
Abstract
While volunteer-based studies such as the UK Biobank have become the cornerstone of genetic epidemiology, the participating individuals are rarely representative of their target population. To evaluate the impact of selective participation, here we derived UK Biobank participation probabilities on the basis of 14 variables harmonized across the UK Biobank and a representative sample. We then conducted weighted genome-wide association analyses on 19 traits. Comparing the output from weighted genome-wide association analyses (neffective = 94,643 to 102,215) with that from standard genome-wide association analyses (n = 263,464 to 283,749), we found that increasing representativeness led to changes in SNP effect sizes and identified novel SNP associations for 12 traits. While heritability estimates were less impacted by weighting (maximum change in h2, 5%), we found substantial discrepancies for genetic correlations (maximum change in rg, 0.31) and Mendelian randomization estimates (maximum change in βSTD, 0.15) for socio-behavioural traits. We urge the field to increase representativeness in biobank samples, especially when studying genetic correlates of behaviour, lifestyles and social outcomes.
Similar content being viewed by others


Main
The overarching aim of genetic epidemiology is to elucidate the genetic underpinning of health and disease. To maximize power for genome-wide discovery, researchers curate large biobanks with rich genetic and phenotypic data. To ensure the validity of findings in genome-wide association (GWA) studies, researchers aim to eliminate potential sources of bias, such as population stratification, assortative mating, measurement error and indirect genetic effects1,2,3,4.
A particularly challenging bias that is typically not considered in genetic studies can occur when biobanks collect data from individuals that are not representative of their target population5,6,7. Under certain conditions, research on non-representative samples can lead to valid conclusions—for example, when study participation is unrelated to both the independent and dependent variables. However, many commonly studied factors influence study participation. These may include mental and physical health, substance use (such as cigarettes and alcohol), income, and educational attainment8,9,10,11,12, where study participants are typically healthier than the target population. Such ‘healthy-volunteer bias’ is well documented in the UK Biobank (UKBB), one of the most widely used resources for biomedical research. Of the nine million people invited to take part in the UKBB, only 5.5% (~500,000) participated in the study—a sample of volunteers with healthier lifestyles, higher levels of education and better health than the general UK population13,14.
Given the growing reliance on non-representative biobanks, it is paramount to assess the extent to which study participation induces bias in genome-wide studies and downstream analyses. In observational studies using UKBB data, participation bias has already been shown to distort phenotypic exposure–outcome associations12,13,15. If study participation includes a genetic component, biased estimates are also expected in genetic studies16. In gene-discovery studies, non-random participation may distort the association between a genetic variant and the outcome (Fig. 1a). In Mendelian randomization (MR) (a causal inference technique using single nucleotide polymorphisms (SNPs) as instrumental variables), participation bias could induce an association between genetic instruments and unmeasured confounders of the exposure–outcome relationship, thereby violating a key assumption of the method (Fig. 1b,c). Recent genome-wide studies investigating proxies of participation bias have already described genetic variation associated with participation and questionnaire responding17,18,19,20,21,22,23,24, indicating that genetic studies are not immune to bias. While much of the recent GWA output has been produced by non-representative biobanks (for example, UKBB, Million Veteran Program and 23andMe), the extent to which participation bias affects gene discovery and downstream analyses is currently unknown.

a–c, The relationships between a genetic variant (G), an exposure (X) or outcome (Y), and study participation (Z). Panel a illustrates the effect of participation bias in GWA studies, where Z is a common consequence of G and Y (red dotted line). Conditioning on a common consequence (Z) induces a non-causal association between G and Y. Panels b,c illustrate the effect of participation bias in MR studies, where bias occurs if Z is a consequence of either X (b) or Y (c). Conditioning on Z induces an association between the genetic variant and confounders, thereby violating the MR assumption of exchangeability. This figure is a simplified illustration of how participation bias can impact results obtained from two commonly employed methods in genomic studies. For further examples illustrating the impact of selection bias, see Hernán et al.7.
Researchers can correct for participation bias by the use of samples that are representative of their target population—a broader group from which a study sample is drawn and to which the study results should generalize. In case of the UKBB, the target population is middle-aged to older adults of recent European ancestry living in the United Kingdom, which is not the same as the general UK population (Supplementary Information). Here we derive a model for participation probability and create a pseudo-sample of the UKBB matching its target population with respect to 14 variables. We can thereby evaluate how a shift towards representativeness impacts genome-wide findings and downstream analyses. We anticipate that these findings will help characterize the impact of participation bias in large volunteer-based samples used for biomedical research and help pin down areas of research that might be particularly susceptible to bias when relying on non-representative samples.
Results
Samples
From the five Health Survey England (HSE) cohorts comprising a total sample of n = 81,118, we retained n = 22,646 after applying the same inclusion criteria used for UKBB recruitment (Methods). After further exclusion of HSE individuals with missing data on the 14 auxiliary variables, we included a final sample of n = 21,816. Comparing the distribution of a subset of auxiliary variables also available in the UK Census Microdata (n = 895,649) shows that the profile of the HSE sample closely matches that of the Census sample (Supplementary Table 1). More specifically, proportions were comparable between the HSE and Census but deviated in the UKBB for most of the selected variables, such as proportion (P) of female gender (PCENSUS = 51%, PHSE = 51%, PUKBB = 54%), proportion of individuals of age ≥65 (PCENSUS = 13%, PHSE = 13%, PUKBB = 19%), mean (M) age when individuals completed full-time education (MCENSUS = 16.6, MHSE = 16.4, MUKBB = 17.2) and proportion of retired individuals (PCENSUS = 19%, PHSE = 19%, PUKBB = 34%). Further inspection of the associations between variables available in the HSE and UK Census (Supplementary Fig. 1) highlights that the HSE captures the characteristics of the population residing in England well.
Of the initial UKBB sample (502,645 participants), we excluded individuals of age >69 and <40 (n = 2463), individuals from Scotland or Wales (n = 56,483), individuals who self-identify as non-white (n = 28,371) and individuals withdrawing consent (n = 161). We further removed 21,868 (5.27%) individuals with missing data for any of the auxiliary variables. Since these individuals can be considered a special case of missingness due to non-participation, which the probability weights were designed to compensate for, we did not impute missing data for the auxiliary variables. The sampling weights were generated for n = 393,299 UKBB individuals, of which 109,550 were removed after we applied quality control steps for genome-wide analyses (Methods).
Performance of the UKBB probability weights
We derived a model for participation probability by comparing 14 harmonized characteristics of UKBB participants with those of a representative sample (HSE). The application of the resulting probability weights then facilitates the creation of a (weighted) pseudo-sample of the UKBB that is more representative of its (representative) target population (HSE). Figure 2a shows the distribution of the normalized probability weights (win) for UKBB individuals. We obtained the probabilities used to construct the weights from a LASSO regression model retaining 454 of the 903 initially included predictors. Figure 2b illustrates which auxiliary variables were the most strongly linked to UKBB participation (UKBB = 1; HSE = 0), highlighting that older (retired), more educated and non-smoking people were particularly likely to participate.

