
Abstract
The target of diastolic blood pressure (DBP) remains controversial in patients with coronary artery disease (CAD). We systematically searched PubMed/Medline and the Cochrane Central database for randomized controlled trials (RCTs) assessing the efficacy and safety of reducing DBP in CAD patients from January 1965 to July 2017. Seven placebo-controlled RCTs enrolling 34,814 CAD patients who achieved DBP <80 mmHg were included in the drug-intervention group. The average achieved blood pressures (BPs) were 126.3/75.1 and 131.5/77.8 mmHg in the drug-intervention and placebo-control groups, respectively. Drug intervention was associated with an 11% reduction in coronary revascularization and a 31% reduction in heart failure. In the drug-intervention group, all-cause death, myocardial infarction, angina pectoris, and stroke were reduced with marginal significance, whereas hypotension was increased by 123%. A meta-analysis of four RCTs, in which the achieved DBP was <75 mmHg, showed that the drug intervention was associated with a 22% reduction in heart failure. These results suggest that reducing DBP to 80 mmHg or less would significantly reduce coronary revascularization and heart failure but at the expense of causing hypotension in CAD patients. Further trials are warranted to prove this issue.
Similar content being viewed by others


Introduction
It has been well established that reducing blood pressure (BP) can prevent cardiovascular events and death. A meta-analysis of 61 prospective observational studies showed that BP was strongly and log-linearly associated with cardiovascular mortality down to 115/75 mmHg [1]. In Japanese people, BP is related to the cumulative incidence of myocardial infarction down to 120/70 mmHg [2]. Importantly, BP reduction is associated with a reduced risk of cardiovascular events irrespective of the class of antihypertensive drugs used, including angiotensin converting enzyme (ACE) inhibitors, calcium-channel blockers, diuretics, and β-blockers [3]. Thus, it is suggested that BP lowering per se is important for preventing cardiovascular events.
Current Japanese guidelines for hypertension management (JSH2014) recommend a BP target of <140/90 mmHg in patients with coronary artery disease (CAD) and <130/80 mmHg in high-risk CAD patients if tolerable [4]. However, previous American and European hypertension guidelines have recommended a target of <140/90 mmHg for patients with CAD [5, 6] because of a J-curve phenomenon; namely, a nonlinear relationship exists between BP and adverse outcomes with higher event rates at both very-low and very-high BP [7, 8]. An observational study enrolling CAD patients showed that a systolic BP (SBP) of less than 120 mmHg and a diastolic BP (DBP) of less than 70 mmHg were associated with an increased risk of cardiovascular disease [9]. An additional analysis of the Systolic Blood Pressure Intervention Trial demonstrated the presence of a J curve for DBP with a nadir of approximately 70 mmHg based on the automated office BP measurement in hypertensive patients with or without cardiovascular disease; however, there was no J curve for SBP [10].
The most recent 2017 ACC/AHA guidelines have lowered the BP target for CAD patients from 140/90 to 130/80 mmHg [11]. The following two studies may have an impact on the lowering of the SBP target: first, the Systolic Blood Pressure Intervention Trial using the automated office BP measurement showed that intensive SBP reduction targeting 120 mmHg significantly reduced not only the composite of myocardial infarction, other acute coronary syndromes, stroke, heart failure, and death from cardiovascular causes but also all-cause mortality, when compared with the standard SBP reduction targeting 140 mmHg in patients with clinical/subclinical cardiovascular diseases other than stroke and in patients at a high risk for cardiovascular disease but without diabetes [12]. Second, a large-scale meta-analysis enrolling 66,504 CAD patients demonstrated that an SBP reduction achieving SBP ≤ 130 mmHg was associated with greater reductions in heart failure and stroke without the increase in all-cause death and cardiovascular death, when compared with the standard SBP reduction of SBP 136–140 mmHg [13]. However, only a few consistent data are available regarding DBP targets based on randomized clinical trials (RCTs) in patients with CAD. Accordingly, we conducted searches of previous trials and performed a systematic review and meta-analysis assessing the efficacy and safety of reducing DBP to <80 mmHg in CAD patients.
