
Abstract
Melatonin is a hormone produced by the pineal gland, predominantly at night, and plays a pivotal role in regulating the circadian rhythm as well as a variety of biological functions, including anti-inflammation, anti-oxidation, inhibition of sympathetic nerve activity, and preservation of endothelial cell function. The intrarenal renin–angiotensin system (RAS) is one of the most important contributors in the pathophysiology of chronic kidney disease (CKD) and hypertension, independent of the circulating RAS, due to sodium reabsorption and inflammation and fibrosis in the kidney. However, the relationship between melatonin secretion and intrarenal RAS activation has remained unknown. It has been recently shown that impaired nighttime melatonin secretion is associated with nighttime urinary angiotensinogen excretion, a surrogate marker of intrarenal RAS activation and renal damage in patients with CKD. Moreover, it has also been indicated that melatonin administered exogenously exercises antioxidant effects that ameliorate intrarenal RAS activation and renal injury in chronic progressive CKD animal models. As a result, the new roles of melatonin in suppressing RAS in the kidney via amelioration of reactive oxygen species have been clarified. Therefore, we review the relationship between melatonin and intrarenal RAS activation and indicate the possibility of a new strategy to suppress CKD, which is a risk factor for cardiovascular and end-stage renal diseases.
Similar content being viewed by others


Introduction
Melatonin is a hormone produced by the pineal gland, predominantly at night, and plays a pivotal role in regulating the circadian rhythms of several biological systems. Moreover, melatonin serves a variety of biological functions, including anti-inflammation, anti-oxidation, inhibition of sympathetic nerve activity, and preservation of endothelial cell function. It is well known that melatonin administration suppresses blood pressure (BP) levels and that endogenous melatonin secretion levels decrease according to renal dysfunction [1,2,3,4,5,6,7].
The intrarenal renin–angiotensin system (RAS) is one of the most important contributors in the pathophysiology of chronic kidney disease (CKD) and hypertension, independent of the circulating RAS, because the intrarenal RAS plays a role in sodium reabsorption and inflammation and fibrosis in the kidney [8,9,10,11,12,13,14,15,16,17,18,19,20,21,22,23]. Moreover, it has also been shown that intrarenal reactive oxygen species (ROS) are activated in some CKD animal models and that intrarenal ROS and RAS activation play pivotal roles in their development [10, 19, 20, 24, 25].
However, the relationship between melatonin secretion and intrarenal ROS and RAS activation has remained unknown. The purpose of this review was to clarify the above issues.
The role of melatonin including regulation of the circadian rhythm as well as a variety of biological functions in the kidney
Melatonin is a hormone produced by the pineal gland, predominantly at night, which plays a major role in regulating the circadian rhythms of several biological systems [1]. In addition to regulation of the circadian rhythm, melatonin serves a variety of biological functions, including anti-inflammation, anti-oxidation, inhibition of sympathetic nerve activity, and preservation of endothelial cell function [2].
In the field of hypertension, a meta-analysis of the efficacy of exogenous melatonin in ameliorating nocturnal BP was performed by Grossman et al. [3]. They demonstrated that systolic and diastolic BPs decreased significantly with melatonin administration (systolic BP, −6.1 mm Hg; 95% confidence interval (CI) −10.7 to −1.5; p = 0.009; and diastolic BP, −3.5 mm Hg; 95% CI −6.1 to −0.9; p = 0.009) and concluded that adding melatonin to antihypertensive therapy is effective in ameliorating nocturnal hypertension (Fig. 1).

Effects of controlled-release (CR) melatonin on nocturnal systolic/diastolic blood pressure. Effects of CR melatonin on systolic blood pressure (left panel) and diastolic blood pressure (right panel). md mean difference, Ci confidence interval. Reprinted from Grossman et al. [3] with permission from the publisher. Copyright 2011, Dovepress Medical Press Ltd Oxford University Press
Moreover, melatonin is associated with renal function and plays a pivotal role in the pathophysiology of the kidney. First, Koch et al. [4] investigated the discrete mean melatonin concentrations at different time points in different renal functions of 28 patients with CKD. They showed that patients with the worst renal function (glomerular filtration rate (GFR) < 30 mL/min) had the lowest mean melatonin concentrations and that patients with the best renal function (GFR > 80 mL/min) had the highest melatonin concentrations (Fig. 2). As a cause, it is thought that impairment in β-adrenoceptor-mediated responsiveness plays an important role in the synthesis of serotonin N-acetyltransferase, the key enzyme in melatonin biosynthesis [26, 27].