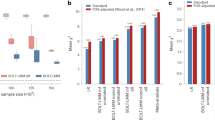
a, Truncated (*) density curves of the normalized probability weights (win) for UKBB participants, ranging from 0.02 to 50.01. b, Standardized coefficients (and 95% confidence intervals) of variables predicting UKBB participation (HSE = 0; UKBB = 1) in univariate logistic regression models. Coefficients are provided for all UKBB participants and for males and females separately. c, Correlation coefficients among all auxiliary variables within the UKBB (obtained from weighted and unweighted analyses) and within the HSE. Highlighted in blue are results where the coefficients between the UKBB (rUKBB) and the reference sample (rHSE) deviated (rdiff > 0.05, where rdiff = |rHSE − rUKBB|). d, Percentage change (for categorical variables) and change in means as a function of weighting, obtained for a number of health-related UKBB phenotypes, including the auxiliary variables (blue) and variables not used to construct the weights. Percentage change was estimated as the difference between the weighted (pw) and unweighted proportion (p), divided by the unweighted value ((pw − p) / p × 100). Change in means was expressed as a standardized mean difference, estimated as the difference between the unweighted mean (m) and the weighted mean (mw), divided by the unweighted standard deviation (mw − m/s.d.).
To evaluate the performance of the weights, we first assessed whether probability weighting recovered the reference (HSE) population distributions. We included the generated weights in a univariate logistic regression model predicting UKBB participation, where UKBB individuals were given their normalized weight (win) and HSE participants were given a weight of 1. When we applied probability weighting (shown on the right side of Fig. 2b), previously significant predictors became non-significant. All means and proportions in the HSE, UKBB (unweighted) and UKBB (weighted) are provided in Supplementary Table 2.
Next, we estimated the degree of bias reduction in our 14 variables following probability weighting. Here we quantified participation bias as the difference between an estimate of association obtained in the UKBB (rUKBB) and the reference sample (rHSE). The largest differences (rdiff = |rHSE − rUKBB|) were for employment status with overall health (rdiff = 0.19; rHSE = −0.25; rUKBB = −0.06), overall health with age (rdiff = 0.12; rHSE = −0.13; rUKBB = −0.01), household size with income (rdiff = 0.10; rHSE = 0.20; rUKBB = 0.31) and employment status with income (rdiff = 0.10; rHSE = −0.25; rUKBB = −0.35) (Fig. 2c). The application of probability weighting reduced bias induced by selective participation (median bias reduction, 0.97; mean, 0.91; range, 0.58–0.998). The estimates were very similar to the cross-validated model (median bias reduction, 0.96; mean, 0.90; range, 0.50–0.998), highlighting that overfitting was unlikely to be a problem.
Finally, Fig. 2d summarizes the changes in means and proportions following probability weighting, estimated for the auxiliary variables (in blue) as well as other UKBB variables (in orange) not used to construct the weights. Weighting resulted in a pseudo-sample with less favourable health outcomes and demographics, including more frequent mental illness (higher rates of schizophrenia and alcohol addiction) and poorer socio-economic status (higher deprivation index and lower job class).
In summary, using probability weighting, we created a pseudo-sample of the UKBB population achieving higher levels of representativeness along the 14 variables used in the weighting model. As a consequence, the weighting also changed the distributions of some variables not used in the weighting model (for example, an increased level of deprivation). Probability weighting thus provides a useful tool for examining bias due to selective participation in genomic studies, by evaluating how reweighting affects genome-wide results and downstream analyses.
Probability-weighted GWA analyses
We next studied how the results of GWA analyses differ between weighted GWA (wGWA) (neffective = 94,643 to 102,215, depending on the trait) and standard GWA analyses (\(\hat \beta\), n = 263,464 to 283,749, depending on a trait). Reductions in the effective sample size in wGWA result from variability among the probability weights: when the weights are normalized to have a mean of one, the effective sample size simplifies to n × {1/[Var(win) + 1]}. This quantity thus depends on the unweighted study sample size and on the variance of the normalized weights across study participants (win).
We assessed the impact of probability weighting on genome-wide findings in terms of changes in effect sizes across SNPs (contrasting weighted SNP effects, \(\hat \beta _{\mathrm{w}}\), to standard SNP effects, \(\hat \beta\)) and the number of significant SNP associations for 19 UKBB health-related traits collected at baseline (Fig. 3). First, Fig. 3a highlights the number of SNPs where weighting reduced (\((|\hat \beta | - |\hat \beta _{\mathrm{w}}|)/\left| {\hat \beta } \right| \ge 0.2\)) or increased (\((|\hat \beta | - |\hat \beta _{\mathrm{w}}|)/\left| {\hat \beta } \right| \le - 0.2\)) SNP effect sizes. Among all genome-wide hits (1,690, with P < 5 × 10−8), effect size reduction following weighting was more common (420 SNPs, 24.85% of all genome-wide SNPs) than increase (290 SNPs, 17.16% of SNPs). More specifically, effect size increase was the most common for cancer (57% of SNPs), loneliness (50%), education (33%) and reaction time (33%), whereas reduction was present for depression/anxiety (67%), coffee intake (63%) and smoking status (58% of SNPs). While a shift towards more representativeness led to both effect size increases and decreases, we found no evidence of changes in the direction of effects (Supplementary Section 3.2).

a,b, Summary of the comparison between SNP effects obtained from wGWA and standard GWA analyses on 19 traits. Panel a summarizes the proportions of overestimated and underestimated SNP effects as a result of participation bias. Shown in b are the numbers and proportions of SNPs reaching genome-wide significance in standard GWA, wGWA or both (GWA and wGWA). The scatter plots to the right plot the weighted (|𝛽w|) against the unweighted (|𝛽|) SNP effects for four selected traits.
Second, with respect to genome-wide discovery (Fig. 3b), we found that of all SNPs identified in either wGWA or GWA analyses (n = 1,690 across all phenotypes), 25 SNPs (1.48%) reached significance only in the weighted analyses. We found new SNPs for 12 of the 19 included traits, most notably for depression and anxiety (50% new genome-wide SNPs), cancer (29%) and loneliness (25%). The detailed results are listed in Supplementary Table 3 and plotted in Supplementary Figs. 2 and 3.
Probability-weighted GWA analysis on sex
The UKBB included proportionally more women (femaleUKBB = 54.38%) than its target population (femaleHSE = 50.74%; femaleCENSUS = 50.62%). Probability weighting recovered the target population prevalence in the UKBB (weighted femaleUKBB = 50.36%). SNP heritability estimates (h2) (Supplementary Fig. 4a) using wGWA led to almost half of that of the standard GWA (h2 on liability scale, 1.2%, P = 0.1 in wGWA versus 2.1%, P = 5.4 × 10−11 in standard GWA). Supplementary Fig. 4b and Supplementary Table 4 display the SNP effects of 49 variants previously associated with sex (P < 5 × 10−8, in an independent sample of >2,400,000 volunteers) to estimates obtained from standard GWA and wGWA. Of those, 18 SNPs (36.73%) showed significantly lower sex-associated effects in wGWA. In contrast, only 3 SNPs (6.12%) had significantly lower sex-associated effects in standard GWA.
