
Abstract
The ventricular arrhythmia (VA)–chronic obstructive pulmonary disease (COPD) association and related risk factors remain unclear. Using 2001–2012 data from National Health Insurance Research Database, we retrospectively reviewed 71,838 patients diagnosed as having COPD and 71,838 age- and sex-matched controls. After adjustments for comorbidities, medication, urbanization level, and monthly income, patients with COPD had higher incidence rates of VA than did the controls (adjusted hazard ratio [aHR] [95% confidence interval (CI)]: 1.45 [1.25–1.68]). More hospitalization or emergency visits because of acute COPD exacerbation (aHRs [95% CIs] for first, second, and third visits: 1.28 [1.08–1.50], 1.75 [1.32–2.32], and 1.88 [1.46–2.41], respectively) and asthma–COPD overlap (aHR [95% CI]: 1.49 [1.25–1.79]) were associated with high VA risk in patients with COPD. In the multivariate analysis, heart failure (aHR [95% CI]: 2.37 [1.79–3.14]), diabetes (aHR [95% CI]:1.64 [1.29–2.08]), age ≥75 (aHR [95% CI]: 2.48 [1.68–3.67]), male (aHR [95% CI]: 1.69[1.34–2.12]), and class III antiarrhythmic drug use (aHR [95% CI]: 2.49 [1.88–3.28]) are the most significant risk factors of new onset of VA in patients with COPD.
Similar content being viewed by others


Introduction
Chronic obstructive pulmonary disease (COPD) is a severe lung disease and a major cause of mortality and morbidity worldwide1. The causes of death in patients with COPD include acute or chronic respiratory failure, infection, coronary artery disease (CAD), heart failure (HF), and cardiac arrhythmia2,3. The major risk factors for mortality in patients with COPD are acute myocardial infarction (AMI) and underlying CAD2. Because COPD is associated with systemic inflammation, which initiates or aggravates comorbid diseases, cardiovascular disease and arrhythmia risks have been reported to be associated with COPD4,5,6,7. In previous studies, supraventricular arrhythmia, particularly atrial fibrillation, was the most common cardiac arrhythmia in patients with COPD6. However, in patients with acute COPD exacerbation, the most common arrhythmia was reported to be ventricular premature beats8. In addition, COPD and its severity have been reported as independent risk factors for ventricular tachycardia7,9. However, because of COPD complexities, such as comorbidities, prescribed medications, and asthma–COPD overlap (ACO) risk, the COPD–ventricular arrhythmia (VA) association remains unclear. In this study, VA risk in patients with COPD was assessed by analyzing nationwide population-based data.
Results
Baseline characteristics of the study population
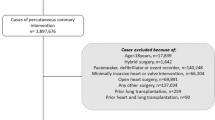
Records of 172,642 patients with COPD were retrieved, of which 71,838 patients met the inclusion criteria (mean age: 57.66 ± 16.61 years, 54% men). The control cohort was matched with the COPD cohort according to sex and age. The total follow-up duration was 491,198.3 and 497,038.3 person-years in the patient and control cohorts, respectively (Fig. 1).

Patients with newly diagnosed COPD since 2001 were matched with controls without COPD at the same index date as the date of diagnosis of COPD.
The baseline characteristics are shown in Table 1. Compared with the control cohort, patients with COPD had a higher prevalence of HF (3.77% vs. 7.44%, p < 0.001), AMI (0.96% vs. 1.38%, p < 0.001), stroke (10.96% vs. 16.85%, p < 0.001), ischemic heart disease (16.21% vs. 24.94%, p < 0.001), peripheral vascular disease (6.73% vs. 7.96%, p < 0.001), hypertension (34.96% vs. 43.77%, p < 0.001), diabetes (17.22% vs. 22.13%, p < 0.001), and renal failure (7.58% vs. 10.86%, p < 0.001) as well as higher CHA2DS2-VASc scores (score = 1: 27.81% vs. 29.48%; score ≥ 4: 21.70% vs. 24.35%, p < 0.001) and ORBIT scores (score = 0–2: 69.68% vs. 74.96%; score ≥ 4: 10.83% vs. 13.19%, p < 0.001).
With regard to the prescribed medication, patients with COPD exhibited a greater use of aspirin, statin, and renin–angiotensin–aldosterone system inhibitors (RAASi) than the controls did. In addition, compared with the control cohort, more patients with COPD were prescribed antiarrhythmic drugs (AADs); this difference was the largest for class II AADs (20.81% vs. 27.10%, p < 0.001) and class IV AADs (11.37% vs. 16.26%, p < 0.001).