Mean melatonin concentrations in four groups with increasingly affected renal functions. The error bars reflect the standard deviations of the raw data. The horizontal axis reflects the time of day (hours), and the vertical axis reflects the mean melatonin concentrations. Reprinted from Koch et al. [4] with permission from the publisher. Copyright 2009, Oxford University Press
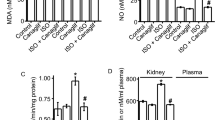
Melatonin has also been shown to contribute to retarding the deterioration of renal function and ameliorating its structure in several experimental animal models, such as 5/6 nephrectomy (Nx) rats, unilateral ureteral obstruction rats, spontaneously hypertensive rats, and adriamycin-induced nephropathy rats [5, 6, 28, 29]. For example, Quiroz et al. [5] demonstrated that melatonin administration improves the course of chronic renal failure in Nx rat models. That is, melatonin administration increased the endogenous hormone levels 13- to 15-fold, and rats in the Nx+ melatonin group had reduced oxidative stress (malondialdehyde levels in plasma and the remnant kidney as well as nitrotyrosine renal abundance), renal inflammation (p65 nuclear factor-κB-positive renal interstitial cells and infiltration of lymphocytes and macrophages), and renal damage (histological markers: increase in collagen, α-smooth muscle actin, and transforming growth factor-β renal abundance and structure (glomerulosclerosis and tubulointerstitial damage) and renal function (plasma creatinine and proteinuria)) (Fig. 3).

The role of melatonin to ameliorate oxidative stress and progression of renal damage in 5/6 nephrectomized rats. A Nitrotyrosine abundance in sham-operated rats (Sham), renal ablation rats without treatment (Nx), and renal ablation rats with melatonin (Nx+MEL). Graphic representation shows integrated optical density normalized for the β-actin control. Open bar, sham; filled bar, Nx; shaded bar, Nx+MEL. Data are presented as the means ± SE; ***p < 0.001 and **p < 0.01. B Collagen IV estimated by western blot in Sham, Nx, and Nx+MEL groups. Data are presented as the means ± SE; ***p < 0.001 and **p < 0.01. Reprinted from Quiroz et al. [5] with permission from the publisher. Copyright 2008, the American Physiological Society
The prevalence of CKD, which causes cardiovascular and end-stage renal diseases
It is known that CKD is one of the risk factors for cardiovascular disease (CVD) and end-stage renal disease (ESRD) [30, 31]. In fact, more than 400,000 Americans have ESRD, and over 300,000 of these patients require maintenance dialysis [32]. In addition, mortality rates remain above 20% per year with the use of dialysis, with more than half of the deaths related to CVD [32] More than 13.3 million people are also predicted to have CKD, and there are 0.2 million people with CKD stage 4+5 in Japan [33]. Moreover, it is expected that the number of affected individuals will increase worldwide in the future.
The association between renal damage and intrarenal RAS or ROS
For many years, it has been known that the circulating RAS plays a critical role in the regulation of arterial pressure and sodium homeostasis. In addition, it has been known that tissue-specific RAS exists in some organs, independent of the circulating RAS [8, 9]. The RAS in the kidney plays a role in sodium reabsorption and inflammation and fibrosis in the kidney and is one of the most important contributors to the pathophysiology of CKD, including IgA nephropathy, diabetic nephropathy, and hypertension. In addition, it has been reported that the activation of intrarenal RAS contributes to renal damage using selected animal models, including Dahl salt-sensitive rats, angiotensin II (AngII)-infused hypertensive rats, spontaneously hypertensive rats, diabetic nephropathy rats, IgA nephropathy model mice (high IgA of ddy (HIGA) mice), crescentic glomerulonephritis rats, and anti-thymocyte serum (ATS) nephritis rats [10,11,12,13,14,15,16,17,18,19,20,21,22,23]. We have also clarified that the levels of glomerular angiotensinogen (AGT) messenger RNA (mRNA), intrarenal AngII, and urinary AGT excretion in the ATS group were increased significantly compared with those in the control group and that administration of olmesartan, an AngII receptor blocker (ARB), significantly decreased the incidence of renal lesions, proteinuria, and intrarenal RAS activity; we have also concluded that an increase in kidney-specific RAS activity plays an important role in the development of ATS nephritis [22].
