
Abstract
Purpose
Obstructive sleep apnea (OSA) is associated with many systemic diseases including diabetes, hypertension, stroke, and cardiovascular disease. The aim of our study was to investigate the association between OSA and optic neuropathy (ON), and to evaluate the efficacy of treatment for OSA on the risk of ON.
Methods
We used the data from the Longitudinal Health Insurance Database, which involved one million insurants from Taiwan National Health Insurance program (Taiwan NHI).
Results
OSA patients had a 1.95-fold higher risk of ON compared with non-OSA patients in all age group. The risk was significantly higher (adjusted hazard ratio: 4.21) in the group aged <45 years and male individuals (adjusted hazard ratio: 1.93). Meanwhile, sleep apnea was associated with ON regardless of the existence of comorbidity or not. OSA patients treated with continuous positive airway pressure (CPAP) had an adjusted 2.31-fold higher hazard of developing ON compared to controls, and those without any treatment had an adjusted 1.82-fold higher hazard of developing ON compared to controls. Moreover, ON patients had a 1.45-fold higher risk of OSA, and those aged between 45 and 64 years (hazard ratio: 1.76) and male individuals (hazard ratio: 1.55) had highest risk.
Conclusions
Our study showed that OSA increased the risk of developing ON after controlling the comorbidities; however, treatment with CPAP did not reduce the risk of ON. Further large population study accessing to medical records about the severity of OSA and treatment for OSA is needed to clarify the efficacy of treatment for OSA in reducing the risk of ON.
Similar content being viewed by others

Introduction
Obstructive sleep apnea (OSA) is characterized by intermittent complete (apnea) or partial (hypopnea) upper airway obstruction during sleep. The repeated episodes of apnea/hypopnea cause cessation of breathing, hypoxia, and contribute to production of reactive oxidative species, inflammation, and promote vascular endothelial damage [1, 2]. Individuals with OSA usually present with snoring at nighttime, fatigue, and somnolence at daytime. The definite diagnosis of OSA is made by diagnostic overnight polysomnography. OSA severity is defined by the apnea (cessation of oro-nasal flow for 10 s)–hypopnea (reduced oro-nasal flow of >50% with a 4% oxygen desaturation) index (sum of apnea and hypopnea events/hour) as none (<5), mild (5–14.9), moderate (15–29.9), and severe (≥30). Risk factors for OSA include large neck circumference, craniofacial abnormalities, nasal obstruction, and increased pharyngeal tissue [3].
It was estimated that the prevalence of OSA was around 4% in middle-aged men, and 2% in middle-aged women (aged 30–60 years) in western country [4], 3.7% in Asian country [5], and 2.6% in Taiwan (3.4% for males and 1.9% for females; males <50 vs. >50 years: 2.3% vs. 5.3%; females <50 vs. >50 years: 1.4% vs. 2.8%) [6]. OSA is associated with increased risk of hypertension, stroke, coronary artery [7], cardiovascular disease [8], diabetes mellitus (DM) [9], autonomic disease [10], and vascular endothelial dysregulation [11, 12].
Accumulating evidences have shown that OSA was associated with ocular diseases such as floppy eyelid syndrome, dry eye syndrome, and central serous chorioretinopathy, as well as optic neuropathy (ON) including open-angle glaucoma, normal tension glaucoma, non-arteritic ischemic ON (NAION), papilledema, and idiopathic intracranial hypertension [13]. However, there are still some debates with regard to the relationship between sleep apnea and ON. Stein et al. [14] conducted a retrospective longitudinal cohort study to clarify the association between sleep apnea and ON including glaucoma using billing records for beneficiaries ≥40 years in the United States. The aim of our study was to investigate the risk of ON in individuals with OSA and the therapeutic effect of treatment for sleep apnea using National Database for beneficiaries ≥20 years in Taiwan.
