
Abstract
Background
Ophthalmic emergencies comprise a significant portion of junior doctors’ workload in accident and emergency (A&E). However, previous studies have demonstrated a lack of training and confidence in the management of such emergencies. This study assessed changes in basic ophthalmic training that A&E junior doctors received in dealing with eye emergencies, their perceived level of confidence and the availability of appropriate ophthalmic equipment in A&E over the last 15 years.
Methods
A prospective, national, combined online and telephone survey using a previously published questionnaire was performed. Foundation year two doctors (FY2s) from each A&E department in the UK listed on the official NHS directory were contacted for participation.
Results
Two hundred and ten A&E departments were contacted and 202 responded (response rate of 96.2%). There was no significant change in the number of A&E departments equipped with slit lamps (82.5% in 2003 vs 79.7% in 2018; p = 0.26). However, the prevalence of training in its use has decreased significantly (68.4% in 2003 vs 52% in 2018; p = 0.005). There was also a significant reduction in the prevalence of training in the management of eye emergencies (77.4% in 2003 vs 45.5% in 2018; p < 0.001) and the proportion of FY2s who felt confident in dealing with such cases (36.1% in 2003 vs 6% in 2018; p < 0.001).
Conclusion
There is a concerning decline in basic ophthalmic training for A&E FY2s, reflected by the alarmingly low level of confidence in the management of eye emergencies. This highlights an urgent need to improve ophthalmic training for junior doctors in A&E.
Similar content being viewed by others

Introduction
Ophthalmic emergencies comprise of a significant portion of the workload in general accident and emergency (A&E) departments [1,2,3], accounting for about 6% of new casualty attendances [4]. Most of these (~69%) are minor in nature and can be managed adequately by non-ophthalmic doctors [4]. With annual attendance numbers for emergency eye care only set to increase in the future [5], the effective management of ophthalmic emergencies by non-ophthalmologists in general A&E departments plays a major role in reducing pressure on dedicated ophthalmic A&E departments and hospital eye services.
Due to the ever-increasing demands on A&E departments in the UK, most patients with eye problems are often seen by junior doctors [6, 7], a significant proportion of which consists of foundation year two doctors [FY2s, previously known as senior house officers (SHOs)] [8]. Despite the importance of junior doctors in this regard, two previous national surveys (1993 and 2003) have demonstrated a concerning lack of training and confidence in the management of eye emergencies amongst this cohort [9, 10].
A number of changes have been introduced since, perhaps most notably Modernising Medical Careers (MMC), a nationwide system introduced in 2005 to facilitate a more competency-based training programme for junior doctors [11]. It was hoped that these changes would serve as a platform to improve ophthalmic training and confidence for future generations of A&E doctors [10]. However, to date, there has been no study assessing the change in ophthalmic training and competence amongst A&E junior doctors since the most recent survey in 2003. The need for a national survey has also been echoed by the ophthalmology community in recent years [8, 12]. The main aim of this study was therefore to investigate if any changes have occurred over the last 15 years.
Methods
A prospective, combined online and telephone survey of all the A&E departments in the UK listed on the official National Health Service (NHS) directory was conducted [13,14,15,16]. This project was deemed exempt from NHS Research Ethics Committee review by the Imperial College London Joint Research Compliance Office. FY2s who were currently working in A&E departments were contacted for participation via social media and e-mail through foundation programme coordinators of individual UK foundation schools. Following this, two follow-up reminders were sent at a fortnightly interval to non-responding A&E departments. Remaining non-responding departments despite online reminders were subsequently contacted by telephone up to four times to improve response rate. Telephone surveys were conducted using a standardised interview script and participants were asked to provide answers over the phone. No additional assistance was provided. This survey was conducted over a 2-month period (October and November 2018) to ensure that all the FY2s had been in their A&E post for at least a month following the national annual changeover in August.
