
Abstract
The bilateral effects of deep brain stimulation (DBS) on motor and non-motor symptoms of Parkinson’s disease (PD) have been extensively studied and reviewed. However, the unilateral effects—in particular, the potential lateralized effects of left- versus right-sided DBS—have not been adequately recognized or studied. Here we summarized the current evidence and controversies in the literature regarding the lateralized effects of DBS on motor and non-motor outcomes in PD patients. Publications in English language before February 2021 were obtained from the PubMed database and included if they directly compared the effects of unilateral versus contralateral side DBS on motor or non-motor outcomes in PD. The current literature is overall of low-quality and is biased by various confounders. Researchers have investigated mainly PD patients receiving subthalamic nucleus (STN) DBS while the potential lateralized effects of globus pallidus interna (GPi) DBS have not been adequately studied. Evidence suggests potential lateralized effects of STN DBS on axial motor symptoms and deleterious effects of left-sided DBS on language-related functions, in particular, the verbal fluency, in PD. The lateralized DBS effects on appendicular motor symptoms as well as other neurocognitive and neuropsychiatric domains remain inconclusive. Future studies should control for varying methodological approaches as well as clinical and DBS management heterogeneities, including symptom laterality, stimulation parameters, location of active contacts, and lead trajectories. This would contribute to improved treatment strategies such as personalized target selection, surgical planning, and postoperative management that ultimately benefit patients.
Similar content being viewed by others

Introduction
Cerebral lateralization refers to the functional specialization of the two cerebral hemispheres1. For instance, the left cerebral cortex is dominant for motor control and verbal processing, whereas the right cerebral cortex is dominant for spatial cognition, body schema, proprioceptive control, and inhibition control2. The basal ganglia—a group of subcortical nuclei—is critical for information integration and processing of the cortex input for motor and cognitive functions3. Thus, it is postulated that the functions of basal ganglia are hemisphere-specific as well. Indeed, both neurobiological4,5 and structural6 basis as well as the electrophysiological pattern asymmetry7 suggest the functional laterality of basal ganglia. Therefore, interventions to left versus right basal ganglia may demonstrate distinctive effects on motor and cognitive features.
Parkinson’s disease (PD) is the second most common neurodegenerative disorder characterized by a selective and progressive loss of dopaminergic neurons in the substantia nigra, resulting in a dopamine deficiency in the basal ganglia8. Deep brain stimulation (DBS) is a well-established neurosurgical treatment for controlling motor symptoms and reducing levodopa-induced complications in advanced PD9,10. Currently, two main structures of the basal ganglia, the subthalamic nucleus (STN) and the globus pallidus interna (GPi), are primarily targeted in DBS surgery11. Bilateral and symmetric placement of DBS is the strategy adopted in the majority of cases as patients with advanced PD often show bilateral disabling motor symptoms12. Thus, bilateral effects of DBS on motor and non-motor symptoms have been extensively investigated11,13. In contrast, the unilateral effects—in particular, the potential lateralized effects of left- versus right-sided DBS, given the postulated functional lateralization of basal ganglia—have not been adequately recognized or studied. Moreover, to the best of our knowledge, no systematic review has been composed regarding this issue. In this review, therefore, we focus on the evidence and controversies regarding the potential lateralized effects of DBS on motor and non-motor symptoms in PD. We also highlight limitations of the current literature and potential factors that may influence the interpretation of the evidence.
Results
Motor features
Whether the unilateral left- and right-sided DBS have different effects on motor symptoms in patients with PD remains debated. Though the lateralization effect is not observed in all patients14,15,16, several studies have suggested that there exists a superiority of unilateral STN DBS in improving motor functions17,18. Schulz et al. enrolled 12 right-handed PD patients with stable bilateral STN DBS and reported that, in the off-medication condition, unilateral left-sided and bilateral STN stimulation resulted in better improvement in non-lateralized motor endpoints and overall motor scores than unilateral right-sided stimulation17. However, by studying 45 PD patients treated with bilateral STN DBS, Tabbal et al. found no differences between unilateral left- and right-sided STN stimulations in the improvement of gait speed in the off-medication state14. The differences between unilateral left- and right-sided stimulations on the improvement of rigidity and bradykinesia were not reported in this study, because authors focused mainly on discrepancies in the effects of ipsilateral and contralateral stimulation on these appendicular motor features14. Similarly, a comparable amelioration of the motor score and the working memory performance (see “neurocognition and speech” section) was described by Hershey et al. between unilateral left- and right-sided STN stimulation conditions in 49 PD patients with bilateral STN DBS in the off-medication state15. Instead, they suggested a potential causal role of the disease asymmetry to explain the different effects of unilateral STN DBS between the more and less affected side on motor functions and working memory performance15. Interestingly, although Lizarraga et al. reported no differences in motor and gait scores in the off-medication state between unilateral left- and right-sided stimulation conditions in 22 PD patients with the presence of the gait dysfunction after receiving bilateral STN DBS, they showed that unilateral right-sided STN stimulation might produce slightly greater improvement in gait kinematics (i.e., stride length) than left-sided stimulation18. They later postulated that the right (non-dominant) hemisphere may be dominant for axial motor control2. Castrioto et al. also reported no significant difference between unilateral left- and right-sided stimulation conditions on motor scores in 22 PD patients with bilateral STN DBS in the off-medication condition. However, they proposed the presence of a ‘dominant-STN’, the stimulation of which may lead to improvements of motor symptoms, similar to bilateral stimulation16. In this study, 11 (50%) participants presented a ‘dominant-STN’, in 8 of whom the dominant-STN was contralateral to the most affected side. Interestingly, the ‘dominant-STN’ phenomenon was associated with longer disease duration and tremor predominance16. A subsequent study further demonstrated that the unilateral stimulation of the ‘dominant-STN’ could offer improvement in gait parameters, which were comparable to those after bilateral stimulation. Whereas in patients without the ‘dominant-STN’, only bilateral stimulation could significantly improve gait parameters (n = 10)19. However, it is currently difficult to preoperatively select patients with underlying ‘dominant-STN’.
