
Abstract
The prognostic value of white-coat hypertension (WCH) remains controversial. We undertook a quantitative literature review to assess the risk of cardiovascular outcomes in untreated participants with WCH compared to that in participants with normotension. We searched databases (PubMed, Cochrane Library and the Ichu-Shi Web Japanese database) for peer-reviewed articles published until December 23, 2017 reporting studies evaluating the risk of cardiovascular outcomes in participants with WCH compared to that in participants with normotension. WCH was defined by having hypertension according to the conventional office blood pressure (BP) and being in the normotensive range (definitions of hypertension and normotension differed according to studies) for out-of-office BP measured at home or in an ambulatory setting. In total, 11 studies were included in the meta-analysis, which assessed the composite outcomes of morbidity and mortality on cardiovascular, stroke, and cardiac diseases, all-cause mortality, and deterioration to sustained hypertension in 8 (n = 11971), 2 (n = 6252), 2 (n = 6252), 5 (n = 10611), and 3 (n = 1722) studies, respectively. The risks for cardiovascular outcome and deterioration to sustained hypertension were significantly higher in WCH participants, with relative risks (95% confidence intervals) of 1.33 (1.10–1.62) and 2.85 (2.32–3.49), respectively, than in participants with normotension. In contrast, no significant differences were observed in the risk for stroke, cardiac outcomes or all-cause mortality. Our study suggests the importance of accurate and appropriate evaluation of WCH by utilizing out-of-office BP monitoring and the necessity for careful long-term follow-up of participants with WCH.
Similar content being viewed by others
Introduction
Recent hypertension guidelines have recommended that, in addition to conventional office blood pressure (BP), physicians should assess out-of-office BP, namely, ambulatory BP monitoring (ABPM) and home BP measurement (HBPM), for the diagnosis and management of hypertension [1,2,3,4]. Of importance, 15–30% of patients with an office BP of 140/90 mmHg or higher show normal readings when measured in an out-of-office setting [2]. This phenomenon of hypertension is known as white-coat hypertension (WCH) [5, 6], which refers to the untreated condition [4].
Office and out-of-office BP monitoring enables us to cross-classify normotension participants as nonhypertensive office and out-of-office BP, WCH as hypertensive office BP and nonhypertensive out-of-office BP, masked hypertension as nonhypertensive office BP and hypertensive out-of-office BP, and sustained hypertension as hypertensive office and out-of-office BP, respectively. Individuals with WCH have mild target organ damage and favorable cardiovascular outcomes compared to those with sustained hypertension [7,8,9,10,11,12]. Furthermore, several studies have reported that participants with WCH have a high potential for deteriorating to sustained hypertension, leading to poor cardiovascular outcomes in the future [13,14,15,16]. However, a previous meta-analysis evaluating the risk of cardiovascular disease in participants with WCH provided inconsistent findings [15, 17,18,19], and the prognosis of participants with WCH remains controversial. Therefore, we aimed to assess whether cardiovascular prognosis and risk for the development to sustained hypertension is poor in individuals with WCH compared to those in individuals with normotension.
Methods
Search strategy
We conducted a current systematic review and meta-analysis according to the Medical Information Network Distribution System (MINDS) manual for guideline development [20].
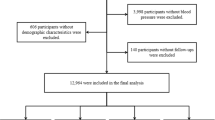
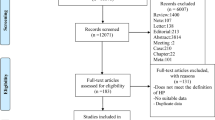
Relevant studies were identified by searching the PubMed, Cochrane Library and Ichu-Shi Web Japanese databases (until December 23, 2017), with language restriction to English or Japanese. We conducted the search strategy and searched the databases using MESH term (White Coat Hypertension [Mesh]) and relevant text words, including “white-coat hypertension” or “white coat effect” or “white coat blood pressure” or “white coat syndrome” or “clinic hypertension” or “clinic blood pressure” or “isolated office hypertension” or “isolated clinic hypertension,” as shown in Supplementary Table 1. The initial literature search identified 1404 articles (Fig. 1), which were screened for titles and abstracts by two authors (T.F. and C.M.; 1st screening). After eliminating 1033 irrelevant and 270 duplicate records, the two authors independently reviewed the screened 101 articles (2nd screening); disagreements were resolved by discussion between the two authors. After a full text review, 68 articles were excluded (44 irrelevant studies, 18 review articles, 3 letters, 2 editorial comments, 1 duplicate study), and 33 studies qualified for the current systematic review.

