
Abstract
Background
The associations between mammographic radiomics and breast cancer clinical endpoints are unclear. We aimed to identify mammographic radiomics features associated with breast cancer prognosis.
Methods
Nested from a large breast cancer cohort in our institution, we conducted an extreme case-control study consisting of 207 cases with any invasive disease-free survival (iDFS) endpoint <5 years and 207 molecular subtype-matched controls with >5-year iDFS. A total of 632 radiomics features in craniocaudal (CC) and mediolateral oblique (MLO) views were extracted from pre-treatment mammography. Logistic regression was used to identify iDFS-associated features with multiple testing corrections (Benjamini–Hochberg method). In a subsample with RNA-seq data (n = 96), gene set enrichment analysis was employed to identify pathways associated with lead features.
Results
We identified 15 iDFS-associated features from CC-view yet none from MLO-view. S(1,−1)SumAverg and WavEnLL_s-6 were the lead ones and associated with favourable (OR 0.64, 95% CI 0.42–0.87, P = 0.01) and poor iDFS (OR 1.53, 95% CI 1.31–1.76, P = 0.01), respectively. Both features were associated with eight pathways (primarily involving cell cycle regulation) in tumour but not adjacent normal tissues.
Conclusion
Our findings suggest mammographic radiomics features are associated with breast cancer iDFS, potentially through pathways involving cell cycle regulation.
Similar content being viewed by others


Introduction
Breast cancer is the most commonly diagnosed cancer and the leading cause of cancer deaths in women [1]. Although targeted therapy has significantly improved breast cancer survival [2], breast cancer mortality remains the fifth leading cause of cancer mortality worldwide, with 685,000 deaths in 2020 [1]. In addition to estrogen receptor (ER), progesterone receptor (PR) and human epidermal growth factor receptor 2 status (HER2), best-validated gene expression assays (e.g. Oncotype Dx [3], MammaPrint [4] and PAM50 [5]) may assist clinical decision-making to improve prognosis. However, non-invasive and low-cost markers, independent of tumour characteristics, in the prediction of breast cancer prognosis are still lacking.
In the past decade, advances in medical image analysis promoted the process of radiomics. Based on the quantitative features of intensity, shape, size or volume and texture, radiomics convert images into higher dimensional data for improved decision support [6]. Radiomics in breast cancer include breast magnetic resonance imaging (MRI), mammography and ultrasonography [7]. Mounting evidence demonstrated the associations of MRI features with diagnosis [8], prognosis [9], molecular subtyping [10] and response to neoadjuvant chemotherapy in breast cancer patients [7, 11]. For instance, pre-operative MRI radiomics signatures were proved to predict invasive disease-free survival (iDFS) in patients with invasive breast cancer [12, 13].
Mammography is a widely applied approach for breast cancer screening and diagnosis. Several automated feature extraction methods have been developed for mammography radiomics features, such as radical edge-gradient analysis [14], deep CNN model [15] and radiomics software (e.g. MAZDA [16], A.K. software [17] and TIK-SNAP software [18]). Although manual mass segmentation is needed for some methods before processing, a favourable agreement has been shown by different readers [19]. It has been shown that mammographic radiomics features were predictive for mass classification [17, 19] and level of tumour-infiltrating lymphocytes [18, 19] and were associated with oncotype DX test recurrence score [20]. However, it is unclear whether mammographic radiomics features are associated with breast cancer clinical endpoints (e.g. iDFS or overall survival).
In the present study, we aimed to identify mammographic radiomics features associated with breast cancer prognosis and explore the potential biological basis using RNA-seq data.
