
Abstract
Computers are increasingly used to improve prescribing decisions in the management of long-term conditions however the effects on asthma prescribing remain unclear. We aimed to synthesise the evidence for the use of computerised alerts that identify excessive prescribing of short-acting beta2-agonists (SABAs) to improve asthma management for people with asthma. MEDLINE, CINAHL, Embase, Cochrane and Scopus databases (1990–2016) were searched for randomised controlled trials using electronic alerts to identify excessive prescribing of SABAs for people with asthma in primary care. Inclusion eligibility, quality appraisal (Cochrane risk of bias tool) and data extraction were performed by two independent reviewers. Findings were synthesised narratively. A total of 2035 articles were screened and four trials were eligible. Three studies had low risk of bias: one reported a positive effect on our primary outcome of interest, excessive SABA prescribing; another reported positive effects on the ratio of inhaled corticosteroid (ICS)-SABA prescribing, and asthma control; a third reported no effect on outcomes of interest. One study at high risk of bias reported a reduction in exacerbations and primary care consultations. There is some evidence that electronic alerts reduce excessive prescribing of SABAs, when delivered as part of a multicomponent intervention in an integrated health care system. However due to the variation in health care systems, intervention design and outcomes measured, further research is required to establish optimal design of alerting and intervening systems.
Similar content being viewed by others

Introduction
Asthma affects an estimated 300 million individuals worldwide and almost 30 million people below 45 years of age in Europe.1 With a prevalence of 6% in 2016–20172 and an estimated 5.4 million people receiving treatment,3 asthma is the most common long-term condition in the United Kingdom (UK).4 In 2015-2016 there were approximately 1.4 million hospital admissions for asthma in England and Wales5 and whilst the number of asthma deaths has fallen by five percent from 2015 to 2016, this remains higher than the 15-year average.6
The National Review of Asthma Deaths (NRAD) identified that, of 195 deaths from asthma between 2012 and 2013, 39% of those who died were prescribed more than 12 short-acting beta2-agonist inhalers (SABAs) in the previous year, with 4% prescribed more than 50 SABAs in the same time period.7
Frequent use of SABAs is an internationally recognised marker of poor control8 and a potentially modifiable warning sign of impending serious asthma attacks9,10,11,12 and asthma death.13,14,15,16,17 Asthma control is defined as the extent to which the manifestations of asthma, commonly wheeze, shortness of breath, chest tightness, cough and variable expiratory airflow limitation, can be observed in the patient, or have been reduced or removed by treatment.18,19 Control can be assessed by current symptoms and future risk of adverse outcomes;8 patients with good asthma control have less need for SABAs and require no emergency visits.20 Following the National Review of Asthma Deaths, the electronic surveillance of prescription refill frequency was recommended to alert clinicians to people with asthma prescribed excessive quantities of SABAs.7
General practice computer systems increasingly use reminders and alerts for preventative care and disease management21,22 including asthma.23,24 Computer decision support systems (CDSSs), defined as ‘active knowledge systems which use two or more items of patient data to generate case-specific advice,’25 have the potential to influence prescribing behaviour. Efforts to automate reminder systems and improve efficiency in both prevention and chronic disease management have yielded some improvements when assessed using randomised trials.26 However, evaluations suggest CDSSs do not consistently improve prescribing behaviour and clinical outcomes27 and the role of electronic alerts to identify and reduce excessive SABA prescribing remains unclear. This review aims to provide a systematic overview of the extent to which electronic alerts in primary care computer systems can identify excessive prescribing of SABAs, and assess the impact of these interventions on SABA prescribing, asthma management and asthma control.
Results
Study selection
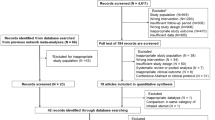
Fig. 1 details the systematic search and eligibility assessment. From 2035 titles, four studies were selected as eligible.28,29,30,31 No ongoing or unpublished trials were identified. Risk of bias is reported in Table 1.

