
Abstract
Objectives
To investigate the differences in lncRNAs expression in whole blood between diabetic retinopathy (DR) patients and healthy subjects, and to evaluate the potential value of lncRNAs as a diagnostic biomarker for proliferative diabetic retinopathy (PDR).
Methods
A series of 34 PDR patients, 34 patients with non-proliferative DR (NPDR) and 34 healthy participants were enroled. Differentially expressed lncRNAs were demonstrated using high-throughput sequencing and validated using qRT-PCR. Gene Ontology (GO) was performed to explore the possible biological function of the differentially expressed lncRNAs. lncRNA/mRNA coexpression network was built to determine the targets of differentially expressed lncRNAs. Receiver operating characteristic (ROC) analysis was utilized to evaluate the diagnostic value of lncRNAs for PDR.
Results
We identified 175 and 179 differentially expressed lncRNAs in PDR patients compared with control samples and NPDR patients, respectively. GO analysis showed that the various metabolic processes were possibly influenced by these dysregulated lncRNAs. Using the differently expressed lncRNAs data, we further identified 82 overlapping lncRNAs in PDR patients with NPDR and control subjects. Part of these overlapping lncRNAs was significantly correlated with nuclear factor kappa B (NF-κB) and Wnt signal pathways. ROC curves were constructed for two upregulated lncRNAs and the ROC analysis indicated that both of them had potential diagnostic value and could distinguish PDR from control subjects and NPDR patients.
Conclusions
LncRNAs expression was altered in PDR patients compared with NPDR and control subjects. Moreover, it provides a resource that lncRNAs might be novel diagnostic and prognostic biomarker for PDR.
Similar content being viewed by others


Introduction
Diabetic retinopathy (DR) is a common complication of diabetes mellitus (DM), which affect ~30% of all diabetic patients [1]. It is classified into non-proliferative DR (NPDR) and proliferative DR (PDR). The retinopathy progresses with the duration of DM, nearly 80% of patients with DM developed DR and 20% of them developed PDR after 15 years of diagnosis [2, 3]. As the disease progresses to PDR, severe visual loss usually happens due to vitreous haemorrhages, tractional retinal detachment and neovascular glaucoma. Although the clinical characteristics of DR are well established and several risk factors for its progression are identified, the exact molecular and biochemical mechanisms remain poorly understood [4, 5]. Considering the prevalence of DM in adults aged 20–79 years is forecast to increase to 10.4% in 2040, the global burden caused by DR will be huge, especially in China [6, 7]. It is essential to explore new methods to early detect and monitor DR progression, which with more high sensitivity and specificity.
Recently, a novel class of transcripts called long noncoding RNAs (lncRNAs), which are pervasively transcribed in the genome, is gaining more attention because of their potential regulatory roles in the progression and prevention of DM. LncRNAs is a class of noncoding RNAs with transcript lengths > 200 nucleotides, which exert an increasingly important role in regulating various biological processes (BP) and influence a significant portion of cellular functionality [8, 9]. A number of studies have proved that lncRNAs participate in the pathogenesis of DM and its related complications, such as DR and diabetic kidney disease [10,11,12,13,14]. Although several studies have been performed to assess the role of lncRNAs in the development of DR, most of them focused on lncRNA expressed in tissues of animal models [15]. To date, few researchers have focused on the lncRNAs’ expression in DR patients and the contribution of lncRNAs to DR development has not been conclusively defined.
The molecular mechanisms underlying DR are complex and an improved understanding of the molecular mechanisms, by which lncRNAs perform their functions and interactions in DR, will provide potential biomarkers and new therapeutic targets for DR treatment [12]. Our previous study has proved that conbercept treatment can change the expression profiles of lncRNAs and mRNAs in the fibrovascular membranes of PDR patients and lncRNAs may contribute to novel therapeutic for PDR [16]. We hypothesized that lncRNAs may be used as a biomarker for diagnosis and prognosis of PDR. Therefore, we performed this study to investigate the differences in lncRNAs expression in whole blood between DR patients and healthy subjects, and to evaluate the possibility of these lncRNAs to serve as diagnostic biomarkers and potential therapeutic targets for PDR treatment.