A 14-item questionnaire, adapted with slight modifications from a previously published version, was used (see Appendix 1) [9]. In brief, questions served to ascertain the level of training A&E FY2s receive with regard to management of ophthalmic emergencies, their self-perceived level of confidence in managing such cases and the availability of appropriate diagnostic equipment in A&E departments. Three additional questions about direct ophthalmoscopy were also added to the original questionnaire to explore its availability, training and FY2s’ confidence in its use. The main exclusion criteria were: (1) paediatric A&E departments, (2) A&E departments with a separate, dedicated eye casualty and (3) those that did not offer training posts for foundation doctors at the time of the survey. Data analysis was performed using IBM SPSS Statistics for Windows, version 23 (IBM Corp., Armonk, NY, USA). Data comparison with that of previous surveys was done using χ2 tests, with Bonferroni correction where appropriate.
Results
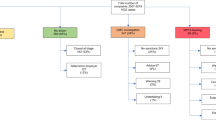
Two hundred and forty-seven A&E departments were identified from the official online NHS directory. After application of the exclusion criteria, 210 were contacted and 202 responded (response rate of 96.2%).
A total of 346 FY2s participated in the national survey, with a minimum of one FY2 per A&E department. Of these, 310 (87.6%) responded to the online survey and 36 (13.4%) to the follow-up telephone survey. Table 1 gives the full details and the results of the questionnaire used.
To allow comparison with the results of the previous surveys in 1993 and 2003 [9, 10], the response of one FY2 from each A&E department was chosen by selecting the first responder for each hospital (n = 202). Table 2 provides a summary and comparison of the main results from the 1993, 2003 and 2018 surveys.
Significant differences were detected for all the main results between the three surveys (Table 2). Post hoc analysis showed a significant reduction in the prevalence of training in the management of eye emergencies [45.5% in 2018 vs 77.4% in 2003 (p < 0.001) and 74% in 1993 (p < 0.001)] and proportion of A&E SHOs/FY2s who felt confident in the management of eye emergencies [6% in 2018 vs 36.1% in 2003 (p < 0.001) and 31.2% in 1993 (p < 0.001).
Although there was a significant increase in the availability of slit lamps since 1993 (79.7% in 2018 vs 57.8% in 1993; p < 0.001), no similar change was detected for the last 15 years (79.7% in 2018 vs 74.4% in 2003; p = 0.26). The prevalence of slit lamp teaching has significantly reduced since 2003 (52% in 2018 vs 68.4% in 2003; p = 0.003), approaching the level of that in 1993 (52% in 2018 vs 47.4% in 1993; p = 0.36). The proportion of A&E SHOs/FY2s who felt confident using the slit lamp has also seen a significant reduction [10.4% in 2018 vs 39.1% in 2003 (p < 0.001) and 27.6% in 1993 (p < 0.001)]. There was also a significant, stepwise decline in the proportion of A&E SHOs/FY2s who saw ≥3 eye cases on an average working day [31.2% in 2018 vs 45.1% in 2003 (p = 0.01) and 59.9% in 1993 (p < 0.001)].
Discussion
The demand for general A&E services have been rising steadily—by nearly half a million annually—for more than a decade since 2004 [17]. In addition to a growing and ageing population, the increasing demand for A&E services has also been attributed to a change in health seeking behaviour that occurred around the time [18]. The latter was mainly blamed on the change in the general practice (GP) out-of-hours contract in 2004 from which 90% of GP practices opted to sacrifice £6000 salary in order to give up responsibility for out-of-hours services, leading to the axing of a crucial provider of emergency care outside general A&E departments.
As ophthalmic emergencies account for a significant proportion (~6%) of the general A&E workload, the rise in the numbers of patients with such conditions will inevitably mirror that of general A&E attendances. This is indirectly corroborated by the increase in the numbers attending large dedicated walk-in eye casualty units over the last decade [5]. Based on first-hand anecdotal and published evidence, most patients with eye problems in general A&E departments in the UK are seen and managed by junior doctors, of which FY2s account for a significant proportion of the workforce [8].
Our follow-up survey in 2018 has demonstrated a worrying decline since 2003. In the 15 years that have passed, there has been a considerable reduction in the level of training that FY2s receive in the management of eye emergencies, with only less than half receiving some form of training during their time in A&E. Perhaps even more alarmingly is the drastic drop in confidence in the management of eye emergencies among this cohort, with more than 90% of FY2s reporting little or no confidence.