Methods
Study design
The Breast Cancer Cohort from our institution is a prospective cohort of patients who were diagnosed with breast cancer in our institution from January 2009 onwards [20]. Information on tumour characteristics, such as tumour size (the largest tumour diameter), tumour stage (TNM stage according to the AJCC Cancer Staging Manual), histologic grade (Scarff-Bloom-Richardson histologic grading system [21]) and molecular subtype [22], as well as treatment, was collected from medical records [23]. Patients were followed every 4 months in the first 3 years after surgery, every 6–12 months in the fourth and fifth years and annually thereafter. Follow-up was operated by office visit, telephone or postal contact. This study was approved by the Clinical Test and Biomedical Ethics Committee of our institution (No. 2019-16). Informed consent was obtained from all patients.
Both diagnostic ultrasound and mammography were routinely performed for patients with suspicious breast mass at our institution. The digital database of mammography images was available from January 2010. Between January 2010 and February 2017, 6455 patients were enrolled on the cohort; among them, 3737 (57.9%) patients received mammography in our institution before surgery. Patients were further excluded according to the following criteria: underwent neoadjuvant therapy (n = 449); with distant metastases (n = 82); carcinoma in situ (n = 157) or with missing information on tumour stage, i.e. unknown number of positive lymph nodes (n = 8) and tumour size (n = 188). Subsequently, 2853 patients with pre-surgical mammography were eligible for this study (Fig. 1).

The flowchart depicts the patient selection process from a prospective cohort of patients being diagnosed with breast cancer in our institution between January 2010 and February 2017.
To optimise the cost-effectiveness and maximise the statistical power, we performed a matched extreme case-control design (comparing patients with the poorest prognosis with those with the most favourable prognosis) which has been proved to successfully identify prognostic biomarkers associated with cancer prognosis [24]. During the follow-up from diagnosis through June 2020 (median: 5.2 years), 207 patients developed iDFS endpoints [25] (including any local or regional recurrence, distant metastasis, contralateral breast cancer, secondary primary cancer, cancer-specific death and death from other causes) during the first 5 years after cancer diagnosis (cases). Patients without any clinical events of iDFS who survived at least 5 years after cancer diagnosis were considered controls (n = 1451). Controls were randomly selected and 1:1 matched on molecular subtype [22]. Finally, 414 patients (207 cases) were included for analysis; fresh-frozen breast tumour tissues were available for 50 cases and 46 controls.
Mammography radiomics features
Both diagnostic ultrasound and mammography were routinely performed for patients with suspicious breast mass for purpose of diagnosing/staging at our institution, a tertiary medical centre. Because no formal mammography screening program has been established in our province, most breast cancers were detected due to symptoms or breast self-examination.
All mammogram images were obtained from the GE SenoBright full-field digital mammography systems (GE Healthcare, Chicago, IL). Leveraging the free radiomics platform MAZDA software (Technical University of Lodz) [16], an experienced and specialised radiologist (one of the first authors having subspecialty experience in breast radiology) manually outlined tumour contours in craniocaudal (CC) and mediolateral oblique (MLO) views of each patient and extracted radiomics features of the lesion area. MAZDA computed six categories of features: histogram, gradient, co-occurrence matrix, run-length matrix (RLM), autoregressive model and Haar wavelet groups. A total of 316 mammography radiomics features were extracted from each view. The values of each feature were normalised through z-score transformation.
RNA sequencing
Fresh-frozen breast tumour tissues and paired adjacent normal tissues were donated at the surgery. RNA integrity was examined using the RNA Nano 6000 Assay Kit of the Agilent Bioanalyzer 2100 system and RNA Integrity Number (RIN) > 7.0 was required to pass the quality control. RNA sequencing was performed on the Illumina Hi-Seq, Paired-end 150. Raw RNA-seq data were processed according to nfcore/rnaseq: a bioinformatics analysis pipeline for RNA sequencing data (https://nf-co.re/rnaseq/1.0/). Fragments Per Kilobase Million (FPKM) of each gene were calculated by dividing the read count by the gene length and the total number of reads mapped to protein-coding genes. A total of 19,448 genes were profiled. The FPKM values were further normalised using z-score transformation.