Methods
Patients’ samples
This cross-sectional study was approved by the Ethical Review Committee of the Second Hospital of Shandong University and was performed according to the provisions of the Declaration of Helsinki for research involving human subjects and written informed consent was obtained from all patients in this study prior to enrolment. The whole blood samples were prospectively collected from 102 patients with type 2 diabetes at different stages of DR (NPDR and PDR) and age-matched healthy participants who undergoing routine cataract surgery at the Second Hospital of Shandong University from March 2019 to October 2019. All of the patients with diabetes were diagnosed according to the criteria of the American Diabetes Association [17]. Patients with the following conditions were excluded: (1) any other ocular disease, high myopia, glaucoma, retinal diseases or history of previous ocular surgery, with the exception of mild cataract, (2) severe systemic diseases, such as malignant tumour, metabolic syndrome not including type 2 diabetes and ongoing infection or autoimmune diseases and (3) PDR patients who received laser or anti-vascular endothelial growth factor (VEGF) treatment within 1 month were also excluded. All the participants received comprehensive ophthalmic evaluation, including best corrected visual activity, intraocular pressure, slit lamp examination, colour fundus photographs and dilated fundus examination by indirect ophthalmoscopy (+90 D). DR was graded as NPDR and PDR according to findings observable on dilated ophthalmoscopy by two ophthalmologists (BL and CC) based on the International Clinical Diabetic Retinopathy Disease Severity Scales [18]. Any discrepancies were resolved by a fundus expert (JW). A standard questionnaire was used to collect past medical history regarding DM, including the date of confirmed diagnosis, current use of medications and treatment history of DR.
The peripheral blood (5 ml) was collected in PAXgene blood RNA tubes (Qiagen) on the first day of admission before any treatment had been implemented and stored at −80 °C in aliquots until further use.
RNA extraction and quality control
Total RNA was isolated from the whole blood using TRIzol reagent (Invitrogen, Carlsbad, CA, USA), according to the manufacturer’s protocol. RNA integrity was evaluated using standard denaturing agarose gel electrophoresis and RNA concentration in each sample was assessed at an OD260/280 using a NanoDrop ND-2000 instrument (Thermo, Waltham, MA, USA).
High-throughput sequencing and analysis
High-throughput sequencing was provided by CloudSeq Biotech Inc. (Shanghai, China) as standard processes [19, 20]. Briefly, total RNA was used for removing the rRNAs using Ribo-Zero rRNA Removal Kits (Illumina, USA) following the manufacturer’s instructions. RNA libraries were constructed by using rRNA-depleted RNAs with TruSeq Stranded Total RNA Library Prep Kit (Illumina, USA) according to the manufacturer’s instructions. Libraries were controlled for quality and quantified using the BioAnalyzer 2100 system (Agilent Technologies, USA). Ten picomolar libraries were denatured as single-stranded DNA molecules, captured on Illumina flow cells, amplified in situ as clusters and finally sequenced for 150 cycles on Illumina HiSeq Sequencer according to the manufacturer’s instructions.
The high-quality reads were aligned to the human reference genome (UCSC HG19) with hisat2 software. Then, guided by the Ensembl gtf gene annotation file, cuffdiff software (part of cufflinks) was used to get the values of fragments per kilobase per million (FPKM) as the expression profiles of LncRNAs, and fold change and P value were calculated based on FPKM. Differentially expressed LncRNA were identified by T test between two groups. Any lncRNAs exhibiting fold changes ≥ 2.0 with adjust P value ≤ 0.15 were considered as having a significant and differentially expressed lncRNAs. LncRNA target genes were predicted by the locations to nearby genes.
