
Abstract
Background
To investigate if anti-androgenic medications 5α-reductase inhibitors (5-ARIs) decrease the risk of developing oesophageal and gastric tumours, analysed by histological type and anatomical sub-site.
Methods
A Swedish population-based cohort study between 2005 and 2018 where men using 5-ARIs were considered exposed. For each exposed participant, ten male age-matched non-users of 5-ARIs (non-exposed) were included. Multivariable Cox regression provided hazard ratios (HR) with 95% confidence intervals (CI) adjusted for age, calendar year, smoking, non-steroidal anti-inflammatory drugs/aspirin use, and statins use. Further adjustments were made depending on the tumour analysed.
Results
The cohort included 191,156 users of 5-ARIs and 1,911,560 non-users. Overall, the use of 5-ARIs was not associated with any statistically significantly reduced risk of oesophageal or cardia adenocarcinoma (adjusted HR 0.92, 95% CI 0.82–1.02) or gastric non-cardia adenocarcinoma (adjusted HR 0.90, 95% CI 0.80–1.02). However, the use of 5-ARIs indicated a decreased risk of oesophageal or cardia adenocarcinoma among obese or diabetic participants (adjusted HR 0.55, 95% CI 0.39–0.80) and a reduced risk of oesophageal squamous cell carcinoma (adjusted HR 0.49, 95% CI 0.37–0.65).
Conclusion
Users of 5-ARIs may have a decreased risk of developing oesophageal or cardia adenocarcinoma among those obese or diabetic, and a decreased risk of oesophageal squamous cell carcinoma.
Similar content being viewed by others

Background
Oesophageal and gastric cancers are the 6th and 2nd leading causes, respectively, of cancer-related deaths globally [1]. The main histological types of oesophageal cancer, i.e. adenocarcinoma and squamous cell carcinoma, have distinct aetiology. Adenocarcinoma is the dominant histological type (>95%) of gastric cancer, but the anatomical sub-sites cardia and non-cardia gastric adenocarcinoma have different aetiology [2, 3]. Oesophageal and cardia adenocarcinoma share the main risk factors of gastro-oesophageal reflux disease and obesity, while tobacco smoking and alcohol overconsumption are the main risk factors for oesophageal squamous cell carcinoma [2]. Helicobacter pylori infection is the main risk factor for gastric non-cardia adenocarcinoma, but does not increase the risk of cardia adenocarcinoma, and decreases the risk of oesophageal adenocarcinoma [4].
Oesophageal and cardia adenocarcinoma are characterised by a strong and unexplained male predominance with a 6-to-1 male-to-female ratio in Europe and up to 9-to-1 in North America [5, 6]. The role of sex hormones in the aetiology of these tumours is supported by a 16-year delayed onset in women compared with men, and associations with circulating sex hormone levels [7,8,9,10]. Oesophageal squamous cell carcinoma and gastric non-cardia adenocarcinoma are also overrepresented in men, but the male predominance is weaker and is largely explained by sex differences in the prevalence of the main risk factors [4, 11, 12].
The medications 5α-reductase inhibitors (5-ARIs) have anti-androgenic properties and are widely used against benign prostatic hyperplasia. They inhibit the 5α-reductase enzyme and reduce the conversion of testosterone to the more potent androgen dihydrotestosterone [13,14,15]. The only previous study that has investigated 5-ARIs use and risk of oesophageal and gastric cancer indicated risk reductions, but that study did not separately analyse histological types or sub-sites of these tumours [16].
This study aimed to test the hypothesis that the use of 5-ARIs decreases the risk of oesophageal and gastric cancer, independent of tumour histology and anatomical sub-site, but that the risk is particularly decreased for oesophageal and cardia adenocarcinoma.