Methods
Eligibility criteria
This systematic review and meta-analysis was conducted according to the PRISMA statement [14]. We conducted a systematic search of MEDLINE and the Cochrane Central Register of Controlled Trials (CENTRAL) from 1965 to July 2017 using medical subject headings and relevant text words for CAD and those for BP or DBP. The search criteria were fairly broad to avoid missing studies through a restricted search. We also checked the reference lists of the original studies, meta-analyses, and review articles that were identified by the electronic searches to find other eligible trials. There was no language restriction placed on the search.
This analysis included RCTs conducted among patients with CAD (excluding the acute phase of myocardial infarction or heart failure) that [1] randomized patients to antihypertensive drug or placebo arms; [2] reported long-term survival or cardiovascular outcomes for at least 1 year; [3] enrolled at least 500 patients to avoid bias associated with small trials; [4] attained a DBP of <80 mmHg in the drug-intervention group. Studies reporting no significant difference in DBP between the two groups were excluded.
Data extraction, synthesis, and analysis
Long-term efficacy and safety outcomes were evaluated. The efficacy outcomes were the following: all-cause mortality, cardiovascular mortality, myocardial infarction, angina pectoris, revascularization, stroke, and heart failure. The safety outcome evaluated was hypotension, as reported, and compared between the two groups. For data synthesis and analysis, we used the Cochrane Review Manager software, Review Manager version 5.3 (RevMan 5.3) (Nordic Cochrane Center, Copenhagen, Denmark).
Assessment of risk of bias in the included studies
Two review authors (RO and EK) independently assessed trial eligibility and trial-bias risk and extracted data. Disagreements were resolved by consensus. The bias risk of the trials was assessed using the six domains of the ‘Risk of bias’ tool according to the method described in the Cochrane Handbook ‘Assessing Risk of Bias in Included Studies’ (http://methods.cochrane.org/bias/assessing-risk-bias-included-studies. Accessed July 11, 2017).
Statistical analysis
Risk ratios (RRs) and 95% confidence intervals (CIs) were estimated for each trial and each outcome. Random-effects models were used to pool RRs and 95% CI for study outcomes. We used the Cochrane chi-squared test and I2 statistics to test the heterogeneity across the trials [15]. A chi-square value of less than 0.05 or an I2 value greater than 50% was regarded as indicating high heterogeneity. Publication bias was assessed using funnel plots. Statistical analysis was performed using RevMan 5.3.
Role of funding source
This study was not funded; hence, no funding source played any role in study design; collection, analysis, and interpretation of the data; or writing the paper.
Results
Trial selection and study characteristics
We identified seven RCTs that fulfilled the inclusion criteria (Fig. 1) [16,17,18,19,20,21,22]. The characteristics of included trials are summarized in Table 1. The drug-intervention group and the placebo-control group included 17,434 and 16,725 patients, respectively. Achieved BPs were 126.3/75.1and 131.5/77.8 mmHg in the drug-intervention and placebo-control groups, respectively. Of note, none of the trials were designed to assign patients to different target levels of SBP or DBP (e.g., DBP less than 80 mmHg). A summary of the risk of bias assessment of each trial is shown in Fig. 4. All seven RCTs were considered to have a low risk of bias.

Study selection. CAD coronary artery disease, DBP diastolic blood pressure, MeSH medical subject heading, PT publication type
Efficacy outcomes
The drug-intervention group with an achieved DBP < 80 mmHg tended to have lower all-cause death (RR 0.94, 95% CI 0.86–1.02, P = 0.12; Fig. 2a), myocardial infarction (RR 0.87, 95% CI 0.74–1.03, P = 0.10; Fig. 2c), angina pectoris (RR 0.88, 95% CI 0.76–1.02, P = 0.08; Fig. 2d), and stroke (RR 0.87, 95% CI 0.73–1.06, P = 0.16; Fig. 2f) when compared with the placebo group, although the differences were not significant. No significant effect was found when comparing cardiovascular death in the drug-intervention group with that in the placebo group (Fig. 2b). However, the intervention group was associated with a significant (11%) reduction in coronary revascularization (Fig. 2e) and a 31% reduction in heart failure (Fig. 2g). There was a low level of heterogeneity for the effects of the intervention across eligible trials for all-cause death, cardiovascular death, stroke, and heart failure; a modest level of heterogeneity for angina pectoris; and a high level of heterogeneity for myocardial infarction (I2 = 56%; Fig. 2c) and revascularization (I2 = 66%; Fig. 2e). There was no clear evidence of publication bias (Supplementary Figure 1).