VA incidence in patients with COPD
The cumulative and relative risks of VA in the patients and controls are presented in Table 2. Compared with the controls, patients with COPD demonstrated higher VA risk during the follow-up period (incidence rates: 57.5 and 98.6 per 105 person-years, respectively; adjusted hazard ratio [aHR]: 1.45; 95% confidence interval [CI]: 1.25–1.68; Fig. 2).

Data were stratified by COPD and non-COPD (log-rank test, χ2 = 31.254; df = 1; p < 0.001).
The subgroup effects in the patients with COPD and controls are shown in Table 2. The results showed that after adjustments for the comorbidities, level of urbanization, and monthly income, compared with controls, patients with COPD had higher VA risk (aHR [95% CI]: 1.45 [1.25–1.68]). Compared with the control cohort, patients with COPD without HF, AMI, angina, peripheral vascular disease, or renal failure had a significantly higher VA risk (aHRs [95% CIs]: 1.51 [1.28–1.77], 1.45 [1.24–1.68], 1.48 [1.26–1.74], and 1.47 [1.26–1.73], respectively). All patients with COPD, irrespective of whether they had ischemic heart disease, hypertension and diabetes, or chronic liver disease, had increased VA risk. Patients with COPD with lower CHA2DS2-VASc scores had higher VA risk (aHRs [95% CIs]: 2.55 [1.48–4.38], 1.36 [0.94–1.95], 1.46 [1.12–1.89], and 1.26 [1.00–1.59] for CHA2DS2-VASc scores of 0, 1, 2, and 3, ≥4, respectively) than control cohort with same CHA2DS2-VASc scores. Compared with the control cohort, patients with COPD with lower ORBIT scores also had higher VA risk (aHRs [95% CIs]: 1.51 [1.26–1.82], 1.24 [0.86–1.79], 1.38 [0.96–1.97] for ORBIT scores 0–2, 3, and ≥4, respectively).
Effect of hospitalization and emergency department visits
Table 3 presents the effects of acute COPD exacerbation on the occurrence of VA. VA risk in patients with COPD increased with each hospitalization or emergency visit because of acute COPD exacerbation. For the first, second, and third visits (whether for hospitalization or an emergency visit), the crude HRs (95% CIs) were 1.35 (1.15–1.59), 3.38 (2.57–4.44), and 4.39 (3.49–5.53), respectively, whereas the aHRs (95% CIs) were 1.29 (1.09–1.52), 1.86 (1.41–2.46), and 2.13 (1.68–2.71), respectively; moreover, after adjustments for the additional drugs prescribed, the aHRs (95% CIs) became 1.28 (1.09–1.52), 1.75 (1.32–2.32), and 1.88 (1.46–2.41), respectively. Notably, the risk remained high in the subgroup analysis when the cohorts were stratified by age or sex. The stratified analysis indicated that in patients with COPD who were hospitalized or made an emergency visit for acute COPD exacerbation, young to middle-aged men had relatively high VA risk. Compared with other patients, young to middle-aged patients with COPD had a higher incidence rate of VA because of acute COPD exacerbation (aHRs [95% CIs] of 20–64-year-old patients: 1.53 [1.17–1.99], 2.04 [1.14–3.65], and 2.91 [1.71–4.94] for the first, second, and third visit, respectively). The men with COPD had a higher incidence rate of VA than did the women with COPD (aHRs [95% CIs]: 1.31 [1.04–1.65], 1.80 [1.25–3.65], and 1.91 [1.45–2.69] for the first, second, and third visit, respectively).
Patients who never had to visit the emergency department or get admitted because of acute exacerbation (COPD on an outpatient basis alone) did not have a significantly increased VA risk compared with the controls, except for patients with a history of diabetes and renal failure (aHRs [95% CIs]: 2.07 [1.19–3.60] and 2.83 [1.52–5.27], respectively).