Moreover, it has also been shown that intrarenal ROS is activated in patients with diabetic nephropathy and IgA nephropathy [10, 24] and activates intrarenal RAS in some animal models, including Dahl salt-sensitive rats, diabetic nephropathy rats, and IgA nephropathy model mice [19, 20, 25]. We have also clarified that the expression of two intrarenal ROS markers (4-hydroxy-2-nonenal and heme oxygenase-1), intrarenal AngII, and markers of renal damage (mesangial matrix expansion and the desmin-positive area) decreased significantly in HIGA mice treated with olmesartan or the superoxide dismutase mimetic tempol, but not in HIGA mice treated with RAS-independent antihypertensive drugs (hydralazine, reserpine, and hydrochlorothiazide), compared with those in untreated HIGA mice and concluded that intrarenal ROS and RAS activation plays a pivotal role in the development of IgA nephropathy [20].
The relationship between melatonin and tissue-specific RAS activity
As mentioned above, the roles of melatonin for hypertension or tissue damage including the kidney have been clarified. Next, the relationships between melatonin and tissue-specific RAS, one of the most contributing factors to tissue damage, especially for the kidney, are reviewed.
The relationship between melatonin and pineal RAS activity
Some studies have reported the relationship between melatonin and pineal RAS activity. Acuña et al. [34] first demonstrated that pinealectomy results in decreased plasma renin activity and that administration of indole melatonin reverses the effects of pinealectomy. Baltatu et al. [35] also detected local RAS in the pineal gland and, thereafter, they demonstrated that the pineal melatonin content was significantly decreased by ARB in vivo, in cultured glands and in transgenic rats with inhibited production of AGT exclusively in astrocytes “TGR(ASrAOGEN)” via significant decreases in pineal 5-hydroxytryptophan, serotonin, 5-hydroxyindole acetic acid, and N-acetylserotonin levels. In addition, they showed that the tryptophan hydroxylase (TPH) mRNA levels were significantly lower in TGR(ASrAOGEN) than in control rats. Therefore, these findings suggest that local pineal RAS mediates a tonic modulation of indole synthesis by influencing the activity of TPH via AngII receptors [36, 37] (Fig. 4).

Relationship between melatonin and brain renin-angiotensin system (RAS) activity. A. Effects of angiotensin II (AngII) type 1 receptor antagonist (losartan) on pineal melatonin production in vivo. Decreased pineal melatonin levels in the control (filled bar, n = 9) and in rats treated with 10 mg/kg/day losartan for 4 days (open bar, n = 10). B. Effects of losartan on pineal melatonin production in vitro. Decreased pineal melatonin levels in untreated (filled bar, n = 23) and losartan-treated pineal cultures (open bar, n = 27). C. Effects of losartan on pineal melatonin production in transgenic rats with inhibited production of angiotensinogen (AGT) exclusively in the astrocytes, TGR(ASrAOGEN) rats (open bar, n = 9) and Hanover Sprague-Dawley (SD) rats (filled bar, n = 9). D. Interaction between pineal RAS and melatonin. AngII, produced from AGT in glial cells, acts on AngII type 1b receptors present in pinealocytes to stimulate tryptophan hydroxylase, which is the rate-limiting enzyme in melatonin synthesis. Both angiotensin and melatonin may interact to regulate rhythmicity either centrally in the suprachiasmatic nucleus (SCN) or peripherally in clocks present in several cardiovascular organs. Reprinted from Baltatu et al. [36] with permission of the publisher (Fig. 4A–C). Copyright 2002, International Society for Neurochemistry. Reprinted from Campos et al. [37] with permission of the publisher (Fig. 4D). Copyright 2013
The relationship between melatonin and intrarenal RAS activity
Clinical settings
As mentioned above, melatonin is a hormone regulating the circadian rhythm and has multiple functions, such as antioxidant and anti-adrenergic effects and enhancement of nitric oxide bioavailability. However, it was not known if impaired endogenous melatonin secretion is related to BP, intrarenal RAS, or renal damage in patients with CKD. Therefore, to clarify these relationships, 24-h ambulatory BP monitoring and collection of urine during the daytime and nighttime were performed in 53 patients with CKD. Thereafter, the relationships between melatonin metabolite urinary 6-sulfatoxymelatonin (U-aMT6s), BP, renal function, urinary angiotensinogen (U-AGT), and urinary albumin (U-Alb) were investigated. As a result, it has been found that patients’ U-aMT6s levels were significantly and negatively correlated with clinical parameters, such as renal function, systolic BP, U-AGT, and U-Alb, in both the daytime and the nighttime, and U-aMT6s levels were significantly associated with U-AGT and U-Alb only at night using multiple regression analyses after adjustment for age, sex, and estimated glomerular filtration rate (eGFR). It was concluded that impaired nighttime melatonin secretion may be associated with nighttime intrarenal RAS activation and renal damage in patients with CKD [38] (Table 1).
