
Abstract
Data on the risk of breast cancer following a benign breast disease (BBD) diagnosis were derived predominantly from populations of women biopsied before the widespread use of mammographic screening and in whom these lesions were mostly incidental findings. Whether or not similar risk associations are seen when these lesions are detected in mammographically screened populations is unknown. To address this, we examined the variation in BBD and breast cancer risk associations by the calendar time of BBD diagnosis (pre- vs. post-mammography era [before vs. 1985 and after]) in a nested case–control study within the Nurses’ Health Study (NHS) and NHSII BBD subcohort (488 cases; 1908 controls). We performed logistic regression analysis, adjusting for matching factors and potential confounders, to estimate odds ratio (ORs) and 95% confidence interval (CI) for the association between BBD subtype (non-proliferative, proliferative without atypia, proliferative with atypical hyperplasia (AH)) and subsequent breast cancer risk. When compared with non-proliferative lesions, both proliferative lesions without atypia (PWA) and AHs were associated with similar levels of risk in the pre-mammographic (pre) and post-mammographic (post) time periods (PWA: OR [95% CI] = 1.73 [1.27, 2.36] pre vs. 1.12 [0.73, 1.74] post; AH: 4.41 [2.90, 6.70] pre vs. 3.69 [2.21, 6.15] post). The interaction by mammography era was not statistically significant (p-interaction = 0.47). These results suggest that the risk associations reported for BBD subtypes in the pre-mammography era remain valid for BBD detected after the widespread implementation of mammographic screening.
Similar content being viewed by others

Introduction
Benign breast disease (BBD) is a term that encompasses a heterogeneous group of lesions with different levels of subsequent breast cancer risk. To date, most epidemiologic studies, including studies from our group, have shown that proliferative lesions without atypia are associated with a 1.5- to 2-fold increase in breast cancer risk, whereas atypical hyperplasias are associated with a 4–5-fold increase in risk1,2,3,4. However, these data were derived from populations of women who, for the most part, were biopsied before the widespread use of screening mammography and in whom these lesions were incidental findings in the context of a clinically symptomatic lesion, most often a palpable mass, that was surgically excised5. It is unknown whether the BBD risk associations based on biopsies performed in the pre-mammography era1,2,3,4 are applicable to the BBDs detected in biopsies performed for a non-palpable lesion detected by screening mammography. This is an important clinical question that could have a significant impact on individual patient counseling, risk estimation models, and design and evaluation of preventive interventions.
In this study, we examined whether the associations of BBD subtype (non-proliferative lesions, proliferative lesions without atypia, atypical hyperplasia) with breast cancer risk were similar between the pre- and post-mammography era (before vs. 1985 and after). We also examined whether the associations vary by BBD detection method (mammogram vs. self-exam/physician’s exam). For these analyses, we used a nested case–control study within the Nurses’ Health Study (NHS) and NHSII BBD subcohort. Because mammographic screening was widely implemented in the United States in the mid-1980, we used 1985 as the surrogate year for defining pre- vs. post-mammography era in primary analyses.
Results
Population characteristics
Participant characteristics of 488 cases and 1908 controls in the pre- and post-mammography era are presented in Table 1. The mean age at BBD biopsy among controls was 41.0 years in pre-mammography era and 49.8 years in the post-mammography period. Compared to women with BBDs detected during pre-mammography era, those with BBDs detected during post-mammography era were more likely to have atypical hyperplasia, higher adult body mass index (BMI), and higher levels of physical activity. They were also less likely to be current smokers. Among controls, 43.5% of BBDs diagnosed during the post-mammography era were detected on mammograms compared with 8.7% during pre-mammography era.
BBD subtype and breast cancer risk
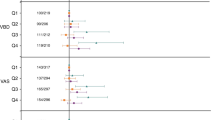
In all women, proliferative lesions without atypia and atypical hyperplasia were associated with a 1.50-fold (95% confidence interval [CI] = 1.17–1.93) and 4.24-fold (95% CI = 3.08–5.83) higher breast cancer risk, respectively, compared with non-proliferative lesions (Table 2). Similar associations were found with vs. without adjustment for potential confounders. When stratified by mammography era, proliferative lesions without atypia were associated with a 1.73-fold higher risk of breast cancer (95% CI = 1.27–2.36), and atypical hyperplasia was associated with a 4.41-fold higher risk (95% CI = 2.90–6.70) compared with non-proliferative lesions during the pre-mammography era (Table 2). The risk associations were similar during the post-mammography era (proliferative lesions without atypia vs. non-proliferative: odds ratio [OR] = 1.12, 95% CI = 0.73–1.74; atypical hyperplasia vs. non-proliferative: OR = 3.69, 95% CI = 2.21–6.15) and the interaction by mammography era was not statistically significant (p-interaction = 0.47). When BBD subtype was further categorized into atypical ductal and lobular hyperplasia, the highest risk was observed with atypical lobular hyperplasia (pre-mammography era: OR = 6.16, 95% CI = 3.43–11.1; post-mammography era: OR = 6.17, 95% CI = 3.23–11.8), followed by atypical ductal hyperplasia (pre-mammography era: OR = 3.58, 95% CI = 2.18–5.88; post-mammography era: OR = 2.55, 95% CI = 1.38–4.71) in both pre- and post-mammography era (p-interaction=0.63) (Supplementary Table 1). When stratified by menopausal status, the association with atypical hyperplasia appeared stronger in postmenopausal women than in premenopausal women, but the interaction was not statistically significant in both the pre- (p-interaction=0.66) and post-mammography era (p-interaction=0.60) (Supplementary Table 2).