Methods
Data source
To build this study, we used the data from the Longitudinal Health Insurance Database (LHID), which involved the one million insurants from Taiwan National Health Insurance program (Taiwan NHI). LHID contained the insurants’ claim data, including the registry of beneficiaries, disease registry record (wrote by the International Classification of Diseases, Ninth Revision, Clinical Modification (ICD-9-CM)), and other medical service. Taiwan government updated the data for LHID every year. The government released the database with de-identification for research. This study was also approved by the Ethics Review Board of China Medical University (CMUH104-REC2-115).
Study population
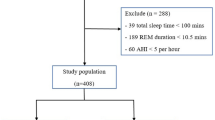
We investigated the association between OSA and ON and organized a population-based bidirectional cohort study design. We built two subcohort studies, an OSA vs. a non-OSA cohort to observe the ON (ICD-9-CM 377) occurrence and an ON vs. non-ON cohort to observe the risk of developing OSA. In the first subcohort study, the OSA cohort involved OSA patients (ICD-9-CM 327.23, 780.51, 780.53, and 780.57) with age >20 years from 2002 to 2010. The non-OSA cohort collected the individuals without OSA and was matched by age, sex, and age of OSA onset at 1:10 ratios. Both cohorts excluded the individuals who had the history of ON before the study. We followed up these two cohorts until the individuals were removed from the LHID, or they developed ON (ICD-9-CM 377) or until December 31, 2010. In the second cohort study, the ON cohort and the corresponding comparison cohort, was also selected from 2002 to 2010 and followed up until December 31, 2010, or individuals were withdrawn from the LHID or OSA occurrence. The corresponding comparison (non-ON subjects) was also matched by age, sex, and onset age of ON at 1:10 ratios. We excluded the subjects who had the OSA diagnosed before the study.
These two subcohort studies selected the same comorbidities, which included hypertension (ICD-9-CM 401-405), DM (ICD-9-CM 250), atherosclerosis (ICD-9-CM 440), coronary artery disease (CAD, ICD-9-CM 410-414), hyperlipidemia (ICD-9-CM 272), and migraine (ICD-9-CM 346). For OSA cohort, we also evaluated the effect of OSA management and divided into four groups: without management, treatment with continuous positive airway pressure (CPAP) only, treatment with surgery (laryngeal surgery or nasal surgery) only, and treatment with both CPAP and surgery.
Statistical analysis
To demonstrate the distribution between different cohorts, we counted the number and percentage of patients in each categories, such as sex and comorbidity, and calculated the mean and corresponding standard deviation (SD) for age. To test the distribution difference, t test was used for age and χ2 test for sex and comorbidities. The incidence density was calculated for the number of event as the numerator and sum of follow-up years as the denominator (per 10,000 person-years). To measure the risk of ON in OSA patients or risk of OSA in ON patients, the hazard ratios (HRs) and corresponding 95% confidence intervals (CIs) were estimated by using single variable and multivariable Cox proportional hazard models. All the data management and analysis were performed by SAS 9.4 software (SAS Institute, Cary, NC, USA). The significant level was set at <0.05 for two-side testing.
Results
Table 1 showed the character for the first subcohort study populations: OSA cohort and non-OSA cohort. The OSA cohort contained 5129 OSA patients and with 10-fold corresponding matched non-OSA comparisons. The mean age of two cohorts was 48 years and the percentage of the male was 65%. The listed comorbidities were more prevalent in OSA cohort than non-OSA cohort (p < 0.0001).
Table 2 demonstrated the risk of ON in the OSA patients. After adjusted for age, sex, hypertension, DM, atherosclerosis, CAD, hyperlipidemia, and migraine, the OSA patients had a nearly 1.95-fold significantly higher risk of ON than non-OSA individuals (HR = 1.95, 95% CI = 1.30–2.92). In the individuals with age <45 years, the risk of ON was nearly 4.21-fold greater for OSA patients than non-OSA group (HR = 4.21, 95% CI = 1.93–9.18). The male OSA patients also was significantly associated with higher risk of ON compared with male non-OSA individuals (HR = 1.93, 95% CI = 1.17–3.18). Compared with non-OSA cohort, the HRs of the ON risk were 2.85 (95% CI = 1.28–6.34) and 1.84 (95% CI = 1.16–2.91) for OSA patients without any comorbidity and with at least one comorbidity.