Animal experiments
As mentioned above, melatonin is recognized as a powerful antioxidant, and it has been clarified that impaired nighttime melatonin secretion correlates negatively with urinary AGT excretion in patients with CKD. However, whether melatonin supplementation ameliorates the augmentation of intrarenal RAS via the reduction of ROS production has remained unknown. Therefore, the association between melatonin and intrarenal RAS and ROS was investigated using 5/6 nephrectomized (Nx) rats as a chronic progressive CKD model. The 5/6 Nx rats were divided into untreated and melatonin-treated Nx rats and compared with control rats, and the levels of intrarenal RAS and ROS components and renal injury were evaluated after 4 weeks of treatment.
As a result, compared with the control rats, the untreated Nx rats exhibited significant increases in higher oxidative stress (8-hydroxy-2’-deoxyguanosine), lower antioxidant (superoxide dismutase) activity, intrarenal AGT, AngII type 1 receptor and AngII, and increased markers of interstitial fibrosis in the remnant kidneys, and treatment with melatonin significantly reversed these abnormalities (Fig. 5). It is concluded that antioxidant treatment with melatonin was shown to ameliorate intrarenal RAS activation and renal injury in a 5/6 Nx rat model [39].

The relationship between melatonin secretion and intrarenal renin-angiotensin system (RAS) activity or renal damage in 5/6 nephrectomized (Nx) rats. A Immunoblot for angiotensinogen (AGT) in the kidney. Representative immunoblot data of AGT and densitometric ratios of AGT/glyceraldehyde-3-phosphate dehydrogenase (GAPDH): densitometric ratios of AGT bands against GAPDH bands are calculated relative to the control group. B Immunostaining for AGT expression in the renal cortex and the degrees of immunoreactivity. Immunostaining for AGT expression in the control group reveals slight expression in the proximal tubular cells and dramatically increased expression in the 5/6 nephrectomized rats without treatment (Nx group). AGT expression is significantly reduced in the 5/6 nephrectomized rats with melatonin (Nx+MEL group) than that in the Nx group. Twenty random microscopic fields (×400) in the renal cortex are examined in each experimental animal, and the average AGT levels, excluding vascular and glomerular lesions, are obtained. The original magnification is ×400. C Immunostaining for intrarenal AngII. Immunostaining for intrarenal AngII in the control group is weak and observed mainly in some distal tubular cells. Immunostaining for AngII in the Nx group reveals significant expression in the proximal and distal tubules, which is significantly reduced in the Nx+MEL group. The original magnification is ×400. Twenty random microscopic fields (×400) in the renal cortex are examined in each experimental animal, and the average AngII-positive areas, excluding vascular and glomerular lesions, are obtained. D Immunostaining for α-smooth muscle actin (α-SMA) in the renal cortex. Normal positive α-SMA staining is seen in the arterioles. Significantly increased α-SMA-positive areas around the glomerulus and in the interstitial area are observed in the 5/6 nephrectomized rats without treatment (Nx group). The α-SMA-positive area is significantly reduced in the Nx+MEL group. Twenty random microscopic fields ((×400) in the renal cortex are examined for each experimental animal, and the average α-SMA-positive areas, excluding vascular and glomerular lesions, are obtained. The original magnification is ×400. The open bar indicates the control group, the filled bar indicates the Nx group, and the shaded bar indicates the Nx+MEL group. Data are presented as the mean ± SE; *p < 0.05 the control group vs. Nx and Nx+MEL groups; #p < 0.05 Nx group vs. Nx+MEL group. AGT angiotensinogen, GAPDH glyceraldehyde-3-phosphate dehydrogenase, Nx nephrectomy, MEL melatonin, AngII angiotensin II, α-SMA α-smooth muscle actin. Reprinted from Ishigaki et al. [39] with permission from the publisher. Copyright 2018, Springer
