
Abstract
Background/Objectives
Most studies assessing the association between coffee consumption and hypertension ascertained caffeine intake in terms of number of cups per days, and yield mixed results. Although the inter-individuals variability in the caffeine metabolism is known, the relation of caffeine metabolites with hypertension remains unsettled. We examined the association of caffeine and 13 direct and indirect caffeine metabolites with hypertension in U.S. adults.
Methods
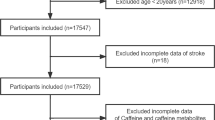
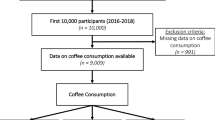
Using data from 2009–2010 National Health and Nutrition Examination Survey, we included 2278 individuals aged 18 to 80 years. Urinary methyluric acids (MU) and methylxanthines (MX) products of caffeine metabolism were measured using high performance liquid chromatography-electrospray ionization-tandem quadrupole mass spectrometry. We used multivariate logistic regression to model hypertension (systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥80 mmHg) as functions of urinary coffee metabolites.
Results
The odds of hypertension decreased across quartiles of 3-MU, 7-MU, 3-MX and 7-MX, with 7-MU being the more powerful metabolite. Compared with adults in the bottom quartile of 7-MU, the odds of hypertension decreased by 81% (95% CI: −90 to −22%) in those in the upper quartile. In contrast, the odds ratio for being hypertensive from the bottom to the upper quartile were 4.47 (95% CI: 1.21–16.50) for 1,3-dimethyluric acid, 4.45 (95% CI: 1.48–13.39) for 1,3-dimethylxanthine, and 5.08 (95% CI: 1.11–23.36) for 1,7-dimethylxanthine. Neither insulin resistance nor abdominal obesity were moderators in these associations.
Conclusions
Final metabolites of caffeine (namely 3-MU, 7-MU, 3-MX and 7-MX), but not caffeine, significantly reduce the odds for hypertension in this population.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout

Similar content being viewed by others

References
Roth GA, Johnson C, Abajobir A, Abd-Allah F, Abera SF, Abyu G. et al. Global, Regional, and National Burden of cardiovascular diseases for 10 causes, 1990 to 2015. J Am Coll Cardiol. 2017;70:1–25. https://doi.org/10.1016/j.jacc.2017.04.052.
Lopez AD, Mathers CD, Ezzati M, Jamison DT, Murray CJ. Global and regional burden of disease and risk factors, 2001: systematic analysis of population health data. Lancet. 2006;367:1747–57.
GBD 2013 Risk Factors Collaborators, Forouzanfar MH, Alexander L, Anderson HR, Bachman VF, Biryukov S, et al. Global, regional, and national comparative risk assessment of 79 behavioural, environmental and occupational, and metabolic risks or clusters of risks in 188 countries, 1990-2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386:2287–323. https://doi.org/10.1016/S0140-6736(15)00128-2.
Mills KT, Bundy JD, Kelly TN, Reed JE, Kearney PM, Reynolds K, et al. Global disparities of hypertension prevalence and control: A systematic analysis of population-based studies from 90 Countries. Circulation. 2016;134:441–50. https://doi.org/10.1161/CIRCULATIONAHA.115.018912.
Lewington S, Clarke R, Qizilbash N, Peto R, Collins R. Prospective Studies Collaboration. Age-specific relevance of usual blood pressure to vascular mortality: a meta-analysis of individual data for one million adults in 61 prospective studies. Lancet. 2012;360:1903–13.
Ford S. Trends in mortality from all causes and cardiovascular disease among hypertensive and nonhypertensive adults in the United States. Circulation. 2011;123:1737–44. https://doi.org/10.1161/CIRCULATIONAHA.110.005645.
USDA (United States Department of Agriculture USA), “Coffee: World Markets and Trade,” Unite States Dep. Agric., p. 9.
Zhang Z, Hu G, Caballero B, Appel L, Chen L. Habitual coffee consumption and risk of hypertension: a systematic review and meta-analysis of prospective observational studies. Am J Clin Nutr. 2011;93:1212–9. https://doi.org/10.3945/ajcn.110.004044.
Xie C, Cui L, Zhu J, Wang K, Sun N, Sun C. Coffee consumption and risk of hypertension: a systematic review and dose-response meta-analysis of cohort studies. J Hum Hypertens. 2018;32:83–93. https://doi.org/10.1038/s41371-017-0007-0.
D’Elia L, La Fata E, Galletti F, Scalfi L, Strazzullo P. Coffee consumption and risk of hypertension: a dose-response meta-analysis of prospective studies. Eur J Nutr. 2017. https://doi.org/10.1007/s00394-017-1591-z.