Table 3 showed the risk of ON among the non-OSA cohort and OSA patients with different management. After adjusting for potential confounding factors, the HRs of the ON risk were 1.82 (95% CI = 1.12–2.97), 2.31 (95% CI = 1.07–4.99), and 2.42 (95% CI = 0.88–6.62) for OSA patients without management, treated with CPAP only, and treated with surgery only, respectively, compared with non-OAS cohorts.
Table 4 showed the distribution of age, sex and comorbidities for the second subcohort populations, ON cohort and non-ON cohort. We enrolled 4143 ON patients, age (mean = 58 years) and sex-matched (male = 51.6%) 41,430 non-ON individuals. The percentage of comorbidities for ON cohort was higher than non-ON cohort (p < 0.0001).
Table 5 displayed the risk of OSA in ON patients compared with non-ON cohort. After controlling for age, sex, hypertension, DM, atherosclerosis, CAD, hyperlipidemia, and migraine, ON cohort had an overall 1.45-fold higher risk of OSA than non-ON cohort (HR = 1.45, 95% CI = 1.02–2.07). Compared with non-ON individuals, the ON patients were significantly associated with higher OSA risk only in those aged 45–64 years (HR = 1.76, 95% CI = 1.08–2.86). The male ON patients had a 1.55-fold higher risk of OSA than male non-ON individuals (HR = 1.55, 95% CI = 1.01–2.39). The HR of the OSA risk was 1.74 (95% CI = 1.17–2.58) for ON patients compared with non-ON individuals who had at least one comorbidity, but the risk of OSA was not statistically significant between two cohorts without any comorbidity (HR = 0.97, 95% CI = 0.42–2.22).
Discussion
Our study confirm previous studies and showed that OSA patients had a 1.95-fold higher risk of ON compared with non-OSA patients in all age groups. In particular, the risk was significantly higher (HR: 4.21) in the individuals at age <45 years and in male individuals (HR: 1.93). Meanwhile, sleep apnea was associated with ON regardless of the existence of comorbidity or not. Interestingly, Liguori and their associates performed electroretinogram (ERG) and visual-evoked potential (VEP) on severe OSA (apnea–hypopnea events/time in bed ≥30/h) patients without medical comorbidities and found that these OSA patients had an alteration of VEP with unaffected ERG as demonstrated by lower amplitude and longer latency of P100 component than healthy controls; they hypothesized that this subclinical optic nerve dysfunction could be caused by hypoxia, acidosis, and hypercarbia due to repetitive airway obstruction; they therefore reinforced the important role of OSA on optic nerve dysfunction [15]. In our study, we also looked at the hazard of developing OSA in ON patients and found that ON patients had a 1.45-fold higher risk of OSA compared with non-ON patients, and those aged between 45 and 64 years (HR: 1.76) and male individuals (HR: 1.55) had highest risk.
Recently, a meta-analysis study showed the pooled odds ratio of developing NAION in the subjects with OSA was 6.18 (95% CI=2.00–19.11) vs. non-OSA controls [16]. However, the association of OSA and glaucoma was still inconclusive [17], because of different criteria for diagnosis of OSA (apnea–hypopnea index (AHI) >5, >15, or >20) and different methods for assessment of glaucoma.
OSA was considered an important risk factor for the development of NAION [3, 18]. The prevalence of OSA in NAION patients varied according to different diagnosis methods. Li et al. [19] found that 30% of NAION patients had OSA by using Sleep Apnea Scale of Disorders Questionnaire for diagnosis of OSA. Mojon et al. [20] reported 71% of patients with NAION had OSA using respiratory disturbance index >10, and the prevalence of OSA was 55.6%, 85%, and 89% in NAION patients using AHI ≥20, >5, or >15, respectively [18, 21, 22].
Several mechanisms including direct OSA-induced hypoxia, OSA-related vascular dysregulation, and OSA-associated increased intracranial pressure and vasoactive substances (vascular endothelial growth factor and endothelin-1) have been proposed to be the pathophysiology of NAION [3].