Validation of candidate lncRNAs using quantitative real-time reverse-transcription polymerase chain reaction (qRT-PCR)
qRT-PCR was used to validate the expression levels of the candidate lncRNAs as we previously reported [16]. In brief, total RNA samples were reverse-transcribed into cDNA and subjected to qRT-PCR on an Applied Biosystems 7500 Fast Real-Time PCR System, in accordance with the manufacturer’s instructions. Triplicate measurements were obtained for each sample. The results were normalized with human GAPDH. The expression levels were analysed by the comparative Ct method. PCR primers are listed in Table 1.
Gene Ontology (GO) analysis for differentially expressed LncRNAs
GO analysis was used to explore the possible biological function of the differentially expressed lncRNAs. GO analysis included three parts: biological processes (BP), cellular components and molecular functions. The significant GO terms were determined using the Fisher’s exact test, and FDR was utilized to correct the P values. A P value < 0.05 was deemed statistically significant.
Construction of the lncRNA–mRNA coexpression network
To determine the functions of differentially expressed lncRNAs, an lncRNA/mRNA coexpression network was built according to the normalized signal intensities of differentially expressed lncRNAs and mRNAs. For each lncRNA–mRNA pair, the Pearson correlation was calculated to identify significantly correlated pairs. The Pearson correlation value cutoff was =0.95, P < 0.05. lncRNA–mRNA coexpression network was visualized using Cytoscape (version 2.8.0).
Statistical analysis
SPSS software (version20; SPSS Inc., Chicago, IL, USA) was used for statistical analysis. Statistical graph was performed by GraphPad Prism 5. Student’s t test or Mann–Whitney test was used, as appropriate, to compare two groups of independent samples. For categorical variables, we performed the Fisher’s exact test or the chi-square test. Receiver operating characteristic (ROC) analysis was utilized to evaluate the diagnostic value of lncRNAs in PDR patients compared to NPDR patients and healthy volunteers. A P value < 0.05 was considered statistically significant. Data for continuous variables were expressed as mean ± standard deviation (SD).
Results
Clinical characteristics of subjects
Overall, 34 patients with PDR, 34 patients with NPDR and 34 age-matched healthy participants were enroled for analysis in our study. The clinical characteristics of the patients, including age, gender, duration of DM, the level of FPG and HbAc1 and the number of antidiabetic drugs, are shown in Table 2. Compared with the NPDR, the PDR patients showed longer duration of DM, higher HbAc1 and higher number of antidiabetic drugs. The flowchart of the study design was presented in Fig. 1.

There were two phases in our project: sequencing phase and validation phase.
Differentially expressed lncRNAs in PDR and GO analysis
We analysed the transcriptome of peripheral whole blood. The expression patterns differed significantly between PDR and control samples. Using a two-fold expression difference as a cutoff, a total of 175 lncRNAs (80 upregulated, 94 downregulated, P < 0.05) were specifically dysregulated in PDR compared with control samples (Fig. 2, Supplementary File S1). We next performed GO analysis to better understand the functional association of target genes with the differentially expressed lncRNAs. The results showed that the BP most influenced by the dysregulated lncRNAs were various metabolic processes, such as cellular response to stress, regulation of histone deacetylation, regulation of protein deacetylation and protein monoubiquitination. More importantly, gene enrichment analysis showed that Wnt signalling pathway and NF-kappa B transcription factor activity might be directly or indirectly regulated by the downregulated lncRNAs (Fig. 3).

A Heatmap from the hierarchical clustering analysis showed the differential expressed lncRNAs between the two groups. Red represents upregulation and green represent downregulation. B Volcano plot indicating upregulated and downregulated lncRNAs in PDR group compared with control group.

Molecular function (MF), Biological process (BP) and Cellular component (CC) of lncRNAs‐targeted mRNAs.
We also performed differential expression analysis for PDR and NPDR samples. Similarly, a total of 179 lncRNAs were differentially expressed (83 upregulated, 93 downregulated, P < 0.05) (Fig. 4, Supplementary File S2). The results of GO analysis were shown in Fig. 5. Their function with regard to BP was determined to be regulation of tumour necrosis factor production, regulation of Wnt signalling pathway, interleukin-1-mediated signalling pathway, etc.