Gunes A, Dahl ML. Variation in CYP1A2 activity and its clinical implications: influence of environmental factors and genetic polymorphisms. Pharmacogenomics. 2008;9:625–37. https://doi.org/10.2217/14622416.9.5.625.
Zhou SF, Liu JP, Chowbay B. Polymorphism of human cytochrome P450 enzymes and its clinical impact. Drug Metab Rev. 2009;41:89–295. https://doi.org/10.1080/03602530902843483.
Klag MJ, Wang NY, Meoni LA, Brancati FL, Cooper LA, Liang KY, et al. Coffee intake and risk of hypertension: the Johns Hopkins precursors study. Arch Intern Med. 2002;162:657–62.
Winkelmayer WC, Stampfer MJ, Willett WC, Curhan GC. Habitual caffeine intake and the risk of hypertension in women. JAMA. 2005;294:2330–5.
Uiterwaal CS, Verschuren WM, Bueno-de-Mesquita HB, Ocké M, Geleijnse JM, Boshuizen HC, et al. Coffee intake and incidence of hypertension. Am J Clin Nutr. 2007;85:718–23.
Palatini P, Dorigatti F, Santonastaso M, Cozzio S, Biasion T, Garavelli G, et al. Association between coffee consumption and risk of hypertension. Ann Med. 2007;39:545–53.
Hu G, Jousilahti P, Nissinen A, Bidel S, Antikainen R, Tuomilehto J. Coffee consumption and the incidence of antihypertensive drug treatment in Finnish men and women. Am J Clin Nutr. 2007;86:457–64.
Grosso G, Stepaniak U, Polak M, Micek A, Topor-Madry R, Stefler D, et al. Coffee consumption and risk of hypertension in the Polish arm of the HAPIEE cohort study. Eur J Clin Nutr. 2016;70:109–15.
Rhee JJ, Qin F, Hedlin HK, Chang TI, Bird CE, Zaslavsky O, et al. Coffee and caffeine consumption and the risk of hypertension in postmenopausal women. Am J Clin Nutr. 2016;103:210–7.
Chei CL, Loh JK, Soh A, Yuan JM, Koh WP. Coffee, tea, caffeine, and risk of hypertension: The Singapore Chinese Health Study. Eur J Nutr. 2018;57:1333–42. https://doi.org/10.1007/s00394-017-1412-4.
Navarro AM, Martinez-Gonzalez MA, Gea A, Ramallal R, Ruiz-Canela M, Toledo E. Coffee concumption and risk of hypertension in the SUN Project. Clin Nutr. https://doi.org/10.1016/j.clnu.2017.12.009.
Guessous I, Pruijm M, Ponte B, Ackermann D, Ehret G, Ansermot N, et al. Associations of ambulatory blood pressure with urinary caffeine and caffeine metabolite excretions. Hypertension. 2015;65:691–6. https://doi.org/10.1161/HYPERTENSIONAHA.114.04512.
Loftfield E, Freedman ND, Dodd KW, Vogtmann E, Xiao Q, Sinha R, et al. Coffee drinking is widespread in the United States, but usual intake varies by key demographic and lifestyle factors. J Nutr. 2016;146:1762–8. https://doi.org/10.3945/jn.116.233940.
Whelton PK, Carey RM, Anorow WS, Casey DE Jr, Collins JK, Dennison Himmelfarb C, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71:1269–324. https://doi.org/10.1161/HYP.0000000000000066.
U.S. CDC National Health and Nutrition Examination Survey. http://www.cdc.gov/nchs/nhanes.htm. Accessed 14 May 2018.
Lelo A, Kjellen G, Birkett DJ, Miners JO. Paraxanthine metabolism in humans: determination of metabolic partial clearances and effects of allopurinol and cimetidine. J Pharm Exp Ther. 1989;248:315–9.
Smith PF, Smith A, Miners J, McNeil J, Proudfoot A. The safety aspects of dietary caffeine. Report from the Expert Working Group from the Australia New Zealand Food Authority (ANZFA), Australia. 2000.
Alsabri SG, Mari WO, Younes S, Alsadawi MA, Oroszi TL. Kinetic and Dynamic description of Caffeine. J Caffeine Adenosine Res. 2018;8. https://doi.org/10.1089/caff.2017.0011
U.S. CDC National Health and Nutrition Examination Survey. https://www.cdc.gov/nchs/data/nhanes/nhanes_09_10/CAFE_F_met.pdf. Accessed 24 May 2018.