Despite the specific changes introduced by MMC in 2005, notably a competency-based Foundation Programme, these have not resulted in any improvement in the training and management of ophthalmic emergencies by A&E FY2s. Indeed, concerns have been raised about the inflexibility of MMC, with it being criticised as being a more rigid training system that often conflicted with the programme’s stated aims [19]. Nonetheless, the observed decline in our study is likely to be complex and multifactorial, involving local, regional and nationwide factors.
An important factor at a local level is undoubtedly the lack of exposure in medical school. Multiple studies have shown that medical students in the UK receive variable and often inadequate ophthalmic training, most of which does not meet the recommended International Council of Ophthalmologists standard [20,21,22,23]. At a regional level, this is further compounded by the lack of formal structured teaching for A&E junior doctors (as corroborated by our results), often owing to time constraints and fragmentation of rotas [12]. In addition, there is no clear definition of the baseline core ophthalmic competencies required of junior doctors in foundation training [12]. On a national level, there is evidence to suggest that the reduction of working hours and transition to a shift system via the implementation of European Working Time Directive in 2004 has impeded training for doctors [24,25,26]. This is also exacerbated by the increasing pressures on NHS services, which have been shown to have negatively impact junior doctors’ education and training [27].
There appears to be a gradual decline over the last 25 years in the number of eye cases seen by A&E junior doctors, as corroborated by the observed stepwise decline in the proportion of A&E FY2s/SHOs who saw ≥3 eye cases on an average working day in our study. Interestingly, a similar trend for non-ophthalmological conditions in general A&E has been demonstrated, with junior A&E doctors being recorded as seeing 17% fewer patients per hour over a 3-year period [28]. Reasons for this are likely to be multifold, with previous studies reporting factors such as general A&E junior doctors being slower and more cautious than before [28] and higher proportions of patients being managed entirely by nurse practitioners [29].
Although this study found an overall good access to and training in the use of direct ophthalmoscopy (a topic not explored by previous surveys), there was a concerning lack of confidence in its use with about 90% of FY2s reporting such an issue. This is not surprising given a similar climate reported in undergraduates [30, 31]. Given the fact that direct ophthalmoscopy is considered a fundamental competency of the Foundation Programme [32], our results may further attest the need for more strategic emphasis on direct ophthalmoscopy training for foundation doctors. Nonetheless, it should be recognised that there is still ongoing debate with mixed views from the ophthalmology community on the value of teaching direct ophthalmoscopy to non-ophthalmologists [33,34,35,36,37,38].
The main limitation of this study is the risk of overestimation of the scale of the problem. The comparison between SHOs previously and FY2s presently is likely to be unfair as the previous “SHO” definition likely included a wider range of training grade doctors who might feel more confident managing eye emergencies due to greater experience and more time in A&E. A&E experience for FY2s, by contrast, will commonly be limited to a single 4 month placement. Conversely, it is also possible that our findings have merely captured the “tip of the iceberg” and underestimate the true scale of the problem as other grades of A&E junior doctors were excluded. Future studies could administer the same survey to investigate if similar issues exist within other groups of primary care practitioners (e.g. GPs and community optometrists) at the forefront of emergency eye care. Given the emergence of nurse practitioners as independent frontline staff, it would be of interest to explore the scale of the shift from doctors to this cohort in the provision of emergency eye care in general A&E departments over the last few decades. Qualitative approaches via focus group interviews could also be employed to provide an in-depth understanding about junior doctors’ perception of the management of ophthalmic emergencies.
A continuation of this state of decline among A&E FY2s will have major implications for both general and dedicated ophthalmic A&E departments and may well perpetuate the decrease in training efforts, under-confidence in managing patients with eye conditions and lack of resources needed to support the real-world burden of eye disease looming just over the horizon. There is an urgent need for concerted and sustained efforts at a local, regional and national level to improve the situation. This should begin at the level of undergraduate education, for instance by embedding critical ophthalmic material and skills (e.g. slit lamp use) into the popular integrative multidisciplinary outcomes-based teaching model, thus complementing other disciplines and positively impacting patient care. On a wider scale, there is a need to push forward an agenda of higher investment in resources and innovative organisational changes to improve ophthalmic training for junior doctors in the UK.
Summary
What was known before
Ophthalmic conditions are generally approached with much apprehension by junior doctors in the A&E department.