Intervention (DBP < 80 mmHg) vs placebo diastolic blood pressure control and outcome. a Total death. b Cardiovascular death. c Myocardial infarction. d Angina pectoris. e Coronary revascularization. f Stroke. g Heart failure. h Hypotension. The size of the data markers represents the weight of each trial. CI confidence interval, df degrees of freedom, I2 inconsistency, IV inverse variance
Next, we performed an additional meta-analysis of four RCTs, CAMELOT-E [17], IMAGINE [19], PART-2 [20], and PEACE [21], in which a DBP of <75 mmHg was attained in the drug-intervention group. When the achieved DBP was <75 mmHg, the drug intervention was associated with a 22% reduction in heart failure when compared with the placebo group (Fig. 3g). There was no heterogeneity for the outcome of heart failure (I2 = 0%; Fig. 3g). In the drug-intervention group, a trend towards reduced all-cause death was observed (Fig. 3a), but there were no significant reductions in cardiovascular death, myocardial infarction, angina pectoris, revascularization, and stroke (Fig. 3b–f). There was no clear evidence of publication bias (Supplementary Figure 2).


Intervention (DBP < 75 mmHg) vs placebo diastolic blood pressure control and outcome. a Total death. b Cardiovascular death. c Myocardial infarction. d Angina pectoris. e Coronary revascularization. f Stroke. g Heart failure. The size of the data markers represents the weight of each trial. CI confidence interval, df degrees of freedom, I2 inconsistency, IV inverse variance
Safety outcome
The drug-intervention group with an achieved DBP of 80 mmHg or less was associated with a 123% increase in hypotension rate (Fig. 2h) when compared with the placebo-control group. There was high heterogeneity in the analysis (I2 = 73%; Fig. 2h), but bias was insignificant (Fig. 4 and Supplementary Tables 1–15).

Risk of bias summary: the review author’s assessment of each risk of bias item for each included study
Discussion
The principal finding of the present study is that the achievement of a DBP of <80 mmHg in the drug-intervention group is associated with a significant reduction in coronary revascularization and heart failure but does not increase all-cause death and cardiovascular death when the achieved SBP is ≤130 mmHg.
A systematic review of the effects of reducing SBP was conducted by Bangalore et al. including 15 RCTs involving CAD patients not having heart failure and acute myocardial infarction, who were randomized to antihypertensive drugs or placebo [13]. The intensive SBP reduction with an achieved SBP of 131–135 mmHg was associated with a 15% decrease in heart failure and a 10% decrease in stroke but at the expense of hypotension, when compared with the standard SBP reduction with an achieved SBP of 136–140 mmHg. Moreover, a more intensive SBP reduction achieving an SBP of ≤130 mmHg was associated with greater reductions in heart failure and stroke (27 and 17%, respectively) as well as borderline reductions in myocardial infarction and angina pectoris, when compared with the standard SBP reduction, while not affecting all-cause death and cardiovascular death. These findings might provide a rationale supporting the setting of an SBP target in CAD patients down to <130 mmHg in the recent 2017 ACC/AHA guidelines [11]. However, this systematic review did not mention the effects of the achieved DBP ranges on the outcomes.