Since many of the lesions in the pre-mammography era were biopsied due to the presence of a clinically symptomatic lesion, we also stratified the analysis by the method of BBD detection. In this analysis, the risk associations were also similar between the stratum of BBD found on self-exam or physician’s exam (proliferative without atypia vs. non-proliferative: OR = 1.49, 95% CI = 1.11–2.01; atypical hyperplasia vs. non-proliferative: OR = 3.98, 95% CI = 2.68–5.92) and the stratum of BBDs found on mammography (proliferative without atypia vs. non-proliferative: OR = 1.45, 95% CI = 0.71–2.98; atypical hyperplasia vs. non-proliferative: OR = 5.12, 95% CI = 2.36–11.1) and the interaction was not statistically significant (p-interaction=0.11) (Table 3).
Sensitivity analyses
In a sensitivity analysis, the results did not change when 1980 was used to define the start of the mammography era (Supplementary Table 3). Because the results could have been influenced by the shorter follow-up time in the post-mammography era, we also excluded individuals with follow-up time >13 years (the maximum follow-up time in the post-mammography era) in another sensitivity analysis and results were similar (Supplementary Table 4).
Discussion
Breast cancer risks associated with BBD subtypes were reported by studies that followed up large cohorts of women undergoing breast biopsies with different baseline characteristics and indications for biopsies, possibly reducing the ability to generalize these results to women undergoing breast biopsies for abnormalities detected by screening mammography. This observation not only has potential consequences for individual patient counseling but could affect some of today’s best-known breast cancer risk prediction models that use features like the number of biopsies and BBD subtype6,7,8,9,10,11. While these differences have been recognized in terms of breast cancer risk development models5,6, we investigated in this study whether the previously estimated BBD–cancer risk associations are still valid after the widespread introduction of screening mammography. In the current study, we found similar BBD–breast cancer risk associations from BBDs detected in the pre- vs. post-mammography era. Consistent with this, we also observed similar associations from BBDs first detected on self-exam or physician’s exam vs. BBDs detected on mammography. Our estimated associations were also similar to those previously reported in other studies from pre-mammography era utilizing distinct cohorts1,5,12. However, in contrast to a prior report from this cohort13, in the current study we found no significant differences in associations when stratifying by menopausal status particularly in the post-mammography era. In a previous iteration of this cohort, with a smaller sample size and shorter follow-up time, we had observed a stronger association with atypical hyperplasia in premenopausal (vs. postmenopausal) women13. This observation was not confirmed in this study in either the pre- or post-mammography era.
In this study, the use of biopsy-confirmed BBDs, the use of prospective study design, and the careful adjustment for potential confounders are important strengths. While we cannot exclude the existence of small significant differences, we were not able to detect these, given our limited sample size; if these existed, they would probably be clinically insignificant. Although sample size may be limited for stratified analyses, this study is still one of the largest studies to date that examined the BBD–breast cancer risk relationship. Our previous study published in 2007 included 395 cases and 1610 controls3, whereas this study includes 488 cases and 1908 controls with biopsy-confirmed BBDs. Although the exact year that should be used for the start of widespread mammography is difficult to determine, we confirmed 77% of NHS/NHSII women aged ≥40 years received mammography in 1988/1989. A proportion of BBDs first detected on mammogram was also higher in post-mammography era (1985 and after) compared with pre-mammography era (44 vs. 9%). Further, it is generally accepted that widespread access to mammographic screening happened in the United States in the mid-1980s, and, therefore, we believe 1985 is an appropriate surrogate14,15,16. It should also be noted that we had sparse information on biopsy method and thus were not able to determine the prevalence of core needle biopsies. This fact made stratified analyses by core needle biopsy vs. surgical biopsy impossible. While such an analysis would have been informative and potentially more generalizable to contemporary practice, it was not until the late 1990s/early 2000s that core needle biopsy became the principal method for the diagnosis of non-palpable breast lesions. As the NHS and NHSII are ongoing prospective studies, it may be possible in the future to confirm our results by including more recent data from patients with image-directed core-biopsied lesions. Nevertheless, we believe this study still provides important insights since it is the first study to date that has compared the BBD–breast cancer risk associations before and after the widespread implementation of screening mammography.