Flow chart of the process of publication selection
Eligibility for the meta-analysis
Although we performed our systematic literature search regardless of the use of antihypertensive medication, we included prospective cohort studies with participants without antihypertensive drug treatment at baseline for the current meta-analysis because WCH refers to the untreated condition [4, 21]. All eligible study participants were aged ≥ 18 years old, with information on the number of participants with WCH, normotension, and the number of outcome events or estimated risks for events associated with WCH compared to normotension. Studies whose enrollments depended on particular conditions, such as dialysis or pregnancy, were excluded. When studies reported the same outcomes from the same cohort, only the most recent article was included. The assessment of out-of-office BP values was based on either ABPM or HBPM.
According to the abovementioned eligibility criteria, all authors assessed the qualified 33 articles in detail, and 22 studies were further excluded for the meta-analysis (12, mixed population with treated and untreated participants; 1, enrollment depended on a particular condition; 3, duplicate cohort; 1, case-control study; 5, meta-analysis). Finally, the current meta-analysis was comprised of 11 full articles published in peer-reviewed journals (Fig. 1).
Study assessments
We abstracted data from each report, including author name, study design, sample size and characteristics of study participants, definition of WCH, definition of normotension, details of outcomes, and duration of follow-up period. When participants were classified as having both normotension and WCH on the basis of multiple definitions within one study, we extracted the most stringent definitions for WCH and normotension.
The outcome measures of this systemic review and meta-analysis are as follows.
Outcome 1: Onset of cardiovascular diseases (composite endpoints consisted of cardiac events and stroke) or death.
Outcome 2: Onset of stroke events or death.
Outcome 3: Onset of cardiac events or death.
Outcome 4: All-cause mortality.
Outcome 5: Deterioration to sustained hypertension.
Quality assessment on the risk of bias was undertaken in accordance with MINDS [20]. The risks of bias consisted of selection bias, performance bias, detection bias, and attribution bias. We evaluated each bias using the three grades of “not serious,” “serious,” and “very serious.”
Statistical analysis
We used generic inverse variance methods to perform the current meta-analysis. The estimated relative risk (RR) was used for the summary measures, and RR as odds ratios or hazard ratios with standard errors calculated by their 95% confidence intervals (CI) of the individual studies were directly entered into the analysis. We used random effects models because the true association was assumed to differ among studies, and statistical heterogeneity among studies was assessed by the chi-square test and statistic of inconsistency (I2) [22]. I2 values of 25, 50, and 75% were considered as low, moderate, and high heterogeneity, respectively. Significant heterogeneity was considered for P < 0.05 or I2 statistic > 25%. A funnel plot was used to examine whether there was a publication bias. Statistical significance was defined as P < 0.05 (two-tailed tests). All analyses were conducted by Review Manager (RevMan) version 5.3 (Nordic Cochrane Centre, The Cochrane Collaboration, 2012, Copenhagen, Denmark).
Ethics
As all data are publicly available; ethical approval was not necessary for the current systemic review and meta-analysis. The current study follows the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).
Results
At baseline, eight studies included only untreated participants [10, 11, 14, 16, 23,24,25,26], and three studies included untreated and treated groups; only the data on untreated participants were used for the current meta-analysis [12, 13, 27]. We summarized the characteristics of 11 studies in Table 1; all studies were observational studies, and none of the intervention trials were included.
Outcome 1: Onset of cardiovascular diseases or death
We included 8 studies in the meta-analysis for Outcome 1 [10,11,12, 23,24,25,26,27]. In total, 9274 participants with normotension and 2697 with WCH were included in the analysis. The follow-up period ranged from 3.2 years to 21 years. Among the included studies, three reported a higher risk of cardiovascular complications in participants with WCH than in those with normotension [12, 23, 25]. The risk for cardiovascular morbidity and mortality among participants with WCH was significantly higher than among those with normotension (RR 1.33, 95% CI: 1.10–1.62; Fig. 2). Low heterogeneity was observed among the included studies (I2 = 4%, P = 0.40).

Risk ratio and 95% confidence interval for the onset of cardiovascular diseases or death between participants with white-coat hypertension and normotension
The definitions of WCH and normotension differed among studies; in particular, three studies used unusual definitions for WCH and normotension [10, 23, 25]. The sensitivity analysis excluding these three studies [10, 23, 25] did not alter the results, with RR of 1.28 (95% CI: 1.06–1.53), and it still revealed significantly higher cardiovascular risk in WCH participants compared to normotension participants. Meanwhile, the definitions of “onset of cardiovascular disease or death” outcomes were also different; the outcomes of two studies [23, 25] and another five studies were cardiovascular disease mortality and composite of cardiovascular disease and death, respectively. The results of the subgroup analysis according to outcome (onset of cardiovascular morbidity or death) showed that participants with WCH had higher risks for both cardiovascular morbidity and cardiovascular death, with RR of 1.27 (95% CI, 1.06–1.53) and 4.72 (95% CI, 1.70–13.12), respectively.