Statistical analysis
Clinical characteristics, including age at diagnosis, menopausal status, molecular subtype, tumour stage, histologic grade, hormone therapy, chemotherapy and radiotherapy, were compared between patients with poor iDFS (cases) and those with favourable iDFS (controls) using t-test for continuous variables or Chi-square test for categorical ones. Using logistic regression, odds ratios (ORs) and 95% confidence intervals (CIs) of iDFS endpoints were estimated for mammography radiomics features from CC and MLO views, respectively. As described above, iDFS endpoints included any local or regional recurrence, distant metastasis, contralateral breast cancer, secondary primary cancer, cancer-specific death and death from other causes. Multiple testing was corrected using Benjamini–Hochberg method to control for the false discovery rate (FDR). We presented ORs without adjustment (Model 1), ORs adjusted for demographic characteristics (age at diagnosis and menopausal status; Model 2) and ORs additionally adjusted for tumour characteristics (molecular subtype, tumour stage and histologic grade; Model 3). Radiomics features with significant associations in Model 3 were considered as lead markers. In a sensitivity analysis, we further adjusted for treatment modes (receipt of chemotherapy, hormone therapy and radiotherapy; Model 4), which should be considered as potential mediators rather than confounders. Many radiomics features were highlighted as correlated. To reduce multiple testing, we used a correlation matrix to examine clusters and identify top independent markers for subsequent analyses, in which Model 3 was applied.
Leveraging the RNA-seq data from breast cancer tissues and paired adjacent normal tissues, we examined the associations between top independent markers and the expression levels of individual genes using linear regression and visualised them in volcano plots. P values were corrected using FDR. To shed light on the biological mechanisms, we performed gene set enrichment analysis using a camera package and identified hallmark and KEGG pathways associated with top independent markers. The gene lists of candidate pathways were downloaded from the Gene Set Enrichment Analysis (http://www.gsea-msigdb.org/gsea/index.jsp).
All statistical tests were two-tailed and conducted using R version 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Compared to patients with favourable iDFS (controls; n = 207), patients with poor iDFS (cases; n = 207) were more likely to be post-menopausal at diagnosis (43.0% vs. 32.4%, P = 0.033), to have advanced tumour stage (42.0% vs. 15.0%, P < 0.001) and high histologic grade (65.7% vs. 54.6%, P = 0.027) and to receive no hormone therapy (57.0% vs. 69.1%, P = 0.015; Table 1). Similar patterns were observed for patients whose tumours have been sequenced for RNA, although the tumour stage was significantly different between the two groups (50.0% vs. 10.9%, P < 0.001; Supplementary Table S1).
Identifying features associated with iDFS
In our primary model, where we adjusted for demographic and tumour characteristics, 15 out of 316 mammography radiomics features from CC-view were significantly associated with iDFS after multiple testing corrections (all P < 0.05; Table 2, Model 3). These associations remained significant with additional adjustments for treatment modes (Supplementary Table S2). In a sensitivity analysis, we excluded cases who died of non-breast-cancer causes and yielded similar findings (Supplementary Table S3). Other CC-view features were not associated with iDFS (Supplementary Table S4). Moreover, no features from the MLO-view were associated with iDFS after multiple testing correlations (all P > 0.05; Supplementary Table S5). Although none of MLO-view features was identified as lead features, three MLO-view features [GrKurtosis, Skewness and S(1,0)SumAverg] appeared associated with iDFS (empirical P < 0.05; Supplementary Table S6).
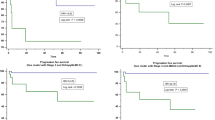
Using the correlation matrix analysis, we identified two clusters from the 15 lead features from CC-view (Supplementary Fig. S1). S(1,−1)SumAverg and WavEnLL_s-6 were the top features (with strongest association with iDFS) in each cluster, and associated with favourable iDFS (OR, 0.64; 95% CI, 0.42–0.87; P = 0.010; Table 2) and poor iDFS (OR, 1.53; 95% CI, 1.31–1.76; P = 0.010; Table 2), respectively. Feature S(1,−1)SumAverg belongs to the category of co-occurrence matrix, while feature WavEnLL_s-6 is part of the Haar wavelet category. In stratified analyses, stronger associations were found in pre-menopausal patients for both features and patients with Luminal A tumour for feature S(1,−1)SumAverg (P-for-interaction < 0.05; Supplementary Table S7). Similar associations were noted for both features across tumour stage and histologic grade groups.
