
Abstract
We aimed to assess contralateral breast cancer (CBC) risk in patients with ductal carcinoma in situ (DCIS) compared with invasive breast cancer (BC). Women diagnosed with DCIS (N = 28,003) or stage I–III BC (N = 275,836) between 1989 and 2017 were identified from the nationwide Netherlands Cancer Registry. Cumulative incidences were estimated, accounting for competing risks, and hazard ratios (HRs) for metachronous invasive CBC. To evaluate effects of adjuvant systemic therapy and screening, separate analyses were performed for stage I BC without adjuvant systemic therapy and by mode of first BC detection. Multivariable models including clinico-pathological and treatment data were created to assess CBC risk prediction performance in DCIS patients. The 10-year cumulative incidence of invasive CBC was 4.8% for DCIS patients (CBC = 1334). Invasive CBC risk was higher in DCIS patients compared with invasive BC overall (HR = 1.10, 95% confidence interval (CI) = 1.04–1.17), and lower compared with stage I BC without adjuvant systemic therapy (HR = 0.87; 95% CI = 0.82–0.92). In patients diagnosed ≥2011, the HR for invasive CBC was 1.38 (95% CI = 1.35–1.68) after screen-detected DCIS compared with screen-detected invasive BC, and was 2.14 (95% CI = 1.46–3.13) when not screen-detected. The C-index was 0.52 (95% CI = 0.50–0.54) for invasive CBC prediction in DCIS patients. In conclusion, CBC risks are low overall. DCIS patients had a slightly higher risk of invasive CBC compared with invasive BC, likely explained by the risk-reducing effect of (neo)adjuvant systemic therapy among BC patients. For support of clinical decision making more information is needed to differentiate CBC risks among DCIS patients.
Similar content being viewed by others

Introduction
Contralateral breast cancer (CBC) is the most frequent second cancer reported after first invasive breast cancer (BC)1,2,3. The cumulative incidence of invasive CBC for women following invasive BC is ~0.4% per year4,5,6. Several studies have shown a decrease in CBC incidence as a result of (neo)adjuvant systemic therapies6,7,8.
Ductal carcinoma in situ (DCIS) is a potential precursor of invasive BC. The incidence of DCIS has increased substantially with widespread introduction of population-based mammography screening including digital mammography and represents 10–25% of all BC patients9,10,11. As DCIS has an excellent prognosis with a disease-specific survival of >98% at 10 years12,13,14, a large group of women is at risk of developing CBC.
The risk of invasive CBC for DCIS patients has not been widely investigated, but the annual risk is estimated between 0.4 and 0.6%11,13,15,16. Moreover, it is unclear if the risk of CBC is comparable between patients diagnosed with invasive BC and patients with DCIS. One study in the United States, using data from the Surveillance, Epidemiology, and End Results (SEER) database, found a similar relative CBC risk for DCIS patients compared to patients with invasive BC17. On the other hand, an indirect assessment between DCIS patients and invasive BC patients has been provided by a CBC risk prediction model developed and validated in the USA, showing a higher relative CBC risk for DCIS compared with invasive BC (relative risk: 1.60, 95% confidence interval (CI) = 1.42–1.93)18,19. The reason for a potential higher CBC risk for DCIS patients is still unclear, but might relate to the risk-reducing effect of adjuvant systemic therapy among invasive BC patients6,20,21. In general, relatively few DCIS patients receive adjuvant systemic therapy. In addition, CBC risks may also differ based on the mode of detection of the first BC. Previous research showed that screen-detected invasive breast tumors have a better BC-specific survival than non-screened tumors and hence receive less adjuvant systemic treatment22.
The aim of this study was to assess the risk of developing invasive CBC in DCIS patients in direct comparison with patients diagnosed with invasive BC using a large population-based cohort of Dutch BC patients, taking age, mode of first BC detection, and (neo)adjuvant systemic therapy into account. In addition, we evaluated the CBC risk prediction performance in patients diagnosed with DCIS.