The frequency of acute exacerbation had more impact on patients without HF, AMI, stroke, ischemic heart disease, angina, peripheral vascular disease, diabetes, and renal failure (aHRs [95% CIs] at the first, second, and third instance of acute exacerbation: 1.34 [1.12–1.60], 1.78 [1.28–2.49], and 2.24 [1.70–2.95], respectively; 1.28 [1.08–1.52], 1.84 [1.38–2.44], and 1.90 [1.47–2.44], respectively; 1.41 [1.14–1.73], 2.35 [1.65–3.36], and 2.51 [1.84–3.43], respectively; 1.33 [1.11–1.58], 2.02 [1.50–2.72], and 1.88 [1.42–2.47], respectively; 1.29 [1.08–1.54], 1.87 [1.39–2.52], 1.89 [1.44–2.46], respectively; 1.32 [1.09–1.61], 1.86 [1.32–2.64], and 2.07 [1.54–2.78], respectively; and 1.40 [1.17–1.67], 2.02 [1.49–2.73], 2.17 [1.66-2.84], respectively). More visits to the emergency department or hospitalizations because of acute COPD exacerbation were associated with lower VA-free survival rate during follow-up (Fig. 3).

Data were stratified by the frequency of COPD acute exacerbations (log-rank test, χ2 = 198.964; df = 3; p < 0.001).
Analysis of patients with ACO
Compared with patients diagnosed as having COPD alone, those diagnosed as having ACO had higher VA risk (aHR [95% CI]: 1.55 [1.30–1.85]; Table 4). The risk remained higher in the ACO group after adjustments for the medication prescribed (aHR [95% CI]: 1.49 [1.25–1.79]). The subgroup analysis revealed that young to middle-aged patients with ACO had higher VA risk than did older patients (aHRs [95% CIs]: 1.67 [1.23–2.27] and 1.45 [1.05–2.01], respectively). Male patients demonstrated higher VA risk than did female patients (aHRs [95% CI]: 1.60 [1.26–2.04] and 1.48 [1.14–1.91], respectively). Patients without HF, AMI, ischemic heart disease, angina, peripheral vascular disease, and renal failure had significantly VA risk (aHRs [95% CIs]: 1.71 [1.41–2.06], 1.56 [1.31–1.87], 1.76 [1.41–2.21], 1.59 [1.31–1.92], 1.56 [1.29–1.88], and 1.68 [1.39–2.04], respectively). VA risk was significantly higher in patients with and without hypertension, diabetes, or stroke. However, higher VA risk was observed in patients without these diseases (aHRs [95% CIs] for those with and without hypertension, diabetes, and stroke: 1.39 [1.35–2.43] and 1.81 [1.35–2.43], respectively; 1.44 [1.05–1.98] and 1.59 [1.29–1.96], respectively; and 1.50 [1.05–2.15] and 1.55 [1.27–1.90], respectively). Patients with ACO exhibited poorer long-term outcomes than those with COPD did (Fig. 4).

Data were stratified as non-COPD, COPD alone, and ACO (log-rank test, χ2 = 34.859; df = 2; p < 0.001).
Analysis of different classes of antiarrhythmic drugs
In the univariate analysis, all patients with COPD who were prescribed class I–IV AADs exhibited high VA risk (HRs [95% CIs] for class I, II, III, and IV: 3.19 [2.16–4.72], 2.00 [1.64–2.44], 6.34 [4.94–8.14], and 2.53 [2.03–3.15], respectively). The only available class III AAD in Taiwan is amiodarone (Table 5).
Effect of COPD inhalation medications
No significantly increased VA risk was observed in patients with COPD who had been prescribed short-acting beta-agonists (SABAs), long-acting beta-agonists (LABAs), long-acting muscarinic antagonists (LAMAs), inhalation corticosteroids (ICSs), or LABA–ICS combination therapy. Patients with COPD who were prescribed SABA–short-acting muscarinic antagonist (SAMA) combination therapy had lower VA risk (HR [95% CI]: 0.62 [0.47–0.82]; Supplementary Table).
Predictor of new-onset VA in patients with COPD
The multivariate analysis indicated that new-onset VA risk was significantly higher in patients with COPD aged 65–74 (HR [95% CI]: 1.62 [1.17–2.23], p = 0.003) or ≥75 (HR [95% CI]: 2.48 [1.68–3.67], p < 0.001) years; male patients (HR [95% CI]: 1.69 [1.34–2.12], p < 0.001); and patients with HF (HR [95% CI]: 2.37 [1.79–3.14], p < 0.001), AMI (HR [95% CI]:1.84 [1.09–3.11], p = 0.02), stroke (HR [95% CI]: 1.48 [1.14–1.93], p = 0.003), hypertension (HR [95% CI]: 1.66 [1.22–2.27], p = 0.001), diabetes (HR [95% CI]: 1.64 [1.29–2.08], p < 0.001), and history of class III AAD use (HR [95% CI]: 2.49 [1.88–3.28], p < 0.001) (Table 5).
