
Abstract
Background
The efficacy and added benefit of platinum-based chemotherapy (PtCT) for metastatic breast cancer (MBC) remain unclear in patients with and without germline BRCA1 or BRCA2 mutations (gBRCA1/2m and gBRCA1/2wt, respectively).
Methods
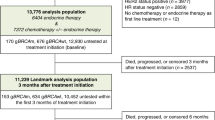
We selected from the French national real-world multicentre ESME cohort (2008–2016) all patients with HER2-negative MBC with known gBRCA1/2 status at first-line chemotherapy initiation. Using multivariable Cox models, we compared the outcome (progression-free (PFS) and overall survival (OS)) of first-line PtCT and non-PtCT regimens based on the patients’ gBRCA1/2 status and tumour subtype.
Results
Patients who received PtCT had more aggressive tumour features. In the multivariable analysis, first-line PtCT was associated with better adjusted PFS and OS in gBRCA1/2m carriers (N = 300), compared with non-PtCT (HR 0.54, 95% CI 0.4–0.73, P < 0.001, and HR 0.70, 95% CI 0.49–0.99, P = 0.047, respectively). Conversely, outcomes were similar in gBRCA1/2wt patients (N = 922) treated with PtCT and non-PtCT, whatever the tumour subtype. Landmark analyses at months 3 and 6 post treatment initiation supported these results.
Conclusions
In this pre-PARP inhibitor real-world cohort, PFS and OS were better after PtCT than non-PtCT in patients with gBRCA1/2m, but not in those with gBRCA1/2wt. These results emphasise the need of early gBRCA1/2 testing in patients with MBC.
Clinical trial number
NCT03275311.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 24 print issues and online access
$259.00 per year
only $10.79 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others


Data availability
The data presented in this study are available on reasonable request from the corresponding author.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
Engel C, Fischer C. Breast cancer risks and risk prediction models. Breast Care. 2015;10:7–12.
Armstrong N, Ryder S, Forbes C, Ross J, Quek RG. A systematic review of the international prevalence of BRCA mutation in breast cancer. Clin Epidemiol. 2019;11:543–61.
Dent R, Trudeau M, Pritchard KI, Hanna WM, Kahn HK, Sawka CA, et al. Triple-negative breast cancer: clinical features and patterns of recurrence. Clin Cancer Res. 2007;13:4429–34.
Elias AD. Triple-negative breast cancer: a short review. Am J Clin Oncol. 2010;33:637–45.
Lakhani SR, Van De Vijver MJ, Jacquemier J, Anderson TJ, Osin PP, McGuffog L, et al. The pathology of familial breast cancer: predictive value of immunohistochemical markers estrogen receptor, progesterone receptor, HER-2, and p53 in patients with mutations in BRCA1 and BRCA2. J Clin Oncol. 2002;20:2310–8.
Stevens KN, Vachon CM, Couch FJ. Genetic susceptibility to triple-negative breast cancer. Cancer Res. 2013;73:2025–30.
Song Y, Barry WT, Seah DS, Tung NM, Garber JE, Lin NU. Patterns of recurrence and metastasis in BRCA1/BRCA2-associated breast cancers. Cancer. 2020;126:271–80.
Carey LA, Dees EC, Sawyer L, Gatti L, Moore DT, Collichio F, et al. The triple negative paradox: primary tumor chemosensitivity of breast cancer subtypes. Clin Cancer Res. 2007;13:2329–34.
Deluche E, Antoine A, Bachelot T, Lardy-Cleaud A, Dieras V, Brain E, et al. Contemporary outcomes of metastatic breast cancer among 22,000 women from the multicentre ESME cohort 2008-2016. Eur J Cancer. 2020;129:60–70.
Turner N, Tutt A, Ashworth A. Hallmarks of ‘BRCAness’ in sporadic cancers. Nat Rev Cancer. 2004;4:814–19.
Liu X, Palma J, Kinders R, Shi Y, Donawho C, Ellis PA, et al. An enzyme-linked immunosorbent poly(ADP-ribose) polymerase biomarker assay for clinical trials of PARP inhibitors. Anal Biochem. 2008;381:240–7.
Helleday T, Petermann E, Lundin C, Hodgson B, Sharma RA. DNA repair pathways as targets for cancer therapy. Nat Rev Cancer. 2008;8:193–204.
Sikov WM, Berry DA, Perou CM, Singh B, Cirrincione CT, Tolaney SM, et al. Impact of the addition of carboplatin and/or bevacizumab to neoadjuvant once-per-week paclitaxel followed by dose-dense doxorubicin and cyclophosphamide on pathologic complete response rates in stage II to III triple-negative breast cancer: CALGB 40603 (Alliance). J Clin Oncol. 2015;33:13–21.