In conclusion, our data suggest that the magnitude of risk associated with BBD subtypes initially reported from women biopsied in the pre-mammography era remains valid for BBD detected after the widespread use of mammography. Given the limited information available on the type of biopsy performed, further studies of patients in which BBDs were detected by core-needle biopsy are needed to confirm our results.
Methods
Study subjects
This study is a nested case–control study within the NHS and NHS II cohorts with biopsy-confirmed BBD. The NHS is an ongoing prospective cohort study that began in 1976, when 121,700 female registered nurses between the ages of 30 and 55 years completed a mailed questionnaire. The NHS II consists of 116,609 female registered nurses who were between the ages of 25 and 42 years when the study began in 1989. In both cohorts, participants have been followed via biennial questionnaires that provide information on lifestyle factors (BMI, physical activity, smoking, and alcohol use), family history of disease, reproductive history, and incident disease17,18. Cumulative response rates for both cohorts were >90% and were similar among women regardless of their BBD diagnosis.
Details on the BBD diagnosis reporting on the questionnaires have been previously described2,19. Briefly, cases were women with biopsy-confirmed BBD who reported a subsequent diagnosis of breast cancer following their BBD diagnosis. Cases (invasive, in situ) were diagnosed between 1976 and 1998 for the NHS and between 1989 and 1999 for the NHS II. Self-reported breast cancers were confirmed by review of medical records. To reduce potential reverse causation, women were excluded if they had evidence of in situ or invasive carcinoma at biopsy or reported a diagnosis of breast cancer within 6 months of their BBD biopsy. There was a mean of 10 years (SD = 6.93) between BBD biopsy and cancer diagnosis. Eligible controls were women who completed the questionnaire in the same year that the breast cancer case was reported and had a previous diagnosis of biopsy-confirmed BBD but were free from breast cancer at the time of the case was diagnosed (index date; date of which the case was diagnosed). Up to four controls were selected for each breast cancer case, matched on year of birth and year of BBD biopsy. Women were excluded if they had unknown BBD lesion type. A total of 488 cases and 1908 controls, in whom the original slides had been reviewed, were eligible for this study. Due to considerable missing information on the laterality of the carcinoma in the cases, this information was not considered in the analysis. The study protocol was approved by the institutional review boards of the Brigham and Women’s Hospital and Harvard T.H. Chan School of Public Health, and those of participating registries as required. Completion of the self-administered questionnaire was presumed to imply informed consent. This study complies with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines20.
Benign breast biopsy specimens
Eligible cases and controls were contacted for permission to obtain their BBD pathology records and biopsy specimens, and specimens were then obtained from hospital pathology departments when possible (as detailed in refs. 2,3,21). The ability to obtain biopsy blocks did not significantly differ by case and control status. Two study pathologists independently reviewed the hematoxylin- and eosin-stained sections from the benign breast biopsy blocks and completed detailed worksheets on the subtype of BBD lesion (i.e., non-proliferative, proliferative without atypia, atypical ductal hyperplasia, atypical lobular hyperplasia) in a blinded manner. The details of this nested case–control study and the BBD assessment have been described previously2,3,19,22.
Mode of BBD diagnosis
Women reported the year of BBD diagnosis and how they found BBD (finding on mammography, self-examination, physician’s examination, cyst aspiration before biopsy, other). We considered BBDs detected on both self-exam/physical exam and mammography as first found on self-exam/physical activity (palpable mass). We categorized women into those who had a BBD diagnosis in the pre- vs. post-mammography era. In primary analysis, we used 1985 as the cutpoint calendar year for defining pre- vs. post-mammography era because mammography screening was widely implemented in the United States. in the mid-1980. In the sensitivity analysis, we repeated the analyses using 1980 as the cutpoint calendar year for defining mammography era. Starting in 1988 in the NHS and 1989 in the NHSII, biennial questionnaires asked questions on whether women received mammogram and the year since the last mammogram. In the NHS, 77% of women have ever had any mammogram in 1988 (with an unknown proportion for screening mammogram) and, among these women, 56% had the most recent mammogram within 1 year. In the NHSII, 77% of women at age ≥40 years have ever had any mammogram in 1989 and, among these women, 79% had the routine screening and 46% had the most recent mammogram within 1 year. In 1990–1991, 76% of NHS participants and 70% of NHSII participants had a screening mammogram.