Results
Patient characteristics
The cohort comprised 28,003 DCIS patients (CBC = 1334) and 275,836 patients with invasive BC (CBC = 12,821), including 86,481 patients with stage I BC not receiving adjuvant systemic therapy; i.e., no chemotherapy, endocrine therapy, nor trastuzumab (Table 1). The percentage of patients diagnosed with DCIS, of all BC patients diagnosed in the Netherlands, was 5.7% in the implementation phase of the mammography screening program (1989–1998) and 10.5% in the period of full national coverage (1999–2017). Median follow-up was 11.4 years.
CBC risk for patients diagnosed with DCIS and invasive BC
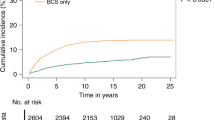
The 10-year cumulative incidence of invasive CBC was 4.8% (95% CI = 4.6–5.2%) for DCIS patients, 4.0% (95% CI = 4.0–4.1%) for all invasive BC patients, and 5.6% (95% CI = 5.4–5.8%) for patients with stage I BC not receiving adjuvant systemic therapy (Table 1, Fig. 123). For comparison, the 10-year cumulative incidence of invasive CBC in patients diagnosed with stage I invasive BC treated with adjuvant systemic therapy was 2.9% (95% CI = 2.5–3.3%). Being diagnosed with DCIS was associated with an increased risk of invasive CBC compared with invasive BC overall (HR = 1.10, 95% CI = 1.04–1.17), and with a lower risk when compared with stage I BC without adjuvant systemic therapy (HR = 0.87, 95% CI = 0.82–0.92, Table 2). Similar results were observed when using competing risk regression (Table 2).

The x axis represents the time since first BC diagnosis (in years) and the y axis the cumulative CBC incidence.
In sensitivity analyses using different time cutoffs for metachronous CBC, results were similar. The HR for invasive CBC developed at least six months after the first BC was 1.10 (95% CI = 1.04–1.17) for DCIS compared with invasive BC, and the HR was 1.09 (95% CI = 1.03–1.16) using a 12-month cutoff.
The cumulative incidence of in situ CBC, death, and invasive ipsilateral BC are shown in Supplementary Figs. 1–323. The 10-year cumulative incidence of in situ CBC was 1.6% (95% CI = 1.5–1.8%) for DCIS patients, 0.8% (95% CI = 0.7–0.8%) for invasive BC patients, and 1.1% (95% CI = 1.0–1.2%) for patients with stage I BC without adjuvant systemic therapy (Table 1). The risk of death was lower in DCIS patients compared to invasive BC patients (HR = 0.47, 95% CI = 0.45–0.49, Supplementary Table 1).
Results by age and screening (period)
Among patients who had their first BC diagnosis during the implementation phase of the national screening program (1989–1998), the risk of invasive CBC was similar in DCIS patients compared with invasive BC patients (HR = 0.93, 95% CI = 0.85–1.03, Table 3, Fig. 2a–c23). In the period of full nationwide coverage of the screening program (1999–2017), the risk of invasive CBC was higher for DCIS patients than for invasive BC patients (HR = 1.19, 95% CI = 1.10–1.27, Table 3, Fig. 2b–d23). The risk of invasive CBC was lower in DCIS patients compared with patients with stage I BC not receiving adjuvant systemic therapy in both periods (1989–1998: HR = 0.90; 95% CI = 0.81–1.00, and 1999–2017: HR = 0.85, 95% CI: 0.79–0.91). The effects were similar stratified by age group (<50 and ≥50 years) (Table 3). The estimated 5- and 10-year cumulative incidences by age and period are shown in Supplementary Table 2.

a patients aged <50 years diagnosed between 1989 and 1998 (implementation phase Dutch mammography screening program); b patients aged <50 years diagnosed between 1999 and 2017 (full national coverage of the Dutch mammography screening program); c patients aged ≥50 years diagnosed between 1989 and 1998; d patients aged ≥50 years diagnosed between 1999 and 2017. The x axis represents the time since first BC diagnosis (in years) and the y axis the cumulative CBC incidence.