Exploring the biological basis for identified features
Feature WavEnLL_s-6 was significantly associated with a more advanced tumour stage (P = 0.029; Supplementary Table S8) but not associated with molecular subtype or histologic grade. Feature S(1,−1)SumAverg was not associated with tumour characteristics.
In a subsample of patients whose tumours were profiled for RNA (n = 96), feature S(1,−1)SumAverg was significantly associated with the expression of gene MOV10L1, LRP1B, ZFY, PITX2, TRAPPC12, MMGT1 and PPP2R2C (all P < 0.05; Fig. 2 and Supplementary Table S9). Feature WavEnLL_s-6 was positively associated with the expression of gene CSNK2A1 (P = 0.005; Fig. 2 and Supplementary Table S9). The above associations were not observed in paired adjacent normal tissues (n = 60; Supplementary Table S9).

Red-coloured genes had negative estimates, while blue-coloured genes had positive estimates. Estimates were adjusted for age, menopausal status, molecular subtype, tumour stage and histologic grade. FDR false discovery rate.
In pathway analysis, we further found that feature S(1,−1)SumAverg was significantly associated with upregulated signalling of 8 pathways, including G2M checkpoint pathway, E2F_target genes, MYC targets v1 and v2 (two subgroups of genes regulated by MYC—version 1 and—version 2), DNA replication, mismatch repair pathway, cell cycle pathway and the ubiquitin-proteasome pathway (all P < 0.05; Table 3). The majority of these pathways were essential for DNA replication, cell cycle progression and DNA damage repair. Feature WavEnLL_s-6 was similarly associated with the aforementioned pathways and with downregulated signalling of the ribosome pathway (all P < 0.05; Table 3). However, in paired adjacent normal tissues (n = 60), both features were not associated with the aforementioned pathways except MYC targets v2 in an opposite direction for feature WavEnLL_s-6 (Table 3).
Discussion
To the best of our knowledge, this is the first study to identify mammography radiomics features associated with invasive disease-free survival among patients with invasive breast cancer. In the extreme case-control study nested from a large prospective cohort, two independent features from CC-view, S(1,−1)SumAverg and WavEnLL_s-6, were associated with invasive disease-free survival, independent of clinical characteristics and after stringent correction for multiple comparisons. Moreover, both features were associated with gene signatures of pathways responsible for DNA replication, cell cycle progression and DNA damage repair in tumour tissue, but not in paired adjacent normal tissue. These findings shed light on the potential biological mechanisms linking identified features to breast cancer prognosis. Although these markers are to be confirmed in an independent setting, the highlighted biological processes underlying these features strongly refute the possibility of findings by pure chance.
In a previous study of 350 patients with ER-positive breast cancer, Woodard et al. found that mammographic breast density, calcification morphology and mass margins were correlated with a prognostic biomarker—the Oncotype DX recurrence score [20]. However, these features were derived from the BI-RADS, which is subjective to the observer’s visual interpretation [26]; and the associations were not confirmed using clinical endpoints. By contrast, mathematical extraction of mammography radiomics features is more objective and feasible for application. In the present study, we also illustrated that the identified radiomics features were associated with iDFS endpoints; and the associations were robust across molecular subtypes and independent of clinical characteristics.