This is corroborated by previous national surveys that have demonstrated a consistent lack of confidence and training in the management of ophthalmic emergencies among this cohort.
What this study adds
There has been a worrying decline since the last national survey; only less than half of FY2s in A&E received training in the management of eye emergencies.
But perhaps more concerning is the alarmingly low confidence in the management of eye emergencies among this cohort, with more than 90% A&E FY2s reporting little or no confidence.
References
Jones NP, Hayward JM, Khaw PT, Claoué CM, Elkington AR. Function of an ophthalmic “accident and emergency” department: results of a six month survey. Br Med J. 1986;292:188–90.
Vernon SA, Do MB. Analysis of all new cases seen in a busy regional centre ophthalmic casualty department during 24-week period. J R Soc Med. 1983;76:279–82.
Chiapella A, Rosenthal A. One year in an eye casualty clinic. Br J Ophthalmol. 1985;69:865–70.
Edwards RS. Ophthalmic emergencies in a district general hospital casualty department. Br J Ophthalmol. 1987;71:938–42.
Smith HB, Daniel CS, Verma S. Eye casualty services in London. Eye. 2013;27:320–8.
Bhopal RS, Parkin DW, Gillie RF, Han KH. Pattern of ophthalmological accidents and emergencies presenting to hospitals. J Epidemiol Community Health. 1993;47:382–7.
Ezra DG, Mellington F, Cugnoni H, Westcott M. Reliability of ophthalmic accident and emergency referrals: a new role for the emergency nurse practitioner? Emerg Med J. 2005;22:696–9.
Murray PI, Benjamin M, Oyede O. Can general A&E doctors manage common eye emergencies. Eye. 2016;30:1399–400.
Tan MM, Driscoll PA, Marsden JE. Management of eye emergencies in the accident and emergency department by senior house officers: a national survey. Emerg Med J. 1997;14:157–8.
Sim DA, Hussain A, Tebbal A, Daly S, Pringle E, Ionides A, et al. National survey of the management of eye emergencies in the accident and emergency departments by senior house officers: 10 years on - has anything changed? Emerg Med J. 2008;25:76–7.
Wall D. Curriculum for the foundation years in postgraduate education and training. Med Teach. 2005;27:298–301.
Ah-Kee EY, Scott RA, Shafi A, McCabe G, Lim LT. Are junior doctors in today’s NHS competent in managing ophthalmic cases in the emergency department. Eye. 2016;30:164.
NHS England. A-Z list of all nhs acute (hospital) trusts in England. NHS England; 2019. https://www.nhs.uk/servicedirectories/pages/nhstrustlisting.aspx. Accessed 8 Sep 2019.
NHS Wales. Health in Wales | hospitals. NHS Wales; 2019. http://www.wales.nhs.uk/ourservices/directory/Hospitals. Accessed 8 Sep 2019.
NHS Scotland. Scotland’s Service Directory. NHS Scotland; 2019. https://www.nhsinform.scot/scotlands-service-directory/aes-and-minor-injuries-units. Accessed 8 Sep 2019.
NHS Northern Ireland. Emergency healthcare | Nidirect. NHS Northern Ireland; 2019. https://www.nidirect.gov.uk/articles/emergency-healthcare. Accessed 8 Sep 2019.
The King’s Fund. Are accident and emergency attendances increasing? The King’s Fund; 2013. https://www.kingsfund.org.uk/blog/2013/04/are-accident-and-emergency-attendances-increasing. Accessed 8 Sep 2019.
The Royal College of Ophthalmologists. The way forward: emergency eye care. The Royal College of Ophthalmologists; 2017. https://www.rcophth.ac.uk/wp-content/uploads/2015/10/RCOphth-The-Way-Forward-Emergency-Eye-Care-300117.pdf. Accessed 8 Sep 2019.
House of Commons Health Committee. Modernising medical careers: third report of session 2007–08 Volume I. London: The House of Commons; 2008. https://publications.parliament.uk/pa/cm200708/cmselect/cmhealth/25/25i.pdf. Accessed 8 Sep 2019.
Baylis O, Murray PI, Dayan M. Undergraduate ophthalmology education – a survey of UK medical schools. Med Teach. 2011;33:468–71.