Outcome 2: Onset of stroke events or death
We included 2 studies in the analysis for Outcome 2 [11, 24], consisting of 5135 participants with normotension and 1117 with WCH; both studies used ABPM for the diagnosis of WCH, and participants in the study by Asayama et al. [24]. came from 12 populations from 3 continents. Neither study included transient ischemic attack in the definition of stroke. The risk for stroke events and death tended to be higher in the participants with WCH than in those with normotension, but this was not statistically significant (RR 1.44, 95% CI 0.95–2.18; Fig. 3). Heterogeneity among the included studies was low (I2 = 0%, P = 0.41). However, the analysis was mainly weighted to the study by Asayama et al. [24], and further additional studies may be necessary to evaluate the risk of stroke in participants with WCH.

Risk ratio and 95% confidence interval for the onset of stroke events or death between participants with white-coat hypertension and normotension
Outcome 3: Onset of cardiac events or death
Similar to Outcome 2, we included 2 studies in the analysis for Outcome 3 [11, 24]. No significant differences were found in the risk for onset of cardiac events or death between the participants with WCH and those with normotension (RR 1.10, 95% CI 0.81–1.50; Fig. 4). Heterogeneity was not significant (I2 = 0% P = 0.56).

Risk ratio and 95% confidence interval for the onset of cardiac events or death between participants with white-coat hypertension and normotension
Outcome 4: All-cause mortality
We included 5 studies in the meta-analysis for Outcome 4 [11, 12, 23,24,25]. There were 8628 participants with normotension and 1983 participants with WCH, ranging from 3.5 to 21 years of follow-up. Among those, only Standberg et al. reported a significantly higher risk for all-cause mortality in participants with WCH compared to those with normotension [23], and no significant risk difference was found between the participants with WCH and those with normotension (RR 1.15, 95% CI 0.93–1.43), without significant heterogeneity (I2 = 32%, P = 0.21; Fig. 5). The sensitivity analysis excluding two studies [23, 25] in which unusual definitions for WCH and normotension were used did not alter the main analysis (RR 1.08, 95% CI, 0.89–1.24).

Risk ratio and 95% confidence interval for all-cause mortality between participants with white-coat hypertension and normotension
Outcome 5: Deterioration to sustained hypertension
We included 3 studies in the analysis for Outcome 5 [13, 14, 16]. Among 1369 normotension and 353 WCH participants, 245 and 141, respectively, developed sustained hypertension. The follow-up period varied from 1 to 11 years. All of the included studies similarly revealed (heterogeneity I2 = 0%, P = 0.81) that the risk for deterioration to sustained hypertension was significantly higher in the participants with WCH than in those with normotension (RR 2.85, 95% CI: 2.32–3.49; Fig. 6).

Risk ratio and 95% confidence interval for the deterioration to sustained hypertension between participants with white-coat hypertension and normotension
Assessment of risk of bias
In terms of performance bias, three studies were possibly affected by antihypertensive medications due to a lack of information on antihypertensive medications after the study enrollment [10] and prior history of use of antihypertensive medications for ≥ 14 days before study enrollment but not at baseline [11, 24]. No detection bias was observed in the included studies. Attribution bias was observed in two studies, which showed insufficient follow-up of study participants [13, 14]. Incomplete confounding adjustments were found in two studies [11, 12]. The number of participants with WCH was small [23], and the reported cardiovascular event rate was low [25]. When defining sustained hypertension, the use of antihypertensive medications was applied [14, 16]. Details for the risk of bias in each study are shown in Supplementary Table 2. We could not quantify the publication bias because of the small number of studies, while a funnel plot did not show evident asymmetry (Supplementary Figure 1).
Recent publication on white-coat hypertension
After the literature search of the present systematic review and meta-analysis was performed in December 2017, Banegas JR et al. reported that WCH was associated with a high risk for all-cause mortality and cardiovascular mortality [28]. We thus added the data from this new report to Outcome 1 and Outcome 4. The risk for onset of cardiovascular diseases or death in the participants with WCH remained significant (RR 1.44, 95% CI 1.16–1.77) without significant heterogeneity (I2 = 17% P = 0.29; Supplementary Figure 2); meanwhile, the participants with WCH showed a high risk for all-cause mortality compared to those with normotension (RR: 1.33, 95% CI: 1.01–1.76; P = 0.04), and the heterogeneity test became significant (I2 = 68% P = 0.007; Supplementary Figure 3).