Statistical analysis
To avoid losing data due to incomplete matched sets (benign biopsy blocks were not available for some cases and controls), we performed unconditional logistic regression analysis, adjusting for matching factors, to estimate ORs and 95% CIs for the association between BBD subtype (non-proliferative, proliferative without atypia, proliferative with atypical hyperplasia) and subsequent breast cancer risk. Multivariable models included matching factors (age at diagnosis [for cases] or at index date [for controls], time between biopsy to breast cancer diagnosis or index date, calendar year of benign breast biopsy) and potential confounders (average body fatness at ages 5–10 years, adult BMI at benign biopsy, age at first birth, menopausal status at benign breast biopsy, current smoking, alcohol intake, physical activity, family history of breast cancer). In the secondary analysis, we further categorized proliferative lesions with atypical hyperplasia into atypical ductal hyperplasia and atypical lobular hyperplasia. To assess the variation in associations by the mode of BBD diagnosis, we stratified the analyses by the calendar time of BBD diagnosis (pre- vs. post-mammography era [before vs. 1985 and after]) and the methods of BBD detection (mammogram vs. self-exam/physician’s exam vs. other). In the sensitivity analysis, we repeated the analyses using 1980 as the cutpoint calendar year for mammography era. Because results could be influenced by the different length of follow-up time in the pre- vs. post-mammography era, we also excluded individuals with follow-up time >13 years (the maximum follow-up time in the post-mammography era) in the sensitivity analysis. Interaction tests were performed using the likelihood ratio test for product terms.
All statistical tests were two-sided with 5% type I error. Analyses were conducted with SAS version 9 (version 9.2, SAS Institute, Cary, NC, USA).
Reporting summary
Further information on experimental design is available in the Nature Research Reporting Summary linked to this paper.
Data availability
The data generated and analyzed during this study are described in the following metadata record: https://doi.org/10.6084/m9.figshare.1322086723. The data that support the findings of this study are available from the Nurses’ Health Studies but restrictions apply to the availability of these data, and so they are not publicly available. However, the data are available from the corresponding author upon reasonable request, and with the permission of Nurses’ Health Studies External Advisory Board. Additional data sharing information and policy details can be accessed at http://www.nurseshealthstudy.org/researchers.
References
Dupont, W. D. & Page, D. L. Risk factors for breast cancer in women with proliferative breast disease. N. Engl. J. Med. 312, 146–151 (1985).
Collins, L. C. et al. The influence of family history on breast cancer risk in women with biopsy-confirmed benign breast disease: results from the Nurses’ Health Study. Cancer 107, 1240–1247 (2006).
Collins, L. C. et al. Magnitude and laterality of breast cancer risk according to histologic type of atypical hyperplasia. Cancer 109, 180–187 (2007).
Hartmann, L. C. et al. Understanding the premalignant potential of atypical hyperplasia through its natural history: a longitudinal cohort study. Cancer Prev. Res. 7, 211–217 (2014).
Menes, T. S. et al. Subsequent breast cancer risk following diagnosis of atypical ductal hyperplasia on needle biopsy. JAMA Oncol. 3, 36 (2017).
Gail, M. H. et al. Projecting individualized probabilities of developing breast cancer for white females who are being examined annually. J. Natl Cancer Inst. 81, 1879–1886 (1989).
Costantino, J. P. et al. Validation studies for models projecting the risk of invasive and total breast cancer incidence. J. Natl Cancer Inst. 91, 1541–1548 (1999).
Tyrer, J., Duffy, S. W. & Cuzick, J. A breast cancer prediction model incorporating familial and personal risk factors. Stat. Med. 23, 1111–1130 (2004).
Pfeiffer, R. M. et al. Risk prediction for breast, endometrial, and ovarian cancer in white women aged 50 y or older: derivation and validation from population-based cohort studies. PLoS Med. 10, e1001492 (2013).
Tice, J. A. et al. Using clinical factors and mammographic breast density to estimate breast cancer risk: development and validation of a new predictive model. Ann. Intern. Med. 148, 337–347 (2008).
Tice, J. A. et al. Breast density and benign breast disease: Risk assessment to identify women at high risk of breast cancer. J. Clin. Oncol. 33, 3137–3143 (2015).
Carter, C. L., Corle, D. K., Micozzi, M. S., Schatzkin, A. & Taylor, P. R. A prospective study of the development of breast cancer in 16,692 women with benign breast disease. Am. J. Epidemiol. 128, 467–477 (1988).