As mentioned above, Tabbal et al. reported that unilateral STN DBS reduced rigidity and bradykinesia both ipsilaterally and contralaterally14. However, the difference between unilateral left- and right-sided DBSs on ipsilateral motor effects was not investigated in this work. In fact, few studies in the current literature focused on this issue. Shemisa et al. investigated 73 right-handed PD patients treated with either unilateral GPi (n = 26) or STN (n = 47) DBS, and this study provided limited evidence of a similar ipsilateral motor improvement in the off-medication state after either unilateral left- or right-sided DBS stimulation, regardless of target20. This study, however, should be interpreted in caution as the target selection was not randomized and could be biased by several baseline factors.
Neurocognition and speech
Lateralized deficits in cognitive performance, especially in language-mediated functions, have been recognized in the era of lesional surgeries for PD21,22,23. Compared with patients with right-sided lesions, PD patients who underwent left globus pallidotomy are more likely to experience postoperative declines in verbal fluency21,23. However, in the era of DBS surgeries, the lateralized effects of DBS on cognitive functions of PD have not been as adequately investigated as the effects of bilateral stimulation.
For GPi DBS, Vingerhoets et al. compared the cognitive outcomes at the 3-month follow-up to that at the preoperative baseline in a cohort of PD patients who received unilateral left- (n = 13) or right-sided (n = 7) GPi DBS in the on-medication condition24. Six patients who underwent the unilateral left-sided GPi DBS showed a tendency for cognitive decline (as measured by cognitive impairment index), which was not observed in patients who had received right-sided GPi DBS24. In another study, 6 PD patients were consecutively recruited to investigate the changes in cognitive performance after staged bilateral GPi DBS in the on-medication condition25. Among the 5 patients who received left-sided stimulation first, 4 showed a decline in semantic fluency. In contrast, only 1 of the 5 patients showed a further decline after the second, right-sided surgery25. Rothlind et al. included both staged bilateral GPi (n = 23) and STN (n = 19) DBS cases to evaluate cognitive outcomes in the on-medication condition. Participants were randomized to receive either staged bilateral GPi or STN DBS to avoid the selection bias. Authors reported that the deleterious effect of unilateral DBS on semantic fluency were largely due to the left-sided treatment26. Patients who initially received right-sided DBS displayed a significant decline in semantic fluency only after left-sided surgery26. Moreover, Zahodne et al. compared the cognitive performance of 22 PD patients with unilateral GPi (n = 12) or STN (n = 10) DBS to that of 19 PD controls27. They found that the unilateral DBS surgery was associated with declines in letter and semantic verbal fluency in the on-medication condition and suggested that such changes may be more common after left-sided DBS27. In contrast, Tröster et al. stated that in PD patients who received unilateral pallidal surgery, the decline in on-medication semantic verbal fluency was not associated with the side of surgery28. However, this finding should be interpreted prudently, as both pallidotomy (23 left-sided, 12 right-sided) and DBS (7 left-sided, 3 right-sided) surgeries were combined in the final analysis to increase the statistical power28.
Similarly, whether STN DBS has a potential lateralized effect on cognitive functions for PD remains controversial. In a preliminary study, Lueken et al. systematically evaluated the performance in the Wisconsin Card Sorting Test of 8 right-handed PD patients with bilateral STN DBS in the on-medication condition, and left- and right-sided stimulation was given in a counterbalanced manner. Compared to right-sided stimulation, selected measures of executive functions were more compromised under left-sided stimulation29. However, a subsequent study did not report any association between changes in the working memory capacity (i.e., spatial delayed response, SDR) and the side of STN stimulation in 49 PD patients with bilateral STN DBS in the off-medication condition15. Instead, the authors demonstrated that stimulation on the more affected side of the brain aggravated the SDR, whereas stimulation on the less affected side did not, suggesting that clinical asymmetry might interact with STN DBS to impact behavioral responses15. David et al. used a memory-guided sequential reaching task to examine the role of STN DBS in the intensive as well as integrative and coordinative aspects of motor control in 10 right-handed PD patients treated with bilateral STN DBS in the off-medication condition. They reported that unilateral right-sided STN stimulation significantly increased finger latency and reduced finger velocity (i.e., the intensive aspect) when compared to left-sided stimulation, but the endpoint error (i.e., the integrative and coordinative aspects) was similar between the two stimulation conditions30. One study that investigated cognitive-motor functions in prosaccade and antisaccade tasks in 10 right-handed PD patients with bilateral STN DBS in the off-medication state also found no difference in the spatiotemporal or the cognitive aspects of oculomotor control between unilateral left- and right-sided STN stimulations31.