Discussion
The present nationwide population-based study showed that compared with the controls, patients with COPD had a significantly higher VA incidence after adjustments for comorbidities, medications, monthly income, and urbanization level. In addition, VA occurrence in patients with COPD increased with the frequency of hospitalization or emergency department visits. Further, the incidence of VA increases with the complexity of airway diseases. Finally, age, chronic or acute heart disease, stroke, hypertension, and amiodarone prescription were VA predictors in patients with COPD. To the best of our knowledge, the present study involved the largest COPD cohort that has been investigated for VA risk thus far.
Studies have demonstrated high VA risk in patients with COPD7,9. COPD is also associated with sudden cardiac death10. According to 24-h Holter recordings, patients with COPD had a higher prevalence of sustained or nonsustained ventricular tachycardia, and COPD severity was associated with the burden of ventricular tachycardia7,9. In the present study, compared with controls, patients with COPD were at higher risk of developing VA in the future, and the risk was not affected by comorbidities or medication. The autonomic system, hypoxemic status, and beta-agonist inhalation are factors that cause arrhythmogenicity in patients with COPD11,12,13. In addition, a significantly higher T-wave peak-to-end interval also puts patients with COPD into proarrhythmic status14,15.
The majority of inhalation medications for COPD used in the present study were not associated with increased fatal VA risk. Bronchodilators could increase supraventricular arrythmia risk, but they did not increase the risk of fatal arrythmias such as ventricular fibrillation, ventricular flutter, or sudden cardiac death13. However, we observed that SABA–SAMA combination therapy helped reduce VA risk. This could be attributed to several reasons. First, the combination of SABA–SAMA inhalation medication was administered mainly during the acute exacerbation stage of COPD. Relief of bronchoconstriction and prevention of further respiratory complications might reduce the risk of occurrence of cardiovascular complications, including VA. Second, SABA–SAMA combination therapy could effectively reduce the hyperdynamic inflation in COPD, which might improve cardiovascular outcomes16,17,18,19.
In the present study, VA risk increased with the frequency of emergency department visits or hospitalization. According to Konecny et al.9, nonsustained or sustained ventricular tachycardia risk increased with COPD severity. In addition to the determination of pulmonary function through spirometry, increased episodes of acute COPD exacerbation was associated with poorer outcomes20. Hirayama et al.21 demonstrated that the risk of hospitalization or emergency events related to atrial fibrillation increased with the frequency of acute COPD exacerbations. In addition, patients with COPD who had no history of emergency department visits or hospitalizations because of acute exacerbation did not show increased VA incidence. Therefore, maintaining a stable status and avoiding episodes of acute exacerbation are essential for reducing VA risk. Furthermore, the present study reported different outcomes in patients with different complexities of airway diseases. Compared with patients with COPD alone, patients with ACO had higher VA risk, and the effects of the complexity remained slightly high after adjustments for comorbidities and medications. A study demonstrated that patients with ACO were more likely to be young; female; and have multiple comorbidities, high obesity risk, or low socioeconomic status22. Despite the conflicting results reported in the literature, the long-term mortality, morbidity, and decline of lung function remained critical concerns in patients with ACO22. Yeh et al.23 demonstrated that compared with patients without ACO, those with ACO had higher cardiac arrhythmia risk, although the types of arrhythmia were not distinguished. To the best of our knowledge, the present study is the first to focus on the effects of ACO on VA occurrence. The results of this study suggest that a more detailed analysis of the relationship between the complexity of lung disease and arrhythmia is required.
CHA2DS2-VASc scores are known to predict ischemic stroke risk in patients with atrial fibrillation. Moreover, a previous study validated the utility of CHA2DS2-VASc scores for predicting major adverse cardiovascular event risk in patients with COPD24. In the present study, patients with lower CHA2DS2-VASc scores or ORBIT scores had significant high VA risk than non-COPD patients with same score. While both scores increased, the difference of risk of VA occurrence became less even non-significant. This indicated that in patients with less comorbidities, the association between COPD and unstable VA became more significant. In the further multivariate analysis, CHA2DS2-VASc scores or ORBIT scores had no significant difference for predicting new-onset VA in patients with COPD.