Conclusion
Melatonin is a hormone that plays a major role in regulating the circadian rhythms of several biological systems. In addition, melatonin also serves a variety of biological functions, including anti-inflammation, anti-oxidation, inhibition of sympathetic nerve activity, and preservation of endothelial cell function. The intrarenal RAS is one of the most important contributors for the pathophysiology of CKD and hypertension. Although the relationship between melatonin secretion and intrarenal RAS activation remained unknown, it has been recently clarified in both patients with CKD and chronic progressive CKD animal models. Therefore, we observed that the antioxidative effect of melatonin ameliorates intrarenal RAS activation and renal injury (Fig. 6). Compared with the administration of RAS inhibitors or melatonin alone, the simultaneous administration of RAS inhibitors and melatonin may be a new strategy to more effectively suppress CKD, which is one of the risk factors for CVD and ESRD.

A scheme of the relationship between melatonin and renal damage via intrarenal reactive oxygen species (ROS) activation or intrarenal renin-angiotensin system (RAS) activation. Arrows indicate increase and dashed arrows indicate suppression
References
Brzezinski A. Melatonin in humans. N Engl J Med. 1997;336:186–95.
Russcher M, Koch B, Nagtegaal E, van der Putten K, ter Wee P, Gaillard C. The role of melatonin treatment in chronic kidney disease. Front Biosci. 2012;17:2644–56.
Grossman E, Laudon M, Zisapel N. Effect of melatonin on nocturnal blood pressure: meta-analysis of randomized controlled trials. Vasc Health Risk Manag. 2011;7:577–84.
Koch BC, van der Putten K, Van Someren EJ, Wielders JP, Ter Wee PM, Nagtegaal JE, et al. Impairment of endogenous melatonin rhythm is related to the degree of chronic kidney disease (CREAM study). Nephrol Dial Transplant. 2010;25:513–9.
Quiroz Y, Ferrebuz A, Romero F, Vaziri ND, Rodriguez-Iturbe B. Melatonin ameliorates oxidative stress, inflammation, proteinuria, and progression of renal damage in renal mass reduction. Am J Physiol Ren Physiol. 2008;294:F336–44.
Escribano BM, Moreno A, Tasset I, Tunez I. Impact of light/dark cycle patterns on oxidative stress in an adriamycin-induced nephropathy model in rats. PLoS ONE. 2014;9:e97713.
Agabiti-Rosei C, Favero G, De Ciuceis C, Rossini C, Porteri E, Rodella LF, et al. Effect of long-term treatment with melatonin on vascular markers of oxidative stress/inflammation and on the anticontractile activity of perivascular fat in aging mice. Hypertens Res. 2017;40:41–50.
Kobori H, Nangaku M, Navar LG, Nishiyama A. The intrarenal renin-angiotensin system: from physiology to the pathobiology of hypertension and kidney disease. Pharmacol Rev. 2007;59:251–87.
Navar LG, Harrison-Bernard LM, Nishiyama A, Kobori H. Regulation of intrarenal angiotensin II in hypertension. Hypertension. 2002;39:316–22.
Kobori H, Katsurada A, Ozawa Y, Satou R, Miyata K, Hase N, et al. Enhanced intrarenal oxidative stress and angiotensinogen in IgA nephropathy patients. Biochem Biophys Res Commun. 2007;22:156–63.