Discussion
To the best of our knowledge, the present meta-analysis is the first to evaluate the risk of multiple cardiovascular outcomes in untreated participants with WCH compared to that in participants with normotension. We revealed that participants with WCH had a higher risk of developing sustained hypertension compared to those with normotension. Our results also showed that participants with WCH were associated with higher cardiovascular risk than those with normotension. For the risk of stroke, participants with WCH tended to have a higher risk compared to normotension, yet the result was not statistically significant. In contrast, the risks for cardiac events and all-cause mortality were not different between participants with WCH and those with normotension.
It is uncertain why participants with WCH had higher cardiovascular risk and tended to have higher risk for stroke than those with normotension. The development of sustained hypertension may lead to higher risk for cardiovascular complications later in participants with WCH, or participants with WCH may have other potential risk factors for cardiovascular disease. Notably, all the studies that reported significantly higher risk of cardiovascular complications in WCH participants compared to normotension participants had followed up participants for long periods (8.3 to 21 years) [12, 23, 25]. Therefore, we may need careful long-term follow-up for participants with WCH. Furthermore, some studies have suggested that participants with WCH with other cardiovascular risk factors, such as diabetes mellitus and chronic kidney disease, have higher risk of cardiovascular events than participants with normotension [29, 30]. These studies may indicate that especially careful follow-up of WCH participants with other cardiovascular risk factors is necessary.
We revealed that participants with WCH had a 2.8 times higher risk of developing sustained hypertension compared to normotension. All the included studies consistently showed significantly increased risk of developing sustained hypertension in WCH participants regardless of the follow-up period (1 to 16 years) [13, 14, 16]. Furthermore, when we look at the rate of progression to sustained hypertension of participants with WCH in long-term follow-up studies included in the current meta-analysis ( > 8 years), almost 50% of participants with WCH developed hypertension [14, 16]. Even though WCH has generally been considered a benign phenomenon, these results indicate that we should not consider WCH as such; rather, we need careful long-term follow-up of patients with WCH.
As for the assessment of WCH, we included studies using ABPM or HBPM for the diagnosis of WCH in the current meta-analysis. The majority of studies used ABPM to define WCH. However, Satoh et al. suggested that the risks of stroke were different according to either complete WCH (participants who met the criteria of WCH by using both ABPM and HBPM) or partial WCH (participants who met the criteria of WCH by using either ABPM or HBPM) [31]. Although difficult in clinical practice, evaluation based on both ABPM and HBPM for the definition of WCH may be necessary for accurate cardiovascular risk stratification.
The finding that the risk for all-cause mortality differed between the meta-analysis with and without the study by Banegas et al. requires careful interpretation [28]. First, the heterogeneity of this supplemental meta-analysis was strong (P = 0.007). Indeed, the estimate risks for all-cause mortality of WCH compared to those of normotension in the study by Banegas et al. were not consistent with those of other studies included in the meta-analysis, and heterogeneity was not observed among studies without Banegas et al. (P = 0.21). Furthermore, the study population was somewhat biased with the nature of participants due to the study design, as participants met guidelines recommended for ABPM, e.g., 25.8% of the 25672 untreated participants had WCH, while only 8.9% had masked hypertension [32]. Further investigations to clarify the risk of all-cause mortality for participants with WCH compared to normotension are needed.
Several limitations of the current review should be considered. First, the definitions of WCH and normotension varied among the included studies. The methods used to evaluate office BP and out-of-office BP (ABPM or HBPM) were not consistent among studies. Patients who showed a WCH profile based on their BP but were under antihypertensive medication treatment were classified into sustained hypertension, and the risk of WCH might be therefore have been underestimated [14]. Furthermore, none of the included studies used the definitions of WCH and normotension based on the latest hypertension guidelines suggested by the American Heart Association in 2017 [33]. Second, the definitions of each outcome were different among studies. Some studies included soft endpoints for the definitions of cardiovascular disease, such as coronary revascularization, heart failure, peripheral revascularization, renal event, and transient ischemic attack [10,11,12, 26]. Third, the majority of studies did not consider the use of antihypertensive medication during the follow-up period. Regarding the fact that participants with WCH have a higher risk of developing sustained hypertension, some participants with WCH who developed sustained hypertension during the follow-up period may have used antihypertensive medication, which could modify the cardiovascular risk in participants with WCH at baseline. Finally, all of the included studies were observational, and we could not evaluate whether the treatment intervention for participants with WCH prevented the development of cardiovascular complications.