One of the two top independent features, S(1,−1)SumAverg, is under the category of co-occurrence matrix [27]. Using the RNA-seq data, we showed that feature S(1,−1)SumAverg was associated with expression levels of genes (i.e. LRP1B and PITX2) in tumour tissue but not in adjacent normal tissue. Both LRP1B [28] and PITX2 [29] are involved in the regulation of the cell cycle and DNA damage repair. In the pathway analysis, we further illustrated that feature S(1,−1)SumAverg was primarily associated with the signalling of pathways playing a pivotal role in DNA replication, cell cycle progression and DNA damage repair, specifically in tumour tissue. These pathways are critical for tumour phenotypes and patient survival [30, 31]. Taken together, our findings lend support to that feature S(1,−1)SumAverg may capture the underlying biological process of cell cycle regulation in breast tumours and therefore is linked to the prognosis.
The other feature, WavEnLL_s-6, is under the category of Haar wavelet [16, 32]. Our data showed that feature WavEnLL_s-6 was associated with CSNK2A1expression, specifically in tumour tissue. It is known that CSNK2A1 promotes proliferation and invasiveness of breast cancer cells through mediating phosphorylation of SIRT6 [33]. Moreover, WavEnLL_s-6 was associated with the same pathways shown for S(1,−1)SumAverg and ribosome pathway. Ribosomal protein RPL15 upregulates the expression of cell cycle mediators and facilitates breast cancer metastasis in vivo [34]. Collectively, we elucidated that the feature WavEnLL_s-6 is associated with breast cancer prognosis potential through the biological process of DNA replication, cell cycle progression and DNA damage repair.
In contrast, we only found three MLO-view features that were empirically suggested for breast cancer iDFS. The reason for fewer hits in MLO-view is unclear. Gupta et al [35]. explored the correlations between CC-view and MLO-view Haralick texture features of breast lesions in 1350 patients. Among 13 feature clusters, they found 4 clusters, including sum average, had weak two-view correlation. These findings suggest that breast lesions displayed distinct textures in terms of the structure regularity in CC and MLO views. Of note, sum average cluster is one of the top features in CC-view associated with breast cancer iDFS. The low correlation between CC-view and MLO-view for this feature cluster may account for the fewer findings from the MLO-view.
One major strength of our study is the rich information on multi-omics data, which allowed us to explore the biological basis linking radiomics features to breast cancer prognosis. The present study, however, has several limitations. First, in our cohort, only 58% of patients had data on mammography prior to surgery, resulting in a limited sample size for this study. However, the clinical characteristics were largely comparable between patients with and without mammography, except that patients with mammography were slightly younger and had less advanced tumour stage (Supplementary Table S10). However, our estimates have been carefully adjusted for age and tumour stage. Moreover, in the stratified analysis, similar associations between the top features and iDFS were found across tumour stages. Stronger results were noted among pre-menopausal patients (i.e. younger ones), suggesting that the associations would slightly attenuate if including patients without mammography who had 7% more pre-menopausal women. Moreover, only patients with fresh-frozen samples were profiled for RNA and were included in the analyses of gene expression and pathway. Yet, the clinical characteristics of those with RNA-seq data were compared with those without, except that they were somewhat younger at diagnosis (Supplementary Table S11). Second, we only analysed the radiomics features within 2 months before surgery. Radiomics features may change along the disease course. Whether the temporal changes associated with prognosis warrants future research. Third, although the MAZDA platform provides objective measures on feature extraction, manual outlining of tumour areas in mammography may be subjective to the readers. However, a fairly good agreement has been shown for data extracted by different readers [19]. Fourth, we considered all-cause mortality as one of the iDFS endpoints, and patients who died of non-breast-cancer causes may not have experienced cancer progression. However, we have yielded very similar associations by excluding patients who died of non-breast-cancer causes. Fifth, it has been well-demonstrated that mammographic density predicts breast cancer risk [36]. Future research is needed to explore the association between mammographic density and breast cancer prognosis.
