
Abstract
Objective
To evaluate the incidence of consecutive exotropia following bilateral medial rectus muscle recession surgery (BMR) for esotropia using non-absorbable compared with absorbable sutures in children undergoing strabismus surgery.
Methods
A retrospective cohort study of all children with esotropia who underwent BMR by a single surgeon in a tertiary public hospital. As of February 2018, only non-absorbable sutures were used. The primary outcome was the incidence of consecutive exotropia.
Results
A total of 121 children were included in the analysis, 3.66 ± 2.62 years, 53% were male. In 80 children (66%) non-absorbable sutures were used (non-absorbable group) and in 41 children (34%) absorbable sutures were used (absorbable group). Consecutive exotropia (≥ 8 prism dioptres) occurred in ten children (24%) in the absorbable group and in three children (4%) in the non-absorbable group (OR = 8.28, 95% CI = 2.13–32.13; P = 0.002). This difference between groups remained significant after adjustment for potential confounders and follow-up time (HR = 4.98, 95% CI = 1.30–19.05, P = 0.019). Mean follow-up time was 22 and 12 months in the absorbable and non-absorbable groups, respectively (P < 0.001). Two children in the non-absorbable group had pyogenic granuloma that resolved after 3 months of topical steroidal therapy.
Conclusion
Routine use of non-absorbable sutures in BMR surgery for esotropia may be a preferable alternative to absorbable sutures for the prevention of consecutive exotropia.
Similar content being viewed by others

Introduction
Consecutive exotropia is the most common cause for re-operation following bilateral medial rectus recession (BMR) for esotropia, reported in 12–27% of cases[1,2,3,4,5]. Overcorrection observed immediately after surgery is usually explained by miscalculation of the amount of medial rectus recession or muscle slippage [6, 7].
Overcorrection that develops more than 1 month after surgery can be related to “stretched scar” formation. This term was suggested by Dr. Irene Ludwig after exploring the muscles of patients with overcorrection. It consists of an elongated scar segment of variable length interposed between the muscle and its insertion site on the sclera that causes weakening of the muscle strength [8]. Several theories regarding the aetiology of stretched scar formation were suggested among them the excessive use of steroids, genetic factors and chronic inflammation induced during the dissolution of the absorbable sutures [8, 9]. Regardless of the cause, the result is the same: overcorrection. It is postulated that a large proportion of consecutive exotropia cases following BMR results from stretched scar formation [10,11,12].
It was previously suggested in clinical trials as well as animal models that the use of non-absorbable sutures can decrease the incidence of stretched scar formation [8, 13, 14]. Parsa et al. showed the rate of overcorrection after adjustable inferior rectus recession was significantly lower with the use of non-absorbable sutures[13]. Awadein et al. had found that in large medial rectus recessions (≥ 6.5 mm) the use of non-absorbable sutures reduced the incidence of consecutive exotropia [15].
In this study, we compared the rate of consecutive exotropia following BMR using absorbable vs. non-absorbable sutures as a routine method in all cases. We hypothesized that the routine use of non-absorbable sutures may reduce the incidence of consecutive exotropia.
Methods
Study design and patient population
We conducted a retrospective cohort study of children who underwent a primary BMR with or without inferior oblique muscle weakening due to esotropia, by a single surgeon (YM) from January 2010 to January 2020. Patients were included if they were under 18 years at the time of surgery, that was their first strabismus surgery and only the direct-to-sclera technique suturing was used. Between the years 2010 and 2018, only absorbable 6-0 polyglactin 910 sutures (Vicryl, Ethicon, Somerville, NJ) were used (absorbable group). As of February 2018, only non-absorbable, polyester fibre sutures (either Ethibond Excel 5.0 [Ethicon, Johnson and Johnson Int] or Mersilene 6.0 [Ethicon, Somerville, NJ]) were used (non-absorbable group). From February 2011 to January 2018, only the hang-back technique was used, hence those children were not included in the study group. Children with a minimal follow-up time of 6 months were included. Patients were excluded from our analysis if other extraocular muscles were operated on, apart from the inferior oblique.