Welch S, Eckstein M. Ophthalmology teaching in medical schools: a survey in the UK. Br J Ophthalmol. 2011;95:748–9.
Hill S, Dennick R, Amoaku W. Present and future of the undergraduate ophthalmology curriculum: a survey of UK medical schools. Int J Med Educ. 2017;8:389–95.
Sheth T, Thia B, Wong N. The state of ophthalmic education in medical schools: a UK perspective. MedEdPublish. 2018;7:45.
Anwar M, Irfan S, Daly N, Amen F. EWTD has negative impact on training for surgeons. BMJ. 2005;331:1476.
O’Gallagher MK, Lewis G, Mercieca K, Moutray T, Ophthalmic Trainees' Group of the Royal College of Ophthalmologists. The impact of the European Working Time Regulations on ophthalmic specialist training – a national trainee survey. Int J Surg. 2013;11:837–40.
Ipsos MORI. The impact of the implementation of the European Working Time Directive (EWTD): a qualitative research report prepared for the General Medical Council (GMC). London: Ipsos MORI; 2011.
General Medical Council. The state of medical education and practice in the UK report. General Medical Council; 2015. www.gmc-uk.org/publications/somep2015.asp. Accessed 8 Sep 2019.
Armstrong PAR, White AL, Thakore S. Reduced productivity among junior trainees in the emergency department and the impact on senior clinicians. Emerg Med J. 2010;27:97–9.
Bhatt R, Sandramouli S. Evidence-based practice in acute ophthalmology. Eye. 2006;21:976.
Wu EH, Fagan MJ, Reinert SE, Diaz JA. Self-confidence in and perceived utility of the physical examination: a comparison of medical students, residents, and faculty internists. J Gen Intern Med. 2007;22:1725–30.
Gupta RR, Lam W-C. Medical students’ self-confidence in performing direct ophthalmoscopy in clinical training. Can J Ophthalmol. 2006;41:169–74.
UK Foundation Programme Office. The Foundation Programme Curriculum. UK Foundation Programme Office; 2016. https://www.foundationprogramme.nhs.uk/sites/default/files/2018-07/Curriculum_0.pdf. Accessed 8 Sep 2019.
Yusuf IH, Salmon JF, Patel CK. Direct ophthalmoscopy should be taught to undergraduate medical students—yes. Eye. 2015;29:987.
Purbrick RMJ, Chong NV. Direct ophthalmoscopy should be taught to undergraduate medical students—No. Eye. 2015;29:990.
Imonikhe RJ, Finer N, Gallagher K, Plant G, Bremner FD, Acheson JF. Direct ophthalmoscopy should be taught to undergraduate medical students. Eye. 2015;30:497.
Orlans HO. Direct ophthalmoscopy should be taught within the context of its limitations. Eye. 2015;30:326.
Hill SCL, Jawaid I, Amoaku W. Response to: ‘direct ophthalmoscopy should be taught to undergraduate medical students’. Eye. 2015;30:327.
Jawaid I, Hill SCL, Amoaku WM. Direct ophthalmoscopy should be taught to undergraduate medical students. Eye. 2015;30:326.
Author information
Authors and Affiliations
Contributions
PYS was involved in conception and design of the study. PYS, CJL, JT and JH were involved in data acquisition, analysis and interpretation. PYS was involved in first draft of the manuscript. PYS, CJL, JT and JH were involved in revising and critically appraising the manuscript. PYS, CJL, JT and JH were involved in final approval for publication. PYS and JH are guarantors.
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Rights and permissions
About this article

Cite this article
Sim, P.Y., La, C.J., Than, J. et al. National survey of the management of eye emergencies in the accident and emergency department by foundation doctors: has anything changed over the past 15 years?. Eye 34, 1094–1099 (2020). https://doi.org/10.1038/s41433-019-0645-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-019-0645-2
This article is cited by
-
The burden of flashes and floaters in traditional general emergency services and utilization of ophthalmology on-call consultation: a cross-sectional study
BMC Ophthalmology (2022)
-
Assessing the subjective quality of smartphone anterior segment photography: a non-inferiority study
International Ophthalmology (2022)