The lateralized effects of STN DBS on changes in verbal fluency (dominant hemisphere) and visuospatial attention (non-dominant hemisphere) are also a subject of debate17,26,27,32,33,34,35. Concordant with the findings from Rothlind et al. and Zahodne et al. as mentioned above, Schulz et al. also suggested that the declines in syntactic and lexical language performance, speech rate, and laryngeal–articulatory coordination for PD patients with bilateral STN DBS may be principally due to the left-sided stimulation17. Sjöberg et al. compared the verbal fluency of 6 PD patients receiving unilateral left-sided STN DBS to that of 10 PD patients receiving bilateral STN DBS in the on-medication condition. At approximately 1.5-year follow-up, the bilateral STN DBS showed a more deleterious effect on both letter and category verbal fluency. A reasonable explanation is that the group receiving unilateral DBS may represent patients who were at an earlier stage of the disease, which may influence their neurocognitive performance32. More recently, Yilmaz et al. reported no significant discrepancy in verbal fluency or visual orientation between unilateral left- and right-sided stimulations in 29 right-handed PD patients with bilateral STN DBS in the on-medication condition33. In contrast, both Witt et al. (n = 12) and Schmalbach et al. (n = 13) reported a mild but significant shift of visuospatial attention towards the right side and a neglect of left-sided visual stimuli under unilateral stimulation of the left STN, similar to the neglect syndrome after right hemispheric lesions. Such declines in visuospatial attention could be corrected by stimulating the right STN34,35.
The difference in the inhibition control performance between unilateral left- and right-sided STN stimulations has also been investigated36,37,38. Ray et al. reported that the performance in stop-signal task declined after left-sided STN stimulation compared to that after right-sided treatment in 16 right-handed PD patients with bilateral STN DBS in the on-medication condition36. In contrast, Mirabella et al. did not find any difference in the performance in stop-signal task between unilateral left- and right-sided STN stimulations by evaluating 10 right-handed PD patients with bilateral STN DBS in the off-medication condition37. More recently, Mancini et al. recruited 20 right-handed PD patients with unilateral STN DBS (10 left-sided, 10 right-sided) and also reported no main effect of stimulating lateralization on the on-medication performance in countermanding task38. However, the discrepancies in findings between these studies should be carefully interpreted, because the PD cohort selection (i.e., participants with bilateral or unilateral DBS) and the medication status (i.e., off- or on-medication condition) during the task were different across studies, which might limit the interpolation of the results.
Regarding other speech-related functions, Santens et al. reported negative effects of unilateral left-sided STN DBS on prosody and articulation (and hence intelligibility) by separately stimulating the left and right STN in 7 PD patients with bilateral STN DBS in the off-medication state39. Similar results have also been reported by other groups17,40,41. Wang et al. examined the speaking rate and articulatory accuracy of syllable repetitions in 20 right-handed PD patients with unilateral STN DBS (10 left-sided, 10 right-sided) before the surgery and at 3- to 6-month follow-up after withdrawal of anti-parkinsonian medication. They concluded that a decrease in articulatory accuracy and speaking rate was associated with unilateral left-sided STN DBS40. They also reported a significant decline in vocal intensity and vowel duration baseline in 3 right-handed PD patients with unilateral left-sided STN DBS at the 3-month follow-up. Such a decline was not observed in patients with unilateral right-sided STN DBS41.
Neuropsychiatry
To date, few studies have assessed the lateralized effects of DBS on mood in PD patients, and findings were not conclusive. Campbell et al. reported that left-sided STN DBS may produce greater mood improvement than right-sided STN DBS42. They measured the mood response with a computerized version of the Visual Analog Scale in 24 PD patients with bilateral STN DBS. Left-sided stimulation resulted in significantly greater amelioration in valence than right-sided stimulation, and trend-level significance was seen for apathy ratings. No significant differences were observed for anxiety ratings or emotional arousal between unilateral left- and right-sided stimulations42. Birchall et al. reported a similar improvement in depressive symptoms at the 6-month follow-up compared to the preoperative baseline between PD patients with unilateral left-sided (n = 26) STN stimulation and those with unilateral right-sided (n = 24) STN stimulation43. In another study, the authors prospectively assessed the apathy score change preoperatively and postoperatively at the 6-month follow-up in PD patients with either unilateral GPi (11 left-sided, 4 right-sided) or unilateral STN (20 left-sided, 13 right-sided) DBS, and concluded that the incidence of postoperative apathy was not associated with the laterality of GPi or STN DBS44.