Primary and secondary outcomes
The primary outcome was the incidence of consecutive exotropia diagnosed as postoperative exotropia of 8 prism dioptre (PD) or more occurring any time after surgery. Surgical success was considered as an alignment within 8 PD at distance and near. Consecutive exotropia was regarded as a dichotomous variable.
Secondary outcomes were residual esotropia and other complications in each group.
Data collection and definition of variables
Data were extracted from the patients’ medical records. The collected data included: gender, age at diagnosis of esotropia and age at surgery, type of esotropia, preoperative cycloplegic refraction with Cyclopentolate hydrochloride and Tropicamide (anisometropia was defined as the absolute difference in mean spherical equivalent powers between the right eye and the left eye of more than one dioptre), data regarding full ophthalmologic examination (including best-corrected visual acuity for children ≥3 years of age, anterior segment and funduscopic examination) and the presence of amblyopia. Measurements of deviation at distance and near preoperatively and on follow-up visits postoperatively were recorded on the first week after surgery and 1, 3, 6 and 12 months after surgery and once a year afterwards, amount of recession, intraoperative and postoperative complications including suture extrusion, pyogenic granuloma and suture break, the incidence of consecutive exotropia diagnosis and deviation measurements at distance and near were also recorded.
Full correction of hypermetropia as determined by cycloplegic retinoscopy was prescribed when indicated.
Surgical technique
The direct-to-sclera suturing technique was used. Briefly, the suture (either absorbable or non-absorbable) was passed through the muscle belly and a knot was tied, then both needles were passed closer to insertion, and secured by another knot. The muscle was detached and sutured to the sclera behind the insertion as needed in a crossed sword configuration. When the non-absorbable suture was used, after suturing the muscle to the sclera, both needles were left attached and not cut. The needles were then passed distally underneath the muscle belly and through the muscle tissue about 3 mm distally and then pulled out through the muscle belly and cut, allowing the loose ends of the suture to retract underneath the muscle belly (Fig. 1 demonstrates the technique). This technique prevents protrusion of the suture’s cut ends through the conjunctiva as well as any contact between the conjunctiva and the sutures which are buried underneath the muscle belly.

A The needle is passed through the sclera angled away from the insertion. B The knot is tied while being covered by muscle tissue. Both needles were intact. C Both needles are passed distally through the muscle belly and the sutures protrude through the muscle. D Both sutures are pulled up and cut just above the muscle tissue. e Sutures retract beneath the muscle belly.
Statistical analysis
The baseline and outcome variables were compared between the two groups with the use of the Student’s t test, the chi-square test and the Mann–Whitney U test, as appropriate. The Student t-test or the Mann–Whitney U test was used for the analysis of continuous variables according to their distribution. Normal distribution was evaluated with Q–Q plot, the Shapiro–Wilk test and histogram chart with a normal distribution curve. Results were considered significant if the P-value was below 0.05 in a two-sided test.
The chi-square test was used to test the association between the incidence of consecutive exotropia and the type of suture in a bivariate manner. Kaplan–Meier survival analysis was used to assess for survival without consecutive exotropia. For the multivariable analysis, we used Cox regression with the likelihood ratio test to choose which confounders to retain in the model. All analyses were performed using IBM SPSS Statistics for Windows version 24.0 (IBM Corp., Armonk, NY, USA).
Results
A total of 121 children were included in the analysis, the mean age was 3.66 ± 2.62 years, 53% were male. All underwent BMR with or without inferior oblique muscle weakening. In 18 children (15%), an inferior oblique overaction was observed and inferior oblique weakening was performed. Mean preoperative measurements of deviation were 31.75 ± 8.97 PD at near and 28.31 ± 9.34 PD at distance. The mean medial rectus recession on each side was 4.86 ± 0.85 mm.
Table 1 shows the demographic and clinical characteristics of the children according to the sutures used. The groups differed significantly in follow-up time.
The non-absorbable group included 80 children (66%) and the absorbable group included 41 (34%) children.
Mean follow-up time after surgery was 22.15 ± 11.82 months and 12.68 ± 8.20 months in the absorbable and non-absorbable groups, respectively (P < 0.001).
