
Abstract
The British Thoracic Society (BTS) Guidelines for Bronchiectasis in adults were published in January 2019, and comprise recommendations for treatment from primary to tertiary care. Here, we outline the practical implications of these guidelines for primary care practitioners. A diagnosis of bronchiectasis should be considered when a patient presents with a recurrent or persistent (>8 weeks) productive cough. A definitive diagnosis is made by using thin-section chest computed tomography (CT). Once diagnosed, patients should be initially assessed by a specialist respiratory team and a shared management plan formulated with the patient, the specialist and primary care teams. The cornerstone of primary care management is physiotherapy to improve airway sputum clearance and maximise exercise capacity, with prompt treatment of acute exacerbations with antibiotics.
Similar content being viewed by others

Introduction
Bronchiectasis is a condition where patients have symptoms of persistent or recurrent bronchial sepsis related to irreversibly damaged and dilated bronchi.1 The incidence and prevalence of bronchiectasis is rising. Using the Clinical Practice Research Datalink (CPRD) in the United Kingdom, patients 18 and over with a Read code of Bronchiectasis were identified, and the point prevalence in February each year from 2004 to 2013 was measured. This showed that the point prevalence of coded bronchiectasis rose from 351 to 566 per 100,000 in women and from 301 to 486 per 100,000 in males between 2004 and 2013.2 A retrospective study using healthcare data from the United States showed a rise in prevalence of 8% between 2001 and 2012, but with a point prevalence of 139/100,000.3 The British Thoracic Society (BTS) Guideline for non-cystic fibrosis (non-CF) bronchiectasis was published in 20104 and included children. The BTS commissioned an update to the guidelines in 2013 to take into account any new evidence. The new BTS Guideline covers bronchiectasis in adults and provides recommendations and good practice points based on an updated evidence review.1
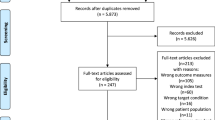
Systematic electronic database searches of relevant literature were carried out in June 2014 and June 2016, identifying relevant papers published since the previous guideline. In total, 1799 such papers were identified and reviewed by pairs of Guideline Committee members. Appraisal of the evidence was carried out based on Scottish Intercollegiate Guidelines Network (SIGN) methodology, as set out in the BTS Guideline Production Manual.5 The reliability of the evidence in each individual study was graded, using the SIGN critical appraisal checklists and levels of evidence assigned to evidence statements, according to the levels of evidence in Table 1.5,6 Recommendations made by the Guideline Committee were formulated based on the evidence statements and graded according to the SIGN grading system (Table 2).6
The composition of the Guideline Committee and the subsequent guideline recommendations were biased towards secondary care. One member of the Guideline Committee (KGJ—lead author of this paper) was from primary care. This paper acknowledges this and with five primary care authors aims to look at the relevance of the guidelines for primary care.
Initial presentation of bronchiectasis
A diagnosis of bronchiectasis should be suspected when a patient presents with a recurrent or persistent (>8 weeks) cough, with production of purulent or mucopurulent sputum, particularly with the relevant associated risk factors, such as COPD. This diagnosis is particularly likely if the patient has a history of two or more COPD exacerbations per year and a previous positive sputum sample for Pseudomonas aeruginosa whilst stable (i.e. not during an exacerbation).1
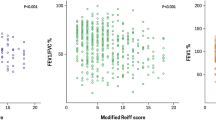
A meta-analysis of six observational studies of 881 patients, mainly based on secondary care, found that the prevalence of bronchiectasis was 54.3% in patients with COPD.7 One study conducted in 110 patients from 29 UK general practices showed that the prevalence of bronchiectasis was 29% in patients with COPD.8 Patients with bronchiectasis and COPD had a lower FEV1-weighted mean difference (WMD)—8%, more frequent exacerbations (WMD 1.54 times more in the previous year) and 7.33 times more likely to have persistent sputum pathogens, especially P. aeruginosa than COPD patients without bronchiectasis.7
In addition to coincident presentation with COPD, a diagnosis of bronchiectasis should be suspected in patients presenting with persistent cough, who also report difficult-to-treat asthma,9 rheumatoid arthritis,10 inflammatory bowel disease (IBD),11 chronic rhinosinusitis12 or the presence of persistent sputum pathogens, especially P. aeruginosa.1
History, examination and investigations
If bronchiectasis is suspected in a patient in a primary care setting, a full medical history and examination should be first directed to exclude other causes of cough, such as COPD, lung cancer, asthma and gastro-oesophageal reflux. Persistent basal, coarse lung crackles may be present.