Yamamoto T, Nakagawa T, Suzuki H, Ohashi N, Fukasawa H, Fujigaki Y, et al. Urinary angiotensinogen as a marker of intrarenal angiotensin II activity associated with deterioration of renal function in patients with chronic kidney disease. J Am Soc Nephrol. 2007;18:1558–65.
Kobori H, Ohashi N, Katsurada A, Miyata K, Satou R, Saito T, et al. Urinary angiotensinogen as a potential biomarker of severity of chronic kidney diseases. J Am Soc Hypertens. 2008;2:349–54.
Kobori H, Alper AB Jr, Shenava R, Katsurada A, Saito T, Ohashi N, et al. Urinary angiotensinogen as a novel biomarker of the intrarenal renin-angiotensin system status in hypertensive patients. Hypertension. 2009;53:344–50.
Saito T, Urushihara M, Kotani Y, Kagami S, Kobori H. Increased urinary angiotensinogen is precedent to increased urinary albumin in patients with type 1 diabetes. Am J Med Sci. 2009;338:478–80.
Nishiyama A, Konishi Y, Ohashi N, Morikawa T, Urushihara M, Maeda I, et al. Urinary angiotensinogen reflects the activity of intrarenal renin-angiotensin system in patients with IgA nephropathy. Nephrol Dial Transplant. 2011;26:170–7.
Kobori H, Nishiyama A, Abe Y, Navar LG. Enhancement of intrarenal angiotensinogen in Dahl salt-sensitive rats on high salt diet. Hypertension. 2003;41:592–7.
Kobori H, Prieto-Carrasquero MC, Ozawa Y, Navar LG. AT1 receptor mediated augmentation of intrarenal angiotensinogen in angiotensin II-dependent hypertension. Hypertension. 2004;43:1126–32.
Kobori H, Ozawa Y, Suzaki Y, Nishiyama A. Enhanced intrarenal angiotensinogen contributes to early renal injury in spontaneously hypertensive rats. J Am Soc Nephrol. 2005;16:2073–80.
Miyata K, Ohashi N, Suzaki Y, Katsurada A, Kobori H. Sequential activation of the reactive oxygen species/angiotensinogen/renin-angiotensin system axis in renal injury of type 2 diabetic rats. Clin Exp Pharmacol Physiol. 2008;35:922–7.
Ohashi N, Katsurada A, Miyata K, Satou R, Saito T, Urushihara M, et al. Role of activated intrarenal reactive oxygen species and renin-angiotensin system in IgA nephropathy model mice. Clin Exp Pharmacol Physiol. 2009;36:750–5.
Urushihara M, Ohashi N, Miyata K, Satou R, Acres OW, Kobori H. Addition of angiotensin II type 1 receptor blocker to CCR2 antagonist markedly attenuates crescentic glomerulonephritis. Hypertension. 2011;57:586–93.
Ohashi N, Yamamoto T, Huang Y, Misaki T, Fukasawa H, Suzuki H, et al. Intrarenal RAS activity and urinary angiotensinogen excretion in anti-thymocyte serum nephritis rats. Am J Physiol Ren Physiol. 2008;295:F1512–8.
Isobe S, Ohashi N, Ishigaki S, Tsuji T, Sakao Y, Kato A, et al. Augmented circadian rhythm of the intrarenal renin-angiotensin systems in anti-thymocyte serum nephritis rats. Hypertens Res. 2016;39:312–20.
Kamiyama M, Urushihara M, Morikawa T, Konishi Y, Imanishi M, Nishiyama A, et al. Oxidative stress/angiotensinogen/renin-angiotensin system axis in patients with diabetic nephropathy. Int J Mol Sci. 2013;14:23045–62.
Kobori H, Nishiyama A. Effects of tempol on renal angiotensinogen production in Dahl salt-sensitive rats. Biochem Biophys Res Commun. 2004;315:746–50.
Souchet T, Brée F, Baatard R, Fontenaille C, D’Athis P, Tillement JP, et al. Impaired regulation of beta 2-adrenergic receptor density in mononuclear cells during chronic renal failure. Biochem Pharmacol. 1986;35:2513–9.
Nagtegaal JE, Smits MG, Kerkhof GA, Pandi-Perumal SR. Chronobiological, clinical and pharmacological aspects of melatonin in human circadian rhythm dysfunction. In: Haldar C, Singaravel M, Kumar Maitra S, editors. Treatise on pineal gland and melatonin. Enfield: Science Publishers; 2002. p. 461–89.