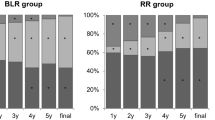
Consecutive exotropia occurred in ten children (24%) in the absorbable group and in three children (4%) in the non-absorbable group (OR = 8.28, 95% CI = 2.13–32.13; P = 0.002). After adjustment for follow-up time using the Kaplan–Meier survival analysis, the difference between groups remained significant (P = 0.003) (Fig. 2). Since follow-up time in the non-absorbable group was shorter (due to the chronologically later use of the non-absorbable suture), some of the children appear as censored. None of the children in this group was lost to follow-up. In the multivariable analysis using Cox regression, adjusting for gender, age, follow-up time, length of recession and surgical intervention on the inferior oblique, the rate of consecutive exotropia in the non-absorbable group was significantly lower than in the absorbable group (HR = 4.98, 95% CI = 1.30–19.05, P = 0.019) (Table 2).

Kaplan–Meier survival curve for the incidence of consecutive exotropia in the absorbable and non-absorbable groups.
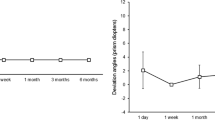
Consecutive exotropia was diagnosed 5.03 ± 4.87 (range 2–18) months after surgery in the absorbable group. In the non-absorbable group, the three children in whom consecutive exotropia occurred were diagnosed 11 days (6 PD at near, 12 PD at distance), 25 days (6 PD at near,14 PD at distance) and 30 days (8 PD at near, 10 PD at distance) after surgery. The time elapsed from surgery to the diagnosis of consecutive exotropia was significantly shorter in the non-absorbable suture group (P = 0.013). In the absorbable group, measured deviation of consecutive exotropia was 18.50 ± 11.76 PD at near and 12.22 ± 6.91 PD at distance.
Five children in the absorbable group underwent a second surgery for the exotropia. The stretched scar was recorded as an intraoperative finding in all surgical reports. Neither of the children in the non-absorbable group had a second surgery as their parents were not bothered by the relatively small deviation.
Residual esotropia (more than 8 PD) was recorded in 16 of the children 1 month after surgery, with no significant difference between groups. In the absorbable group, seven children with mean residual esotropia of 9.87 ± 3.86 PD, and 9 children with mean residual esotropia of 10.80 ± 4.44 PD in the non-absorbable group (P = 0.69). Mean residual esotropia at near and distance on the follow-up visit 3 months after surgery was recorded in 2 (5%) and 6 (7%) of patients in the absorbable and non-absorbable group, respectively (P = 0.45). Two children in the non-absorbable group had pyogenic granuloma that resolved after 3 months of topical steroidal therapy. In one patient of the non-absorbable group, suture break necessitated revision under anaesthesia 3 days after the original operation. The groups did not differ significantly in the complications rate (OR = 3.11, 95% CI = 0.27–29.65, P = 0.36).
Discussion
Overcorrection after strabismus surgery and the possible need for a second surgery are major causes of stress and concern for children and their families. Exploring ways to lower the incidence of overcorrection and subsequent second surgeries could have a large impact, both emotionally and economically. One such approach which has received relatively little attention in recent years is the use of non-absorbable sutures [8, 13, 15]. The major finding of this study is that the incidence of consecutive exotropia was reduced by more than 75% by using non-absorbable sutures without increasing adverse outcomes.
Consecutive exotropia might present as early as one week after surgery. Early occurring overcorrection is usually due to excessive recession [2,3,4] or a result of a slipped muscle due to an inappropriate surgical technique as described previously by Parks and Bloom [6, 7]. Late-onset consecutive exotropia diagnosed after at least 1 month postoperatively may be the result of a stretched scar appearing upon dissolution of the absorbable sutures. The timing of appearance of consecutive exotropia in the absorbable group in our study supports this observation, and indeed, stretched scar was identified in many of the children that were re-operated. In contrast, the consecutive exotropia in the non-absorbable group was diagnosed within the first month after surgery suggesting overcorrection due to a larger than needed recession. Surgical results remained stable thereafter, suggesting good scar formation between the muscle and the sclera.
Another finding that supports the hypothesis on the stretched scar formation is the difference in deviation for distance and near in the consecutive exotropia patients in each group. While the consecutive exotropia in the absorbable group was larger for near rather than for distance, in the non-absorbable group, the consecutive exotropia deviation in all three patients was larger for distance. This may suggest that in the absorbable group, the formation of a stretched scar is weakening the medial rectus convergence force causing convergence insufficiency. However, in the non-absorbable group, the larger deviation for distance is caused by an imbalance between the lateral rectus and the medial rectus due to excessive recession while the convergence force is maintained.