Investigations in the primary care setting should encompass:
-
Diagnostic spirometry to look for other/coexistent diagnoses (such as COPD) and may be normal, restrictive or obstructive.
-
Sputum microbiology is helpful in identifying the presence of persistent pathogens, especially P. aeruginosa (indicating a worse prognosis).
-
A chest X-ray should be carried out to help exclude alternative diagnoses, but has limited sensitivity for diagnosing bronchiectasis, especially in mild disease.
-
Definitive diagnosis of bronchiectasis is made, using thin-section CT scanning of the chest. It is highly accurate and diagnostic for bronchiectasis, with false-positive and false- negative rates of 1% and 2%, respectively.13 Referral for CT will usually be made via a secondary care specialist, although some primary care practitioners may have direct access.
Figure 1 shows a suggested diagnostic algorithm by the authors of this article for patients suspected of having bronchiectasis in primary care.

Proposed algorithm for the diagnostic pathway in primary care of patients suspected of having bronchiectasis
Assessment and routine
It is recommended that the initial assessment after diagnosis of bronchiectasis is carried out by a specialist respiratory team, where investigations can take place to elucidate any underlying cause and to formulate a treatment plan, which can be shared with the patient, primary care team and community team where appropriate. Single-centre studies suggest that investigations into the underlying cause of bronchiectasis can change management in 5–37% patients.14
The underlying causes can include conditions such as allergic bronchopulmonary aspergillosis, immune deficiency, cystic fibrosis (in relevant patients) and non-tubeculous mycobacterial (NTM) disease.14,15 Co-morbid conditions should be assessed, including asthma, COPD, gastro-oesophageal reflux disease (GORD), rheumatoid arthritis and inflammatory bowel disease, and treated accordingly.
The treatment plan should give details of treatment in the stable condition, advice on treatment in the event of an acute exacerbation and arrangements for follow-up (primary care, hospital care and shared care). See Fig. 2 for a suggested checklist as part of the algorithm for review and management of patients wth bronchiectasis in primary care.

Proposed algorithm for the review and management of patients with bronchiectasis in primary care
Routine review
Patients at higher risk of future exacerbations should be reviewed in specialist care, where they present with or develop one or more of the following clinical situations:1
-
They experience three or more exacerbations in 1 year.
-
They have chronic Pseudomonas aeruginosa, non-tuberculous mycobacteria (NTM) or methicillin-resistant Staphylococcus aureus (MRSA) colonisation.
-
There is deteriorating bronchiectasis with declining lung function.
-
They have associated rheumatoid arthritis, immune deficiency, inflammatory bowel disease or primary ciliary dyskinesia.
-
They have allergic bronchopulmonary aspergillosis.
-
Patients with advanced disease and those considering lung transplantation.
Lower-risk patients can be routinely reviewed in primary care. The exact frequency of review should be determined in the initial treatment plan, in consultation with the respiratory specialist and also by changing clinical conditions, but should be at a minimum frequency of once a year.
Factors to be routinely monitored by the primary care team (see Fig. 2) include:
-
Assessment of symptoms (cough, sputum production and breathlessness) and their impact on daily activities.
-
Chronic cough that can have a significant effect on daily activities, including sexual relations and urinary incontinence in women.16
-
Exacerbation frequency.
-
Body mass index (BMI).
-
Pulse oximetry.
-
Spirometry.
-
The sputum should be sent for microbiological analysis when the patient is clinically stable, and should be sent at the start of an exacerbation before antibiotic treatment is started.1
-
Compliance with sputum clearance exercises and shared treatment plan.
Deterioration in lung function, exacerbation frequency or clinical state should prompt specialist referral (see above). If the patient’s BMI is <20 kg/m2, then specialist nutritional advice should be sought. In addition, the patient should be referred to a respiratory physiotherapist to reinforce the sputum clearance exercises if necessary. Similarly, referral for pulmonary rehabilitation should be considered, if the patient has functionally disabling breathlessness (MRC score ≥ 2).