A Heatmap from the hierarchical clustering analysis showed the differential expressed lncRNAs between the two groups. Red represents upregulation and green represent downregulation. B Volcano plot indicating upregulated and downregulated lncRNAs in PDR group compared with NPDR group.

Molecular function (MF), Biological process (BP) and Cellular component (CC) of lncRNAs‐targeted mRNAs.
Construction of the lncRNA–mRNA coexpression network
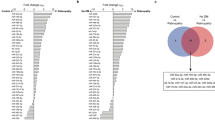
Using the differently expressed lncRNA data, we identified 81 overlapping lncRNAs (37 upregulated and 44 downregulated) in PDR patients with NPDR and control subjects (Fig. 6, Supplementary File S3). In order to investigate the potential function of these overlapping lncRNAs, we constructed our lncRNA–mRNA coexpression network. The results showed the relationships between these aberrantly expressed lncRNAs and mRNAs and we found that part of these overlapping lncRNAs were significantly correlated with nuclear factor kappa B (NF-κB) and Wnt signal pathways, which have been generally acknowledged as critical role in the pathogenesis of PDR (Fig. 7).

A Venn diagram of the overlapping number of upregulated lncRNAs in PDR patients with NPDR and control subjects. B Venn diagram of the overlapping number of downregulated lncRNAs in PDR patients with NPDR and control subjects.

Red dots indicate that lncRNA expression is upregulated and green dots indicate downregulation.
Validation of the differentially expressed lncRNAs
Four upregulated and four downregulated lncRNAs were selected randomly from the overlapping lncRNAs for validation purposes. The qRT-PCR results indicated similar trends to our sequencing results (Fig. 8).

qRT-PCR experiments were conducted to verify the expression level of eight selected lncRNAs in the three groups. Bar represent mean ± SD. **p < 0.01, ***p < 0.001.
The diagnostic performance of blood lncRNAs for PDR patients
We then explored the diagnostic value of these validated lncRNAs in distinguishing PDR patients from NPDR and healthy populations. ROC curves were constructed for two upregulated lncRNAs (ENST00000505731 and NR-126161). Compared with the control subjects and NPDR, the ROC analysis indicated that the AUC values of ENST00000505731 were 0.880 (95% confidence interval: 0.7880–0.9720, specificity = 80.0%, sensitivity = 86.7%) and 0.857 (95% confidence interval: 0.7639–0.9505, specificity = 86.7%, sensitivity = 70%), respectively. ROC analysis for NR-126161 showed the similar result (Fig. 9). These results indicated that blood ENST00000505731 and NR-126161 had potential diagnostic value and could distinguish PDR from control subjects and NPDR patients.

A, C ENST00000505731 and NR-126161 differentiated between PDR and NPDR patients. B, D ENST00000505731 and NR-126161 differentiated between PDR and control subjects.
Discussion
As a late stage of DR, PDR is one of the most serious microvascular complications of DM and is the leading cause of blindness among working age adults worldwide [21]. A better understanding of the predictors of DR development may lead to more personalized treatment and help improve clinical outcomes. Although lncRNAs have been identified as minimally invasive biomarkers for diagnosis, prognosis or monitoring curative effects in various cancers, the diagnostic and prognostic values of lncRNAs in DR remain unclear [22]. In this study, we compared differential expression profiles of lncRNAs among PDR, NPDR and control subjects; our results suggested that lncRNAs could be new potential biomarkers to detect early and monitor DR progression in DM patients.
LncRNAs can be detected in different kinds of body fluid, such as aqueous humour (AH), vitreous humour (VH) and peripheral whole blood [13, 23, 24]. Because it is difficult to collect adequate volumes of AH and VH and it is impossible to obtain AH and VH samples from healthy living human eyes, we choose peripheral whole blood which is easy to obtain and with minimally invasive procedures in this study. After comparing PDR, NPDR and control groups, we found 82 differentially expressed lncRNAs (37 upregulated and 45 downregulated) and the results were validated by qRT-PCR. Most of the differentially expressed lncRNAs in this study were not reported before. In order to reveal the potential functions of the lncRNAs in this study, we next performed a GO analysis and found that their biological functions were mainly involved in the canonical Wnt signalling pathway and regulation of NF-κB transcription factor activity, which are related to retinal neovascularization.