PRISMA flow chart
Study characteristics
RCTs were conducted between 2001 and 2015; two recent studies (published in 2014 and 2015) were carried out within integrated healthcare systems in the United States30 and Canada31 respectively, whilst two older studies were from the United Kingdom (published in 2001 and 2002).28,29 The features of interventions are summarised in Table 2. A detailed description of the interventions can be found in Supplementary Appendix 1. Methods of alerting included computerised prompts,28,29 an electronic message to physicians30 and a dashboard alert.31 Three of the four studies included people with asthma under-18 years of age, of which the lower age range for inclusion was 5 years of age,31 12 years of age30 and one not reported.28 No studies stratified findings by age range. The characteristics of studies are presented in Table 3.
Primary outcome
A brief summary of findings is presented in Table 4. A detailed description of findings can be found in Table 5.
Study-defined excessive SABA prescribing
Zeiger et al.30 reported a reduction in the number of patients being dispensed excessive SABAs (p = 0.007) and an increase in length of time between SABA prescriptions (p = < 0.001). These effects were noted in the subgroup of patients without prior asthma specialist care who received the intervention (p = < 0.001). Tamblyn et al.31 reported excessive SABA (expressed as fast-acting b-agonist) dispensing as a composite primary outcome – the rate of out-of-control asthma episodes–which included emergency department (ED) attendances and hospitalisations. It was therefore not possible to determine the effect of the intervention on SABAs alone.
Secondary outcomes
SABA prescribing
Zeiger et al.30 reported a reduction in the number of SABAs dispensed at 3 months (p = < 0.001), 6 months (p = < 0.001) and 12 months (p = < 0.001) in the subgroup of patients without prior specialist asthma care. Eccles et al.29 reported no significant effect of a computerised decision support system on SABA prescription in the 12 months before and after the intervention (odds ratio (OR) 1.04, 95% CI 0.83–1.31).
ICS prescribing
Zeiger et al.30 reported no difference in the number of patients dispensed ICS (not as a combination inhaler), whilst Eccles et al.29 reported no difference in the number of patients prescribed ICS before and after the intervention. McCowan et al.28 reported no between-group difference in maintenance prescribing patterns and no difference in the proportion of patients classified by management step.
Ratio of ICS-SABA prescribed
Tamblyn et al.31 reported an increase in the ratio of ICS-SABAs dispensed (mean difference (MD) 0.27, p = 0.03; 95% CI 0.02–0.51) with higher ratios reported in both subgroups of patients whose asthma was controlled and out of control at the start of the study. Zeiger et al.30 reported a controller (ICS) to total medication ratio of greater or equal to 0.5 at 3, 6 and 12 months, in particular for those without prior asthma specialist care. As the ICS to total medication ratio was calculated by the number of ICS canisters or 30-day supplies of oral controller medications dispensed, divided by the total number of controller units and SABA inhalers, it was not possible to determine the ICS-SABA ratio specifically.
ICS/LABA prescribing
Zeiger et al.30 reported an increase in the number of patients in the subgroup without prior asthma specialist care dispensed an ICS-LABA inhaler at 3 months (p = 0.004), 6 months (p = < 0.001) and 12 months (p = 0.03).
Asthma reviews
McCowan et al.28 reported no reduction in the number of patients attending practice-initiated asthma reviews.
Study-defined asthma exacerbations
McCowan et al.28 observed a reduction in asthma exacerbations, with 8% of patients who received the intervention reporting an acute asthma exacerbation compared to 17% in the control group (OR 0.42; 95% CI 0.21-0.85). However, there was no difference in the use of oral steroids to manage these attacks in the intervention and control group. Zeiger et al.30 reported no difference in the numbers of patients prescribed oral steroids for an exacerbation irrespective of prior asthma specialist care status. Neither McCowan et al.28 nor Zeiger et al.30 explicitly defined an asthma exacerbation. Eccles et al.29 reported no difference in the numbers of patients prescribed oral steroids before and after the intervention but did not specifically report asthma exacerbations.
Unscheduled consultations for asthma
Eccles et al.29 found no between-group reduction in the number of primary care asthma consultations, whilst McCowan et al.28 reported that patients who received the intervention initiated fewer primary care consultations (OR 0.59; 95% CI 0.37–0.95). However neither study clarified whether consultations were scheduled or unscheduled. Both McCowan et al.28 and Zeiger et al.30 reported no effect of the intervention on ED attendances or hospitalisations for asthma. Tamblyn et al.31 reported ED visits and hospitalisations for asthma as a composite outcome defined as ‘rate of out-of-control asthma episodes,’ therefore secondary care consultations for asthma could not be specifically determined.