GWA study on UKBB participation
We conducted a wGWA on UKBB participation in neffective = 102,215 participants. A total of 28 SNPs reached genome-wide significance (P < 5 × 10−8), of which we selected 23 linkage disequilibrium (LD)-independent SNPs after clumping. Supplementary figures (Manhattan and QQ plots) and information (gene and phenotype annotation) for these SNPs are available in Supplementary Figs. 5 and 6 and Supplementary Tables 5 and 6.
SNP heritability for UKBB participation was h2 = 0.009 (s.e. = 0.005; LD-score intercept, 1.055). LD-score regression analyses (Fig. 4b and Supplementary Table 7) implicated substantial genetic correlations between UKBB participation and phenotypes related to socio-economic factors and previously assessed participatory behaviour, including educational attainment (rg = 0.85), income (rg = 0.77), participation (provided e-mail address for recontact and mental health survey completion) (rg = 0.69 and rg = 0.61, respectively), intelligence (rg = 0.62) and cigarette use (age of onset) (rg = −0.70).

Shown are the genetic correlations (rg) and corresponding 95% confidence intervals of UKBB participation (n standard GWA = 283,749) with traits indexing participatory behaviour (in green) and other traits (in blue) (including publically available summary statistics generated using standard GWA. SBP, systolic blood pressure; IR,: Item-response theory.
Weighted SNP heritability and genetic correlation estimates
We next assessed differences in SNP heritability \((h_{{\mathrm{DIFF}}}^2 = h^2 - h_{\mathrm{w}}^2)\) and genetic correlations (rg,DIFF = rg − rg,w) between standard GWA and wGWA analyses (Fig. 5). On average, heritability estimates differed by 1.5% (liability scale \(|h_{{\mathrm{DIFF}}}^2|\), 0.015; range, 0 to 0.05). \(h_{{\mathrm{DIFF}}}^2\) was the highest for BMI (h2 = 0.24; \(h_{\mathrm{w}}^2\) = 0.19), education (h2 = 0.21; \(h_{\mathrm{w}}^2\) = 0.24) and diabetes (h2 = 0.19; \(h_{\mathrm{w}}^2\) = 0.16). Of all assessed traits included in the LD-score regression (n = 18), five showed significant (PFDR < 0.05) \(h_{\mathrm{DIFF}}^2\), of which four (80%) were lower and one (education) was higher in the more representative (weighted) sample. The weighted and unweighted heritability estimates are plotted in Supplementary Fig. 7, and additional statistics (for example, LD-score intercepts) are provided in Supplementary Table 8.

a, Differences in SNP heritability (\(h_{{\mathrm{DIFF}}}^2 = h^2 - h_{\mathrm{w}}^2\)) and genetic correlations (rg,DIFF = |rg| − |rg,w|) obtained from weighted and standard GWA analyses. The diagonal shows the differences in SNP heritability, where biases leading to overestimation (\(h_{\mathrm{DIFF}}^2\) > 0.02) are plotted in orange and biases leading to underestimation (\(h_{\mathrm{DIFF}}^2\) < −0.02) are plotted in yellow. The off-diagonal highlights overestimated genetic correlations (rg,DIFF > 0.1) in blue and underestimated genetic correlations (rg,DIFF < −0.1) in green. Tiles coloured in turquoise index genetic correlations where rg and rg,w show opposite directions (with rg printed at the top and rg,w printed at the bottom of the tile). b, Estimates of genetic correlations (rg shown as circles; rg,w shown as triangles) and the corresponding 95% confidence intervals for two selected traits. The asterisks indicate estimates showing significant differences (PFDR < 0.05). All P values are from two-sided tests and are corrected for multiple testing using FDR correction (controlled at 5%).
Concerning estimates of genetic correlations, we found an average difference of |rg,DIFF| = 0.07 (range, 0 to 0.31) between results obtained from standard GWA and wGWA analyses. rg decreased the most notably for rg(BMI, smoking status) (rg = 0.27; rg,w = 0.13), rg(fruit intake, physical activity) (rg = 0.32; rg,w = 0.18) and rg(alcohol use frequency, smoking status) (rg = 0.35; rg,w = 0.21). The increase in rg after weighting was the most prominent for rg(insomnia, risk taking) (rg = 0.02; rg,w = 0.31), rg(vegetable intake, physical activity) (rg = 0.3; rg,w = 0.58) and rg(depression/anxiety, risk taking) (rg = 0.27; rg,w = 0.47). For five (3.27%) of the assessed trait pairs (n = 153) the weighted and standard genetic correlations were significantly (PFDR < 0.05) different, of which education was the most implicated trait (Supplementary Fig. 8 and Supplementary Table 9). Change in the sign of genetic correlations because of participation bias was less common (17 of the 153 assessed trait pairs, but none of these rg,DIFF were significant (PFDR > 0.05), Supplementary Section 3.3).
Weighted MR estimates
Figure 6 summarizes MR estimates with differences between the standard and weighted MR estimates (\(\alpha_{\mathrm{DIFF}} = \hat \alpha - \hat \alpha _{\mathrm{w}}\)).

a,b, Summary of results obtained from weighted (\(\hat \alpha _{\mathrm{w}}\)) and standard (\(\hat \alpha\)) MR. MR estimates subject to overestimation (\(|\hat \alpha | - |\hat \alpha _{\mathrm{w}}| > 0.1\)) as a result of participation bias are highlighted in violet. MR estimates subject to underestimation (\(|\hat \alpha | - |\hat \alpha _{\mathrm{w}}| < -0.1\)) are highlighted in cyan. The asterisks highlight results where \(\hat \alpha\) and \(\hat \alpha _{\mathrm{w}}\) showed significant (PFDR < 0.05) differences. The error bars (b) indicate the 95% confidence intervals corresponding to \(\hat \alpha\) and \(\hat \alpha _{\mathrm{w}}\). All P values are from two-sided tests and are corrected for multiple testing using FDR correction (controlled at 5%).