Loibl S, O’Shaughnessy J, Untch M, Sikov WM, Rugo HS, McKee MD, et al. Addition of the PARP inhibitor veliparib plus carboplatin or carboplatin alone to standard neoadjuvant chemotherapy in triple-negative breast cancer (BrighTNess): a randomised, phase 3 trial. Lancet Oncol. 2018;19:497–509.
Loibl S, Weber KE, Timms KM, Elkin EP, Hahnen E, Fasching PA, et al. Survival analysis of carboplatin added to an anthracycline/taxane-based neoadjuvant chemotherapy and HRD score as predictor of response-final results from GeparSixto. Ann Oncol. 2018;29:2341–7.
Hahnen E, Lederer B, Hauke J, Loibl S, Krober S, Schneeweiss A, et al. Germline mutation status, pathological complete response, and disease-free survival in triple-negative breast cancer: secondary analysis of the geparsixto randomized clinical trial. JAMA Oncol. 2017;3:1378–85.
Poggio F, Bruzzone M, Ceppi M, Ponde NF, La Valle G, Del Mastro L, et al. Platinum-based neoadjuvant chemotherapy in triple-negative breast cancer: a systematic review and meta-analysis. Ann Oncol. 2018;29:1497–508.
Wang D, Feng J, Xu B. A meta-analysis of platinum-based neoadjuvant chemotherapy versus standard neoadjuvant chemotherapy for triple-negative breast cancer. Future Oncol. 2019;15:2779–90.
Pandy JGP, Balolong-Garcia JC, Cruz-Ordinario MVB, Que FVF. Triple negative breast cancer and platinum-based systemic treatment: a meta-analysis and systematic review. BMC Cancer. 2019;19:1065.
Garutti M, Pelizzari G, Bartoletti M, Malfatti MC, Gerratana L, Tell G, et al. Platinum salts in patients with breast cancer: a focus on predictive factors. Int J Mol Sci. 2019;20:3390.
Tutt A, Tovey H, Cheang MCU, Kernaghan S, Kilburn L, Gazinska P, et al. Carboplatin in BRCA1/2-mutated and triple-negative breast cancer BRCAness subgroups: the TNT Trial. Nat Med. 2018;24:628–37.
Cardoso F, Paluch-Shimon S, Senkus E, Curigliano G, Aapro MS, Andre F, et al. 5th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 5). Ann Oncol. 2020;31:1623–49.
Lesueur F, Mebirouk N, Jiao Y, Barjhoux L, Belotti M, Laurent M, et al. GEMO, a national resource to study genetic modifiers of breast and ovarian cancer risk in BRCA1 and BRCA2 pathogenic variant carriers. Front Oncol. 2018;8:490.
Harvey JM, Clark GM, Osborne CK, Allred DC. Estrogen receptor status by immunohistochemistry is superior to the ligand-binding assay for predicting response to adjuvant endocrine therapy in breast cancer. J Clin Oncol. 1999;17:1474–81.
Allison KH, Hammond MEH, Dowsett M, McKernin SE, Carey LA, Fitzgibbons PL, et al. Estrogen and progesterone receptor testing in breast cancer: ASCO/CAP guideline update. J Clin Oncol. 2020;38:1346–66.
Wolff AC, Hammond MEH, Allison KH, Harvey BE, Mangu PB, Bartlett JMS, et al. Human epidermal growth factor receptor 2 testing in breast cancer: American society of clinical oncology/college of American pathologists clinical practice guideline focused update. J Clin Oncol. 2018;36:2105–22.
Litton JK, Hurvitz SA, Mina LA, Rugo HS, Lee KH, Goncalves A, et al. Talazoparib versus chemotherapy in patients with germline BRCA1/2-mutated HER2-negative advanced breast cancer: final overall survival results from the EMBRACA trial. Ann Oncol. 2020;31:1526–35.
Robson M, Im SA, Senkus E, Xu B, Domchek SM, Masuda N, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N Engl J Med. 2017;377:523–33.
Robson ME, Tung N, Conte P, Im SA, Senkus E, Xu B, et al. OlympiAD final overall survival and tolerability results: olaparib versus chemotherapy treatment of physician’s choice in patients with a germline BRCA mutation and HER2-negative metastatic breast cancer. Ann Oncol. 2019;30:558–66.
Dieras V, Han HS, Kaufman B, Wildiers H, Friedlander M, Ayoub JP, et al. Veliparib with carboplatin and paclitaxel in BRCA-mutated advanced breast cancer (BROCADE3): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet Oncol. 2020;21:1269–82.