The canonical Wnt signalling pathway is a well-known, evolutionarily conserved pathway comprised of Wnts, frizzled receptors and co-receptors. It plays important roles in many ocular diseases, including DR [25]. VEGF is a major pro-angiogenic factor in physiological and pathological angiogenesis and has been identified as a downstream target gene of canonical Wnt signalling. It is correlated with the severity of DR and involved in the pathogenesis of PDR. Previous study reported that activation of Wnt signalling increases VEGF levels in the retina of diabetic animal models, while suppression of Wnt signalling downregulates the expression of VEGF. Furthermore, the canonical Wnt signalling pathway can also participate in the pathogenesis of DR by mediating oxidative stress and inflammation. Recent researches show that many lncRNAs can influence a variety of cellular functionalities, such as cell apoptosis, proliferation and migration, via the Wnt signalling pathway [26]. In order to reveal the potential relationship between these dysregulated lncRNAs and the Wnt signalling pathway, we constructed an lncRNA–mRNA coexpression network and found that many differentially expressed lncRNAs may be involved in the regulation of the Wnt signalling pathway.
Because lncRNAs can modulate multiple targets at the transcriptional and post-transcriptional levels, lncRNAs tend to play functional roles in more than one biological pathway [27]. In current study, the results of the lncRNA–mRNA coexpression network revealed that many differentially expressed lncRNAs are possibly involved in Wnt and NF-κB pathways. NF-ĸB is a master regulator of various genes involved in inflammation, angiogenesis, cell proliferation and apoptosis. It can be activated by hypoxia, bacteria, viral proteins, various cytokines and trophic factors. NF-ĸB activation plays a key role in the development and progression of DR [28]. It was observed that increased activation of NF-κB has a significant link with increased VEGF expression in both NPDR and PDR subjects. Activation of NF-κB was shown to promote expression of pro-inflammatory cytokines and various pro-apoptotic regulators in retinal endothelial cells, and ultimately lead to retinal vessel dysfunction and DR progression [29]. Moreover, selective inhibition of NF-κB activation can inhibit diabetes-induced retinal leukostasis and retinal expressions of ICAM-1 and VEGF in vivo. Therefore, we hypothesized that these differentially expressed lncRNAs may possibly influence the progression of diabetes through the regulation of Wnt and NF-κB pathways [30]. These information might help us to explore the underlying mechanisms of lncRNAs involved in the development of DR.
A good biomarker should be highly sensitive and specific. LncRNAs are expressed in a cell type-, tissue-, developmental stage- or disease state-specific pattern, making them good candidates for disease-specific biomarkers [31]. In this study, the ROC curves were constructed for top two upregulated lncRNAs, and the results indicated that these two lncRNAs had high sensitivity to discriminate PDR patients from NPDR patients and controls and could serve as new potential biomarkers for predicting and diagnosing PDR.
There are several limitations to our study that need to be considered. First, the number of patients participated in this study is small. Despite the small sample size, the results demonstrated statistically significant so that the small number of patients may only serve to strengthen the results in this study. Second, a referral bias may exist because all patients were recruited from a single centre. Finally, the possibility that a variety of medications applied, laser treatment and the use of anti-VEGF may have affected the expression profiles of lncRNAs in both PDR and NPDR patients. Therefore, a multicentre clinical study with larger cohorts may be warranted in future.
In conclusion, our findings indicated that lncRNAs might be novel biomarkers for early diagnosis and prognosis evaluation of diabetic patients with PDR. Further studies are still needed to completely elucidate the biological functions of these genes and to confirm the molecular mechanisms on the development of PDR.
Summary
What was known before
-
A number of studies have proved that lncRNAs participate in the pathogenesis of DM and its related complications, such as DR and diabetic kidney disease. Although several studies have been performed to assess the role of lncRNAs in the development of DR, most of them focused on lncRNA expressed in tissues of animal models. To date, few researchers have focused on the lncRNAs’ expression in DR patients and the contribution of lncRNAs to DR development has not been conclusively defined.