In conclusion, our findings suggest that mammography radiomics features S(1,−1)SumAverg and WavEnLL_s-6 from CC-view are associated with invasive disease-free survival among patients with breast cancer, potential through pathways involving DNA replication and damage response and cell cycle regulation. If confirmed in other studies, our findings may provide important evidence to incorporate top mammography radiomics features into the conventional breast cancer prognostic nomograms. These radiomics features could be easily obtained from the standard of care at minimal cost and aid healthcare providers to identify high-risk patients and navigate treatment decisions.
Data availability
The datasets generated and/or analysed during the current study are available from the corresponding author on reasonable request.
References
Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA: a cancer journal for clinicians. 2021;71:209–49. https://doi.org/10.3322/caac.21660.
(EBCTCG) Early Breast Cancer Trialists’ Collaborative group. Trastuzumab for early-stage, HER2-positive breast cancer: a meta-analysis of 13 864 women in seven randomised trials. Lancet Oncol. 2021;22:1139–50. https://doi.org/10.1016/s1470-2045(21)00288-6.
Paik S, Shak S, Tang G, Kim C, Baker J, Cronin M, et al. A multigene assay to predict recurrence of tamoxifen-treated, node-negative breast cancer. N Engl J Med. 2004;351:2817–26. https://doi.org/10.1056/NEJMoa041588.
Cardoso F, van’t Veer LJ, Bogaerts J, Slaets L, Viale G, Delaloge S, et al. 70-gene signature as an aid to treatment decisions in early-stage breast cancer. N Engl J Med. 2016;375:717–29. https://doi.org/10.1056/NEJMoa1602253.
Lænkholm AV, Jensen MB, Eriksen JO, Rasmussen BB, Knoop AS, Buckingham W, et al. PAM50 risk of recurrence score predicts 10-year distant recurrence in a comprehensive danish cohort of postmenopausal women allocated to 5 years of endocrine therapy for hormone receptor-positive early breast cancer. J Clin Oncol. 2018;36:735–40. https://doi.org/10.1200/jco.2017.74.6586.
Lambin P, Leijenaar RTH, Deist TM, Peerlings J, de Jong EEC, van Timmeren J, et al. Radiomics: the bridge between medical imaging and personalized medicine. Nat Rev Clin Oncol. 2017;14:749–62. https://doi.org/10.1038/nrclinonc.2017.141.
Valdora F, Houssami N, Rossi F, Calabrese M, Tagliafico AS. Rapid review: radiomics and breast cancer. Breast Cancer Res Treat. 2018;169:217–29. https://doi.org/10.1007/s10549-018-4675-4.
Dong Y, Feng Q, Yang W, Lu Z, Deng C, Zhang L, et al. Preoperative prediction of sentinel lymph node metastasis in breast cancer based on radiomics of T2-weighted fat-suppression and diffusion-weighted MRI. Eur Radiol. 2018;28:582–91. https://doi.org/10.1007/s00330-017-5005-7.
Li H, Zhu Y, Burnside ES, Drukker K, Hoadley KA, Fan C, et al. MR imaging radiomics signatures for predicting the risk of breast cancer recurrence as given by research versions of mammaprint, oncotype DX, and PAM50 gene assays. Radiology. 2016;281:382–91. https://doi.org/10.1148/radiol.2016152110.
Li H, Zhu Y, Burnside ES, Huang E, Drukker K, Hoadley KA, et al. Quantitative MRI radiomics in the prediction of molecular classifications of breast cancer subtypes in the TCGA/TCIA data set. npj Breast Cancer. 2016;2. https://doi.org/10.1038/npjbcancer.2016.12.
Braman NM, Etesami M, Prasanna P, Dubchuk C, Gilmore H, Tiwari P, et al. Intratumoral and peritumoral radiomics for the pretreatment prediction of pathological complete response to neoadjuvant chemotherapy based on breast DCE-MRI. Breast Cancer Res. 2017;19:57. https://doi.org/10.1186/s13058-017-0846-1.