On average, increasing sample representativeness led to an absolute change of 0.038 in standardized MR estimates (range, 0 to 0.15). Associations between lifestyle choices, including coffee intake on BMI (\(\hat \alpha\) = 0.8; \(\hat \alpha _{\mathrm{w}}\) = 0.65), fruit consumption on LDL cholesterol (\(\hat \alpha\) = 0.03; \(\hat \alpha _{\mathrm{w}}\) = −0.12) and fruit consumption on coffee intake (\(\hat \alpha\) = 0.15; \(\hat \alpha _{\mathrm{w}}\) = 0.01) (Supplementary Fig. 9 and Supplementary Table 10), were the most affected. Of all exposure–outcome associations tested (k = 234), 14 (6%) estimates were either decreased (2%, \(|\hat \alpha | - |\hat \alpha _{\mathrm{w}}| > 0.1\)) or increased (4%, \(|\hat \alpha | - |\hat \alpha _{\mathrm{w}}| < -0.1\)) after weighting. We found significant (PFDR < 0.05) differential effects for two exposure–outcome associations (education on BMI and smoking status on fruit consumption). There was little evidence of changes in the direction of MR estimates as a result of weighting, which occurred for only two exposure–outcome pairs, neither of which was significant (αDIFF PFDR > 0.05) (Supplementary Section 3.4).
Discussion
While large volunteer-based biobanks are key to advancing genetic epidemiology, it is unclear to what extent selective participation impacts genotype–phenotype associations obtained from their data. In this work, we derived probability weights for the UKBB (based on 14 variables harmonized with data from a representative sample) and conducted inverse-probability-weighted GWA analyses on 19 traits. Conducting genome-wide analyses in a more representative (weighted) sample of the UKBB, we found that selective participation can distort genome-wide findings and downstream analyses.
Overall, increasing representativeness mostly affected the magnitude of effects rather than their direction. We found several differences in estimates in all sets of genome-wide analyses, in both directions (for example, a decrease in SNP effects after weighting for cancer and education and an increase in SNP effects for coffee intake and depression/anxiety). Of note, although effect size estimates can increase with the use of more representative samples, the increased standard errors of the inverse probability weighting (due to reduced effective sample size) make new SNP discovery difficult. Despite this caveat, using wGWA revealed new loci for 12 traits. Reweighting also changed heritability estimates, genetic correlations and MR estimates, most notably for socio-behavioural traits including education, diet, smoking and BMI.
In contrast, we observed smaller changes between wGWA and GWA estimates for molecular and physical traits (for example, low-density lipoproteins and systolic blood pressure). This pattern is in line with existing studies23,24, as well as our findings of high genetic correlations between the liability to UKBB participation and socio-behavioural traits (particularly education, income and substance use). More broadly, different sources of bias probably affect similar phenotypes in genome-wide studies, in that genome-wide findings on socio-behavioural phenotypes are biased by selective participation23,24, indirect genetic effects3, assortative mating4, error in measurements25 and population stratification26.
Our work builds on and extends recent efforts evaluating bias due to selective participation. We replicate findings showing that phenotypic exposure–outcome associations in the UKBB differ from those estimated in probability samples13,15: participation bias, defined as the difference in exposure–outcome associations in the UKBB and the reference sample (HSE), was substantial for several associations. For example, phenotypically, participation bias distorted the association of overall health with age and employment status. The application of probability weighting eliminated a significant proportion (>90%) of bias due to selective participation in the UKBB.
We highlight patterns of bias and point to areas of research that are the most impacted by this bias. Since GWA summary statistics are increasingly used in epidemiological research to study causal questions concerning education, diet and behaviour, greater care should be taken when relying on data obtained from non-random samples. If researchers cannot assess participation bias in biobank data (for example, in self-selected samples without a defined target population), their data may be of only limited use when scrutinizing genotype–phenotype relationships. As part of this work, we provide software to perform wGWA, which allows researchers to conduct sensitivity checks when relying on non-representative samples. Alternatively, recruitment schemes incorporating probability sampling can help reduce bias, but samples are typically small given the substantial costs associated with recruitment.
Our results should be interpreted with caution. First, while the application of probability weighting successfully reduced bias resulting from selective participation in the UKBB based on our 14 variables, residual bias still exists. We may have missed important factors independently predicting UKBB participation when modelling participation probability, as we chose our auxiliary variables on the basis of the availability of variables that could be harmonized between the UKBB and the reference sample. Still, some of these omitted variables may be proxied by (the combination of) some of the 14 variables, hence not compromising the probability weights. Probability weighing would not correct bias in situations where the exposure and the outcome of interest both link to an aspect of study participation that is unrelated to the auxiliary variables. This also means that wGWA for outcome traits such as education level is expected to be accurate, since this trait has been used when modelling participation probability. Finally, even for outcome traits completely unrelated to the 14 auxiliary variables but linked to traits influencing study participation, it is extremely unlikely that wGWA would be more biased than unweighted GWA. Hence, when substantial differences are observed between wGWA and standard GWA results, it is likely that the latter is (more) biased. Still, weighting—like any other method of adjusting for non-representativeness—should therefore be considered as only the second-best option when tackling participation bias, as only the implementation of probability sampling at the recruitment stage can ensure full elimination of this type of bias.
Second, when choosing a reference population, there is a trade-off between the representativeness of the reference sample and the number of available variables to match the samples. We chose to use the HSE as a reference sample to strike a balance between these two factors, but biases can remain if the reference sample is not representative enough. Third, genome-wide analyses were restricted to phenotypes with little missing data. This is a shortcoming since traits with substantial missing data are perfect candidates for characteristics influencing participation. We therefore did not evaluate the impact of participation bias on variables collected at follow-up.
Finally, the UKBB probability weights are sample-specific, constructed for a sample that is better educated, healthier and older and includes more women than the target population. Bias due to selective participation will differ across study contexts, and the participation mechanisms evaluated in this study are therefore not generalizable to other cohorts. For example, large health-registry-based biobanks, where older individuals with poorer health tend to be over-represented, do not have the healthy-volunteer bias but have different kinds of selection biases27. Similarly, the genome-wide results discussed here can be generalized only to adults of European genetic ancestry who also self-identify as white. Future work should also assess the impact of participation bias in more diverse samples, notably other ancestries and racial and ethnic groups, as well as younger individuals.
In conclusion, our results highlight that GWA and downstream analyses are sensitive to bias resulting from selective participation, most visibly for socio-behavioural traits. Moving forward, more efforts ensuring either sample representativeness or methods correcting for participation bias are paramount, especially when studying the genetic underpinnings of behaviour, lifestyles and educational outcomes.
Methods
We first derived a model for participation probability by comparing 14 harmonized characteristics of the UKBB sample with those of a representative sample. Using the estimated participation probabilities, we conducted wGWA analyses on 19 UKBB traits. Second, to explore the genetic basis of UKBB participation, we conducted a GWA on the participation probability and evaluated the genetic findings. Finally, comparing wGWA results with those obtained from standard GWA analyses, we assessed the impact of participation bias on the estimation of three frequently studied quantities: (1) the effect of genetic markers on complex traits, (2) heritability and genetic correlation estimates, and (3) exposure–outcome associations obtained from MR.