The current standard treatment of OSA was CPAP, our study found OSA patients treated with CPAP had an adjusted 2.31-fold higher hazard of developing ON compared to controls, and those without any treatment had an adjusted 1.82-fold higher hazard of developing ON compared to controls. We do not know whether the OSA patients treated with CPAP had more severe OSA than those without treatment. In a large retrospective cohort study using billing records, individuals with OSA not receiving treatment of CPAP had a 1.41-fold higher risk of NAION relative to controls, and those with OSA treated with CPAP had a 1.96-fold higher risk of NAION relative to controls. However, this study showed that individuals diagnosed with OSA not receiving treatment with CPAP had a 16% increased hazard of developing NAION after controlling for confounding factors. Furthermore, there was no difference in hazard of experiencing NAION between individuals with OSA treated with CPAP and controls [14]. However, Behbehani et al. [23] found that some individuals treated with CPAP still did not prevent the development of NAION [23]. In our study, it is interesting that some OSA patients treated with surgery including oropharyngeal or nasal surgery had a 2.42-fold higher risk of ON compared to controls, but those treated with both surgery and CPAP had no difference in developing ON compared to controls.
Limitation of this study was that we cannot confirm the diagnosis of OSA and severity of OSA without access to medical records. Also, the diagnosis of NAION was made mostly by the neuro-ophthalmologists, and the incidence of NAION was usually underestimated. Given the low incidence of NAION, we used the diagnostic code (377: ON) to cover the two main ON including glaucomatous ON and ischemic ON, but the other ON could also be included. Moreover, OSA patients treated with CPAP did not have lower HR of developing ON compared to those without any treatment. Further large population study accessing to medical records about the severity of OSA and treatment for OSA are needed to clarify the efficacy of treatment for OSA in reducing the risk of ON.
Summary
What was known before
-
OSA was known for one of most important risk factors for ON including glaucoma and non-arteritic anterior ischemic ON.
What this study adds
-
This is the first study in Asia to investigate the association between sleep apnea and ON using National-wide population database.
References
Kohler M, Stradling JR. Mechanisms of vascular damage in obstructive sleep apnea. Nat Rev Cardiol. 2010;7:677–85.
Langenfeld MR, Simmons LA, McCrohon JA, Raitakari OT, Lattimore JD, Hennessy A, et al. Nitric oxide does not mediate the vasodilation of early human pregnancy. Heart Lung Circ. 2003;12:142–8.
Archer EL, Pepin S. Obstructive sleep apnea and nonarteritic anterior ischemic optic neuropathy: evidence for an association. J Clin Sleep Med. 2013;9:613–8.
Young T, Palta M, Dempsey J, Skatrud J, Weber S, Badr S. The occurrence of sleep-disordered breathing among middle-aged adults. N Engl J Med. 1993;328:1230–5.
Mirrakhimov AE, Sooronbaev T, Mirrakhimov EM. Prevalence of obstructive sleep apnea in Asian adults: a systematic review of the literature. BMC Pulm Med. 2013;13:10.
Chuang LP, Hsu SC, Lin SW, Ko WS, Chen NH, Tsai YH. Prevalence of snoring and witnessed apnea in Taiwanese adults. Chang Gung Med J. 2008;31:175–81.
Pepin JL, Tamisier R, Baguet JP, Levy P. Arterial health is related to obstructive sleep apnea severity and improves with CPAP treatment. Sleep Med Rev. 2013;17:3–5.
Shamsuzzaman AS, Gersh BJ, Somers VK. Obstructive sleep apnea: implications for cardiac and vascular disease. JAMA. 2003;290:1906–14.
Nagayoshi M, Punjabi NM, Selvin E, Pankow JS, Shahar E, Iso H, et al. Obstructive sleep apnea and incident type 2 diabetes. Sleep Med. 2016;25:156–61.