The multivariate analysis indicated that age >65 years; male sex; previous HF; and a history of stroke, AMI, hypertension, and diabetes mellitus predicted VA risk in patients with COPD. These risk factors are also well-known factors associated with atherosclerotic disease. VA is a complication that occurs in patients with CAD25. The major therapies for VA include AAD use, implantable cardioverter defibrillators, and catheter ablation25,26. Notably, in our study cohort, the use of class III AADs in patients with COPD was associated with high VA risk. The only class III AAD available in Taiwan is amiodarone, which is widely used for treating arrhythmia in patients with COPD, particularly in patients who cannot tolerate beta-blockers or calcium channel blockers. The association between amiodarone and high VA risk could have several possible explanations. First, amiodarone was reported to exhibit pulmonary toxicity, which may occur even at low doses27. A study reported that arrhythmia risk may increase with a decline in respiratory function in patients with COPD, even if their left ventricular function is intact28. Second, amiodarone is an AAD that can cause prolongation of the QT interval. In patients with COPD, an increase in the severity of disease is associated with a prolonged QT interval29. In addition, the QT interval was noted to be associated with mortality, and it is significantly prolonged in the acute stage of COPD30. Excess prolongation of QT intervals increases the risk of VAs such as torsades de pointes31.
The present study has several limitations. First, this was a retrospective study, and information on several critical factors, such as direct measurements of pulmonary function and COPD stage, could not be obtained. Rather than direct measurements of COPD severity, emergency department visit and hospitalization frequencies were considered, because acute COPD exacerbation is an indication of COPD severity. In addition, the presence of ACO indicated the complexity of the disease. Second, other possible causes of VA, such as acid–base status, electrolyte levels, renal function, and levels of cardiac biomarkers (e.g., troponin, creatinine kinase, and B-type natriuretic peptide) could not be determined. Using propensity matching, most of the diseases associated with abnormalities in the aforementioned laboratory data were adjusted and equalized in both cohorts. In addition, biomarkers have limited clinical applicability and debatable utility as predictors of sudden death32. Finally, some medications that have been demonstrated to reduce VA risk, such as angiotensin–neprilysin inhibitors33, were not investigated in the present study, because these drugs were not available in Taiwan from 2008 to 2012. We adjusted for all other medications that had been used for the treatment of cardiovascular disease according to the applicable guidelines34,35,36,37.
In conclusion, in the present nationwide population-based cohort study, the presence of COPD, acute COPD exacerbation, and airway disease complexity were positively associated with VA risk. In addition to risk factors that are similar to CAD, male and class III AAD use were found to be crucial associated risk factors for VA.
Methods
The National Health Insurance (NHI) program, established in 1995, provides health insurance coverage to >98% of the population of Taiwan (which approximately 23 million). The NHI Research Database (NHIRD) has been extensively analyzed and validated previously38,39. The NHIRD research committee and the Joint Institutional Review Board of Taipei Medical University approved our study protocol (TMU-JIRB No. N201905004) and waived the need for informed consents from participants. This waiver does not affect the rights and welfare of the participants.
Study cohort
Patients were included in this study if they were diagnosed as having COPD between 1 January 2001 and 31 December 2012, had at least two COPD diagnoses as inpatients or outpatients, and were aged >20 years. A control cohort was selected by blinding the outcome, using SAS (version 9.4, SAS, Cary, NC, USA). Each patient with COPD was matched for birth date and sex with a control who did not have COPD, to compare the incidence of VA. Any individual with prior VA in a matched pair was excluded. In total, 143,676 matched pairs were obtained, comprising individuals in the COPD and control cohorts. The cohort entry date (index date) for patients with COPD was defined as the date of first COPD diagnosis. ACO was defined as COPD diagnosis with a concurrent diagnosis of asthma, with at least two outpatient visits or one admission40. The matched pair had the same date of diagnosis of COPD (index date) for follow-up. All patients were followed up until one of the following occurred: an initial diagnosis of ventricular tachycardia (ICD-9-CM code 427.1), ventricular fibrillation, or ventricular flutter (ICD-9-CM code 427.4, 427.41, or 427.42); loss to follow-up; death; withdrawal from the NHI program; or 31 December 2012. Patients who were diagnosed as having only ventricular premature beats (ICD-9-CM code 427.69) during the follow-up period were not enrolled.