Samples
UKBB
The UKBB is a large-scale prospective population-based research resource focusing on the role of genetic, environmental and lifestyle factors in health outcomes in middle age and later life. More than 9,000,000 men and women between 40 and 69 registered with the UK National Health Service were invited to take part. Of those, 5.4% (~500,000 individuals) were recruited in 22 assessment centres across England, Wales and Scotland between 2006 and 201028,29. Included in this study were data from UKBB participants of European genetic ancestry who also identify as white and passed standard GWA analysis quality control measures30. We further filtered the sample according to geographic region (excluding individuals from Scotland and Wales) to match the geographic regions included in the reference sample (HSE), and we removed individuals with missing data in the auxiliary variables used to generate the propensity scores (further described below). The UKBB resource was approved by the UKBB Research Ethics Committee, and all participants provided written informed consent to participate.
HSE
The HSE is an annual probability sample set out to measure health and related behaviours in a nationally representative sample of adults and children living in private households in England31. In our study, we included data from five cohorts recruiting a sample of more than 80,000 individuals between 2006 and 2010 (that is, the UKBB recruitment period). We applied the same inclusion criteria to the HSE data as used for UKBB recruitment, retaining only individuals aged between 40 and 69 years who self-identify as white. HSE response rates ranged between 64% and 68%31. HSE sample weights are supplied to account for the unequal probabilities of selection and non-response32, weighing individuals as a function of sex, household type, region and social class. In this study, the HSE weights were incorporated in LASSO regression predicting UKBB participation (described below).
UK Census data
We also exploited data from the 2011 Census Microdata, a 5% sample of anonymized individual-level Census records33, which runs every ten years to collect basic demographic variables (for example, educational attainment, age and general health) through a paper-based or online questionnaire. With a 95% response rate, the UK Census Microdata is highly representative of the UK population. We applied the same selection criteria to the Census data as to the UKBB and HSE (that is, filtered according to geographic region, ethnic group and age), resulting in a relevant sample of n = 895,649. We extracted all variables that could be harmonized with the UKBB and HSE data (further described in the Supplementary Information). The Census data were solely used to assess the level of representativeness of the HSE, by comparing the distributions and associations between variables present in both the HSE and the Census sample. For the generation of UKBB probability weights, we used the HSE sample, given its richer phenotypic data, which are critical for accurate weight estimation.
Analysis
Auxiliary variables
We adjusted for participation bias in the UKBB using probability weighting34. This approach adjusts for non-response bias by weighting over-represented and under-represented individuals, thereby creating a pseudo-population that is more representative of its target population35. Probability weighting relies on auxiliary variables available for both a selected (non-representative) and a representative reference sample. In this study, we selected auxiliary variables tapping into dimensions related to health, lifestyle, education and basic demographics. We included all variables that could be harmonized across the two datasets (HSE and UKBB) with few missing observations (that is, <50,000 in the UKBB and <500 in the HSE). Fourteen variables derived from 12 measures were included and harmonized across the two datasets. The five continuous variables included age, BMI, weight, height and education (age when the individual completed full-time education). The nine categorical variables included household size (1, 2, 3, 4, 5, 6, or 7 or more), sex (male or female), alcohol consumption frequency (never, a few times per year, monthly, once or twice weekly, three or four times weekly, or daily), smoking status (never, previous or current), employment status (employed, economically inactive, retired or unemployed), income (<18k, 18k–31k, 31k–52k, 52k–100k or >100k), obesity status (underweight, healthy weight, overweight or obese), overall health (poor, fair or good) and degree of urbanisation (village/hamlet, town/fringe, urban). Further details of the coding of the variables in each dataset are provided in the Supplementary Information.
Construction and evaluation of UKBB probability weights
To derive the model for participation probability, we first combined the harmonized UKBB data with the data from the reference sample (HSE). We then used LASSO regression in glmnet36 to predict UKBB participation (Pi, with UKBB = 1; HSE = 0), conditional on the harmonized auxiliary variables described above. We included 14 main effects (5 continuous variables and 9 binary/categorical variables) in the model. All categorical and binary variables were entered as dummy variables, indexing each possible level of the variable. In addition, we included all possible two-way interaction terms among the dummy and continuous variables, resulting in 903 included predictors. LASSO performs variable selection by shrinking the coefficients for variables that contribute the least to prediction accuracy. The shrinkage is controlled by the tuning parameter (λ), which was obtained using fivefold cross-validation that minimizes the cross-validated error.
The predicted probabilities (Pi) were then used to build the individual sampling weights (wi). The weights were calculated as an extension of standard inverse probability weights (wi = (1 − Pi)/Pi), designed to make the weighted sample estimates conform to the population estimates35. To assess the performance of the generated weights, we evaluated the extent to which the weighting recovered means (for continuous variables) and prevalences (for binary traits) in the UKBB and hence mitigated participation bias. We also quantified participation bias as the differences between the correlations among all auxiliary variables within the UKBB (rUKBB) and the HSE (rHSE). The degree to which the weighted correlations (rUKBB,w) reduced bias was estimated as (|rHSE − rUKBB| − |rHSE − rUKBB,w|)/(|rHSE − rUKBB|), where a value of one indicates that weighting fully eliminated bias. The weighted means (and proportions) for a given variable (Xi) were estimated using the weights (wi), with the expression \(\frac{1}{W}\mathop {\sum }\nolimits_{i = 1}^N w_iX_i\), where \(W = \mathop {\sum }\nolimits_{i = 1}^N w_i\).
We further evaluated whether overfitting was a problem by rerunning LASSO in train–test splits of the data (fivefold leave-one-out cross-validation, with a split ratio of 80:20). Here we used the training sample (80% of the data) for model estimation and the test sample (20% of the data) to generate the out-of-sample predicted probabilities. The degree of participation bias reduction was then compared between the out-of-sample predicted probabilities and the full-sample probabilities.
Probability-weighted GWA analyses
To evaluate the extent to which SNP effects were distorted by participation bias in the UKBB, we conducted wGWA analyses. wGWA was performed for 19 UKBB health-related traits collected at baseline with few missing observations (nmissing < 50,000). Some of these traits (education, frequency of alcohol use, weight, height and smoking status) were used in the model deriving the probability weights. The coding of all variables, genotyping, imputation and quality control procedures are described in the Supplementary Information. Additional quality control filters for genome-wide analyses were applied to select participants (that is, restricting the sample to unrelated individuals of European genetic ancestry and excluding individuals with high missing rate and high heterozygosity on autosomes) and genetic variants (Hardy–Weinberg disequilibrium P > 1 × 10−6, minor allele frequency > 1% and call rate > 90%).
We obtained unweighted SNP estimates \((\hat \beta )\) from a standard ordinary least squares linear regression model. The weighted SNP estimates \((\hat \beta _{\mathrm{w}})\) were obtained from weighted least squares regression. All GWA analyses were conducted in LDAK (version 5.2)37,38, which was extended to accommodate sampling weights in a linear weighted least squares model (linear; sample-weights). The standard least squares estimate of the variance is based on the assumption of homoskedasticity (that is, that the residual variance is constant across individuals). Since the use of sampling weights violates this assumption, we used the Huber–White estimator39 to estimate the variance of the coefficients:
with
where Y denotes the phenotypic outcome vector, W is a diagonal matrix with the probability weights sitting on the diagonal and X is a column vector of the genotype values.