In this study, the incidence of consecutive exotropia in the absorbable group is similar to that reported in previous studies [2,3,4]. This highlights the significantly low rate of consecutive exotropia of 4% in the non-absorbable group which remained significant when adjusting for follow-up time, age, gender, amount of recession and surgical intervention on the inferior oblique muscle. In a similar study, Awadein et al. compared the incidence of consecutive exotropia with the use of absorbable and non-absorbable sutures using the hang-back technique in children with large esotropia. The results were comparable with ours; consecutive exotropia was diagnosed in 30% of patients in the absorbable group compared with 6% in the non-absorbable group. However, these results were limited to a specific group of patients with large medial rectus recessions (6.5–7 mm) [15]. The authors also described a stretched scar (or pseudo-tendon as they call it) or muscle retraction within the muscle sleeve (slipped muscle) discovered at re-operation. These two phenomena can possibly be prevented by using a non-absorbable suture that is safely anchoring the muscle to the sclera and prevents slippage of muscle fibres within its sleeve. Moreover, we have found that the association between the use of non-absorbable sutures and the lower risk of consecutive exotropia remained significant after adjusting for the amount of recession. Hence, the use of non-absorbable sutures decreased the risk of consecutive exotropia in any amount of recession – both small and large, a concept yet to be implemented in common practice.
The main reason for the wide use of absorbable sutures in BMR is the concern of a possible extrusion of the permanent knot through the conjunctiva and tissue irritation. In order to reduce the risk of this complication, the sutures should be carefully buried allowing the knot to be fully covered by muscle tissue. This is a simple technique and should not be regarded as an obstacle when considering the use of non-absorbable sutures in this procedure. Another possible complication with the use of non-absorbable sutures is the risk of pyogenic granuloma formation due to the continuing irritation of tissue. Although this complication can occur also with absorbable suture use, it occurred twice in our non-absorbable group. We later learned to avoid this complication by assuring that the entire suture is covered by the muscle belly. To achieve that goal, the surgical field was inspected at the end of the surgery, if suture material that is not covered by muscle tissue was identified, an 8–0 Vicryl suture was used to stretch the muscle tissue over the suture so that it will be completely covered (this was used only in two children in our study group, and when excluded from analysis—there was no change in the results).
Of the four rectus muscles, the inferior rectus is known for its relatively high rate of late overcorrection following a recession. The routine use of non-absorbable sutures is recommended by many to eliminate this complication [13]. In this study, we have shown that the medial rectus is also prone to this late overcorrection. One possible explanation is the relatively short arch of contact between these muscles and the sclera that may facilitate the formation of a stretched scar. Another plausible explanation is that these muscles generate higher and more frequent force during convergence as opposed to divergence, and downgaze as opposed to up-gaze.
To our knowledge, this is the first cohort study to examine the effect of routine use of non-absorbable sutures in BMR surgeries on the incidence of consecutive exotropia. The strengths of the study are its relatively long follow-up, the use of the same surgical technique and the fact that all surgeries were performed by the same experienced surgeon. All of which minimize possible confounding effects, emphasizing that the suture type serves as an independent risk factor for consecutive exotropia.
This study has several limitations. First, follow-up period was longer in the absorbable group. We therefore used the Kaplan–Meier and Cox regression analyses which inherently take differences in follow-up time into account. Second, due to the retrospective nature of the study, not all possible confounders could be measured or accounted for. Third, longer follow-up times might be needed to uncover subtle or less common adverse outcomes which this study did not detect.
In conclusion, in this study, we have shown that the routine use of non-absorbable sutures in BMR surgery could result in a significantly lower rate of consecutive exotropia regardless of the amount of recession. This finding suggests that with the correct suture burying technique, the use of non-absorbable sutures presents a potentially preferable alternative to absorbable sutures in the correction of childhood esotropia.
Summary
What was known before
-
Bilateral medial rectus recession surgery is one of the most commonly performed surgeries in paediatric ophthalmology.