What this study adds
-
Our findings indicated that lncRNAs might be novel biomarkers for early diagnosis and prognosis evaluation of diabetic patients with PDR.
References
Wong TY, Cheung CM, Larsen M, Sharma S, Simó R. Diabetic retinopathy. Nat Rev Dis Primers. 2016;2:16012.
Varma R, Paz SH, Azen SP, Klein R, Globe D, Torres M, et al. The Los Angeles Latino Eye Study: design, methods, and baseline data. Ophthalmology. 2004;111:1121–31.
Varma R, Torres M, Peña F, Klein R, Azen SP, Los Angeles Latino Eye Study Group. Prevalence of diabetic retinopathy in adult Latinos: the Los Angeles Latino Eye Study. Ophthalmology. 2004;111:1298–306.
Fenwick EK, Xie J, Man R, Sabanayagam C, Lim L, Rees G, et al. Combined poor diabetes control indicators are associated with higher risks of diabetic retinopathy and macular edema than poor glycemic control alone. PLoS ONE. 2017;12:e0180252.
Stratton IM, Kohner EM, Aldington SJ, Turner RC, Holman RR, Manley SE, et al. UKPDS 50: risk factors for incidence and progression of retinopathy in type II diabetes over 6 years from diagnosis. Diabetologia. 2001;44:156–63.
Ogurtsova K, da Rocha Fernandes JD, Huang Y, Linnenkamp U, Guariguata L, Cho NH, et al. IDF Diabetes Atlas: global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res Clin Pr. 2017;128:40–50.
Zhong Y, Wu J, Yue S, Zhang G, Liu L, Chen L. Burden of diabetic retinopathy in mainland China: protocol for an updated systematic review and meta-analysis of prevalence and risk factors to identify prevention policies. Medicine. 2018;97:e13678.
Kapranov P, Cheng J, Dike S, Nix DA, Duttagupta R, Willingham AT, et al. RNA maps reveal new RNA classes and a possible function for pervasive transcription. Science. 2007;316:1484–8.
Mirza AH, Kaur S, Pociot F. Long non-coding RNAs as novel players in β cell function and type 1 diabetes. Hum Genom. 2017;11:17.
Biswas S, Sarabusky M, Chakrabarti S. Diabetic retinopathy, lncRNAs, and inflammation: a dynamic, interconnected network. J Clin Med. 2019;8:1033.
Galvan DL, Green NH, Danesh FR. The hallmarks of mitochondrial dysfunction in chronic kidney disease. Kidney Int. 2017;92:1051–7.
Gong Q, Su G. Roles of miRNAs and long noncoding RNAs in the progression of diabetic retinopathy. Biosci Rep. 2017;37:BSR20171157.
Thomas AA, Biswas S, Feng B, Chen S, Gonder J, Chakrabarti S. lncRNA H19 prevents endothelial-mesenchymal transition in diabetic retinopathy. Diabetologia. 2019;62:517–30.
Yan B, Tao ZF, Li XM, Zhang H, Yao J, Jiang Q. Aberrant expression of long noncoding RNAs in early diabetic retinopathy. Investig Ophthalmol Vis Sci. 2014;55:941–51.
Liu JY, Yao J, Li XM, Song YC, Wang XQ, Li YJ, et al. Pathogenic role of lncRNA-MALAT1 in endothelial cell dysfunction in diabetes mellitus. Cell Death Dis. 2014;5:e1506.
Wang J, Gao X, Liu J, Wang J, Zhang Y, Zhang T, et al. Effect of intravitreal conbercept treatment on the expression of long noncoding RNAs and mRNAs in proliferative diabetic retinopathy patients. Acta Ophthalmol. 2019;97:e902–12.
Chamberlain JJ, Rhinehart AS, Shaefer CF Jr, Neuman A. Diagnosis and management of diabetes: synopsis of the 2016 American Diabetes Association Standards of Medical Care in Diabetes. Ann Intern Med. 2016;164:542–52.