Egger SJ, Willson ML, Morgan J, Walker HS, Carrick S, Ghersi D, et al. Platinum-containing regimens for metastatic breast cancer. Cochrane Database Syst Rev. 2017;6:CD003374.
Metzger-Filho O, Collier K, Asad S, Ansell PJ, Watson M, Bae J, et al. Matched cohort study of germline BRCA mutation carriers with triple negative breast cancer in brightness. npj Breast Cancer. 2021;7:142.
Tung N, Robson ME, Ventz S, Santa-Maria CA, Nanda R, Marcom PK, et al. TBCRC 031: randomized phase II study of neoadjuvant cisplatin versus doxorubicin-cyclophosphamide in germline BRCA carriers with HER2-negative breast cancer (the INFORM trial). J Clin Oncol. 2020;38:1539–48.
Jacot W, Heudel PE, Fraisse J, Gourgou S, Guiu S, Dalenc F, et al. Real-life activity of eribulin mesylate among metastatic breast cancer patients in the multicenter national observational ESME program. Int J Cancer. 2019;145:3359–69.
Delaloge S, Perol D, Courtinard C, Brain E, Asselain B, Bachelot T, et al. Paclitaxel plus bevacizumab or paclitaxel as first-line treatment for HER2-negative metastatic breast cancer in a multicenter national observational study. Ann Oncol. 2016;27:1725–32.
Carrick S, Parker S, Thornton CE, Ghersi D, Simes J, Wilcken N. Single agent versus combination chemotherapy for metastatic breast cancer. Cochrane Database Syst Rev. 2009;CD003372: https://doi.org/10.1002/14651858.CD003372.pub3.
Vos JR, Hsu L, Brohet RM, Mourits MJ, de Vries J, Malone KE, et al. Bias correction methods explain much of the variation seen in breast cancer risks of BRCA1/2 mutation carriers. J Clin Oncol. 2015;33:2553–62.
Geyer CE, Sikov WM, Huober J, Rugo HS, Wolmark N, O’Shaughnessy J, et al. Long-term efficacy and safety of addition of carboplatin with or without veliparib to standard neoadjuvant chemotherapy in triple-negative breast cancer: 4-year follow-up data from BrighTNess, a randomized phase III trial. Ann Oncol. 2022;33:384–94.
Schmid P, Cortes J, Dent R, Pusztai L, McArthur H, Kummel S, et al. Event-free survival with pembrolizumab in early triple-negative breast cancer. N Engl J Med. 2022;386:556–67.
Acknowledgements
We thank the 18 French Comprehensive Cancer Centers (Institut Curie, Paris and Saint-Cloud; Gustave Roussy, Villejuif; Institut Cancerologie de l’Ouest, Angers and Nantes; Centre Francois Baclesse, Caen; Institut du Cancer de Montpellier, Montpellier; Centre Leon Berard, Lyon; Centre Georges-Francois Leclerc, Dijon; Centre Henri Becquerel, Rouen; Institut Claudius Regaud, Toulouse; Centre Antoine Lacassagne, Nice; Institut de Cancerologie de Lorraine, Nancy; Centre Eugene Marquis, Rennes; Institut Paoli-Calmettes, Marseille; Centre Jean Perrin, Clermont Ferrand; Institut Bergonie, Bordeaux; Centre Paul Strauss, Strasbourg; Institut de Cancerologie Jean-Godinot, Reims; and Centre Oscar Lambret, Lille) for providing the data and each ESME contact for coordinating the project at the local level. Moreover, we thank the central coordination team of Unicancer and the ESME strategic and scientific committee members for their ongoing support.
Funding
The ESME-MBC database receives financial support from an industrial consortium (Roche, Pfizer, AstraZeneca, MSD, Eisai, and Daiichi Sankyo). Data collection, analysis and publication are managed entirely by UNICANCER, independently of the industrial consortium.
Author information
Authors and Affiliations
Contributions
WJ: conceptualisation, formal analysis, investigation, methodology, visualisation, writing—original draft, writing—review and editing. AL: conceptualisation, data curation, formal analysis, methodology, visualisation, funding acquisition, writing—original draft, writing—review and editing. CV: investigation, writing—review and editing. AM: investigation, writing—review and editing. TDLMR: investigation, writing—review and editing. LC: investigation, writing—review and editing. CL: investigation, writing—review and editing. AP: investigation, writing—review and editing. ID: investigation, writing—review and editing. LU: investigation, writing—review and editing. JCT: investigation, writing—review and editing. MR: investigation, writing—review and editing. OC: investigation, writing—review and editing. OT: investigation, writing—review and editing. TF: conceptualisation, data curation, investigation, writing—review and editing. JSF: conceptualisation, investigation, writing—review and editing. SD: conceptualisation, investigation, writing—review and editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
This study was authorised by the French data protection authority ([Registration ID 1704113 and authorisation N_DE-2013.-117], NCT03275311). Moreover, in compliance with the applicable European regulations, a complementary authorisation was obtained for the ESME Data Warehouse on 14 October 2019. All data were obtained retrospectively, and no procedure was taken to recover unavailable data by contacting healthcare providers or patients. The present analysis was approved by an independent French ethics committee (Comité de Protection des Personnes Sud-Est II-2015–79).