In conclusion, the present systematic review and meta-analysis suggests that the risks of cardiovascular morbidity and mortality, as well as development of sustained hypertension, are higher in participants with WCH than in participants with normotension. Appropriate and accurate evaluation of BP based on office and out-of-office measurements is necessary for risk stratification in individuals, and an attentive long-term follow-up of participants with WCH is warranted.
References
National Clinical Guideline Centre (UK).London: Royal College of Physicians (UK); Hypertension: the clinical management of primary hypertension in adults. Update of clinical guidelines 18 and 34. NICE clinical guideline No. 127. 2011. Accessed on January 2018. http://guidance.nice.org.uk/CG127.
Shimamoto K, Ando K, Fujita T, Hasebe N, Higaki J, Horiuchi M, et al. Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension. The Japanese Society of Hypertension Guidelines for the management of hypertension (JSH 2014). Hypertens Res. 2014;37:253–390.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:1269–324.
Williams B, Mancia G, Spiering W, Agabiti Rosei E, Azizi M, Burnier M, et al. 2018 ESC/ESH Guidelines for the management of arterial hypertension. Eur Heart J. 2018;39:3021–104.
Pickering TG, James GD, Boddie C, Harshfield GA, Blank S, Laragh JH. How common is white coat hypertension? JAMA. 1988;259:225–8.
Verdecchia P, Schillaci G, Borgioni C, Ciucci A, Porcellati C. White-coat hypertension. Lancet. 1996;348:1444–5.
Ohkubo T, Kikuya M, Metoki H, Asayama K, Obara T, Hashimoto J, et al. Prognosis of “masked” hypertension and “white-coat” hypertension detected by 24-h ambulatory blood pressure monitoring 10-year follow-up from the Ohasama study. J Am Coll Cardiol. 2005;46:508–15.
Pierdomenico SD, Cuccurullo F. Prognostic value of white-coat and masked hypertension diagnosed by ambulatory monitoring in initially untreated subjects: an updated meta analysis. Am J Hypertens. 2011;24:52–8.
Tientcheu D, Ayers C, Das SR, McGuire DK, de Lemos JA, Khera A, et al. Target Organ Complications and Cardiovascular Events Associated With Masked Hypertension and White-Coat Hypertension: Analysis From the Dallas Heart Study. J Am Coll Cardiol. 2015;66:2159–69.
Verdecchia P, Porcellati C, Schillaci G, Borgioni C, Ciucci A, Battistelli M, et al. Ambulatory blood pressure. An independent predictor of prognosis in essential hypertension. Hypertension. 1994;24:793–801.
Kario K, Shimada K, Schwartz JE, Matsuo T, Hoshide S, Pickering TG. Silent and clinically overt stroke in older Japanese subjects with white-coat and sustained hypertension. J Am Coll Cardiol. 2001;38:238–45.
Stergiou GS, Asayama K, Thijs L, Kollias A, Niiranen TJ, Hozawa A, et al. International Database on HOme blood pressure in relation to Cardiovascular Outcome (IDHOCO) Investigators. Prognosis of white-coat and masked hypertension: International Database of HOme blood pressure in relation to Cardiovascular Outcome. Hypertension. 2014;63:675–82.
Cacciolati C, Hanon O, Dufouil C, Alperovitch A, Tzourio C. Categories of hypertension in the elderly and their 1-year evolution. The Three-City Study. J Hypertens. 2013;31:680–9.
Siven SS, Niiranen TJ, Kantola IM, Jula AM. White-coat and masked hypertension as risk factors for progression to sustained hypertension: the Finn-Home study. J Hypertens. 2016;34:54–60.
Briasoulis A, Androulakis E, Palla M, Papageorgiou N, Tousoulis D. White-coat hypertension and cardiovascular events: a meta-analysis. J Hypertens. 2016;34:593–9.
Ugajin T, Hozawa A, Ohkubo T, Asayama K, Kikuya M, Obara T, et al. White-coat hypertension as a risk factor for the development of home hypertension: the Ohasama study. Arch Intern Med. 2005;165:1541–6.
Fagard RH, Comelissen VA. Incidence of cardiovascular events in white-coat, masked and sustained hypertension versus true normotension: a meta-analysis. J Hypertens. 2007;25:2193–8.