Potential confounders
The cohort was also classified based on sociodemographic characteristics of the participants, such as age (20–64, 65–74, and ≥75 years), sex, urbanization level (urban, suburban, and rural), and monthly income (US$0, US$0.03–US$700, US$700–US$1,100, and ≥US$1,100). The following diagnoses were used to establish the history of baseline comorbidities for each participant: CHA2DS2-VASc scores—comprising age, sex, congestive HF history, hypertension history, stroke history, vascular disease history, and diabetes history—grouped into four segments (0, 1, 2–3, and ≥4)41,42; ORBIT scores—comprising sex, age, bleeding history, glomerular filtration rate (<60 mL/min/1.73 m2)— grouped into three segments (0–2, 3, and ≥4)43; HF; AMI; stroke; ischemic heart disease; angina; peripheral vascular disease; hypertension; diabetes; depression; renal failure; chronic liver disease; and dementia. Use of the following medications was also controlled for: aspirin; statin; RAASi; and AADs of class I (sodium channel blockers), class II (beta-blockers), class III (potassium channel blockers), and class IV (calcium channel blockers).
We also evaluated the effects of severity of COPD on the occurrence of VA. ACO, a mixed-type airway disease, was evaluated as a risk factor.
Statistical analysis
The aforementioned baseline patient characteristics are presented in Table 1. Categorical variables were reported as percentages and number of occurrences, and quantitative variables were reported as their mean ± standard deviation. The t-test and chi-square test were used to compare the COPD and control cohorts. To determine VA risk in the COPD and control cohorts, a Cox proportional hazards model was used to calculate the HRs and 95% CIs. HRs were adjusted with respect to the aforementioned confounders. Stratified analysis was conducted with the data segmented by age and sex (Table 2). The Cox proportional hazards model was used to estimate the risk of various VA types, with respect to the number of acute exacerbations (Table 3) and complexity (Table 4), in the COPD and control cohorts. Finally, multivariate analysis was used to estimate the association of sociodemographic characteristics, comorbidity, and medications with VA risk (Table 5). Using the Kaplan–Meier method, the VA-free survival rates for the COPD and control cohorts were compared. To examine the effects of hospital admission or emergency department visits (because of acute COPD exacerbation) on VA-free survival rate, we categorized the patients into four groups according to their COPD status (0, 1, 2, and ≥3). To examine the effects of the severity of COPD on VA-free survival rate, we categorized the patients into three groups according to their COPD status: without COPD, with COPD alone, and with ACO. All analyses were performed using SAS, and two-tailed p values <0.05 indicated statistical significance.
Reporting summary
Further information on experimental design is available in the Nature Research Reporting Summary linked to this article.
Data availability
The data supporting the findings of the present research were sourced from NHIRD in Taiwan. Owing to the legal restrictions imposed by the Government of Taiwan related to the Personal Information Protection Act, the database cannot be made publicly available. However, with reasonable request from authors and with permission from Taiwan NHIRD, the relevant data are available.
Code availability
No custom codes or software were developed in this study.
References
Lozano, R. et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 380, 2095–2128 (2012).
Hansell, A. L., Walk, J. A. & Soriano, J. B. What do chronic obstructive pulmonary disease patients die from? A multiple cause coding analysis. Eur. Respir. J. 22, 809–814 (2003).
Zielinski, J. et al. Causes of death in patients with COPD and chronic respiratory failure. Monaldi Archiv. Chest Dis. [Archiv. Monaldi malattie torace] 52, 43–47 (1997).
Laratta, C. R. & van Eeden, S. Acute exacerbation of chronic obstructive pulmonary disease: cardiovascular links. BioMed. Res. Int. 2014, 528789 (2014).
Miravitlles, M. et al. Comorbidities of patients in tiotropium clinical trials: comparison with observational studies of patients with chronic obstructive pulmonary disease. Int. J. Chron. Obstr. Pulm. Dis. 10, 549–564 (2015).
Desai, R. et al. The burden and impact of arrhythmia in chronic obstructive pulmonary disease: insights from the National Inpatient Sample. Int. J. Cardiol. 281, 49–55 (2019).
Konecny, T. et al. Chronic obstructive pulmonary disease as a risk factor for ventricular arrhythmias independent of left ventricular function. Heart Rhythm 15, 832–838 (2018).