Consent to publish
Not applicable.
Competing interests
Dr. TDlMR reports personal fees and non-financial support from AstraZeneca, personal fees from Clovis oncology, personal fees from GSK, grant and personal fees from MSD, grant, personal fees and non-financial support from Pfizer, personal fees from Tesaro, personal fees and non-financial support from Roche Genentech, grant from SeattleGenetics, grant from Novartis, personal fees from Eisai, grant from Novartis, outside the submitted work. Dr. SD reports grants and non-financial support from Pfizer, grants from Novartis, grants and non-financial support from AstraZeneca, grants and non-financial support from Roche Genentech, grants from Lilly, grants from Puma, grants from Myriad, grants from Orion, grants from Amgen, grants from Sanofi, grants from Genomic Health, grants from GE, grants from Servier, grants from MSD, grants from BMS, grants from Pierre Fabre, grants from Seagen, grants from Exact Sciences, grants from Rappta, grants from Besins, grants from European Commission, grants from French government grants, grants from Fondation ARC, outside the submitted work. Dr. TF reports fees to its institution from Cellectis, grants from BMS, outside the submitted work. Dr. JSF reports personal fees from Roche Genentech, personal fees and non-financial support from SeattleGenetics, personal fees and non-financial support from Novartis, personal fees and non-financial support from Pfizer, personal fees and non-financial support from Lilly, personal fees and non-financial support from Novartis, personal fees and non-financial support from GSK, personal fees and non-financial support from Clovis oncoloy, personal fees and non-financial support from AstraZeneca, personal fees and non-financial support from Daiichi Sankyo, personal fees and non-financial support from Gilead, personal fees and non-financial support from MSD, personal fees and non-financial support from Pierre Fabre, personal fees and non-financial support from Amgen, outside the submitted work. Dr. WJ reports grants, personal fees and non-financial support from AstraZeneca, personal fees and non-financial support from Eisai, personal fees and non-financial support from Novartis, personal fees and non-financial support from Roche, personal fees and non-financial support from Pfizer, personal fees and non-financial support from Eli Lilly, personal fees from MSD, personal fees from BMS, personal fees and non-financial support from Chugai, personal fees from Seagen, grants and personal fees from Daiichi Sankyo, outside the submitted work. Dr. CL reports personal fees from Roche, non-financial support from MSD, grants from Lilly, other from DAIICHI, other from Pfizer, other from SANDOZ, outside the submitted work. Dr. AP reports other from Lilly, other from Pfizer, other from Pierre Fabre, others from Daiichi Sankyo, outside the submitted work. Dr. MR reports non-financial support from Roche, outside of the submitted work. Dr. JCT reports personal fees and non-financial support from PFIZER, personal fees from MSD, personal fees from ASTRA ZENECA, non-financial support from NOVARTIS, outside the submitted work. Dr. OT reports grants and personal fees from Roche, grants and personal fees from MSD-Merck, grants from BMS, personal fees from Novartis-Sandoz, personal fees from Pfizer, personal fees from Lilly, personal fees from AstraZeneca, personal fees from Daiichi Sankyo, personal fees from Eisai, personal fees from Pierre Fabre, personal fees from Seagen, personal fees from Gilead, outside the submitted work. Dr. CV reports personal fees from AstraZeneca, grants from BMS, non-financial support from IPSEN, personal fees from Novartis, personal fees and non-financial support from Pfizer, personal fees from Daiichi Sankyo, outside the submitted work. Drs. LC, OC, ID, AL, AM and LU have nothing to disclose.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Springer Nature or its licensor holds exclusive rights to this article under a publishing agreement with the author(s) or other rightsholder(s); author self-archiving of the accepted manuscript version of this article is solely governed by the terms of such publishing agreement and applicable law.
About this article

Cite this article
Jacot, W., Lusque, A., Vicier, C. et al. Outcomes of patients with HER2-negative metastatic breast cancer after platinum- and non-platinum-based first-line chemotherapy among patients with and without pathogenic germline BRCA1/2 mutations. Br J Cancer 127, 1963–1973 (2022). https://doi.org/10.1038/s41416-022-02003-1
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-022-02003-1