In a subgroup of patients diagnosed during or after 2011, with information available on the mode of first BC detection, the HR of invasive CBC was 1.53 (95% CI = 1.29–1.82) for DCIS patients compared with invasive BC patients, and 0.86 (95% CI = 0.71–1.03) compared with patients with stage I BC without adjuvant systemic therapy (Table 4). Among all screen-detected first BCs, the HR of invasive CBC was 1.38 (95% CI = 1.35–1.68) for DCIS patients compared with invasive BC patients and 0.81 (95% CI = 0.66–1.00) compared with stage I BC without adjuvant systemic therapy (Table 4). When the first BC was not detected by screening, the HR of invasive CBC was 2.14 (95% CI = 1.46–3.13) for DCIS patients compared to invasive BC patients and 1.04 (95% CI = 0.68–1.59) compared with stage I BC without adjuvant systemic therapy (Table 4). The risk of death in patients with DCIS compared with invasive BC and stage I BC without adjuvant systemic therapy among screen-detected and not screen-detected is shown in Supplementary Table 3.
Subtype-specific CBC risk
DCIS patients had a lower risk of stage IV CBC (HR = 0.45, 95% CI = 0.22–0.92), and higher risks of grade I invasive CBC (HR = 1.55, 95% CI = 1.31–1.84) and ER-positive invasive CBC (HR = 1.49, 95% CI = 1.33–1.66) compared with all invasive BC patients (Supplementary Table 4). Overall, the subtype-specific CBC risk in DCIS patients was comparable to patients with stage I BC not receiving adjuvant systemic therapy (Supplementary Table 4).
Multivariable model
In the multivariable model, no strong predictors of CBC were identified in DCIS patients (Table 5). The C-index of the multivariable model of invasive CBC was 0.52 (standard deviation (SD = 0.01) for cause-specific Cox regression; when we considered all CBC (in situ and invasive) the C-index was 0.51 (SD = 0.01) (Table 5). When we performed the analyses in a subgroup of patients diagnosed during or after 2011, the C-index was 0.55 (SD = 0.01) without information on the mode of first BC detection, and 0.56 (SD = 0.01) with information available on the mode of first BC detection (data not shown).
Discussion
In this large population-based study, the 10-year cumulative incidence of invasive CBC was 4.8% for DCIS patients. The risk of developing invasive CBC was lower for DCIS patients compared with stage I BC patients not receiving adjuvant systemic therapy (HR = 0.87), but the risk was slightly higher compared with all invasive BC patients (HR = 1.10). A multivariable model, based on the clinical information currently available, was unable to differentiate risks of invasive CBC among DCIS patients.
The slightly higher invasive CBC risk in DCIS patients compared with all invasive BC patients may be explained by the risk-reducing effect of adjuvant systemic therapy among invasive BC patients6,20,21. In our previous study using NCR data6 we showed that adjuvant endocrine therapy, chemotherapy, and trastuzumab combined with chemotherapy were associated with overall 54%, 30%, and 43% risk reductions of CBC, respectively. In our study, a large group (57%) of patients with invasive BC received (neo)adjuvant systemic therapy. According to the Dutch guidelines, DCIS patients are not offered treatment with adjuvant systemic therapy24. The potential influence of adjuvant systemic therapy is supported by the CBC risk evaluation in patients diagnosed with stage I BC not receiving adjuvant systemic therapy, showing a higher CBC risk in such patients than in patients diagnosed with DCIS.
To our knowledge, only one previous study in the United States investigated the risk of CBC in patients with DCIS in direct comparison with patients diagnosed with invasive BC using SEER data17. They found a similar CBC risk (including in situ and invasive) for invasive ductal BC in comparison with DCIS, with a relative risk of 0.98 (95% CI = 0.90–1.06). However, that analysis was based on an earlier, largely pre-screening, period (1973–1996), and lacked information on adjuvant systemic therapy use. Previous studies examining cohorts of DCIS patients have reported a subsequent annual invasive CBC risk of 0.4–0.6%13,15,16, comparable to our finding.
When analyses were restricted to patients with information available on the mode of first BC detection, trends were similar overall. However, the higher CBC risk for DCIS patients compared with invasive BC was more pronounced within the not screen-detected BC group compared with the screen-detected BC group. Tumors not detected by screening could be interval tumors or those arising in women not attending for screening. Certainly, invasive interval tumors tend to be more aggressive than screen-detected BCs and hence receive more often adjuvant systemic treatment22.