Both models included the same covariates (PC1–PC5, sex, age and batch effect). We applied a linear model to all outcomes (continuous and binary traits). This was done to allow for the standardization of SNP estimates and to ensure the comparability of effect sizes. A more detailed discussion on the advantages and disadvantages of using a linear over a logistic model for binary outcomes is provided by von Hippel40,41, as well as the Neale Lab42 discussing its application specifically when using UKBB data.
Two additional sets of analyses were conducted to explore the genetic basis of UKBB participation. First, we conducted autosomal wGWA and standard GWA on biological sex and evaluated whether wGWA reduced sex-differential participation bias. As previously suggested23, autosomal heritability linked to biological sex could result from sex-differential participation. As such, reduced heritability estimates in wGWA compared with GWA would provide evidence for the utility of wGWA for participation bias correction. In addition, we compared the resulting SNP effects with the effects of previously identified sex-associated variants (P < 5 × 10−8). Here 49 variants assessed in an independent sample of >2,400,000 volunteers curated by 23andMe23 were selected.
Second, we conducted a genome-wide analysis on the liability to UKBB participation, by including the individual participation probabilities as the outcome of interest in wGWA. The application of standard GWA analysis is not possible in this context, as this approach stratifies for the outcome of interest by selecting a subset of the population willing to participate. LD-independent SNPs reaching genome-wide significance (P < 5 × 10−8) were selected via clumping (clump-kb, 250; clump-r2, 0.1; following standard recommendations43). PhenoScanner44, a database of genotype–phenotype associations from existing GWA studies, was used to explore previously identified associations of lead SNPs with other phenotypes. Genetic correlations with other traits were estimated using LD-score regression45 as implemented in the R package GenomicSEM46. The summary statistic files used in LD-score regression were obtained for 49 health and behavioural phenotypes, using publicly available summary statistic files accessible via consortia websites or the MRC-IEU OpenGWAS project (https://gwas.mrcieu.ac.uk)47 (see Supplementary Table 11 for the details).
LD score regression and heritability estimates
SNP heritability estimates were obtained for both the standard GWA and wGWA output (h2 and \(h_{\mathrm{w}}^2\), respectively) using LD score regression as implemented in GenomicSEM. We applied the default settings (restricted SNPs to minor allele frequency > 0.01, LD scores from the European-ancestry sample in the 1000 Genomes Project48). For binary phenotypes, the observed scale was converted to the liability scale49, where the population prevalence was set to be equal to the weighted prevalence in the UKBB. We also estimated bivariate genetic correlations among all phenotypes included in standard GWA and wGWA (rg and rg,w, respectively). To compare the estimates obtained from wGWA and standard GWA, we calculated the difference (rg,DIFF = rg − rg,w and \(h_{{\mathrm{DIFF}}}^2 = h^2 - h_{\mathrm{w}}^2\)) and used the following test statistic (here exemplified for rg,DIFF):
The correlation coefficients \(r(h^2,h_{\mathrm{w}}^2)\) and r(rg, rg,w) were obtained from 200-block jackknife analysis. For this, we split the genome into 200 equal blocks of SNPs and removed one block at a time to perform jackknife estimation.
MR analyses
To evaluate the impact of selection bias when using MR, we assessed whether sample weighting altered MR estimates. As genetic instruments, we selected LD-independent (clump-kb, 10,000; clump-r2, 0.001; adhering to standard MR protocols50) SNPs reaching genome-wide significance (P < 5 × 10−8) in either wGWA or standard GWA for a given phenotype. Phenotypes with few (<10) genetic instruments were not included in the MR analyses. We used the inverse-variance weighted (IVW) MR estimator, which combines the ratio estimates of the individual genetic variants Gj to derive the causal effect \((\hat \alpha _{{\mathrm{IVW}}})\). The ratio estimate is \(\hat \alpha _j = \hat \beta _j^{{\mathrm{OUT}}}/\hat \beta _j^{{\mathrm{EXP}}}\), where \(\hat \beta _j^{{\mathrm{EXP}}}\) corresponds to the SNP–exposure association and \(\hat \beta _j^{{\mathrm{OUT}}}\) corresponds to the SNP–outcome association. Since the IVW estimator assumes that the uncertainty in the genetic association with the exposure is zero, we used the following correction51 to account for selected genetic variants \((\hat \beta _j^{{\mathrm{EXP}}})\) that were genome-wide significant in one analysis (for example, standard GWA) but not the other (for example, wGWA) for the same trait: \(\hat \alpha _{{\mathrm{IVW,corrected}}} = \hat \alpha _{{\mathrm{IVW}}}\frac{{S^2}}{{\hat \sigma }}\), where \(S^2 = \frac{1}{{m - 1}}\mathop {\sum }\nolimits_{j = 1}^m \left( {\hat \beta _j^{{\mathrm{EXP}}} - \overline {\hat \beta _{{\mathrm{EXP}}}} } \,\right)^2\) and \(\hat \sigma ^2 = S^2 - \frac{1}{m}\mathop {\sum }\nolimits_{j = 1}^m {\mathrm{Var}}\left( {\hat \beta _j^{{\mathrm{EXP}}}} \right)\), where m refers to the number of SNPs selected as instruments. The corresponding variance was estimated as \({\mathrm{Var}}(\hat \alpha _{{\mathrm{IVW,corrected}}}) = {\mathrm{Var}}(\hat \alpha _{{\mathrm{IVW}}})\frac{{S^2}}{{\hat \sigma ^2}}\).
For each exposure–outcome association, we obtained (1) an MR estimate using the SNP effects from standard GWA analyses and (2) an MR estimate using the SNP effects from wGWA analyses. We included in MR the standardized SNP effects and standard errors (that is, the effect of the genotype on the standardized outcome), which were derived using the following formula52: \(\beta _{{\mathrm{STD}}} = Z/\sqrt {2p(1 - p)(n + Z^2)}\) and \({\mathrm{s.e.}}(\beta _{{\mathrm{STD}}}) = 1/\sqrt {2p(1 - p)(n + Z^2)}\), where n is the sample size, p is the minor allele frequency and Z is the SNP effect \(\hat \beta\) divided by its standard error (\(Z = \hat \beta /{\mathrm{s.e.}}(\hat \beta )\)). Of note, when standardizing the weighted estimates \((\hat \beta _{\mathrm{w}})\), n was replaced by the effective sample size (\(n_{\mathrm{effective}} = W^2 / \mathop {\sum }\nolimits_{i = 1}^N w_{in}^2\)) to account for the unequal contribution per observation. win refers to the normalized probability weights, obtained by dividing wi by its mean (\(w_{in} = w_i/ {\overline {w_i}}\)).