Huang Y, Huang W, Mai W, Cai X, An D, Liu Z, et al. White-coat hypertension is a risk factor for cardiovascular diseases and total mortality. J Hypertens. 2017;35:677–88.
Muntner P, Booth JN 3rd, Shimbo D, Schwartz JE. Is white-coat hypertension associated with increased cardiovascular and mortality risk? J Hypertens. 2016;34:1655–8.
Kojimahara N, Nakayama T, Morizane T, Yamaguchi N, Yoshida M. Minds manual for guideline development. Ver.2.0. Tokyo, Japan: Council for Quality Health Care. 2016.
Franklin SS, Thijs L, Hansen TW, O’Brien E and Staessen JA. White-coat hypertension: new insights from recent studies. Hypertens (Dallas, Tex: 1979). 2013;62:982–7.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Strandberg TE and Salomaa V. White coat effect, blood pressure and mortality in men: prospective cohort study. Eur Heart J. 2000;21:1714–8.
Asayama K, Thijs L, Li Y, Gu YM, Hara A, Liu YP, et al. Setting thresholds to varying blood pressure monitoring intervals differentially affects risk estimates associated with white-coat and masked hypertension in the population. Hypertension. 2014;64:935–42.
Sung SH, Cheng HM, Wang KL, Yu WC, Chuang SY, Ting CT, et al. White coat hypertension is more risky than prehypertension: important role of arterial wave reflections. Hypertension. 2013;61:1346–53.
Pierdomenico SD, Lapenna D, Di Mascio R, Cuccurullo F. Short- and long-term risk of cardiovascular events in white-coat hypertension. J Hum Hypertens. 2008;22:408–14.
Fagard RH, Van Den Broeke C, De Cort P. Prognostic significance of blood pressure measured in the office, at home and during ambulatory monitoring in older patients in general practice. J Hum Hypertens. 2005;19:801–7.
Banegas JR, Ruilope LM, de la Sierra A, Vinyoles E, Gorostidi M, de la Cruz JJ, et al. Relationship between clinic and ambulatory blood-pressure measurements and mortality. N Eng J Med. 2018;378:1509–20.
Franklin SS, Thijs L, Asayama K, Li Y, Hansen TW, Boggia J, et al. The cardiovascular risk of white-coat hypertension. J Am Coll Cardiol. 2016;68:2033–43.
Kushiro T, Kario K, Saito I, Teramukai S, Sato Y, Okuda Y, et al. Increased cardiovascular risk of treated white coat and masked hypertension in patients with diabetes and chronic kidney disease: the HONEST Study. Hypertens Res. 2017;40:87–95.
Satoh M, Asayama K, Kikuya M, Inoue R, Metoki H, Hosaka M, et al. Long-term stroke risk due to partial white-coat or masked hypertension based on home and ambulatory blood pressure measurements: the ohasama Study. Hypertension. 2016;67:48–55.
Bursztyn M and Asayama K. Twenty-four-hour ambulatory systolic blood pressure may be a better predictor of all-cause and cardiovascular mortality than clinic blood pressure. BMJ Evid Based Med. 2018. https://doi.org/10.1136/bmjebm-2018-111051.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr., Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:e13–115.
Acknowledgements
We thank Dr. Satoshi Umemura, Dr. Hisatomi Arima, and committee members of the JSH 2019 guidelines.
Author contributions
TF and CM wrote the first draft of this manuscript, and both authors contributed equally to this work. All authors conducted this study and commented on the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Fujiwara, T., Matsumoto, C., Asayama, K. et al. Are the cardiovascular outcomes of participants with white-coat hypertension poor compared to those of participants with normotension? A systemic review and meta-analysis. Hypertens Res 42, 825–833 (2019). https://doi.org/10.1038/s41440-019-0254-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-019-0254-2
Keywords
This article is cited by
-
Improving measurement accuracy and feasibility to support long-term blood pressure management
Hypertension Research (2022)
-
Effects of white-coat, masked and sustained hypertension on coronary artery stenosis and cardiac arrhythmia
Hypertension Research (2020)
-
White-coat and masked hypertension and coronary artery disease: are they related or not?
Hypertension Research (2020)
-
Impact of hypertension phenotypes on the office and 24-h pulse wave velocity and augmentation index in individuals with or without antihypertensive medication use
Hypertension Research (2019)
-
Resistant Hypertension Updated Guidelines
Current Cardiology Reports (2019)