Sleep
Interestingly, Amara et al. measured the short-term effect of unilateral STN DBS on sleep quality in 53 PD patients (28 left-sided, 25 right-sided)45. They reported that the improvement in subjective sleep quality at the 6-month follow-up was greater in right-sided stimulation group than in the left-sided group. However, the preoperative baseline sleep quality score was also worse in the right-sided stimulation group. Therefore, it is possible that the reported results were due to more easily detectable improvements in patients with worse baseline sleep dysfunction rather than a direct lateralized stimulating effect of the treatment45. To the best of our knowledge, no other studies have been published to support or oppose this finding.
Potential confounding factors
Study design
To compare the differential effects of unilateral left- versus right-sided DBS in PD patients, several studies20,24,27,28,38,40,43,44,45 have analyzed two separate cohorts with respective unilateral left- and right-sided DBS implantation. One study also compared the group with unilateral left-sided STN DBS with that with bilateral treatment32. Consequently, differences in baseline characteristics between the two groups may limit the interpretation of the results. Other studies14,15,16,17,18,19,25,26,29,30,31,33,34,35,36,37,42 recruited PD patients with simultaneous or staged bilateral DBS and collected the outcome data under unilateral on-stimulation conditions in a randomized or counterbalanced manner. Among these, some studies applied randomized stimulation in consecutive days to ensure a sufficient ‘washout’ interval. However, some required patients to complete tests under different stimulating conditions on the same day with a shorter ‘washout’ period. In addition, the medication conditions (i.e., on- or off-medication) also differed across studies. For example, the majority of the studies that evaluated the potential lateralized stimulating effects on motor outcomes were conducted in the off-medication condition to exclude the interference of drug effects. In contrast, several studies investigating the cognitive outcomes reported their results in the on-medication state to reduce the possibility for motor symptoms to limit the neurocognitive performance. Actually, current literature suggests both beneficial and detrimental cognitive effects of levodopa in PD46. Moreover, if the analysis included a comparison between the pre- and post-operative status in the on-medication condition, the different management of postoperative medication could be another confounding factor. Last but not least, the follow-up periods in different studies ranged from months to years, and several studies only assessed the clinical outcomes in a subacute setting. Therefore, the discrepancies in the study design may considerably limit the interpretation and comparison of the literature.
Baseline characteristics
One of the prominent clinical characteristics in PD is an asymmetrical distribution of motor symptoms at the onset and during the disease course47. The asymmetrical loss of dopaminergic innervation in the striatum has been suggested as the root of the symptom laterality in PD. Because of the hemispherical lateralization of several cognitive and affective functions and the potential role of impaired dopaminergic transmission in non-motor symptoms in PD, several studies have been focused on the correlation between the symptom laterality and the prevalence and severity of several aspects of cognitive and neuropsychiatric domains in PD48,49,50. For instance, one literature review concluded that right-sided motor symptom predominance (i.e., a putative left-sided hemisphere dominant dopamine deficiency) was associated with deficits in language-related functions and verbal memory in PD patients. In contrast, patients with left-sided motor symptom predominance (i.e., a putative right-sided hemisphere dominant dopamine deficiency) showed worse performance in tasks of spatial attention, visuospatial orienting, and memory and mental imagery48. However, several studies, failed to identify such a relationship in patients with early-stage unmedicated PD49,50. These studies suggest a negative effect of dopamine-replacement therapy on the development of lateralized cognitive deficits in relation to the symptom laterality. Nevertheless, symptom laterality serves as a non-negligible factor for the interpretation of the putative lateralization of DBS efficacy in PD.
Furthermore, right- or left-handedness—a critical phenotype for hemispheric language dominance51,52,53—was not systematically and objectively analyzed in the articles included in this review. We suggest that the precise and individualized determination of cerebral dominance would be beneficial for delineating the potential lateralized effects of DBS in PD.
Trajectory and location of lead contacts
The surgical trajectory and electrode placement in relation to the STN topography are critical sources of variation in postoperative outcome in PD54,55,56,57,58. For example, York et al. reported that declines of several aspects of neuropsychological outcomes after STN DBS in PD patients may be related to the trajectory as well as electrode location in a hemisphere-specific manner54. Witt et al. also indicated an association between surgical trajectory through the head of the caudate nuclei and declines in global cognitive performance in PD patients with STN DBS55. Specifically, Tripoliti et al. found that the medially located electrodes in the left STN and the high stimulating intensity of the left electrode were significantly associated with the poor outcome of the speech intelligibility after bilateral STN DBS surgery57. More recently, Petry-Schmelzer et al. reported that the inter-individual variability of non-motor outcomes (e.g., mood/apathy, attention/memory, and sleep outcomes) after STN DBS in PD patients may depend on the location of neurostimulation58.
Moreover, the number of microelectrode recording (MER) trajectories has been hypothesized to contribute to cognitive declines following DBS surgery, because the degree of local injury along the trajectory or at the target site would increase as the number of MER passes increase59. Limited evidence suggests that the microlesional effect could contribute to the early transient verbal fluency decline following DBS surgery, while the long-term fluency impairment might be related to the direct effect of STN DBS60. Later, two retrospective studies concordantly reported that the postoperative cognitive change at approximately 1-year follow-up was not correlated with the number of MER trajectories59,61. Prospective studies are warranted to confirm these findings in the future.