Asthma control
Tamblyn et al.31 reported a reduction in the rate of out-of-control asthma events, defined as a composite outcome of excessive SABA use, ED attendance and hospitalisations for asthma, in the sub-group of patients whose asthma was out-of-control at the beginning of the study (MD −28.4, p = 0.04; 95% CI −55.6, −1.2). When stratified by intervention component, the rate of out-of-control asthma events further reduced when patients were treated with CDSS alone (rate difference (RD) −36.9/100 per year, p = 0.01) in comparison to those threated with both CDSS and the asthma home care monitoring programme (RD -28.4, p = 0.04; 95% CI −55.6,−1.2).
Discussion
Main findings
Given the few studies identified, the evidence to support the use of alerts to reduce excessive SABA prescribing in primary care is limited but promising. This review found that electronic alerts, when delivered as a multicomponent intervention in an integrated health care system, have the potential to successfully identify and reduce excessive SABA prescribing. The greatest effect on our outcomes of interest occurred when an alert, delivered in an integrated health care system, flagged excessive SABA prescribing to clinicians and prompted/facilitated intervening actions including referral to an allergy specialist and a patient information letter.30 None of the studies included used a SABA alert as a sole intervention.
Interpretations in relation to published literature
Our findings support previous research on the use of computer decision support for long-term conditions including asthma, chronic obstructive pulmonary disease, diabetes and osteoporosis which found that interventions consisting of multiple components are associated with greater improvement in outcomes than single-target interventions with fewer components.24,32,33
There is however no consensus definition on excessive SABA use in the literature. Definitions of excessive SABA use vary from three or more SABAs per quarter34 to 12 or more SABAs a year.7 Of the two included studies in which excessive SABA use was reported, definitions varied from greater or equal to seven canisters per year (at least four puffs per day per year)30 to greater than 250 doses of SABA in the past 3 months.31
The identification and reduction of excessive SABA use in Zeiger et al.30 study was facilitated by alerts that were not restricted to point-of-care presentation. Such methods of alerting may offer a solution to the dilemma that automatic provision of decision support at point of decision making neither guarantees clinician uptake or engagement27 nor predicts improvements in process of care or patient outcomes.35 The two studies that showed greatest effects on our outcomes of interest were those carried out recently (in the past three years), in which decision support was integrated with electronic health record (EHRs).30,31 Although research has indicated that advice presented within EHRs is less likely to improve care or outcomes than stand-alone programmes,35 our findings support the evidence that computer decision support integrated with clinician workflow is associated with improved outcomes.22,32 Zeiger et al’s finding of a reduction of excessive SABA use supports the evidence that electronic health records and electronic messaging in an integrated health care system increases clinician adherence to evidence-based guidelines.36
In one study, users failed to engage with decision support29 whilst in another, clinicians failed to interact with the CDSS in approximately 60% of cases.31 However it is not clear whether levels of engagement were consistent between clinicians and whether clinician interaction declined over time. There may be valid reasons to account for the variability in decision support engagement which include technical design of the CDSS, the setting in which the system is deployed and the characteristics of users and the patients treated.27 The higher user engagement in Tamblyn et al.31 is likely due to the increased ease of use associated with more recent, sophisticated decision support integrated within a comprehensive EHR system that accesses pharmacy, as well as primary and secondary care data. This is in comparison to older interventions, such as that of Eccles et al.29 where the intervention was not integrated with the EHR, and in which pharmacy and secondary care data was not captured.
Alerts integrated within EHRs may interrupt clinician workflow and result in “alert fatigue” with up to 96% of alerts over ridden or ignored in one study.37 Following user feedback, Eccles et al.29 altered decision support to trigger when a clinician entered a relevant morbidity code rather than being automatically activated upon entering a patient’s medical record. Whilst this may have been an attempt to minimise alert fatigue it did not improve CDSS user interaction. It is likely that very low CDSS interactions reflected clinical guidelines being located in a separate system not supported within clinician workflow.