We observed that the invasive CBCs developed within the DCIS group were less aggressive than the invasive CBCs developed after invasive first BC, i.e., more estrogen receptor positive (ER-positive), and lower tumor stage and grade. This may be explained by underlying etiological factors and/or be related to the use of adjuvant systemic therapy among invasive BC patients. Studies have shown that adjuvant systemic therapy influences subtype-specific CBC risk, e.g., endocrine therapy strongly reduces the risk of developing ER-positive CBC, but not ER-negative CBC6,21. This is supported by our subgroup analyses in patients with stage I BC not receiving adjuvant systemic therapy, who tended to develop similar CBC subtypes compared with DCIS patients.
The main strength of this study was the use of a large population-based nationwide cohort of DCIS and invasive BC patients, with complete follow-up on CBC over a long period. The NCR did not have follow-up information on distant metastases for all years included and therefore we could not take distant metastasis as a competing event into account. However, in the years where we had information on distant metastases (2003–2006), the median survival was 1.1 years and the 5-year overall survival after distant metastasis was fairly poor (6%). This indicates that death could be used as a proxy for distant metastasis. As we had complete information on death (as a competing event), we do not expect that the lack of information on distant metastases has led to an underestimation of the CBC risk. We also did not have information available about contralateral prophylactic mastectomy (CPM), which may have resulted in an underestimation of the CBC risk and may not have had equal uptake in all groups. According to Dutch guidelines24 only women carrying a BRCA1 or BRCA2 germline mutation are advised to undergo a contralateral preventive mastectomy, as their CBC risk is high with an estimated 10-year risk of ~10–20%25,26 Unfortunately, information about BRCA1 and BRCA2 mutation was lacking. However, we do not expect that this missing information importantly influenced the results since only 1–2% of the DCIS population27, and 3–5% of the invasive BC population25,28 will be BRCA1 or BRCA2 mutation carriers. Finally, <1% of the DCIS patients were not treated according to the Dutch guideline since they received adjuvant chemotherapy, endocrine therapy, and/or trastuzumab. However, since this number is low, we do not expect that this affected our results.
Despite low CBC risks, the use of CPM has increased in recent years, both in patients diagnosed with invasive BC and in patients diagnosed with DCIS, especially in the United States14,29. Therefore, a need of individualized CBC risk prediction may be as important for patients diagnosed with DCIS as for patients with invasive BC. At present, CBC risk prediction models have been developed and validated for patients with invasive BC, but these models may not be appropriate for DCIS patients since most of the information available for invasive BC is not routinely collected in DCIS18,19,30,31. In our study, we had limited information on biological characteristics of DCIS, e.g., no information on receptor subtypes, and our multivariable model was therefore unable to differentiate CBC risk among DCIS patients. So, based on the clinical information currently available, CBC risk prediction in DCIS patients is insufficiently robust to be clinically actionable. More biological knowledge is needed to improve CBC prediction in DCIS patients.
Based on the results of this study we do not suggest to start treating DCIS patients with adjuvant systemic therapy to prevent CBC as the absolute invasive CBC risk is low. To facilitate patients and physicians in decision making, a comprehensive risk prediction model specifically developed for patients with DCIS would be desirable, including information on genetic, clinical, and lifestyle factors.
Methods
Study population
We evaluated 323,285 patients diagnosed with in situ or invasive first BC in 1989–2017, who underwent surgery, from the Netherlands Cancer Registry (NCR) (Supplementary Fig. 4). The NCR is an on-going nationwide population-based data registry of all newly diagnosed cancer patients in the Netherlands, with full coverage since 198932. We excluded nine patients with first diagnosis without cytological or histological confirmation, 5785 with stage IV BC or with incomplete staging information, 66 with squamous cell carcinoma, and 4145 with in situ BC that was not pure DCIS (i.e., lobular, other subtype, or mixed with ductal). Follow-up for all patients started 3 months after the first diagnosis; therefore, 9,441 patients who had developed synchronous CBC (invasive or in situ), invasive ipsilateral BC, or died within 3 months after the first diagnosis were excluded.