Because the RCTs, which investigated the effects of the achieved DBP ranges on the outcomes, were not found using a systematic search, we performed a systematic review of RCTs examining the effects of reducing DBP in CAD patients who were randomized to antihypertensive drugs or placebo. Of note, all seven RCTs we included in our study are included in the meta-analysis by Bangalore et al., as mentioned above [13]. Indeed, the achieved SBP was 126.3 mmHg in the drug-intervention group and 131.5 mmHg in the placebo-control group in our study (Table 1). Our meta-analysis showed that the achievement of a DBP < 80 mmHg was associated with an 11% reduction in coronary revascularization and a 31% reduction in heart failure (Fig. 2). We could not perform a meta-analysis of the effects on renal failure because only the EUROPA trial reported the incidence of renal failure among seven RCTs [18]. An intervention group with a DBP < 75 mmHg, including the four RCTs of CAMELOT-E [17], IMAGINE [19], PART-2 [20] and PEACE [21], was associated with a 22% reduction in heart failure and no increase in total death, cardiovascular death, myocardial infarction, revascularization, or stroke (Fig. 3). Thus, it is important to note that controlling DBP to less than 80 or even 75 mmHg can prevent heart failure in patients with CAD.
The identified seven RCTs (DBP < 80 mmHg) used calcium-channel blockers and ACE inhibitors in the intervention group, and only ACE inhibitors were used in the four intensive RCTs (DBP < 75 mmHg). This fact might be interesting given that calcium-channel blockers directly dilate the coronary artery while ACE inhibitors can improve autoregulation in the coronary artery [23].
The J-curve phenomenon has been reported, especially in post-hoc analysis and observational studies. Coronary revascularization reduced the rate of primary outcome (all-cause death, nonfatal myocardial infarction or nonfatal stroke) by half in the group achieving DBP < 60 mmHg in the INVEST study [24]. Another post-hoc analysis of the INVEST trial showed that the relation between cardiovascular outcome and DBP was linear in patients with CAD and revascularization by coronary artery bypass grafting (CABG), and the lowest event rates were observed in patients with a DBP of 125/55 mmHg [25]. The authors concluded that a more complete revascularization can attenuate hypoperfusion at a low DBP [25]. Therefore, it seems that severe coronary lesions, which need revascularization, contribute to the increased rate of primary outcome at a low DBP. After total coronary revascularization, there is no reason to hesitate to decrease DBP down to 80 mmHg. Indeed, in the Japan CREDO-Kyoto registry, a DBP ≤ 70 mmHg was not found to be an independent risk factor for cardiovascular death in patients with CAD after revascularization [26]. A higher event rate was not observed in patients older than 75 years, even in those with a DBP < 60 mmHg [27]. Importantly, no RCT has been performed that enables us to evaluate the effect of a DBP less than 70 mmHg in CAD patients. Further RCT studies targeting a DBP less than 70 mmHg are necessary.
Study limitations
None of the trials were designed to compare different DBP target levels. In seven RCTs, calcium antagonists and ACE inhibitors were used. Interestingly, only ACE inhibitors were used in trials that achieved DBP levels <75 mmHg in the intervention group. Thus, we could not compare differences relating to the types of antihypertensive agents used in this meta-analysis.
Conclusions
The present study showed that the achievement of a DBP < 80 mmHg significantly reduces coronary revascularization and heart failure but at the expense of causing hypotension in CAD patients with an achieved SBP < 130 mmHg. We should not hesitate to target SBP down to 130 mmHg in patients with CAD when we observe DBP values of down to 80 mmHg, which are tolerable. Our results can support the targeted DBP of 90 to 80 mmHg, which has been set in the newly published US guidelines [11].
References
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2002;360:1903–13.
Wakugami K, Iseki K, Kimura Y, Okumura K, Ikemiya Y, Muratani H, et al. Relationship between serum cholesterol and the risk of acute myocardial infarction in a screened cohort in Okinawa, Japan. Jpn Circ J. 1998;62:7–14.
Turnbull F. Effects of different blood-pressure-lowering regimens on major cardiovascular events: results of prospectively-designed overviews of randomised trials. Lancet. 2003;362:1527–35.