Common co-morbidities, such as mild-to-moderate asthma or COPD, can be treated in the primary care setting, according to national or international guidelines for these conditions.17,18,19,20 It is recommended that chronic rhinosinusitis be treated with nasal saline douching and intranasal steroids. There is a strong association between bronchiectasis and gastro-oesophageal disease (GORD) and patients with GORD have a more severe disease.21 The guideline recommends that symptoms of GORD are specifically sought out and treated, according to the existing NICE guidance, but do not provide evidence that treatment of GORD will improve bronchiectasis outcomes.
Management
The overall aims of management are to prevent further damage (treat the underlying cause if possible), maximise function and quality of life and prevent and treat exacerbations. Figure 3 shows a stepwise approach to management.1

Stepwise management of patients with bronchiectasis. Reproduced from ref. 1, with permission from BMJ Publishing Group Ltd.
Physiotherapy
All patients with bronchiectasis should be assessed by a respiratory physiotherapist. Chest physiotherapy can mobilise secretions and aid effective expectoration,22,23,24 providing improvement in cough scores. Table 3 shows the key elements of physiotherapy intervention.
Influenza and pneumococcal immunisation
It is important to offer annual influenza immunisation to all patients with bronchiectasis.25 In addition, the guidelines recommend that polysaccharide pneumococcal vaccination should be offered to all patients with bronchiectasis (if not previously given), although this recommendation comes from evidence that 23 valent pneumococcal vaccinations can reduce the risk of all-cause pneumonia.26
Inhaled corticosteroids and bronchodilators
Treatment with inhaled corticosteroids (ICS) in bronchiectasis is not recommended, unless the drug is needed for comorbid diseases, such as asthma or COPD, according to treatment guidelines.17,18,19,20 A Cochrane review showed that treatment with ICS demonstrated a minimal reduction in sputum volume, but no effect on exacerbations.27 The studies included in the article used a relatively high dose of ICS (≥ 800 mcg of beclometasone equivalent) and there was a high incidence of local and systemic side effects. It is recommended to offer a trial of long-acting inhaled bronchodilators in patients with significant breathlessness or where there is coexistent asthma and/or COPD.1
No evidence was found for the use of short-acting beta-2 agonists and limited evidence for long-acting beta-2 agonists (LABA) and long-acting anti-muscarinic agents (LAMA).28 Use of LABA and LAMA is recommended in patients with significant breathlessness and coexistent obstructive airway disease of whatever aetiology.
Long-term antibiotic therapy
Long-term—3 months or more—antibiotic therapy should be considered for patients with three or more exacerbations per year, which should be initiated and monitored by specialist teams in secondary care. Treatment with oral azithromycin, 250 mg, three times weekly for a year can reduce the incidence of exacerbations in patients with bronchiectasis,29 and this is recommended as a pragmatic starting dose in the guidelines.1 In patients with concurrent P. aeruginosa infection, the recommended first-line therapy is inhaled colistin. Sputum samples from a secondary care population show that H. influenzae and P. aeruginosa are the most common bacterial isolates with other pathogens, such as M. catarrhalis, S. pneumoniae and non-tuberculous mycobacteria also being found.30 The presence of P. aeruginosa not only guides the choice of antibiotic therapy, but also signifies a worse prognosis with a threefold risk in mortality, higher risk of hospital admission and poorer quality of life.31
Management of the acute exacerbation
Where an acute exacerbation incident is suspected, the first step should be to assess the vital signs (pulse oximetry, pulse rate, respiratory rate, temperature and blood pressure). In the primary care setting, the patient should be treated for acute co-morbidities, such as asthma and COPD, according to disease-specific guidelines.17,18,19,20,32 The patient should be considered for admission to a secondary care setting, where there are features of sepsis or respiratory distress, where there are significant co-morbidities and/or psychosocial factors or there is a need for intravenous antibiotics, where a community service to provide these is not available.
Acute antibiotic therapy
Where possible, the sputum should be obtained for culture and sensitivity testing prior to commencing antibiotics. However, empirical antibiotics can be started whilst awaiting the sputum results. Table 4 shows common organisms associated with acute exacerbations of bronchiectasis and their treatment in primary care. In general, antibiotic courses for 14 days are standard and should always be used in patients infected with P. aeruginosa. Shorter courses may suffice in patients with mild bronchiectasis (usually 7–10 days). It is recommended to consider providing a home sputum pot and standby antibiotics for future exacerbations.