Park H, Lim Y, Ko ES, Cho HH, Lee JE, Han BK, et al. Radiomics signature on magnetic resonance imaging: association with disease-free survival in patients with invasive breast cancer. Clin Cancer Res. 2018;24:4705–14. https://doi.org/10.1158/1078-0432.Ccr-17-3783.
Yu Y, Tan Y, Xie C, Hu Q, Ouyang J, Chen Y, et al. Development and validation of a preoperative magnetic resonance imaging radiomics-based signature to predict axillary lymph node metastasis and disease-free survival in patients with early-stage breast cancer. JAMA Netw Open. 2020;3:e2028086. https://doi.org/10.1001/jamanetworkopen.2020.28086.
Huo Z, Giger ML, Vyborny CJ, Bick U, Lu P, Wolverton DE, et al. Analysis of spiculation in the computerized classification of mammographic masses. Med Phys. 1995;22:1569–79. https://doi.org/10.1118/1.597626.
Shi B, Grimm LJ, Mazurowski MA, Baker JA, Marks JR, King LM, et al. Prediction of occult invasive disease in ductal carcinoma in situ using deep learning features. J Am Coll Radiol. 2018;15:527–34. https://doi.org/10.1016/j.jacr.2017.11.036.
Szczypiński P M, Strzelecki M, Materka A, Klepaczko A. MaZda—a software package for image texture analysis. Comput Methods Prog Biomed. 2009;94:66–76. https://doi.org/10.1016/j.cmpb.2008.08.005.
Mao N, Yin P, Wang Q, Liu M, Dong J, Zhang X, et al. Added value of radiomics on mammography for breast cancer diagnosis: a feasibility study. J Am Coll Radiol. 2019;16:485–91. https://doi.org/10.1016/j.jacr.2018.09.041.
Yu H, Meng X, Chen H, Han X, Fan J, Gao W, et al. Correlation between mammographic radiomics features and the level of tumor-infiltrating lymphocytes in patients with triple-negative breast cancer. Front Oncol. 2020;10:412. https://doi.org/10.3389/fonc.2020.00412.
Stelzer PD, Steding O, Raudner MW, Euller G, Clauser P, Baltzer PAT. Combined texture analysis and machine learning in suspicious calcifications detected by mammography: potential to avoid unnecessary stereotactical biopsies. Eur J Radiol. 2020;132:109309. https://doi.org/10.1016/j.ejrad.2020.109309.
Woodard Genevieve A, Ray Kimberly M, Joe Bonnie N, Price Elissa R. Qualitative radiogenomics: association between oncotype DX test recurrence score and BI-RADS mammographic and breast MR imaging features. Radiology. 2018;286:60–70. https://doi.org/10.1148/radiol.2017162333.
Bloom HJG, Richardson WW. Histological grading and prognosis in breast cancer. Br J Cancer. 1957;11:359–77. https://doi.org/10.1038/bjc.1957.43.
Senkus E, Kyriakides S, Ohno S, Penault-Llorca F, Poortmans P, Rutgers E, et al. Primary breast cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2015:v8-30. https://doi.org/10.1093/annonc/mdv298.
Xie Y, Valdimarsdóttir UA, Wang C, Zhong X, Gou Q, Zheng H, et al. Public health insurance and cancer‐specific mortality risk among patients with breast cancer: a prospective cohort study in China. Int J Cancer. 2020;148:28–37. https://doi.org/10.1002/ijc.33183
Salim A, Ma X, Fall K, Andrén O, Reilly M. Analysis of incidence and prognosis from ‘extreme’ case-control designs. Stat Med. 2014;33:5388–98. https://doi.org/10.1002/sim.6245.