Qualitative research used in conjunction with RCTs has the potential to beneficially influence intervention design and delivery38 however none of the included studies reported using qualitative methods to complement intervention design. Such methods may optimise alert design, improve clinician interaction with decision support and aid the interpretation of results.
Strength and limitations
As interventions to improve prescribing volumes/rates do not necessarily result in more ‘appropriate’ prescribing or improved patient outcomes27 both process and clinical outcomes were assessed in this review. However few studies met our inclusion criteria, with only one study reporting our primary outcome of interest. Due to the limited number of published reports of randomised controlled trials in our analyses, there may be possibility of publication bias or selective reporting. Interventions in the two older studies28,29 were poorly described which may have limited our interpretation of the findings. We were unable to conduct a meta-analysis due to heterogeneity in intervention design and outcomes evaluated. Due to a lack of reporting no conclusions could be made on health economics.
Implications for clinical care and future research
There is an increased focus on the digitalisation of the NHS in an attempt to improve safety and quality of care.39 Recommendations have called for the national use of electronic alerts to identify excessive prescribing of SABAs in the UK.7,40 Due to the few studies identified in this review, the role of alerts to reduce excessive SABA prescribing in the UK’s publically funded national health service (NHS) remains unclear. Integrated care can take many forms involving collaboration between policy providers and commissioners and between service providers, however benefits arise primarily when clinical teams and services are brought together and incentives are aligned to support service improvement.36 It is likely that a combination of design, technical capabilities and variety of intervention components, when delivered in an integrated health care system, facilitated the improvements to SABA prescribing and asthma management identified in recent studies. In a publicly funded health care system such as the NHS it remains challenging to deliver such improvements. However this review identifies a number of areas where potential exists and where further research is recommended.
In the UK, 78% of bronchodilators are issued on repeat prescription41 yet research fails to address the use of alerts at this point in the prescribing process. Furthermore, two studies from the UK, carried out over a decade ago, did not integrate interventions within EHRs, in contrast to more recent studies from North America. Future research should consider novel ways to deliver SABA alerts as a sole intervention and/or as part of a multicomponent intervention in primary care. Furthermore, the point in the prescribing process at which a SABA alert will have greatest impact should be explored. Interventions should be trialled both in and outside of the consultation to target clinicians and people with asthma.
Standardised methods for the design and reporting of CDSS interventions are recommended to enable a thorough evaluation of process and clinical outcomes. We support previous recommendations that studies use a taxonomy or framework such as Kawamoto et al.21 and Berlin et al.42 to theoretically underpin the design and reporting of interventions.25,43 An explicitly defined outcome set that includes more standardised endpoints, e.g., excessive SABA prescribing and asthma exacerbations, may help the translation of research findings into clinical practice. We recommend that future studies report on both the implementation process and health economics outcomes associated with CDSS-based alerts. Third party external validation of CDSSs is recommended.35 Systems evaluation involving academic-commercial collaborations and user testing should be explored to aid the translational research process. End-users should be involved in the design of alerts to optimise interventions and trial design. Future studies should consider mixed methods designs that incorporate qualitative methods before, during and/or after an RCT. Such methods may help determine the barriers and facilitators to alert usage in practice, as well as assisting in the development of alerts that are transferable to the real-world clinical setting.
Conclusion
There is some evidence that electronic alerts integrated with EHRs and delivered as part of a multicomponent intervention reduce excessive SABA prescribing. Due to variations in health care systems, intervention designs and outcomes measured, further research is required to determine the effects of alerts on excessive SABA prescribing in a publically funded health system. Future research should determine the point at which novel alerts will most effectively reduce excessive SABA prescribing and be accepted by users.
Materials and methods
The study design was a systematic review, performed following PRISMA-guidelines.44 Methods of analysis and inclusion criteria were specified in advance and documented in a protocol45 and registered on PROSPERO (International Prospective Register of Systematic Reviews; www.crd.york.ac.uk/PROSPERO/) with identifier CRD 42016035633.
Selection criteria
Studies were considered for inclusion in this systematic review according to the following criteria.
Participants
Studies that delivered care to adults and/or children with asthma, in a primary care setting. Primary care was defined as healthcare delivered in a community setting, most commonly in general practice, by a clinician, nurse or pharmacist. Non-clinical staff for example administrators and/or receptionists were also included.