Patient and tumor characteristics
Clinico-pathological data were provided by the NCR. After notification by the nationwide network and registry of histo- and cytopathology in the Netherlands and the national hospital discharge database, registration clerks of the NCR collect data directly from patients’ records. Follow-up information on vital status and second cancers was complete up to 31 January 2018.
Staging was coded according to the TNM Classification of Malignant Tumors using the edition valid at the date of diagnosis, ranging from the 4th to the 8th edition33. If pathological stage was missing, clinical stage was used34.
Receptor status was determined by immunohistochemistry (IHC), and was included in the NCR since 2005. Tumors were defined as estrogen receptor (ER) positive or progesterone receptor (PR) positive when >10% of the tumor cells stained positive (from 2011 the threshold was ≥10%). A tumor was defined human epidermal growth factor receptor 2/neu-receptor (HER2) positive if IHC was 3+ (strong and complete membranous expression in >10% of tumor cells) or if IHC score 2+ when additional confirmation with in situ hybridization was available, but considered unknown if in situ hybridization confirmation was missing.
The NCR did not record information on BRCA1 and BRCA2 germline mutation status and family history.
From 2011, the NCR recorded the mode of first BC detection, i.e., if the DCIS or invasive BC was screen-detected or not detected by screening. We did not have detailed information available on the tumors not detected by screening, but these may include interval tumors, non-screen attendant, or screened outside the national program (e.g., owing to family history). According to the Dutch guidelines, mammographic follow-up is similar for DCIS and invasive BC24.
Data used in this study were included in the NCR under an opt-out regime according to Dutch legislation and codes of conduct34. The NCR Privacy Review Board approved this study under reference number K18.245. Data were handled in accordance with privacy regulations for medical research34.
Statistical analyses
The primary outcome was the development of metachronous CBC, defined as an invasive BC in the contralateral breast diagnosed at least three months after the first BC diagnosis (DCIS or invasive BC). Follow-up started three months after the first BC diagnosis, and ended at date of in situ- or invasive CBC, invasive ipsilateral BC, or last date of follow-up (owing to death, lost to follow-up, or end of study), whichever occurred first.
Cox proportional hazard models were performed to investigate the association of having DCIS compared with invasive BC as primary diagnosis with the cause-specific hazard of invasive CBC. We also performed analyses with in situ CBC, invasive ipsilateral BC, and death as the outcome. According to the Dutch guideline, DCIS patients do not receive adjuvant systemic therapy. We evaluated the impact of adjuvant systemic therapy by comparing the invasive CBC risk between DCIS patients and patients diagnosed with stage I BC not receiving adjuvant systemic therapy (no chemotherapy, endocrine therapy, nor trastuzumab), i.e., a subgroup of patients that resembles as much as possible the DCIS patient group in terms of treatment conditions. As hazard ratios (HRs) based on Cox regressions do not have a direct relationship with the cumulative incidence of the event of interest, we also performed competing risks regression to estimate the HRs for the subdistribution hazards of the Fine and Gray model35,36. In situ CBC, invasive ipsilateral BC, and death were considered as competing risks. We performed both univariable analyses and analyses adjusted for age- and year of first BC diagnosis. Since 1989, women in the Netherlands aged 50–70 have been invited for biannual screening by mammography, which was extended to women aged 75 since 1998. Based on this, we categorized age at first BC diagnosis into <50 years and ≥50 years. Based on the gradual implementation of the Dutch BC screening, we categorized year at first BC diagnosis into two periods: 1989–1998 (implementation phase) and 1999–2017 (full nationwide coverage; attendance rate is 78.8%37 and detection rate of invasive BC 6.6 per 1000 in 201738 and for DCIS 0.94 per 1000 between 2004–201139). We also performed our analyses stratified by mode of first BC detection. These analyses only included patients diagnosed during or after 2011 and aged 50–75 (eligible for screening).
Cumulative incidence curves of invasive CBC for DCIS patients, all invasive BC patients, and patients with stage I BC not receiving adjuvant systemic therapy were calculated considering in situ CBC, invasive ipsilateral BC, and death as competing risks. These curves were stratified by year of first BC diagnosis (1989–1998 and 1999–2017) and by age (<50 and ≥50 years).