Conclusions
A diagnosis of bronchiectasis should be suspected when a patient presents with a persistent or recurrent productive cough. Definitive diagnosis is made by thin-section CT scan of the chest. Assessment of bronchiectasis should be carried out in secondary/tertiary care, where a shared management plan should be formulated with the patient and the community/primary care team.
Many patients can be routinely managed in primary care, where the cornerstone of management is physiotherapy to improve sputum clearance and maximise exercise capacity and prompt treatment of exacerbations with antibiotics.
The British Thoracic Society Bronchiectasis Guidelines provide advice for diagnosis and management of primary care in the United Kingdom. Although some of the advice, such as the type of antibiotics to be used, is specific to the United Kingdom, many of the recommendations are in line with those of the European Respiratory Society Guidelines 2017,34 and provide a sound basis for primary care management of this increasingly prevalent disease throughout the world.
Data availability
This article draws on the BTS Guideline for Bronchiectasis in Adults—evidence tables supporting the guideline are available on the BTS website: https://www.brit-thoracic.org.uk/quality-improvement/guidelines/bronchiectasis-in-adults/.
References
Hill, A. T. et al. British Thoracic Guideline for bronchiectasis in adults. Thorax. 74(Suppl 1), 1–69 (2019).
Quint, J. K. et al. Changes in the incidence, prevalence and mortality of bronchiectasis in the UK from 2004 to 2013: a population‐based cohort study. Eur. Respir. J. 47, 186–193 (2016).
Weycker, D. et al. Prevalence and incidence of noncystic fibrosis bronchiectasis among US adults. 2013 Chronic Respir. Dis. 14, 377–384 (2013).
Pasteur, M. C. et al. British Thoracic Society Guidelines for non-cystic fibrosis bronchiectasis. Thorax. 65(Suppl 1), i1–i58 (2010).
British Thoracic Society Standards of Care Committee Guideline Production Manual 2016. www.brit-thoracic.org.uk (2016).
Scottish Intercollegiate Guidelines Network (SIGN). SIGN 50: a Guideline Developer’s Handbook. (SIGN: Edinburgh, 2003).
Ni, Y. et al. Clinical characteristics of patients with chronic obstructive pulmonary disease and bronchiectasis: a systematic review and meta-analysis. Int J. Chron. Pulmon Dis. 10, 1465–1475 (2015).
O’Brien, C. et al. Physiological and radiological characterisation of patients diagnosed with chronic obstructive pulmonary disease in primary care. Thorax. 55, 635–642 (2000).
Gupta, S. et al. Qualitative analysis of high‐resolution CT scans in severe asthma. Chest 136, 1521–1528 (2009).
Allain, J. et al. Prevalence of symptomatic bronchiectasis in patients with rheumatoid arthritis. Rev. Rheum. Eng. Ed. 64, 531–537 (1997).
Black, H., Mendoza, M. & Murin, S. Thoracic manifestations of inflammatory Bowel disease. Chest 131, 524–532 (2007).
Shoemark, A., Ozerovitch, L. & Wilson, R. Aetiology in adult patients with bronchiectasis. Respir. Med. 101, 1163–1170 (2007).
Young, K. A. & Kolbenstvedt, A. High resolution CT and bronchography in the assessment of bronchiectasis. Acta Radiol. 32, 439–441 (1991).
Pasteur, M. C. et al. An investigation into causative factors in patients with bronchiectasis. Am. J. Respir. Crit. Care Med. 162(4 Pt 1), 1277–1284 (2000).
Lonni, S. et al. Etiology of non-cystic fibrosis bronchiectasis in adults and it’s correlation to disease severity. Ann. Am. Thorac. Soc. 2, 1764–1770 (2015).
Rees, J. T. et al. Managing urinary incontinence in adults with bronchiectasis. Br. J. Nurs. 22, S15–S16 (2013). S18.
BTS/SIGN Guideline for the management of asthma. www.brit-thoracic.org.uk/standards-of-care/guidelines/btssign-british-guideline-on-the-management-of-asthma (2016).
National Institute of Health and Care Excellence (NICE) Guideline NG115 December 2018: Chronic Obstructive Pulmonary disease in over 16’s. Diagnosis and management. www.nice.org.uk/guidance/ng115 (2018).
Global Initiative for Chronic Lung Disease (GOLD) Global Strategy for Diagnosis, Management and Prevention of Chronic Obstructive Obstructive Disease. www.goldcopd.org (2019).