Intervention
CDSSs were included if they incorporated an alert initiated by the excessive prescribing or dispensing of SABAs for asthma. Alerts used in secondary or tertiary care, for other respiratory conditions that were not asthma were excluded.
Comparison
The comparator was ‘usual care.’
Outcomes
Our primary outcome of interest was excessive SABA prescribing. Excessive prescribing of SABA was assessed on a study-defined basis. Secondary outcomes of interest included additional measures of prescribing and process of care (future SABA and ICS prescribing, ICS/SABA prescribing ratio, ICS/long-acting beta2-agonist prescribing (LABA), asthma reviews), and clinical outcomes (asthma exacerbations with/without oral steroids, unscheduled primary and secondary care asthma consultations, asthma control).
Study design
Only randomised controlled trials (RCTs), in any language, were included as they are considered the most rigorous way to evaluate intervention effectiveness.46
Search strategy
We searched Medline, Embase, Cinahl, Scopus and Cochrane Library databases from 1990 to 2016 with the search terms listed in Supplementary Appendix 2. We contacted the authors of included studies to clarify intervention design and outcomes measured where necessary. Ongoing and unpublished trials were searched for using the following websites: https://www.isrctn.com/ and https://clinicaltrials.gov/.
Two authors (SM and CG) independently screened titles and abstracts, assessing them against the inclusion criteria. Both authors reviewed the full text of each potentially eligible paper to determine suitability for inclusion. Disagreements were resolved by discussion and, if necessary, arbitration of a third researcher (ADS, AB, MT).
Data extraction and quality appraisal
Using a piloted data extraction form, SM and ADS independently extracted the following data from included trials: country, setting, funding, study design, healthcare professional and patient population, features of the CDSS intervention, description of the control group, outcome measures, results and risk of bias assessment. SM and ADS compared data extraction, and disagreements were arbitrated by a third researcher (CG) if necessary.
We assessed the risk of bias in each trial using the seven-criteria approach described in section eight of the Cochrane Handbook for Systematic Reviews of Interventions.47
Data analysis
Due to heterogeneity in the CDSS interventions used and in outcomes measured, we undertook a narrative synthesis.
Data availability
Authors confirm that all relevant data are included in the paper and/or its supplementary information files.
References
Gibson, J. G., Loddenkemper, R., Lundbäck., B. & Sibille, Y. Respiratory health and disease in Europe: the new European lung white book. Eur. Respir. J. 42, 559–563 (2013).
Health and Social Care Information Centre. Quality and Outcomes Framework-Prevalence, Achievements and Exceptions Report, England 2016–2017. https://www.gov.uk/government/statistics/quality-and-outcomes-framework-achievement-prevalence-and-exceptions-data-2016-to-2017.
Asthma U.K. Asthma facts and statistics. https://www.asthma.org.uk/about/media/facts-and-statistics/.
National Institute for Health and Excellence. Asthma Quality Standard (QS25). https://www.nice.org.uk/guidance/qs25.
NHS Digital. Hospital Admitted Patient Care Activity, 2015-16. https://www.gov.uk/government/statistics/hospital-admitted-patient-care-activity-2015-to-2016.
Asthma U.K. Asthma UK calls for action to end preventable asthma deaths. (2017).
Royal College of Physicians. Why Asthma Still Kills-The National Review of Asthma Deaths (NRAD) Confidential Enquiry report. https://www.rcplondon.ac.uk/projects/national-review-asthma-deaths (2014).
Global Initiative for Asthma. Global Strategy for Asthma Management and Prevention. http://ginasthma.org/2017-gina-report-global-strategy-for-asthma-management-and-prevention/ (2017).
Schatz, M. et al. Asthma quality-of-care markers using administrative data. Chest 128, 1968–1973 (2005).
Paris, J. et al. Relationship between recent short-acting beta-agonist use and subsequent asthma exacerbations. Ann. Allergy Asthma Immunol. 101, 482–487 (2008).
Patel, M. et al. Metrics of salbutamol use as predictors of future adverse outcomes in asthma. Clin. Exp. Allergy 43, 1144–1151 (2013).
British Thoracic Society and Scottish Intercollegiate Guidelines Network. British guideline on the management of asthma: a national clinical guideline. (2016).