Stimulation parameters
Varying stimulating parameters (i.e., contact, stimulating intensity, frequency, and pulse width) may also considerably affect the treatment efficacy and introduce adverse effects in PD62,63. As mentioned above, Tripoliti et al. presented a correlation between the high stimulating intensity of the left electrode and the result of poor speech intelligibility after bilateral STN DBS surgery57. Moreover, severe gait disturbances and freezing episodes often appear in patients with long-term high-frequency DBS64. Evidence suggested an amelioration of gait disorders with low-frequency (60 Hz) STN stimulation in PD64,65. In addition, several studies showed that a lateralized STN neuromodulation (i.e., unilateral reduction of stimulating intensity) can also affect the gait disturbance and posture in PD66,67. For example, Fasano et al. showed that reducing the STN stimulation voltage on the contralateral side of the leg with a longer step length could improve the frequency and duration of gait freezing66. Twenty-two participants with bilateral STN DBS were assessed in four stimulation conditions (i.e., off-stimulation, bilateral on-stimulation, unilateral on-stimulations) in a subacute setting, while the chronic effect of stimulating intensity reduction on axial and appendicular motor functions was not investigated. More recently, a PD case with Pisa syndrome following chronic bilateral STN DBS successfully treated with left-sided stimulating intensity reduction was reported by Lizarraga et al.67. The lateral trunk flexion angle reduced from 12° to 4° by reducing the left-STN stimulation voltage from 4.8 to 3.8 V67. Although these findings are preliminary and should be interpreted with caution given the methodological drawbacks and limited sample size, the potential feasibility of the lateralized STN neuromodulation strategy suggests the presence of a functional lateralization of the basal ganglia.
Limitations
The main limitation of this comprehensive review relies on the overall low-quality of the current literature investigating the potential lateralized effects of DBS in PD. The majority of the studies were conducted on small samples, possibly due in part to the substantial burden of clinical evaluation under various stimulus conditions. Most of the studies assessed clinical outcomes only in a subacute setting or at a short-term follow-up. Few studies used or specified a randomized and blinded evaluation paradigm to minimize biases. Furthermore, potential confounding factors discussed above were not well addressed in the current literature, which considerably limited the interpolation of the findings. For instance, effects of location of active contacts and trajectories on neurocognitive outcomes were poorly discussed in the literature involved in this review. Furthermore, authors paid little attention to the correlation between changes in motor and non-motor symptoms when investigating the presumed lateralized DBS effects. This could be interesting because a lack of correlation might suggest different underlying mechanisms of the potential lateralized DBS effects on motor and non-motor domains of PD.
Conclusions and future directions
There is insufficient evidence in current literature to draw solid conclusions about the lateralized effects of DBS on motor and non-motor outcomes in PD. Several factors, such as the inherent bias in experimental design, symptom laterality, and location of active contacts with respect to the putative topography of the nuclei, surgical trajectory, and DBS programming strategies should be considered for the accurate interpretation of results. Nevertheless, limited evidence suggests potential lateralized effects of STN DBS on both axial motor symptoms and language-related functions in PD.
To date, most of the studies have focused on STN DBS, and the potential efficacy of lateralization of GPi DBS in PD has not been adequately investigated. In addition, whether STN and GPi DBS exert differential lateralization effects on motor and non-motor outcomes in PD also warrants further investigation. Ongoing research focusing on delineating the lateralized effects of DBS can lead to a better understanding of the therapeutic mechanisms of DBS in PD. This would potentially contribute to improving treatment strategies such as personalized target selection (e.g., bilateral asymmetric implant68), surgical planning, and postoperative management that ultimately benefits patients.
Methods
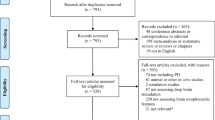
Ethical approval and patient consent were not required for this study. The main inclusion criteria were articles that directly compared the efficacy of unilateral left- to right-sided DBS on motor or non-motor symptoms in PD. Publications in English language before February 2021 were initially searched in PubMed database by using the following search criteria: ((((((((left[Title/Abstract]) OR (right[Title/Abstract])) OR (sided[Title/Abstract])) OR (left-sided[Title/Abstract])) OR (right-sided[Title/Abstract])) OR (laterality[Title/Abstract])) AND (deep brain stimulation[MeSH Terms])) AND (parkinson’s disease[MeSH Terms])) AND (english[Language]). The search results were verified manually. Of the 243 publications, 225 articles were excluded after title and abstract screening. Subsequently, the full texts of potentially relevant publications were analyzed. The references, citations, and similar articles suggested in PubMed for the included articles were also screened for additional eligible studies. The literature search was conducted by Z. Lin and C. Zhang. Finally, after duplicate removal, 27 publications were included in this review (Table 1). The quality of the publications was classified according to the Classification of Evidence Schemes of the Clinical Practice Guideline Process Manual of the American Academy of Neurology69.
Data availability
No datasets were generated or analyzed during the current study.
References
Groen, M. A., Whitehouse, A. J. O., Badcock, N. A. & Bishop, D. V. M. Does cerebral lateralization develop? A study using functional transcranial Doppler ultrasound assessing lateralization for language production and visuospatial memory. Brain Behav. 2, 256–269 (2012).