To compare the standard (\(\hat \alpha\)) to the weighted MR (\(\hat \alpha _{\mathrm{w}}\)) estimates, we estimated αDIFF (\(\hat \alpha - \hat \alpha _{\mathrm{w}}\)) and the corresponding test statistic as Z = αDIFF/s.e.(αDIFF), where
The correlation coefficient was derived using a jackknife procedure, where we performed MR leaving out each SNP in turn to then calculate the correlation \(r\left( {\hat \alpha ,\hat \alpha _{\mathrm{w}}} \right)\) from these results. The results were corrected for multiple testing using FDR correction (controlled at 5%), correcting for the total number of conducted MR analyses.
Reporting summary
Further information on research design is available in the Nature Portfolio Reporting Summary linked to this article.
Data availability
All summary statistic files generated using standard and weighted genome-wide analyses are accessible on the GWAS catalogue (https://www.ebi.ac.uk/gwas/) at the accession numbers GCST90267266 to GCST90267307. The UKBB probability weights generated as part of this study are available via the UK Biobank repositories.
Code availability
The following software was used to run the analyses: LDAK (http://dougspeed.com/downloads/; a tutorial on how to perform standard and weighted genome-wide analyses is available at https://tabeaschoeler.github.io/TS2021_UKBBweighting/wGWA.html), TwoSampleMR (https://mrcieu.github.io/TwoSampleMR/) and GenomicSEM (https://github.com/GenomicSEM/GenomicSEM). All analytical scripts are available at https://github.com/TabeaSchoeler/TS2021_UKBBweighting.
References
Abdellaoui, A. & Verweij, K. J. H. Dissecting polygenic signals from genome-wide association studies on human behaviour. Nat. Hum. Behav. 5, 686–694 (2021).
Sjaarda, J. & Kutalik, Z. Partner choice, confounding and trait convergence all contribute to phenotypic partner similarity. Nat. Hum. Behav. https://doi.org/10.1038/s41562-022-01500-w (2023).
Howe, L. J. et al. Within-sibship genome-wide association analyses decrease bias in estimates of direct genetic effects. Nat. Genet. 54, 581–592 (2022).
Border, R. et al. Assortative mating biases marker-based heritability estimators. Nat. Commun. 13, 660 (2022).
Fry, A. et al. Comparison of sociodemographic and health-related characteristics of UK Biobank participants with those of the general population. Am. J. Epidemiol. 186, 1026–1034 (2017).
Swanson, J. M. The UK Biobank and selection bias. Lancet 380, 110 (2012).
Hernán, M. A., Hernández-Díaz, S. & Robins, J. M. A structural approach to selection bias. Epidemiology 15, 615–625 (2004).
Knudsen, A. K., Hotopf, M., Skogen, J. C., Overland, S. & Mykletun, A. The health status of nonparticipants in a population-based health study: the Hordaland Health Study. Am. J. Epidemiol. 172, 1306–1314 (2010).
Drivsholm, T. et al. Representativeness in population-based studies: a detailed description of non-response in a Danish cohort study. Scand. J. Public Health 34, 623–631 (2006).
Bisgard, K. M., Folsom, A. R., Hong, C.-P. & Sellers, T. A. Mortality and cancer rates in nonrespondents to a prospective study of older women: 5-year follow-up. Am. J. Epidemiol. 139, 990–1000 (1994).
Manjer, J. et al. The Malmö diet and cancer study: representativity, cancer incidence and mortality in participants and non-participants. Eur. J. Cancer Prev. 10, 489–499 (2001).
van Alten, S., Domingue, B. W., Galama, T. & Marees, A. T. Reweighting the UK Biobank to reflect its underlying sampling population substantially reduces pervasive selection bias due to volunteering. Preprint at medRxiv https://doi.org/10.1101/2022.05.16.22275048 (2022).
Stamatakis, E. et al. Is cohort representativeness passé? Poststratified associations of lifestyle risk factors with mortality in the UK Biobank. Epidemiology 32, 179–188 (2021).
Davis, K. A. S. et al. Mental health in UK Biobank—development, implementation and results from an online questionnaire completed by 157 366 participants: a reanalysis. BJPsych Open 6, e18 (2020).
Batty, G. D., Gale, C. R., Kivimäki, M., Deary, I. J. & Bell, S. Comparison of risk factor associations in UK Biobank against representative, general population based studies with conventional response rates: prospective cohort study and individual participant meta-analysis. BMJ https://doi.org/10.1136/bmj.m131 (2020).
Munafò, M. R., Tilling, K., Taylor, A. E., Evans, D. M. & Davey Smith, G. Collider scope: when selection bias can substantially influence observed associations. Int. J. Epidemiol. 47, 226–235 (2018).
Wendt, F. R. et al. Using phenotype risk scores to enhance gene discovery for generalized anxiety disorder and posttraumatic stress disorder. Mol. Psychiatry https://doi.org/10.1038/s41380-022-01469-y (2022).
Mignogna, G. et al. Patterns of item nonresponse behavior to survey questionnaires are systematic and have a genetic basis. Preprint at bioRxiv https://doi.org/10.1101/2022.02.11.480140 (2022).
Tyrrell, J. et al. Genetic predictors of participation in optional components of UK Biobank. Nat. Commun. 12, 886 (2021).
Adams, M. J. et al. Factors associated with sharing e-mail information and mental health survey participation in large population cohorts. Int. J. Epidemiol. 49, 410–421 (2020).
Martin, J. et al. Association of genetic risk for schizophrenia with nonparticipation over time in a population-based cohort study. Am. J. Epidemiol. 183, 1149–1158 (2016).
Taylor, A. E. et al. Exploring the association of genetic factors with participation in the Avon Longitudinal Study of Parents and Children. Int. J. Epidemiol. 47, 1207–1216 (2018).
Pirastu, N. et al. Genetic analyses identify widespread sex-differential participation bias. Nat. Genet. 53, 663–671 (2021).
Benonisdottir, S. & Kong, A. The genetics of participation: method and analysis. Preprint at bioRxiv https://doi.org/10.1101/2022.02.11.480067 (2022).
Xue, A. et al. Genome-wide analyses of behavioural traits are subject to bias by misreports and longitudinal changes. Nat. Commun. 12, 988 (2021).
Sanderson, E., Richardson, T. G., Hemani, G. & Davey Smith, G. The use of negative control outcomes in Mendelian randomization to detect potential population stratification. Int. J. Epidemiol. 50, 1350–1361 (2021).
Lee, J. et al. Quantifying the causal impact of biological risk factors on healthcare costs. Preprint at medRxiv https://doi.org/10.1101/2022.11.19.22282356 (2022).
Allen, N. et al. UK Biobank: current status and what it means for epidemiology. Health Policy Technol. 1, 123–126 (2012).
Sudlow, C. et al. UK Biobank: an open access resource for identifying the causes of a wide range of complex diseases of middle and old age. PLoS Med. 12, e1001779 (2015).