We used joint Cox proportional hazard models40 to investigate subtype-specific CBC risk (according to stage, grade, ER, PR, and HER2 status) in DCIS patients compared with patients with invasive BC and compared with patients with stage I BC who did not receive adjuvant systemic therapy. Each model included subtype-specific CBC (e.g., ER-positive CBC, ER-negative CBC, ER unknown CBC), in situ CBC, ipsilateral invasive BC, and death as possible outcomes. As the NCR actively registered receptor status from 2005, these analyses only included patients diagnosed between 2005–2017.
Multivariable Cox regression was used to quantify the effect of clinico-pathological and treatment characteristics on CBC risk (all CBC and invasive CBC only) in DCIS patients. In addition, multivariable Fine and Gray regressions were performed to assess the association between every factor and the CBC cumulative incidence. Variables included in the models were age at first DCIS diagnosis, tumor grade, type of surgery (mastectomy or breast conserving surgery), and radiotherapy. The proportional hazard assumption of the models was assessed by examining the Schoenfeld residuals, and restricted cubic splines were used to verify whether linearity of age at first DCIS diagnosis would hold41. The discrimination ability of the models to identify patients developing CBC was calculated using the C-index42. Missing data were multiply imputed by chained equations to avoid loss of information owing to case-wise deletion causing bias and reduction in efficiency43,44. Multiple imputation accounts for missing data mechanisms assuming that the probability of missingness depends on the observed data namely missing at random. For every predictor with missing data, every imputation model selects predictors based on correlation structure underlying the data. Details about the imputation model are provided in Supplementary Methods.
Analyses were performed using STATA version 16.0, SAS (SAS Institute Inc., Cary, NC, USA) version 9.4, and R software version 3.5.345.
Reporting summary
Further information on research design is available in the Nature Research Reporting Summary linked to this article.
Data availability
The data sets generated and/or analyzed during the current study are not publicly available, as the study has used external data from the Netherlands Cancer Registry. The data sets will be made available from the Netherlands Cancer Registry upon reasonable request (data request study number K18.245). To apply for data access, please visit https://www.iknl.nl/en/ncr/apply-for-data. The data sets that support Figs. 1 and 2, and supplementary figs. 1–3, are publicly available in the figshare repository, in the following data record: https://doi.org/10.6084/m9.figshare.1298242423.
Code availability
The codes developed during this study are available upon reasonable request. Analyses were performed using STATA version 16.0, SAS (SAS Institute Inc., Cary, NC, USA) version 9.4, and R software version 3.5.3.
References
Evans, H. S. et al. Incidence of multiple primary cancers in a cohort of women diagnosed with breast cancer in southeast England. Br. J. Cancer 84, 435–440 (2001).
Soerjomataram, I. et al. Primary malignancy after primary female breast cancer in the South of the Netherlands, 1972-2001. Breast Cancer Res. Treat. 93, 91–95 (2005).
Brenner, H., Siegle, S., Stegmaier, C. & Ziegler, H. Second primary neoplasms following breast cancer in Saarland, Germany, 1968-1987. Eur. J. Cancer 29A, 1410–1414 (1993).
Portschy, P. R. et al. Perceptions of contralateral breast cancer risk: a prospective, longitudinal study. Ann. Surg. Oncol. 22, 3846–3852 (2015).
Hartman, M. et al. Genetic implications of bilateral breast cancer: a population based cohort study. Lancet Oncol. 6, 377–382 (2005).
Kramer, I. et al. The influence of adjuvant systemic regimens on contralateral breast cancer risk and receptor subtype. J. Natl. Cancer Inst. 111, 709–718 (2019).
Prater, J., Valeri, F., Korol, D., Rohrmann, S. & Dehler, S. Incidence of metachronous contralateral breast cancer in the Canton of Zurich: a population-based study of the cancer registry. J. Cancer Res. Clin. Oncol. 142, 365–371 (2016).
Nichols, H. B., Berrington de Gonzalez, A., Lacey, J. V. Jr., Rosenberg, P. S. & Anderson, W. F. Declining incidence of contralateral breast cancer in the United States from 1975 to 2006. J. Clin. Oncol. 29, 1564–1569 (2011).