Gourgou-Bourgade S, Cameron D, Poortmans P, Asselain B, Azria D, Cardoso F, et al. Guidelines for time-to-event end point definitions in breast cancer trials: results of the DATECAN initiative (Definition for the Assessment of Time-to-event Endpoints in CANcer trials. J Ann Oncol. 2015;26:2505–6. https://doi.org/10.1093/annonc/mdv478.
van Timmeren JE, Cester D, Tanadini-Lang S, Alkadhi H, Baessler B. Radiomics in medical imaging-“how-to” guide and critical reflection. Insights Imaging. 2020;11:91. https://doi.org/10.1186/s13244-020-00887-2.
Haralick RM. Statistical and structural approaches to texture. Proc IEEE. 1979;67:786–804. https://doi.org/10.1109/PROC.1979.11328.
Asano Y, Takeuchi T, Okubo H, Saigo C, Kito Y, Iwata Y, et al. Nuclear localization of LDL receptor-related protein 1B in mammary gland carcinogenesis. J Mol Med. 2019;97:257–68. https://doi.org/10.1007/s00109-018-01732-2.
Xu YY, Yu HR, Sun JY, Zhao Z, Li S, Zhang XF, et al. Upregulation of PITX2 promotes letrozole resistance via transcriptional activation of IFITM1 signaling in breast cancer cells. Cancer Res Treat. 2019;51:576–92. https://doi.org/10.4143/crt.2018.100.
Otto T, Sicinski P. Cell cycle proteins as promising targets in cancer therapy. Nat Rev Cancer. 2017;17:93–115. https://doi.org/10.1038/nrc.2016.138.
Oshi M, Takahashi H, Tokumaru Y, Yan L, Rashid OM, Matsuyama R, et al. G2M cell cycle pathway score as a prognostic biomarker of metastasis in estrogen receptor (ER)-positive breast cancer. Int J Mol Sci. 2020;21. https://doi.org/10.3390/ijms21082921.
Mallat SG. Multifrequency channel decompositions of image and wavelet models. IEEE Trans Acoust Speech Signal Process. 1989;37:2091–110. https://doi.org/10.1109/29.45554.
Bae JS, Park SH, Jamiyandorj U, Kim KM, Noh SJ, Kim JR, et al. CK2α/CSNK2A1 phosphorylates SIRT6 and is involved in the progression of breast carcinoma and predicts shorter survival of diagnosed patients. Am J Pathol. 2016;186:3297–315. https://doi.org/10.1016/j.ajpath.2016.08.007.
Ebright RY, Lee S, Wittner BS, Niederhoffer KL, Nicholson BT, Bardia A, et al. Deregulation of ribosomal protein expression and translation promotes breast cancer metastasis. Science. 2020;367:1468–73. https://doi.org/10.1126/science.aay0939.
Gupta S, Markey MK. Correspondence in texture features between two mammographic views. Med Phys. 2005;32:1598–606. https://doi.org/10.1118/1.1915013.
Brentnall AR, Cuzick J, Buist DSM, Bowles EJA. Long-term accuracy of breast cancer risk assessment combining classic risk factors and breast density. JAMA Oncol. 2018;4:e180174. https://doi.org/10.1001/jamaoncol.2018.0174.
Funding
This work was supported by the National Natural Science Foundation of China (grant number: 81872307; to DL) and the Key Research and Development Program of Sichuan Province (grant number: 2022YFS0206; to DL) and the Science and Technology Support Program of Sichuan Province (grant number: 2021YJ0236; to SZ). Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
CL and DL had full access to the data used for the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: CL, SZ and DL. Acquisition, analysis or interpretation of the data: CL, SZ and DL. Drafting of the manuscript: CL and DL. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: CL. Obtained funding: SZ and DL. Administrative, technical or material support: DL. Study supervision: DL.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Clinical Test and Biomedical Ethics Committee at West China Hospital (No. 2019-16).
Consent to publish
Not applicable.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Luo, C., Zhao, S., Peng, C. et al. Mammography radiomics features at diagnosis and progression-free survival among patients with breast cancer. Br J Cancer 127, 1886–1892 (2022). https://doi.org/10.1038/s41416-022-01958-5
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-022-01958-5
