 trial. Nat Med 27, 1536–1543 (2021). https://doi.org/10.1038/s41591-021-01444-0
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41591-021-01444-0
This article is cited by
-
Cost-effectiveness of pembrolizumab versus chemotherapy in patients with platinum-pretreated, recurrent or metastatic nasopharyngeal cancer
Cost Effectiveness and Resource Allocation (2024)
-
Nasopharyngeal carcinoma: current views on the tumor microenvironment's impact on drug resistance and clinical outcomes
Molecular Cancer (2024)
-
Machine learning-based extrachromosomal DNA identification in large-scale cohorts reveals its clinical implications in cancer
Nature Communications (2024)
-
Remodeling the tumor-immune microenvironment by anti-CTLA4 blockade enhanced subsequent anti-PD-1 efficacy in advanced nasopharyngeal carcinoma
npj Precision Oncology (2024)
-
Toripalimab plus capecitabine in the treatment of patients with residual nasopharyngeal carcinoma: a single-arm phase 2 trial
Nature Communications (2024)