Ozbek E, Ilbey Y, Ozbek M, Simsek A, Cekmen M, Somay A. Melatonin attenuates unilateral ureteral obstruction-induced renal injury by reducing oxidative stress, iNOS, MAPK, and NF-kB expression. J Endourol. 2009;23:1165–73.
Nava M, Quiroz Y, Vaziri N, Rodriguez-Iturbe B. Melatonin reduces renal interstitial inflammation and improves hypertension in spontaneously hypertensive rats. Am J Physiol Ren Physiol. 2003;284:F447–54.
Go AS, Chertow GM, Fan D, McCulloch CE, Hsu CY. Chronic kidney disease and the risks of death, cardiovascular events, and hospitalization. N Engl J Med. 2004;351:1296–305.
Drey N, Roderick P, Mullee M, Rogerson M. A population-based study of the incidence and outcomes of diagnosed chronic kidney disease. Am J Kidney Dis. 2003;42:677–84.
Renal Data System. USRDS 2003 annual data report: atlas of end-stage renal disease in the United States. Bethesda: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2003.
Imai E, Horio M, Watanabe T, Iseki K, Yamagata K, Hara S, et al. Prevalence of chronic kidney disease in the Japanese general population. Clin Exp Nephrol. 2009;13:621–30.
Acuña D, Soler A, García-Torres L, Vargas F, García del Río C, Quesada T, et al. Inhibition of the renin-angiotensin system by pinealectomy in female rats. Rev Esp Fisiol. 1982;38:251–5.
Baltatu O, Lippoldt A, Hansson A, Ganten D, Bader M. Local renin-angiotensin system in the pineal gland. Brain Res Mol Brain Res. 1998;54:237–42.
Baltatu O, Afeche SC, José dos Santos SH, Campos LA, Barbosa R, Michelini LC, et al. Locally synthesized angiotensin modulates pineal melatonin generation. J Neurochem. 2002;80:328–34.
Campos LA, Cipolla-Neto J, Amaral FG, Michelini LC, Bader M, Baltatu OC. The angiotensin-melatonin axis. Int J Hypertens. 2013;2013:521783.
Ishigaki S, Ohashi N, Isobe S, Tsuji N, Iwakura T, Ono M, et al. Impaired endogenous nighttime melatonin secretion relates to intrarenal renin-angiotensin system activation and renal damage in patients with chronic kidney disease. Clin Exp Nephrol. 2016;20:878–84.
Ishigaki S, Ohashi N, Matsuyama T, Isobe S, Tsuji N, Iwakura T, et al. Melatonin ameliorates intrarenal renin-angiotensin system in a 5/6 nephrectomy rat model. Clin Exp Nephrol. 2018;22:539–49.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Ohashi, N., Ishigaki, S. & Isobe, S. The pivotal role of melatonin in ameliorating chronic kidney disease by suppression of the renin–angiotensin system in the kidney. Hypertens Res 42, 761–768 (2019). https://doi.org/10.1038/s41440-018-0186-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41440-018-0186-2
Keywords
This article is cited by
-
Bupi Yishen formula attenuates kidney injury in 5/6 nephrectomized rats via the tryptophan-kynurenic acid-aryl hydrocarbon receptor pathway
BMC Complementary Medicine and Therapies (2021)
-
Melatonin ameliorates hypertension in hypertensive pregnant mice and suppresses the hypertension-induced decrease in Ca2+-activated K+ channels in uterine arteries
Hypertension Research (2021)
-
Circadian rhythm of the intrarenal renin–angiotensin system is caused by glomerular filtration of liver-derived angiotensinogen depending on glomerular capillary pressure in adriamycin nephropathy rats
Hypertension Research (2021)
-
Possible benefits of exogenous melatonin for individuals on dialysis: a narrative review on potential mechanisms and clinical implications
Naunyn-Schmiedeberg's Archives of Pharmacology (2021)
-
Elderly as a High-risk Group during COVID-19 Pandemic: Effect of Circadian Misalignment, Sleep Dysregulation and Melatonin Administration
Sleep and Vigilance (2020)