Rusinowicz, T., Zielonka, T. M. & Zycinska, K. Cardiac arrhythmias in patients with exacerbation of COPD. Adv. Exp. Med. Biol. 1022, 53–62 (2017).
Konecny, T. et al. Relation of chronic obstructive pulmonary disease to atrial and ventricular arrhythmias. Am. J. Cardiol. 114, 272–277 (2014).
Narayanan, K. et al. Chronic obstructive pulmonary disease and risk of sudden cardiac death. JACC Clin. Electrophysiol. 1, 381–387 (2015).
Tükek, T. et al. Effect of diurnal variability of heart rate on development of arrhythmia in patients with chronic obstructive pulmonary disease. Int. J. Cardiol. 88, 199–206 (2003).
Krause, P. C., Inoue, H. & Zipes, D. P. Electrophysiologic alterations produced by hypoxia in the canine heart. Am. Heart J. 117, 550–561 (1989).
Wilchesky, M., Ernst, P., Brophy, J. M., Platt, R. W. & Suissa, S. Bronchodilator use and the risk of arrhythmia in COPD: Part 2: Reassessment in the larger Quebec cohort. Chest 142, 305–311 (2012).
Tural Onur, S., Emet, S., Sokucu, S. N. & Onur, I. T wave peak-to-end interval in COPD. Int. J. Chron. Obstruct. Pulm. Dis. 13, 2157–2162 (2018).
Cosgun, A., Oren, H. & Turkkani, M. H. The relationship between systolic pulmonary arterial pressure and Tp-e interval, Tp-e/QT, and Tp-e/QTc ratios in patients with newly diagnosed chronic obstructive pulmonary disease. Ann. Noninvasive Electrocardiol. 25, e12691 (2020).
Fujimoto, K. et al. Effects of bronchodilators on dynamic hyperinflation following hyperventilation in patients with COPD. Respirology 12, 93–99 (2007).
Kitaguchi, Y. et al. Additive efficacy of short-acting bronchodilators on dynamic hyperinflation and exercise tolerance in stable COPD patients treated with long-acting bronchodilators. Respir. Med. 107, 394–400 (2013).
Tzani, P. et al. Dynamic hyperinflation is associated with a poor cardiovascular response to exercise in COPD patients. Respir. Res. 12, 150 (2011).
Vassaux, C. et al. Effects of hyperinflation on the oxygen pulse as a marker of cardiac performance in COPD. Eur. Respir. J. 32, 1275–1282 (2008).
Groenewegen, K. H., Schols, A. M. & Wouters, E. F. Mortality and mortality-related factors after hospitalization for acute exacerbation of COPD. Chest 124, 459–467 (2003).
Hirayama, A. et al. Acute exacerbation of chronic obstructive pulmonary disease and subsequent risk of emergency department visits and hospitalizations for atrial fibrillation. Circ. Arrhythm. Electrophysiol. 11, e006322 (2018).
Leung, J. M. & Sin, D. D. Asthma-COPD overlap syndrome: pathogenesis, clinical features, and therapeutic targets. BMJ 358, j3772 (2017).
Yeh, J. J., Wei, Y. F., Lin, C. L. & Hsu, W. H. Association of asthma-chronic obstructive pulmonary disease overlap syndrome with coronary artery disease, cardiac dysrhythmia and heart failure: a population-based retrospective cohort study. BMJ Open 7, e017657 (2017).
Ooi, H. et al. CHA2DS2-VASc scores predict major adverse cardiovascular events in patients with chronic obstructive pulmonary disease. Clin. Respir. J. 12, 1038–1045 (2018).
Lo, R., Chia, K. K. & Hsia, H. H. Ventricular tachycardia in ischemic heart disease. Card. Electrophysiol. Clin. 9, 25–46 (2017).
Santangeli, P. et al. Comparative effectiveness of antiarrhythmic drugs and catheter ablation for the prevention of recurrent ventricular tachycardia in patients with implantable cardioverter-defibrillators: a systematic review and meta-analysis of randomized controlled trials. Heart Rhythm 13, 1552–1559 (2016).
Ott, M. C., Khoor, A., Leventhal, J. P., Paterick, T. E. & Burger, C. D. Pulmonary toxicity in patients receiving low-dose amiodarone. Chest 123, 646–651 (2003).
Kang, H. et al. The relationship between chronic atrial fibrillation and reduced pulmonary function in cases of preserved left ventricular systolic function. Korean Circ. J. 39, 372–377 (2009).