Global Initiative for Asthma (GINA). Global strategy for asthma management and prevention. www.ginasthma.org (2018).
Mandal, P. et al. Symptoms of airway reflux predict exacerbations an quality of life in bronchiectais. Respir. Med. 107, 1008–1013 (2013).
Murray, M. P. et al. A randomised crossover trial of chest physiotherapy in non‐cystic fibrosis bronchiectasis. Eur. Respir. J. 34, 1086–1092 (2009).
O’Neill, B. et al. current physiotherapy management of patients with bronchiectasis: a UK survey. Int J. Clin. Pract. 56, 34–35 (2002).
Lee, A. L. et al. The short and long term effects of exercise training in non‐cystic fibrosis bronchiectasis; a randomized controlled trial. Respir. Res. 15, 44 (2014).
Poole, P. J. et al. Influenza vaccine for patients with chronic obstructive pulmonary disease. Cochrane Database Syst. Rev. 2006, CD002733 (2006).
Moberley, S. et al. Vaccines for preventing pneumococcal infection in adults. Cochrane Database Syst. Rev. 213, CD000422 (2013).
Kapur, N. et al. Inhaled steroids for bronchiectasis. Cochrane Database Syst. Rev. 86, CD000996 (2009).
Nogrady, S. et al. Reversibility of airways obstruction in bronchiectasis. Thorax. 33, 635–637 (1978).
Altenburg, J. et al. Effect of azithromycin maintenance treatment on infectious exacerbations among patients with non‐cystic fibrosis bronchiectasis: the BAT randomized controlled trial. JAMA 309, 1251–1259 (2013).
Kelly, M. G., Murphy, S. & Elborn, J. S. Bronchiectasis in secondary care: a comprehensive profile of a neglected disease. Eur. J. Intern Med. 2003 14, 488–492 (2003).
Goeminne, P. C. et al. Mortality in non‐cystic fibrosis bronchiectasis: a prospective cohort analysis. Respir. Med. 108, 287–296 (2014).
British Thoracic Society Guidelines for management of community acquired pneumonia. www.brit-thoracic.org.uk/document-library/clinical-information/pneumonia/adult-pneumonia/a-quick-reference-guide-bts-guidelines-for-the-management-of-community-acquired-pneumonia-in-adults (2009).
Ellis, D. A. et al. Present outlook in bronchiectasis: clinical and social study and review of factors influencing prognosis. Thorax. 36, 659–664 (1981).
Polverino, E. et al. European Respiratory Society guidelines for the management of adult bronchiectasis. Eur. Respir. J. 50, 1700629 (2017).
Acknowledgements
The support of the British Thoracic Society and the Primary Care Respiratory Society in the development of this article is acknowledged. The BTS Guideline for Bronchiectasis in Adults was funded by the British Thoracic Society—no external funding.
Author information
Authors and Affiliations
Contributions
K.G.J. was the lead author and member of the Guideline group and led the drafting and revision of the paper. A.T.H., A.L.S. and M.R.L. chaired the guideline group. All authors undertook revisions of the paper. K.G.J. and A.T.H. had final responsibility for the paper, which was approved by all authors.
Corresponding author
Ethics declarations
Competing interests
K.G.J. has declared funding from Boehringer Ingelheim, GlaxoSmithkline, Astra Zeneca, Napp, TEVA, Chiesi, Nutricia and Novartis. M.R.L. has declared funding from Astra Zeneca, Bayer Healthcare, Insmed, Pulmocide, Griffols, Polyphor and Savara. V.K. has declared funding for educational sessions from Astra Zeneca, Napp, Chiesi, Pfizer, Boehringer Ingelheim, TEVA and GSK. A.T.H., D.K., A.L.S., K.P., A.H., L.G., X.R., A.W. and S.A.W. declare no competing interests.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Gruffydd-Jones, K., Keeley, D., Knowles, V. et al. Primary care implications of the British Thoracic Society Guidelines for bronchiectasis in adults 2019. npj Prim. Care Respir. Med. 29, 24 (2019). https://doi.org/10.1038/s41533-019-0136-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41533-019-0136-8
This article is cited by
-
Practical tips in bronchiectasis for Primary Care
npj Primary Care Respiratory Medicine (2022)
-
The self-management abilities test (SMAT): a tool to identify the self-management abilities of adults with bronchiectasis
npj Primary Care Respiratory Medicine (2022)