Spitzer, W. O. et al. The use of beta-agonists and the risk of death and near death from asthma. N. Engl. J. Med 326, 501–506 (1992).
Suissa, S. et al. A cohort analysis of excess mortality in asthma and the use of inhaled beta-agonists. Am. J. Respir. Crit. Care Med. 149, 604–610 (1994).
Suissa, S., Blais, L. & Ernst, P. Patterns of increasing beta-agonist use and the risk of fatal or near-fatal asthma. Eur. Respir. J. 7, 1602–1609 (1994).
Anderson, H. R. et al. Bronchodilator treatment and deaths from asthma: case-control study. BMJ 330, 117 (2005).
Lanes, S. F., Garcia Rodriguez, L. A. & Huerta, C. Respiratory medications and risk of asthma death. Thorax 57, 683–686 (2002).
Reddel, H. K. et al. An official American Thoracic Society/European Respiratory Society statement: asthma control and exacerbations: standardizing endpoints for clinical asthma trials and clinical practice. Am. J. Respir. Crit. Care Med. 180, 59–99 (2009).
Taylor, D. R. et al. A new perspective on concepts of asthma severity and control. Eur. Respir. J. 32, 545–554 (2008).
Bateman, E. D. et al. Global strategy for asthma management and prevention: GINA executive summary. Eur. Respir. J. 31, 143–178 (2008).
Kawamoto, K., Houlihan, C. A., Balas, E. A. & Lobach, D. F. Improving clinical practice using clinical decision support systems: a systematic review of trials to identify features critical to success. BMJ 330, 765 (2005).
Pearson, S. A. et al. Do computerised clinical decision support systems for prescribing change practice? A systematic review of the literature (1990-2007). BMC Health Serv. Res. 9, 154 (2009).
Fathima, M., Peiris, D., Naik-Panvelkar, P., Saini, B. & Armour, C. L. Effectiveness of computerized clinical decision support systems for asthma and chronic obstructive pulmonary disease in primary care: a systematic review. BMC Pulm. Med. 14, 189 (2014).
Matui, P., Wyatt, J. C., Pinnock, H., Sheikh, A. & McLean, S. Computer decision support systems for asthma: a systematic review. NPJ Prim. Care Respir. Med. 24, 14005 (2014).
Wyatt, J. & Spiegelhalter, D. Field trials of medical decision-aids: potential problems and solutions. Proc. Annu. Symp. Comput. Appl. Med. Care, 3–7 (1991). http://www.ncbi.nlm.nih.gov/pubmed/1807610.
Black, A. D. et al. The impact of eHealth on the quality and safety of health care: a systematic overview. PLoS Med. 8, e1000387 (2011).
Moxey, A. et al. Computerized clinical decision support for prescribing: provision does not guarantee uptake. J. Am. Med. Inform. Assoc. 17, 25–33 (2009).
McCowan, C. et al. Lessons from a randomized controlled trial designed to evaluate computer decision support software to improve the management of asthma. Med. Inform. Internet Med. 26, 191–201 (2001).
Eccles, M. et al. Effect of computerised evidence based guidelines on management of asthma and angina in adults in primary care: Cluster randomised controlled trial. BMJ 325, 941–944 (2002).
Zeiger, R. S. et al. Real-time asthma outreach reduces excessive short-acting β2-agonist use: a randomized study. J. Allergy Clin. Immunol. Pract. 2, 445–456 (2014). e1–e5.
Tamblyn, R. et al. Evaluating the impact of an integrated computer-based decision support with person-centered analytics for the management of asthma in primary care: a randomized controlled trial. J. Am. Med. Inform. Assoc. 22, 773–783 (2015).
Roshanov, P. S. et al. Computerized clinical decision support systems for chronic disease management: a decision-maker-researcher partnership systematic review. Implement Sci. 6, 92 (2011).
Kastner, M. & Straus, S. E. Clinical decision support tools for osteoporosis disease management: a systematic review of randomized controlled trials. J. Gen. Intern Med. 23, 2095–2105 (2008).
Silver, H. S. et al. Quarterly assessment of short-acting β2-adrenergic agonist use as a predictor of subsequent health care use for asthmatic patients in the United States. J. Asthma 47, 660–666 (2010).