-
Consecutive exotropia is the most common cause for re-operation following bilateral medial rectus recession for the esotropia due to the formation of a stretched scar.
-
It was previously suggested in clinical trials as well as animal models that the use of non-absorbable sutures can decrease the incidence of stretched scar formation.
What this study adds
-
The use of non-absorbable sutures in bilateral medial rectus recession surgery demonstrated a significantly lower rate of consecutive exotropia regardless of the amount of recession.
-
The use of non-absorbable sutures was safe and resulted in predictable, stable and satisfying surgical outcomes.
References
Zehavi-Dorin T, Ben-Zion I, Mezer E, Wygnanski-Jaffe T. Long-term results of bilateral medial rectus muscle recession in children with developmental delay. Strabismus. 2016;24:7–11.
Repka MX, Guyton DL. Comparison of hang-back medial rectus recession with conventional recession. Ophthalmology. 1988;95:782–7.
Spierer O, Spierer A. Comparison of hang-back and conventional bimedial rectus recession in infantile esotropia. Graefes Arch Clin Exp Ophthalmol. 2010;248:901–5.
Oh SY, Park K-A, Oh SY. Comparison of recurrent esotropia and consecutive exotropia with horizontal muscle reoperation in infantile esotropia. Jpn J Ophthalmol. 2018;62:693–8.
Ganesh A, Pirouznia S, Ganguly SS, Fagerholm P, Lithander J. Consecutive exotropia after surgical treatment of childhood esotropia: a 40-year follow-up study. Acta Ophthalmol. 2011;89:691–5.
Bloom JN, Parks MM. The etiology, treatment and prevention of the “slipped muscle”. J Pediatr Ophthalmol Strabismus. 1981;18:6–11.
Parks MM, Bloom JN. The “slipped” muscle. Ophthalmology 1979;86:1389–96.
Ludwig H. Scar remodeling after strabismus surgery. Trans Am Ophthalmol Soc. 1999;97:583–651.
Ryu WY, Kim ST, Roh MS. Postoperative muscle migration through stretched scar formation after superior rectus muscle nonscleral sutured resection in rabbit eyes. J Pediatr Ophthalmol Strabismus. 2019;56:254–60.
Hatt SR, Leske DA, Jung JH, Holmes JM. Intraoperative findings in consecutixotropia with and without adduction deficit. Ophthalmology. 2017;124:828–34.
Negishi T, Hikoya A, Isoda H, Tsuchiya Y, Sawada M, Hotta Y, et al. Magnetic resonance imaging of the medial rectus muscle of patients with consecutive exotropia after medial rectus muscle recession. Ophthalmology. 2010;117:1876–82.
Akbari MR, Hassanpoor N, Aghsaei Fard M, Nozarian Z, Yaseri M, Mirmohammadsadeghi A. Clinical and Histopathologic Features of Consecutive Exotropia. Strabismus. 2018;26:84–9.
Parsa CF, Soltan-Sanjari M & Guyton DL. Non-absorbable sutures should be used for adjustable inferior rectus muscle [Internet]. In: Jan-Tjeerd De Faber, editors. 29th European Strabismological Association Meeting. CRC Press; London, England; 2003. p. 115–20.
Ludwig IH, Chow AY. Scar remodeling after strabismus surgery. J AAPOS. 2000;4:326–33.
Awadein A, Marsh JD, Guyton DL. Nonabsorbable versus absorbable sutures in large, hang-back medial rectus muscle recessions. J Am Assoc Pediatr Ophthalmol Strabismus. 2016;20:206–9.
Acknowledgements
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Author information
Authors and Affiliations
Contributions
All authors contributed to the study conception and design. Material preparation, data collection and analysis were performed by BD-P, YM, AE-L, EP and MEH. The first draft of the manuscript was written by BD-P, YM and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethical considerations
The study was approved by the Shamir Medical Centre Studies Institutional Review Board and adhered to the tenets of the declaration of Helsinki.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Dubinsky-Pertzov, B., Einan-Lifshitz, A., Pras, E. et al. Routine use of non-absorbable sutures in bi-medial rectus recession as a measure to reduce the incidence of consecutive exotropia. Eye 36, 1772–1776 (2022). https://doi.org/10.1038/s41433-021-01724-6
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01724-6