Wilkinson CP, Ferris FL 3rd, Klein RE, Lee PP, Agardh CD, Davis M, et al. Proposed international clinical diabetic retinopathy and diabetic macular edema disease severity scales. Ophthalmology. 2003;110:1677–82.
Lu Q, Gong W, Wang J, Ji K, Sun X, Xu C, et al. Analysis of changes to lncRNAs and their target mRNAs in murine jejunum after radiation treatment. J Cell Mol Med. 2018;22:6357–67.
Xu TP, Wang WY, Ma P, Shuai Y, Zhao K, Wang YF, et al. Upregulation of the long noncoding RNA FOXD2-AS1 promotes carcinogenesis by epigenetically silencing EphB3 through EZH2 and LSD1, and predicts poor prognosis in gastric cancer. Oncogene. 2018;37:5020–36.
Cheung N, Mitchell P, Wong TY. Diabetic retinopathy. Lancet. 2010;376:124–36.
Evans JR, Feng FY, Chinnaiyan AM. The bright side of dark matter: lncRNAs in cancer. J Clin Investig. 2016;126:2775–82.
Botti G, Marra L, Malzone MG, Anniciello A, Botti C, Franco R, et al. LncRNA HOTAIR as prognostic circulating marker and potential therapeutic target in patients with tumor diseases. Curr Drug Targets. 2017;18:27–34.
Wang X, Chang X, Zhang P, Fan L, Zhou T, Sun K. Aberrant expression of long non-coding RNAs in newly diagnosed type 2 diabetes indicates potential roles in chronic inflammation and insulin resistance. Cell Physiol Biochem. 2017;43:2367–78.
Wang Z, Liu CH, Huang S, Chen J. Wnt Signaling in vascular eye diseases. Prog Retin Eye Res. 2019;70:110–33.
Zarkou V, Galaras A, Giakountis A, Hatzis P. Crosstalk mechanisms between the WNT signaling pathway and long non-coding RNAs. Noncoding RNA Res. 2018;3:42–53.
Kung JT, Colognori D, Lee JT. Long noncoding RNAs: past, present, and future. Genetics. 2013;193:651–69.
Duraisamy AJ, Mishra M, Kowluru A, Kowluru RA. Epigenetics and regulation of oxidative stress in diabetic retinopathy. Investig Ophthalmol Vis Sci. 2018;59:4831–40.
Lamoke F, Shaw S, Yuan J, Ananth S, Duncan M, Martin P, et al. Increased oxidative and nitrative stress accelerates aging of the retinal vasculature in the diabetic retina. PLoS ONE. 2015;10:e0139664.
Nagai N, Izumi-Nagai K, Oike Y, Koto T, Satofuka S, Ozawa Y, et al. Suppression of diabetes-induced retinal inflammation by blocking the angiotensin II type 1 receptor or its downstream nuclear factor-kappaB pathway. Investig Ophthalmol Vis Sci. 2007;48:4342–50.
Boon RA, Jaé N, Holdt L, Dimmeler S. Long noncoding RNAs: from clinical genetics to therapeutic targets. J Am Coll Cardiol. 2016;67:1214–26.
Funding
This study was supported by the National Natural Science Foundation of China (81700831), Beijing Bethune Charitable Foundation (BJ-LM2018003J) and the Key R&D plan of Shandong Province (2019GSF108081).
Author information
Authors and Affiliations
Contributions
All authors conceived of and designed the experimental protocol and read and approved the final manuscript. CC, YM, YHM and HZ collected the data. BL and JW were involved in the analysis and interpretation of the data. BL wrote the first draft of the manuscript. JW and HZ reviewed and revised the manuscript and produced the final version.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare no competing interests.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Liu, B., Cong, C., Ma, Y. et al. Potential value of lncRNAs as a biomarker for proliferative diabetic retinopathy. Eye 36, 575–584 (2022). https://doi.org/10.1038/s41433-021-01507-z
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-021-01507-z