Netherlands Cancer Registry (NCR). Survival and prevalence of cancer. https://www.cijfersoverkanker.nl (2016).
Ernster, V. L. et al. Detection of ductal carcinoma in situ in women undergoing screening mammography. J. Natl. Cancer Inst. 94, 1546–1554 (2002).
Elshof, L. E. et al. Subsequent risk of ipsilateral and contralateral invasive breast cancer after treatment for ductal carcinoma in situ: incidence and the effect of radiotherapy in a population-based cohort of 10,090 women. Breast Cancer Res. Treat. 159, 553–563 (2016).
Mariotti, C. Ductal Carcinoma in Situ of the Breast. Springer International Publishing (2018).
Miller, M. E. et al. Contralateral breast cancer risk in women with ductal carcinoma in situ: is it high enough to justify bilateral mastectomy? Ann. Surg. Oncol. 24, 2889–2897 (2017).
Tuttle, T. M. et al. Increasing rates of contralateral prophylactic mastectomy among patients with ductal carcinoma in situ. J. Clin. Oncol. 27, 1362–1367 (2009).
Falk, R. S., Hofvind, S., Skaane, P. & Haldorsen, T. Second events following ductal carcinoma in situ of the breast: a register-based cohort study. Breast Cancer Res. Treat. 129, 929–938 (2011).
Claus, E. B., Stowe, M., Carter, D. & Holford, T. The risk of a contralateral breast cancer among women diagnosed with ductal and lobular breast carcinoma in situ: data from the Connecticut Tumor Registry. Breast 12, 451–456 (2003).
Gao, X., Fisher, S. G. & Emami, B. Risk of second primary cancer in the contralateral breast in women treated for early-stage breast cancer: a population-based study. Int J. Radiat. Oncol. Biol. Phys. 56, 1038–1045 (2003).
Chowdhury, M., Euhus, D., Onega, T., Biswas, S. & Choudhary, P. K. A model for individualized risk prediction of contralateral breast cancer. Breast Cancer Res. Treat. 161, 153–160 (2017).
Chowdhury, M. et al. Validation of a personalized risk prediction model for contralateral breast cancer. Breast Cancer Res. Treat. 170, 415–423 (2018).
Akdeniz, D. et al. Risk factors for metachronous contralateral breast cancer: a systematic review and meta-analysis. Breast 44, 1–14 (2018).
Langballe, R. et al. Systemic therapy for breast cancer and risk of subsequent contralateral breast cancer in the WECARE Study. Breast Cancer Res. 18, 65 (2016).
Mook, S. et al. Independent prognostic value of screen detection in invasive breast cancer. J. Natl. Cancer Inst. 103, 585–597 (2011).
Giardiello, D. et al. Data and metadata supporting the published article: contralateral breast cancer risk in patients with ductal carcinoma in situ and invasive breast cancer. https://doi.org/10.6084/m9.figshare.12982424 (2020).
Oncoline. Borstkanker. Landelijke richtlijn, Versie: 2.0. https://www.oncoline.nl/ (Aug 2020 data last accessed).
van den Broek, A. J. et al. Impact of age at primary breast cancer on contralateral breast cancer risk in BRCA1/2 mutation carriers. J. Clin. Oncol. 34, 409–418 (2016).
Kuchenbaecker, K. B. et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA 317, 2402–2416 (2017).
Claus, E. B., Petruzella, S., Matloff, E. & Carter, D. Prevalence of BRCA1 and BRCA2 mutations in women diagnosed with ductal carcinoma in situ. JAMA 293, 964–969 (2005).
Thompson, D. & Easton, D. The genetic epidemiology of breast cancer genes. J. Mammary Gland Biol. Neoplasia 9, 221–236 (2004).
Murphy, J. A., Milner, T. D. & O’Donoghue, J. M. Contralateral risk-reducing mastectomy in sporadic breast cancer. Lancet Oncol. 14, e262–e269 (2013).
Basu, N. N., Ross, G. L., Evans, D. G. & Barr, L. The Manchester guidelines for contralateral risk-reducing mastectomy. World J. Surg. Oncol. 13, 237 (2015).