Nilsson, U., Kanerud, I., Diamant, U.-B., Johansson, B. & Lindberg, A. The prevalence of QTc-prolongation increase by GOLD stage in COPD. Eur. Respir. J. 50, PA1568 (2017).
Van Oekelen, O. et al. Significance of prolonged QTc in acute exacerbations of COPD requiring hospitalization. Int. J. Chron. Obstruct. Pulm. Dis. 13, 1937–1947 (2018).
Trinkley, K. E., Page, R. L. II, Lien, H., Yamanouye, K. & Tisdale, J. E. QT interval prolongation and the risk of torsades de pointes: essentials for clinicians. Curr. Med. Res. Opin. 29, 1719–1726 (2013).
Havmöller, R. & Chugh, S. S. Plasma biomarkers for prediction of sudden cardiac death: another piece of the risk stratification puzzle? Circ. Arrhythm. Electrophysiol. 5, 237–243 (2012).
de Diego, C. et al. Effects of angiotensin-neprilysin inhibition compared to angiotensin inhibition on ventricular arrhythmias in reduced ejection fraction patients under continuous remote monitoring of implantable defibrillator devices. Heart Rhythm 15, 395–402 (2018).
Priori, S. G. et al. 2015 ESC Guidelines for the management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: The Task Force for the Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death of the European Society of Cardiology (ESC). Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC). Eur. Heart J. 36, 2793–2867 (2015).
Knuuti, J. et al. ESC guidelines for the diagnosis and management of chronic coronary syndromes. Eur. Heart J. 41, 407–477 (2019).
Al-Khatib, S. M. et al. 2017 AHA/ACC/HRS guideline for management of patients with ventricular arrhythmias and the prevention of sudden cardiac death: executive summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society. Heart Rhythm 15, e190–e252 (2018).
Fihn, S. D. et al. 2014 ACC/AHA/AATS/PCNA/SCAI/STS focused update of the guideline for the diagnosis and management of patients with stable ischemic heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines, and the American Association for Thoracic Surgery, Preventive Cardiovascular Nurses Association, Society for Cardiovascular Angiography and Interventions, and Society of Thoracic Surgeons. J. Am. Coll. Cardiol. 64, 1929–1949 (2014).
Liu, J. C. et al. Influenza vaccination reduces hemorrhagic stroke risk in patients with atrial fibrillation: a population-based cohort study. Int J. Cardiol. 232, 315–332 (2017).
Chen, C. C. et al. Statins dose-dependently exert significant chemopreventive effects against various cancers in chronic obstructive pulmonary disease patients: a population-based cohort study. J. Cancer 7, 1892–1900 (2016).
Shantakumar, S. et al. Burden of asthma and COPD overlap (ACO) in Taiwan: a nationwide population-based study. BMC Pulm. Med. 18, 16 (2018).
Kuo, L. et al. Usefulness of the CHA2DS2-VASc score to predict the risk of sudden cardiac death and ventricular arrhythmias in patients with atrial fibrillation. Am. J. Cardiol. 122, 2049–2054 (2018).
Kurtul, A. & Acikgoz, S. K. Validation of the CHA2DS2-VASc score in predicting coronary atherosclerotic burden and in-hospital mortality in patients with acute coronary syndrome. Am. J. Cardiol. 120, 8–14 (2017).
Simon, D. N. et al. The ORBIT bleeding score: a simple bedside score to assess bleeding risk in atrial fibrillation. Eur. Heart J. 36, 3258–3264 (2015).
Acknowledgements
This work was supported in part by the Ministry of Science and Technology, Taiwan, under grant no. MOST 108-2745-8-038-001. The funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript. This manuscript was edited by Wallace Academic Editing.
Author information
Authors and Affiliations
Contributions
L.C.S. and J.-C.L. are the guarantors of this paper. Study conception and design: C.-C.C-, C.-H.L.; acquisition of data: Y.-A.F.; analysis and interpretation of data: Y.-A.F., L.-C.S., W.-R.H., C.-C.C.; manuscript drafting and critical review: all authors; final approval of the manuscript: all authors.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Chen, CC., Lin, CH., Hao, WR. et al. Association between chronic obstructive pulmonary disease and ventricular arrhythmia: a nationwide population-based cohort study. npj Prim. Care Respir. Med. 31, 8 (2021). https://doi.org/10.1038/s41533-021-00221-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41533-021-00221-3