Lizarraga, K. J. et al. Asymmetric neuromodulation of motor circuits in Parkinson’s disease: the role of subthalamic deep brain stimulation. Surg. Neurol. Int. 8, 261 (2017).
Utter, A. A. & Basso, M. A. The basal ganglia: an overview of circuits and function. Neurosci. Biobehav. Rev. 32, 333–342 (2008).
Glick, S. D., Ross, D. A. & Hough, L. B. Lateral asymmetry of neurotransmitters in human brain. Brain Res. 234, 53–63 (1982).
Cheesman, A. L. et al. Lateralisation of striatal function: evidence from 18F-dopa PET in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 76, 1204–1210 (2005).
Kooistra, C. A. & Heilman, K. M. Motor dominance and lateral asymmetry of the globus pallidus. Neurology 38, 388–390 (1988).
Eitan, R. et al. Asymmetric right/left encoding of emotions in the human subthalamic nucleus. Front. Syst. Neurosci. 7, 69 (2013).
Kalia, L. V. & Lang, A. E. Parkinson’s disease. Lancet 386, 896–912 (2015).
Weaver, F. M. et al. Bilateral deep brain stimulation vs best medical therapy for patients with advanced Parkinson disease: a randomized controlled trial. JAMA 301, 63–73 (2009).
Williams, A. et al. Deep brain stimulation plus best medical therapy versus best medical therapy alone for advanced Parkinson’s disease (PD SURG trial): a randomised, open-label trial. Lancet Neurol. 9, 581–591 (2010).
Ramirez-Zamora, A. & Ostrem, J. L. Globus pallidus interna or subthalamic nucleus deep brain stimulation for Parkinson disease: a review. JAMA Neurol. 75, 367–372 (2018).
Okun, M. S. Deep-brain stimulation for Parkinson’s disease. N. Engl. J. Med. 367, 1529–1538 (2012).
Limousin, P. & Foltynie, T. Long-term outcomes of deep brain stimulation in Parkinson disease. Nat. Rev. Neurol. 15, 234–242 (2019).
Tabbal, S. D. et al. Unilateral subthalamic nucleus stimulation has a measurable ipsilateral effect on rigidity and bradykinesia in Parkinson disease. Exp. Neurol. 211, 234–242 (2008).
Hershey, T. et al. Unilateral vs. bilateral STN DBS effects on working memory and motor function in Parkinson disease. Exp. Neurol. 210, 402–408 (2008).
Castrioto, A. et al. The dominant-STN phenomenon in bilateral STN DBS for Parkinson’s disease. Neurobiol. Dis. 41, 131–137 (2011).
Schulz, G. M. et al. Selective left, right and bilateral stimulation of subthalamic nuclei in Parkinson’s disease: differential effects on motor, speech and language function. J. Parkinsons. Dis. 2, 29–40 (2012).
Lizarraga, K. J., Jagid, J. R. & Luca, C. C. Comparative effects of unilateral and bilateral subthalamic nucleus deep brain stimulation on gait kinematics in Parkinson’s disease: a randomized, blinded study. J. Neurol. 263, 1652–1656 (2016).
Rizzone, M. G., Ferrarin, M., Lanotte, M. M., Lopiano, L. & Carpinella, I. The dominant-subthalamic nucleus phenomenon in bilateral deep brain stimulation for Parkinson’s disease: evidence from a gait analysis study. Front. Neurol. 8, 575 (2017).
Shemisa, K. et al. Unilateral deep brain stimulation surgery in Parkinson’s disease improves ipsilateral symptoms regardless of laterality. Parkinsonism Relat. Disord. 17, 745–748 (2011).
Green, J. & Barnhart, H. The impact of lesion laterality on neuropsychological change following posterior pallidotomy: a review of current findings. Brain Cogn. 42, 379–398 (2000).
Tröster, A. I., Woods, S. P. & Fields, J. A. Verbal fluency declines after pallidotomy: an interaction between task and lesion laterality. Appl. Neuropsychol. 10, 69–75 (2003).
Obwegeser, A. A. et al. Predictors of neuropsychological outcome in patients following microelectrode-guided pallidotomy for Parkinson’s disease. J. Neurosurg. 93, 410–420 (2000).
Vingerhoets, G. et al. Cognitive outcome after unilateral pallidal stimulation in Parkinson’s disease. J. Neurol. Neurosurg. Psychiatry 66, 297–304 (1999).
Fields, J. A., Tröster, A. I., Wilkinson, S. B., Pahwa, R. & Koller, W. C. Cognitive outcome following staged bilateral pallidal stimulation for the treatment of Parkinson’s disease. Clin. Neurol. Neurosurg. 101, 182–188 (1999).
Rothlind, J. C., Cockshott, R. W., Starr, P. A. & Marks, W. J. J. Neuropsychological performance following staged bilateral pallidal or subthalamic nucleus deep brain stimulation for Parkinson’s disease. J. Int. Neuropsychol. Soc. 13, 68–79 (2007).