Roshanov, P. S. et al. Features of effective computerised clinical decision support systems: meta-regression of 162 randomised trials. BMJ 346, f657 (2013).
Curry, N. & Ham, C. Clinical and service integration: the route to improved outcomes. The King’s Fund. http://www.kingsfund.org.uk/publications/clinical-and-service-integration (2010).
van der Sijs, H., Aarts, J., Vulto, A. & Berg, M. Overriding of drug safety alerts in computerized physician order entry. J. Am. Med Inform. Assoc. 13, 138–147 (2006).
Cathain, A., Thomas, K. J., Drabble, S. J., Rudolph, A. & Hewison, J. What can qualitative research do for randomised controlled trials? A systematic mapping review. BMJ Open 3, e002889 (2013).
Brailer, J. A.-M. et al. Making IT work-harnessing the power of health information technology to improve care in England. (Department of Health, London, 2016).
Asthma U.K. Connected asthma: how technology will transform care. https://www.asthma.org.uk/connectedasthma (2016).
Petty, D. The repeat prescription report. Pharmacy2U. https://www.pharmacy2u.co.uk/prescription-report.html (2017).
Berlin, A., Sorani, M. & Sim, I. A taxonomic description of computer-based clinical decision support systems. J. Biomed. Inform. 39, 656–667 (2006).
Car, J. et al. The Impact of eHealth on the Quality and Safety of Healthcare. A Report for the NHS Connecting for Health Evaluation Programme: Extended executive summary (2008).
Moher, D. et al. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. 6, e1000097 (2009).
McKibben, S., Bush, A., Thomas, M. & Griffiths, C. The use of electronic alerts in primary care computer systems to identify the over-prescription of short-acting beta2-agonists in people with asthma: a protocol for a systematic review. NPJ Prim. Care Respir. Med. 27, 30 (2017).
Craig, P. et al. Developing and evaluating complex interventions: the new medical research council guidance. BMJ 337, a1655 (2008).
Higgins J. P. T. & Green S. (eds) Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration. http://www.cochrane-handbook.org (2011).
Acknowledgements
The authors wish to thank Asthma UK and Queen Mary University London for funding this work as part of a PhD studentship carried out by S.M. A.D.S. is funded by a NIHR Academic Clinical Lectureship. A.B. is a National Institute for Health Research (NIHR) Senior Investigator and additionally was supported by the NIHR Respiratory Disease Biomedical Research Unit at the Royal Brompton and Harefield NHS Foundation Trust and Imperial College London. M.T. is supported by the NIHR Collaboration for Leadership in Applied Health Research and Care (CLAHRC) Wessex, NIHR School of Primary Care Research and NIHR Southampton Biomedical Research Centre. C.G. is supported by the NIHR CLAHRC North Thames at Bart’s Health NHS Trust. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health. This work is funded by Asthma UK and Queen Mary University of London.
Author information
Authors and Affiliations
Contributions
This work forms part of an Asthma UK Centre for Applied Centre PhD Studentship being undertaken by S.M. C.G. had the original idea for the study. S.M., A.B., M.T. and C.G. contributed to the plan and/or design of the study. S.M. and C.G. completed study screening. S.M. and A.D.S. performed data extraction. S.M. drafted the manuscript and A.D.S., A.B., M.T. and C.G. commented on each draft version. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
C.G. is an assistant editor of npj Primary Care Respiratory Medicine and M.T. is an associate editor of npj Primary Care Respiratory Medicine but were involved in neither the editorial review of, nor any decision to publish or not publish this article.
Additional information
Publisher's note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
McKibben, S., De Simoni, A., Bush, A. et al. The use of electronic alerts in primary care computer systems to identify the excessive prescription of short-acting beta2-agonists for people with asthma: a systematic review. npj Prim Care Resp Med 28, 14 (2018). https://doi.org/10.1038/s41533-018-0080-z
Received:
Revised:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41533-018-0080-z
This article is cited by
-
“Tossing a coin:” defining the excessive use of short-acting beta2-agonists in asthma—the views of general practitioners and asthma experts in primary and secondary care
npj Primary Care Respiratory Medicine (2018)