Neale Lab. Rapid GWAS of thousands of phenotypes for 337,000 samples in the UK. Neale Lab blog http://www.nealelab.is/blog/2017/7/19/rapid-gwas-of-thousands-of-phenotypes-for-337000-samples-in-the-uk-biobank (2017).
Mindell, J. et al. Cohort profile: the Health Survey for England. Int. J. Epidemiol. 41, 1585–1593 (2012).
Health Survey for England 2018 (NHS Digital, 2018); https://digital.nhs.uk/data-and-information/publications/statistical/health-survey-for-england/2018
2011 Census Microdata (Office for National Statistics, 2011); https://www.ons.gov.uk/census/2011census/2011censusdata/censusmicrodata
Rosenbaum, P. & Rubin, D. The central role of the propensity score in observational studies for causal effects. Biometrika 70, 41–55 (1983).
Schonlau, M. & Couper, M. P. Options for conducting web surveys. Stat. Sci. 32, 279–292 (2017).
Hastie, T., Qian, J. & Tay, K. An introduction to glmnet. glmnet https://glmnet.stanford.edu/articles/glmnet.html (2021).
Zhang, Q., Privé, F., Vilhjálmsson, B. & Speed, D. Improved genetic prediction of complex traits from individual-level data or summary statistics. Nat. Commun. 12, 4192 (2021).
Speed, D., Holmes, J. & Balding, D. J. Evaluating and improving heritability models using summary statistics. Nat. Genet. 52, 458–462 (2020).
Lumley, T. Computing the (simplest) sandwich estimator incrementally. Biased and Inefficient https://notstatschat.rbind.io/2016/06/04/computing-the-simplest-sandwich-estimator-incrementally/ (2016).
von Hippel, P. Linear vs. logistic probability models: which is better, and when? Statistical Horizons https://statisticalhorizons.com/linear-vs-logistic/ (2015).
von Hippel, P. When can you fit a linear probability model? More often than you think. Statistical Horizons https://statisticalhorizons.com/when-can-you-fit/ (2017).
Howrigan, D., Abbott, L., Churchhouse, C., Palmer, D. & Neale, B. Details and considerations of the UK Biobank GWAS. Neale Lab blog http://www.nealelab.is/blog/2017/9/11/details-and-considerations-of-the-uk-biobank-gwas (2017).
Adam, Y., Samtal, C., Brandenburg, J., Falola, O. & Adebiyi, E. Performing post-genome-wide association study analysis: overview, challenges and recommendations. F1000Research 10, 1002 (2021).
Kamat, M. A. et al. PhenoScanner V2: an expanded tool for searching human genotype–phenotype associations. Bioinformatics 35, 4851–4853 (2019).
Bulik-Sullivan, B. K. et al. LD score regression distinguishes confounding from polygenicity in genome-wide association studies. Nat. Genet. 47, 291–295 (2015).
Grotzinger, A. D. et al. Genomic structural equation modelling provides insights into the multivariate genetic architecture of complex traits. Nat. Hum. Behav. 3, 513–525 (2019).
Elsworth, B. et al. The MRC IEU OpenGWAS data infrastructure. Preprint at bioRxiv https://doi.org/10.1101/2020.08.10.244293 (2020).
1000 Genomes Project Consortium An integrated map of genetic variation from 1,092 human genomes. Nature 491, 56–65 (2012).
Lee, S. H., Wray, N. R., Goddard, M. E. & Visscher, P. M. Estimating missing heritability for disease from genome-wide association studies. Am. J. Hum. Genet. 88, 294–305 (2011).
Rasooly, D. & Patel, C. J. Conducting a reproducible Mendelian randomization analysis using the R analytic statistical environment. Curr. Protoc. Hum. Genet. 101, e82 (2019).
Frost, C. & Thompson, S. G. Correcting for regression dilution bias: comparison of methods for a single predictor variable. J. R. Stat. Soc. A 163, 173–189 (2000).
Zhu, Z. et al. Integration of summary data from GWAS and eQTL studies predicts complex trait gene targets. Nat. Genet. 48, 481–487 (2016).
Acknowledgements
This research has been conducted with the UK Biobank Resource under application number 16389; we thank all biobank participants for sharing their data. We thank all participants involved in the Health Survey England and the 2011 Census Microdata, and we thank the Office for National Statistics for granting access to the data. This study would not have possible without the use of publicly available genome-wide summary data and software tools. We acknowledge these resources and thank the research participants, research teams and institutions that have contributed to this research. The computations were performed on the HPC cluster of the Lausanne University Hospital. We thank Y. Tillé for helpful discussions and relevant comments. Z.K. was funded by the Swiss National Science Foundation (grant no. 310030-189147). T.S. is funded by a Wellcome Trust Sir Henry Wellcome fellowship (grant no. 218641/Z/19/Z). For the purpose of open access, we have applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission. J.-B.P. has received funding from the European Research Council under the European Union’s Horizon 2020 research and innovation programme (grant agreement no. 863981) and is supported by the Medical Research Foundation 2018 Emerging Leaders 1st Prize in Adolescent Mental Health (grant no. MRF-160-0002-ELP-PINGA). D.S. is supported by the Aarhus University Research Foundation, by the Independent Research Fund Denmark under project no. 7025-00094B and by a Lundbeck Foundation Experiment Grant. The funders had no role in study design, data collection and analysis, decision to publish or preparation of the manuscript.
Funding
Open access funding provided by University of Lausanne.
Author information
Authors and Affiliations
Contributions
Z.K. and T.S. conceptualized the study. T.S. performed the statistical analyses. D.S. provided the software. Z.K., D.S., J.-B.P., E.P. and N.P. discussed the results and provided comments on the paper. All authors critically reviewed the manuscript.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Peer review
Peer review information
Nature Human Behaviour thanks Andrea Ganna, David Braudt and the other, anonymous, reviewer(s) for their contribution to the peer review of this work. Peer reviewer reports are available.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Supplementary Information
Supplementary Sections 1–5 and Figs. 1–9.
Supplementary Tables
Supplementary Tables 1–11.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Schoeler, T., Speed, D., Porcu, E. et al. Participation bias in the UK Biobank distorts genetic associations and downstream analyses. Nat Hum Behav 7, 1216–1227 (2023). https://doi.org/10.1038/s41562-023-01579-9
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41562-023-01579-9
This article is cited by
-
NHS Health Check attendance is associated with reduced multiorgan disease risk: a matched cohort study in the UK Biobank
BMC Medicine (2024)
-
Brain asymmetries from mid- to late life and hemispheric brain age
Nature Communications (2024)
-
Considerations for clinical implementation of polygenic risk scores in diverse US populations
Nature Medicine (2024)
-
Exome sequencing identifies genes associated with sleep-related traits
Nature Human Behaviour (2024)
-
Genetics of human brain development
Nature Reviews Genetics (2024)