Zahodne, L. B. et al. Cognitive declines one year after unilateral deep brain stimulation surgery in Parkinson’s disease: a controlled study using reliable change. Clin. Neuropsychol. 23, 385–405 (2009).
Tröster, A. I., Woods, S. P., Fields, J. A., Hanisch, C. & Beatty, W. W. Declines in switching underlie verbal fluency changes after unilateral pallidal surgery in Parkinson’s disease. Brain Cogn. 50, 207–217 (2002).
Lueken, U., Schwarz, M., Hertel, F., Schweiger, E. & Wittling, W. Impaired performance on the Wisconsin Card Sorting Test under left- when compared to right-sided deep brain stimulation of the subthalamic nucleus in patients with Parkinson’s disease. J. Neurol. 255, 1940–1948 (2008).
David, F. J., Goelz, L. C., Tangonan, R. Z., Metman, L. V. & Corcos, D. M. Bilateral deep brain stimulation of the subthalamic nucleus increases pointing error during memory-guided sequential reaching. Exp. Brain Res. 236, 1053–1065 (2018).
Goelz, L. C. et al. The effects of unilateral versus bilateral subthalamic nucleus deep brain stimulation on prosaccades and antisaccades in Parkinson’s disease. Exp. Brain Res. 235, 615–626 (2017).
Sjöberg, R. L. et al. Verbal fluency in patients receiving bilateral versus left-sided deep brain stimulation of the subthalamic nucleus for Parkinson’s disease. J. Int. Neuropsychol. Soc. 18, 606–611 (2012).
Yilmaz, R., Akbostancı, M. C., Mercan, F. N., Sorgun, M. H. & Savaş, A. No effect of different stimulation conditions on verbal fluency and visuospatial orientation in patients with subthalamic nucleus deep brain stimulation. Stereotact. Funct. Neurosurg. 93, 326–332 (2015).
Witt, K., Kopper, F., Deuschl, G. & Krack, P. Subthalamic nucleus influences spatial orientation in extra-personal space. Mov. Disord. 21, 354–361 (2006).
Schmalbach, B. et al. The subthalamic nucleus influences visuospatial attention in humans. J. Cogn. Neurosci. 26, 543–550 (2014).
Ray, N. J. et al. The role of the subthalamic nucleus in response inhibition: evidence from deep brain stimulation for Parkinson’s disease. Neuropsychologia 47, 2828–2834 (2009).
Mirabella, G. et al. Deep brain stimulation of subthalamic nuclei affects arm response inhibition in Parkinson’s patients. Cereb. Cortex 22, 1124–1132 (2012).
Mancini, C. et al. Unilateral Stimulation of subthalamic nucleus does not affect inhibitory control. Front. Neurol. 9, 1149 (2018).
Santens, P., De Letter, M., Van Borsel, J., De Reuck, J. & Caemaert, J. Lateralized effects of subthalamic nucleus stimulation on different aspects of speech in Parkinson’s disease. Brain Lang. 87, 253–258 (2003).
Wang, E. Q. et al. Hemisphere-specific effects of subthalamic nucleus deep brain stimulation on speaking rate and articulatory accuracy of syllable repetitions in Parkinson’s disease. J. Med. Speech Lang. Pathol. 14, 323–334 (2006).
Wang, E., Verhagen Metman, L., Bakay, R., Arzbaecher, J. & Bernard, B. The effect of unilateral electrostimulation of the subthalamic nucleus on respiratory/phonatory subsystems of speech production in Parkinson’s disease–a preliminary report. Clin. Linguist. Phon. 17, 283–289 (2003).
Campbell, M. C. et al. Mood response to deep brain stimulation of the subthalamic nucleus in Parkinson’s disease. J. Neuropsychiatry Clin. Neurosci. 24, 28–36 (2012).
Birchall, E. L. et al. The effect of unilateral subthalamic nucleus deep brain stimulation on depression in Parkinson’s disease. Brain Stimul. 10, 651–656 (2017).
Kirsch-Darrow, L. et al. The trajectory of apathy after deep brain stimulation: from pre-surgery to 6 months post-surgery in Parkinson’s disease. Parkinsonism Relat. Disord. 17, 182–188 (2011).
Amara, A. W. et al. Unilateral subthalamic nucleus deep brain stimulation improves sleep quality in Parkinson’s disease. Parkinsonism Relat. Disord. 18, 63–68 (2012).
Cools, R. Dopaminergic modulation of cognitive function-implications for L-DOPA treatment in Parkinson’s disease. Neurosci. Biobehav. Rev. 30, 1–23 (2006).
Djaldetti, R., Ziv, I. & Melamed, E. The mystery of motor asymmetry in Parkinson’s disease. Lancet Neurol. 5, 796–802 (2006).
Verreyt, N., Nys, G. M. S., Santens, P. & Vingerhoets, G. Cognitive differences between patients with left-sided and right-sided Parkinson’s disease. A review. Neuropsychol. Rev. 21, 405–424 (2011).
Erro, R. et al. Side of onset does not influence cognition in newly diagnosed untreated Parkinson’s disease patients. Parkinsonism Relat. Disord. 19, 256–259 (2013).