Shimamoto K, Ando K, Fujita T, Hasebe N, Higaki J, Horiuchi M, Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension. et al. The Japanese Society of Hypertension Guidelines for the management of hypertension (JSH 2014). Hypertens Res. 2014;37:253–390.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, et al. 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA. 2014;311:507–20.
Mancia G, Fagard R, Narkiewicz K, Redon J, Zanchetti A, Böhm M, et al. 2013 ESH/ESC guidelines for the management of arterial hypertension: the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension (ESH) and of the European Society of Cardiology (ESC). Eur Heart J. 2013;34:2159–219.
Kang YY, Wang JG. The J-curve phenomenon in hypertension. Pulse (Basel). 2016;4:49–60.
Tanna MS, Bangalore S. Antihypertensive therapy and the J-curve: fact or fiction? Curr Hypertens Rep. 2015;17:6.
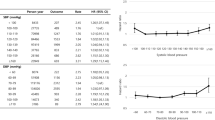
Vidal-Petiot E, Ford I, Greenlaw N, Ferrari R, Fox KM, Tardif JC, CLARIFY Investigators. et al. Cardiovascular event rates and mortality according to achieved systolic and diastolic blood pressure in patients with stable coronary artery disease: an international cohort study. Lancet. 2016;388:2142–52.
Khan NA, Rabkin SW, Zhao Y, McAlister FA, Park JE, Guan M, et al. Effect of lowering diastolic pressure in patients with and without cardiovascular disease: analysis of the SPRINT (Systolic Blood Pressure Intervention Trial). Hypertension. 2018;71:840–7.
Whelton PK, Carey RM, Aronow WS, Casey DE Jr, Collins KJ, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:1269–324.
SPRINT Research Group, Wright JT Jr., Williamson JD, Whelton PK, Snyder JK, Sink KM, Rocco MV, et al. A randomized trial of intensive versus standard blood-pressure control. N Engl J Med. 2015;373:2103–16.
Bangalore S, Kumar S, Volodarskiy A, Messerli FH. Blood pressure targets in patients with coronary artery disease: observations from traditional and Bayesian random effects meta-analysis of randomised trials. Heart. 2013;99:601–13.
Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339:b2535.
Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ. 2003;327:557–60.
Poole-Wilson PA, Lubsen J, Kirwan BA, van Dalen FJ, Wagener G, Danchin N, Coronary disease Trial Investigating Outcome with Nifedipine gastrointestinal therapeutic system investigators. et al. Effect of long-acting nifedipine on mortality and cardiovascular morbidity in patients with stable angina requiring treatment (ACTION trial): randomised controlled trial. Lancet. 2004;364:849–57.
Nissen SE, Tuzcu EM, Libby P, Thompson PD, Ghali M, Garza D, CAMELOT Investigators. et al. Effect of antihypertensive agents on cardiovascular events in patients with coronary disease and normal blood pressure: the CAMELOT study: a randomized controlled trial. JAMA. 2004;292:2217–25.
Fox KM. Efficacy of perindopril in reduction of cardiovascular events among patients with stable coronary artery disease: randomised, double-blind, placebo-controlled, multicentre trial (the EUROPA study). Lancet. 2003;362:782–8.
Rouleau JL, Warnica WJ, Baillot R, Block PJ, Chocron S, Johnstone D, IMAGINE (Ischemia Management with Accupril post-bypass Graft via Inhibition of the coNverting Enzyme) Investigators. et al. Effects of angiotensin-converting enzyme inhibition in low-risk patients early after coronary artery bypass surgery. Circulation. 2008;117:24–31.
MacMahon S, Sharpe N, Gamble G, Clague A, Mhurchu CN, Clark T, et al. Randomized, placebo-controlled trial of the angiotensin-converting enzyme inhibitor, ramipril, in patients with coronary or other occlusive arterial disease. PART-2 Collaborative Research Group. Prevention of Atherosclerosis with Ramipril. J Am Coll Cardiol. 2000;36:438–43.
Braunwald E, Domanski MJ, Fowler SE, Geller NL, Gersh BJ, Hsia J, PEACE Trial Investigators. et al. Angiotensin-converting-enzyme inhibition in stable coronary artery disease. N Engl J Med. 2004;351:2058–68.