Woodson BT, Brusky LT, Saurajen A, Jaradeh S. Association of autonomic dysfunction and mild obstructive sleep apnea. Otolaryngol Head Neck Surg. 2004;130:643–8.
Lattimore JD, Celermajer DS, Wilcox I. Obstructive sleep apnea and cardiovascular disease. J Am Coll Cardiol. 2003;41:1429–37.
Levy P, Pepin JL, Arnaud C, Baguet JP, Dematteis M, Mach F. Obstructive sleep apnea and atherosclerosis. Prog Cardiovasc Dis. 2009;51:400–10.
McNab AA. The eye and sleep apnea. Sleep Med Rev. 2007;11:269–76.
Stein JD, Kim DS, Mundy KM, Talwar N, Nan B, Chervin RD, et al. The association between glaucomatous and other causes of optic neuropathy and sleep apnea. Am J Ophthalmol. 2011;152:989–.e983.
Liguori C, Palmieri MG, Pierantozzi M, Cesareo M, Romigi A, Izzi F, et al. Optic nerve dysfunction in obstructive sleep apnea: an electrophysiological study. Sleep. 2016;39:19–23.
Wu Y, Zhou L-M, Lou H, Cheng J-W, Wei R-L. The association between obstructive sleep apnea and nonarteritic anterior ischemic optic neuropathy: a systematic review and meta-analysis. Curr Eye Res. 2015;41:987–92.
Fraser CL. Obstructive sleep apnea and optic neuropathy: is there a link? Curr Neurol Neurosci Rep. 2014;14:465.
Bilgin G, Koban Y, Arnold AC. Nonarteritic anterior ischemic optic neuropathy and obstructive sleep apnea. J Neuro-Ophthalmol. 2013;33:232–4.
Li J, McGwin G Jr., Vaphiades MS, Owsley C. Non-arteritic anterior ischaemic optic neuropathy and presumed sleep apnoea syndrome screened by the Sleep Apnea scale of the Sleep Disorders Questionnaire (SA-SDQ). Br J Ophthalmol. 2007;91:1524–7.
Mojon DS, Hedges TR III, Ehrenberg B, Karam EZ, Goldblum D, Abou-Chebl A. et al. Association between sleep apnea syndrome and nonarteritic anterior ischemic optic neuropathy. Arch Ophthalmol. 2002;120:601–5.
Arda H, Birer S, Aksu M, Ismailogullari S, Karakucuk S, Mirza E, et al. Obstructive sleep apnoea prevalence in non-arteritic anterior ischaemic optic neuropathy. Br J Ophthalmol. 2013;97:206–9.
Palombi K, Renard E, Levy P, Chiquet C, Deschaux C, Romanet JP, et al. Non-arteritic anterior ischaemic optic neuropathy is nearly systematically associated with obstructive sleep apnoea. Br J Ophthalmol. 2006;90:879–82.
Behbehani R, Mathews MK, Sergott RC, Savino PJ. Nonarteritic anterior ischemic optic neuropathy in patients with sleep apnea while being treated with continuous positive airway pressure. Am J Ophthalmol. 2005;139:518–21.
Acknowledgements
This study was supported by Taiwan Ministry of Health and Welfare, Clinical Trial and Research Center of Excellence (MOHW105-TDU-B-212-133019); China Medical University Hospital and Academia Sinica Taiwan Biobank Stroke Biosignature Project (BM10501010037); NRPB Stroke Clinical Trial Consortium (MOST 104-2325-B-039 -005); and Tseng-Lien Lin Foundation, Taichung, Taiwan; Taiwan Brain Disease Foundation, Taipei, Taiwan as well as Katsuzo and Kiyo Aoshima Memorial Funds, Japan, respectively.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The authors declare that they have no conflict of interest.
Rights and permissions
About this article

Cite this article
Sun, MH., Liao, Y.J., Lin, CC. et al. Association between obstructive sleep apnea and optic neuropathy: a Taiwanese population-based cohort study. Eye 32, 1353–1358 (2018). https://doi.org/10.1038/s41433-018-0088-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41433-018-0088-1