Pellicano, C. et al. Neuropsychiatric and cognitive symptoms and body side of onset of parkinsonism in unmedicated Parkinson’s disease patients. Parkinsonism Relat. Disord. 21, 1096–1100 (2015).
Annett, M. Handedness and cerebral dominance: the right shift theory. J. Neuropsychiatry Clin. Neurosci. 10, 459–469 (1998).
Knecht, S. et al. Handedness and hemispheric language dominance in healthy humans. Brain 123(Pt 12), 2512–2518 (2000).
Isaacs, K. L., Barr, W. B., Nelson, P. K. & Devinsky, O. Degree of handedness and cerebral dominance. Neurology 66, 1855–1858 (2006).
York, M. K., Wilde, E. A., Simpson, R. & Jankovic, J. Relationship between neuropsychological outcome and DBS surgical trajectory and electrode location. J. Neurol. Sci. 287, 159–171 (2009).
Witt, K. et al. Relation of lead trajectory and electrode position to neuropsychological outcomes of subthalamic neurostimulation in Parkinson’s disease: results from a randomized trial. Brain 136, 2109–2119 (2013).
Mosley, P. E. et al. The site of stimulation moderates neuropsychiatric symptoms after subthalamic deep brain stimulation for Parkinson’s disease. NeuroImage. Clin. 18, 996–1006 (2018).
Tripoliti, E. et al. Effects of subthalamic stimulation on speech of consecutive patients with Parkinson disease. Neurology 76, 80–86 (2011).
Petry-Schmelzer, J. N. et al. Non-motor outcomes depend on location of neurostimulation in Parkinson’s disease. Brain 142, 3592–3604 (2019).
Mulders, A. E. P. et al. The association between surgical characteristics and cognitive decline following deep brain stimulation of the subthalamic nucleus in Parkinson’s disease. Clin. Neurol. Neurosurg. 200, 106341 (2021).
Lefaucheur, R. et al. Early verbal fluency decline after STN implantation: is it a cognitive microlesion effect? J. Neurol. Sci. 321, 96–99 (2012).
Smith, K. M., O’Connor, M., Papavassiliou, E., Tarsy, D. & Shih, L. C. Phonemic verbal fluency decline after subthalamic nucleus deep brain stimulation does not depend on number of microelectrode recordings or lead tip placement. Parkinsonism Relat. Disord. 20, 400–404 (2014).
Francel, P. et al. Deep brain stimulation for Parkinson’s disease: association between stimulation parameters and cognitive performance. Stereotact. Funct. Neurosurg. 82, 191–193 (2004).
Dayal, V., Limousin, P. & Foltynie, T. Subthalamic nucleus deep brain stimulation in Parkinson’s disease: the effect of varying stimulation parameters. J. Parkinsons. Dis. 7, 235–245 (2017).
Moreau, C. et al. STN-DBS frequency effects on freezing of gait in advanced Parkinson disease. Neurology 71, 80–84 (2008).
Xie, T. et al. Low-frequency stimulation of STN-DBS reduces aspiration and freezing of gait in patients with PD. Neurology 84, 415–420 (2015).
Fasano, A. et al. Modulation of gait coordination by subthalamic stimulation improves freezing of gait. Mov. Disord. 26, 844–851 (2011).
Lizarraga, K. J., Naghibzadeh, M., Boutet, A., Elias, G. J. B. & Fasano, A. Management of Pisa syndrome with lateralized subthalamic stimulation. J. Neurol. 265, 2442–2444 (2018) .
Zhang, C. et al. Combined unilateral subthalamic nucleus and contralateral globus pallidus interna deep brain stimulation for treatment of Parkinson disease: a pilot study of symptom-tailored stimulation. Neurosurgery 87, 1139–1147 (2020).
Gronseth, G. S., et al.; on behalf of the Guideline Development, Dissemination, and Implementation Subcommittee of the American Academy of Neurology. 2017. Clinical Practice Guideline Process Manual, 2017 ed. Minneapolis, MN: The American Academy of Neurology (2017).
Acknowledgements
This study was sponsored by Shanghai Sailing Program (20YF1426500 to ZCC). C.Z. is supported by the fellowship of Shanghai Research Center for Brain Science and Brain-Inspired Intelligence. We appreciate the intellectual inputs from Linbin Wang and Xinmeng Xu.
Author information
Authors and Affiliations
Contributions
Study concept and design: B.S. and D.L.; Data collection and interpretation: Z.L.; Drafting of the manuscript: Z.L.; Critical revision of the manuscript: All authors.
Corresponding authors
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Lin, Z., Zhang, C., Li, D. et al. Lateralized effects of deep brain stimulation in Parkinson’s disease: evidence and controversies. npj Parkinsons Dis. 7, 64 (2021). https://doi.org/10.1038/s41531-021-00209-3
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41531-021-00209-3
This article is cited by
-
Deep brain stimulation of the subthalamic nucleus in severe Parkinson’s disease: relationships between dual-contact topographic setting and 1-year worsening of speech and gait
Acta Neurochirurgica (2023)
-
“Suboptimal” placement of STN DBS electrodes as a novel strategy in Parkinson’s disease?
Acta Neurochirurgica (2023)