O’Donnell, M. Estimating contralateral breast cancer risk. Curr. Breast Cancer Rep. 10, 91–97 (2018).
Font-Gonzalez, A. et al. Inferior survival for young patients with contralateral compared to unilateral breast cancer: a nationwide population-based study in the Netherlands. Breast Cancer Res Treat. 139, 811–819 (2013).
Brierley, J. D., Gospodarowicz, M. K. & Wittekind, C. TNM classification of malignant tumours. 8th edn (Wiley-Blackwell, 2017).
Foundation Federation of Dutch Medical Scientific Societies. Human Tissue and Medical Research: Code of Conduct for responsible use (Federa, 2011).
Latouche, A., Allignol, A., Beyersmann, J., Labopin, M. & Fine, J. P. A competing risks analysis should report results on all cause-specific hazards and cumulative incidence functions. J. Clin. Epidemiol. 66, 648–653 (2013).
Van Der Pas, S., Nelissen, R. & Fiocco, M. Different competing risks models for different questions may give similar results in arthroplasty registers in the presence of few events. Acta Orthop. 89, 145–151 (2018).
RIVM. Breast Cancer screening program; facts and figures. https://www.rivm.nl/en/breast-cancer-screening-programme/background/facts-and-figures (May 2020, date last accessed).
IKNL. National evaluation of breast cancer screening in the Netherlands 2017/2018. https://www.iknl.nl/getmedia/8b019b63-0eb1-4afa-a824-31c4d10cc86e/Breast_cancer_screening_in_the_Netherlands_2017-2018_en.pdf (Aug 2020, date last accessed).
Sankatsing, V. D. V. et al. Detection and interval cancer rates during the transition from screen-film to digital mammography in population-based screening. BMC Cancer 18, 256 (2018).
Xue, X. et al. A comparison of the polytomous logistic regression and joint cox proportional hazards models for evaluating multiple disease subtypes in prospective cohort studies. Cancer Epidemiol. Biomark. Prev. 22, 275–285 (2013).
Harrell, F. E., Jr. Regression Modeling Strategies with applications to linear models, logistic and ordinal regression, and survival analysis. 2nd edn (Springer Series in Statistics, 2015).
Koziol, J. A. & Jia, Z. The concordance index C and the Mann-Whitney parameter Pr(X>Y) with randomly censored data. Biom. J. 51, 467–474 (2009).
Van Buuren, S. Flexible imputation of missing data. 2nd edn (Chapman and Hall/CRC, 2018).
Madley-Dowd, P., Hughes, R., Tilling, K. & Heron, J. The proportion of missing data should not be used to guide decisions on multiple imputation. J. Clin. Epidemiol. 110, 63–73 (2019).
R: A Language and Environment for Statistical Computing (R: Foundation for Statistical Computing, 2020).
Acknowledgements
The authors thank the registration team of the Netherlands Comprehensive Cancer Organization (IKNL) for the collection of data for the Netherlands Cancer Registry (NCR) as well as IKNL staff for scientific advice. We thank all patients whose data we used for this study and the clinicians who treated these patients. This work was supported by the Alpe d’HuZes/Dutch Cancer Society (KWF Kankerbestrijding) [grant number A6C/6253] and by Cancer Research UK/KWF Kankerbestrijding [grant numbers C38317, A24043]. The funders had no role in the design of the study, the statistical analyses, interpretation of the data, and writing of the manuscript.
Author information
Authors and Affiliations
Contributions
The data used for this study were derived from by the Netherlands Cancer Registry. M.K.S. designed the study; I.K. prepared and coded the data for analysis; D.G. performed the statistical analyses; I.K., D.G., M.K.S. interpreted the results and drafted the first version of the manuscript; all other authors contributed to the interpretation of the results and revisions of the manuscript. D.G. and I.K. shared co-first authorship. All authors approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Giardiello, D., Kramer, I., Hooning, M.J. et al. Contralateral breast cancer risk in patients with ductal carcinoma in situ and invasive breast cancer. npj Breast Cancer 6, 60 (2020). https://doi.org/10.1038/s41523-020-00202-8
Received:
Accepted:
Published:
DOI: https://doi.org/10.1038/s41523-020-00202-8