U.S. CDC National Health and Nutrition Examination Survey. https://wwwn.cdc.gov/Nchs/Data/Nhanes/2015-6/Manuals/2015_Physician_Examination_Procedures_Manual.pdf. Accessed 15 May 2018.
Textor J, Hardt J, Knüppel S. DAGitty: A graphical tool for analyzing causal diagrams. Epidemiology. 2011;5:745. https://doi.org/10.1097/EDE.0b013e318225c2be.
Textor J, Liskiewicz M. Adjustment Criteria in Causal Diagrams: An Algorithmic Perspective. http://arxiv.org/ftp/arxiv/papers/1202/1202.3764.pdf. Accessed 24 May 2018.
Hanley AJ, Williams K, Stern MP, Haffner SM. Homeostasis model assessment of insulin resistance in relation to the incidence of cardiovascular disease: The San Antonio Heart Study. Diabetes Care. 2002;25:1177–84.
U.S.CDC. Centers for Disease Control and Prevention (CDC) National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey. Hyattsville, MD: U.S: Department of Health and Human Services, Centers for Disease Control and Prevention. 2018. https://www.cdc.gov/nchs/data/nhanes/nhanes_09_10/labcomp_f.pdf. Accessed 8 Jan 2019.
U.S.CDC. Centers for Disease Control and Prevention (CDC) National Center for Health Statistics (NCHS). National Health and Nutrition Examination Survey. Hyattsville, MD: U.S: Department of Health and Human Services, Centers for Disease Control and Prevention. Serum, Plasma and Urine specimens. 2018. https://www.cdc.gov/nchs/nhanes/biospecimens/serum_plasma_urine.htm. Accessed 8 Jan 2019.
Lancaster T, Muir J, Silagy C. The effects of coffee on serum lipids and blood pressure in a UK population. J R Soc Med. 1994;87:506–7.
Stensvold I, Tverdal A, Foss OP. The effect of coffee on blood lipids and blood pressure. Results from a Norwegian cross-sectional study, men and women, 40–42 years. J Clin Epidemiol. 1989;42:877–84.
Lopez-Garcia E, van Dam RM, Willett WC, Rimm EB, Manson JE, Stampfer MJ, et al. Coffee consumption and coronary heart disease in men and women: a prospective cohort study. Circulation. 2006;113:2045–53.
Liu HH, Cao YX, Li S, Guo YL, Zhu CG, Wu NQ, et al. Impacts of prediabetes mellitus alone or plus hypertension on the coronary severity and cardiovascular outcomes. Hypertension. 2018;71:1039–46. https://doi.org/10.1161/HYPERTENSIONAHA.118.11063.
Martínez-López S, Beatriz Sarriá B, Baeza G, Mateos R, Bravo-Clemente L. Pharmacokinetics of caffeine and its metabolites in plasma and urine after consuming a soluble green/roasted coffee blend by healthy subjects. Food Res Int. 2014;64:125–33. https://doi.org/10.1016/j.foodres.2014.05.043.
Nurminen ML, Niittynen L, Korpela R, Vapaatalo H. Coffee, caffeine and blood pressure: a critical review. Eur J Clin Nutr. 1999;53:831–9.
Hartley TR, Sung BH, Pincomb GA, Whitsett TL, Wilson MF, Lovallo WR. Hypertension risk status and effect of caffeine on blood pressure. Hypertension. 2000;36:137–41.
Kaminsky LA, Martin CA, Whaley MH. Caffeine consumption habits do not influence the exercise blood pressure response following caffeine ingestion. J Sports Med Phys Fit. 1998;38:53–58.
Conde SV, Nunes da Silva T, Gonzalez C, Mota Carmo M, Monteiro EC, Guarino MP. Chronic caffeine intake decreases circulating catecholamines and prevents diet-induced insulin resistance and hypertension in rats. Br J Nutr. 2012;107:86–95. https://doi.org/10.1017/S0007114511002406.
Ohnishi A, Branch RA, Jackson K, Hamilton R, Biaggioni I, Deray G, et al. Chronic caffeine administration exacerbates renovascular, but not genetic, hypertension in rats. J Clin Invest. 1986;78:1045–50.
Acknowledgements
This research was supported by a grant from the Canadian Institute of Health Research (CIHR) (#146885) to GN.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Conflict of interest
The author declares that he has no conflict of interest.
Additional information
Publisher’s note: Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Ngueta, G. Caffeine and caffeine metabolites in relation to hypertension in U.S. adults. Eur J Clin Nutr 74, 77–86 (2020). https://doi.org/10.1038/s41430-019-0430-0
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41430-019-0430-0