Pitt B, Byington RP, Furberg CD, Hunninghake DB, Mancini GB, Miller ME, et al. Effect of amlodipine on the progression of atherosclerosis and the occurrence of clinical events. PREVENT Investigators. Circulation. 2000;102:1503–10.
Rouleau JR, Simard D, Blouin A, Kingma JG Jr. Angiotensin inhibition and coronary autoregulation in a canine model of LV hypertrophy. Basic Res Cardiol. 2002;97:384–91.
Messerli FH, Mancia G, Conti CR, Hewkin AC, Kupfer S, Champion A, et al. Dogma disputed: can aggressively lowering blood pressure in hypertensive patients with coronary artery disease be dangerous? Ann Intern Med. 2006;144:884–93.
Denardo SJ, Gong Y, Nichols WW, Hewkin AC, Kupfer S, Champion A, et al. Blood pressure and outcomes in very old hypertensive coronary artery disease patients: an INVEST substudy. Am J Med. 2010;123:719–26.
Kai H, Ueno T, Kimura T, Adachi H, Furukawa Y, Kita T, Imaizumi T, CREDO-Kyoto Investigators. Low DBP may not be an independent risk for cardiovascular death in revascularized coronary artery disease patients. J Hypertens. 2011;29:1889–96.
Kai H, Kimura T, Fukuda K, Fukumoto Y, Kakuma T, Furukawa Y. Impact of low diastolic blood pressure on risk of cardiovascular death in elderly patients with coronary artery disease after revascularization–The CREDO-Kyoto Registry Cohort-1. Circ J. 2016;80:1232–41.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The Department of Cardiology and Nephrology, Mie University Graduate School of Medicine, received research grants from Bristol-Myers Squibb, MSD K.K., Pfizer Japan Inc., Takeda Pharmaceutical Co., Ltd., Astellas Pharma Inc., Daiichi Sankyo Pharmaceutical Co., Ltd., Genzyme Japan, Shionogi & Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., Mitsubishi Tanabe Corporation, Otsuka Pharmaceutical Co., Ltd., Bayer Yakuhin, Ltd., AstraZeneca K.K., and Boehringer Ingelheim Co., Ltd. Rei Shibata received honoraria from Medtoronic, Boehringer Ingelheim, Eli Lilly and Mitsubishi Tanabe Pharma. Toshio Ohtsubo received lecture fees from Sanwa Kagaku Kenkyusho Co., Ltd. Hisashi Kai received lecture fees from Daiichi Sankyo Co Pharmaceutical Co., Ltd., Mitsubishi Tanabe Corporation, Shionogi & Co., Ltd., Sumitomo Dainippon Pharma Co., Ltd., and Takeda Pharmaceutical Co., Ltd. Masaaki Ito received lecture fees from Daiichi Sankyo Co Pharmaceutical Co., Ltd., Mitsubishi Tanabe Corporation, Bayer Yakuhin, Ltd. and Takeda Pharmaceutical Co., Ltd.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Okamoto, R., Kumagai, E., Kai, H. et al. Effects of lowering diastolic blood pressure to <80 mmHg on cardiovascular mortality and events in patients with coronary artery disease: a systematic review and meta-analysis. Hypertens Res 42, 650–659 (2019). https://doi.org/10.1038/s41440-018-0189-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-018-0189-z
Keywords
This article is cited by
-
Is it necessary to set a lower limit target for blood pressure control for the advanced-age population?
Hypertension Research (2023)
-
Low blood pressure and cardiovascular events in diabetic patients with coronary artery disease after revascularization: the CREDO-Kyoto registry cohort-1
Hypertension Research (2020)
-
Increased arterial stiffness and cardiovascular risk prediction in controlled hypertensive patients with coronary artery disease: post hoc analysis of FMD-J (Flow-mediated Dilation Japan) Study A
Hypertension Research (2020)
-
The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019)
Hypertension Research (2019)