London, S. J., Connolly, J. L., Schnitt, S. J. & Colditz, G. A. A prospective study of benign breast disease and the risk of breast cancer. JAMA 267, 941–944 (1992).
Welch, H. G., Prorok, P. C., O’Malley, A. J. & Kramer, B. S. Breast-cancer tumor size, overdiagnosis, and mammography screening effectiveness. N. Engl. J. Med. 375, 1438–1447 (2016).
Vierkant, R. A. et al. Mammographic breast density and risk of breast cancer in women with atypical hyperplasia: an observational cohort study from the Mayo Clinic Benign Breast Disease (BBD) cohort. BMC Cancer 17, 84 (2017).
Bleyer, A. & Welch, H. G. Effect of three decades of screening mammography on breast-cancer incidence. N. Engl. J. Med. 367, 1998–2005 (2012).
Tamimi, R. M., Byrne, C., Colditz, G. A. & Hankinson, S. E. Endogenous hormone levels, mammographic density, and subsequent risk of breast cancer in postmenopausal women. J. Natl Cancer Inst. 99, 1178–1187 (2007).
Colditz, G. A. & Hankinson, S. E. The Nurses’ Health Study: lifestyle and health among women. Nat. Rev. Cancer 5, 388–396 (2005).
Tamimi, R. M. et al. Expression of IGF1R in normal breast tissue and subsequent risk of breast cancer. Breast Cancer Res. Treat. 128, 243–250 (2011).
von Elm, E. et al. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 4, e296 (2007).
Aroner, S. A. et al. Radial scars and subsequent breast cancer risk: results from the Nurses’ Health Studies. Breast Cancer Res. Treat. 139, 277–285 (2013).
Beca, F. et al. EZH2 protein expression in normal breast epithelium and risk of breast cancer: results from the Nurses' Health Studies. Breast Cancer Res. 19, 21 (2017).
Beca, F., Oh, H., Collins, L. C., Tamimi, R. M. & Schnitt S. J. Metadata supporting the article: the impact of mammographic screening on the subsequent breast cancer risk associated with biopsy-proven benign breast disease. figshare https://doi.org/10.6084/m9.figshare.13220867 (2021).
Acknowledgements
This work was supported by the National Cancer Institute (NCI) at the National Institute of Health (UM1 CA186107 and UM1 CA176726). F.B. was supported by a trainee stipend from the Arthur Purdy Stout Society of Pathologist, the Department of Pathology of the Stanford University School of Medicine Pathology Trainee Mentored Award in Precision Health and Earlier.org—Friends for An Earlier Breast Cancer Test® Medical Research Grant. H.O. was supported by the National Research Foundation of Korea (NRF) grants (2019R1G1A1004227, 2019S1A3A2099973). Dana-Farber/Harvard Cancer Center is supported, in part, by an NCI Cancer Center Support Grant (P30CA06516). We would like to thank the participants and staff of the Nurses’ Health Study and Nurses’ Health Study II for their valuable contributions, and the following state cancer registries for their help: AL, AZ, AR, CA, CO, CT, DE, FL, GA, ID, IL, IN, IA, KY, LA, ME, MD, MA, MI, NE, NH, NJ, NY, NC, ND, OH, OK, OR, PA, RI, SC, TN, TX, VA, WA, and WY. We would also like to thank Dana-Farber/Harvard Cancer Center in Boston, MA, USA for the use of the Tissue Microarray Imaging Core, which provided the TMA construction service. The authors assume full responsibility for analyses and interpretation of these data.
Author information
Authors and Affiliations
Contributions
F.B., H.O., R.M.T., and S.J.S. conceived and designed the study. F.B., H.O., R.M.T., and S.J.S. ran the data analyses and interpreted the results. F.O. and H.O. are co-first authors, R.M.T. and S.J.S. are co-last authors of the manuscript. All authors participated in the manuscript writing. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
F.B. is currently an employee and equity holder of Seattle Genetics, Inc.; however, this work is outside the scope of his current role and responsibilities. Therefore, this author declares that he has no relevant or material financial interests that relate to the research described in this paper. All other authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Beca, F., Oh, H., Collins, L.C. et al. The impact of mammographic screening on the subsequent breast cancer risk associated with biopsy-proven benign breast disease. npj Breast Cancer 7, 23 (2021). https://doi.org/10.1038/s41523-021-00225-9
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41523-021-00225-9
This article is cited by
-
Early life body size, pubertal timing, and risks of benign breast disease in a large cohort of Danish female adolescents and women
European Journal of Pediatrics (2022)