Methods
Design
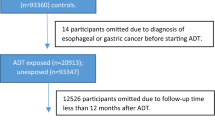
This was a nationwide Swedish population-based cohort study of men between July 1, 2005 and December 31, 2018, where exposure to 5-ARIs was examined in relation to the risk of developing the outcomes of oesophageal or gastric cancer. The source population was all male Swedish residents aged 18 years or older who were included in the Swedish Prescribed Drugs and Health Cohort (SPREDH), which has been presented in detail in a cohort description [17]. In brief, SPREDH combines data from four national Swedish health data registries: Prescribed Drug Registry, Patient Registry, Cancer Registry and Cause of Death Registry. These registries achieved complete nationwide coverage well before the study period, and the linkage of individuals’ data between multiple registries was enabled by the unique personal identity number, assigned to each resident in Sweden at birth or immigration. SPREDH included 8,269,978 adults with at least one record of a selected commonly prescribed medication during the study period. The data used for the present study were basic characteristics, prescribed and dispensed medications, healthcare utilisation, diagnoses, and dates and causes of death. Individuals were excluded if they had any previous diagnosis of oesophageal cancer, gastric cancer, or male genital cancers (including prostate cancer), or had undergone oesophagectomy or gastrectomy before cohort entry (details provided in Supplementary Table 1).
Exposure
The exposure was at least two dispensed records of the 5-ARIs finasteride or dutasteride during the study period. These medications were identified from the Swedish Prescribed Drug Registry by their anatomical therapeutic chemical (ATC) classification codes (Supplementary Table 2). For each exposed participant, ten individuals unexposed to 5-ARIs were randomly selected from SPREDH and matched by age (±1 year) at cohort entry (2nd 5-ARI purchase). Non-users of 5-ARIs were censored if the first dispensation of any 5-ARI was recorded. Non-users were shifted to the exposed group at any second dispensed record of 5-ARIs. All participants were followed up until the date of any of the outcomes, death or the end of the study period (December 31, 2018), whichever occurred first.
Outcomes
Among a total of three outcomes, the main outcome was oesophageal or cardia adenocarcinoma. These tumours were combined because of their adjacent anatomical positioning, shared aetiology and similarly strong male predominance. The secondary outcomes were oesophageal squamous cell carcinoma and gastric non-cardia adenocarcinoma. All cancer diagnoses were identified from the Cancer Registry by the diagnosis codes in the International Classification of Diseases, 7th version (ICD-7) (150 for oesophageal cancer, 151.1 for cardia cancer, and 151 excluding 151.1 for gastric non-cardia cancer) and histology codes in the WHO/HS/CANC/24 classification (096 for adenocarcinoma and 146 for squamous cell carcinoma).
Covariates
There were nine covariates in total: age (continuous), calendar year (continuous), gastro-oesophageal reflux disease (yes or no), obesity or diabetes (yes or no), tobacco smoking or smoking-related diagnoses (yes or no), alcohol overconsumption-related diagnoses (yes or no), Helicobacter pylori eradication treatment (yes or no), use of non-steroidal anti-inflammatory drugs (NSAIDs) or aspirin (yes or no), and use of statins (yes or no). The combined covariate obesity and diabetes diagnoses were used as a proxy for obesity because the obesity diagnosis was under-recorded in the Patient Registry and the vast majority (81.9%) of diabetes patients are overweight [18]. Diagnoses confirmed within 10 years before cohort entry were searched for in the Patient Registry. Helicobacter pylori eradication treatment was defined by a record of a specific eradication package in the Prescribed Drug Registry during the study period and was treated as a time-varying variable. Use of NSAIDs/aspirin and statins were defined by at least two dispensed records of these medications in the Prescribed Drug Registry within one year before cohort entry.
Statistical analysis
Cox proportional hazards regression was performed to estimate the risks of the study outcomes in 5-ARI users compared with non-users of 5-ARI, providing hazard ratios (HR) with 95% confidence intervals (CI). Both crude and multivariable models were applied. The multivariable models were tailored for each outcome, but all models were adjusted for five covariates: Age, calendar year, tobacco smoking or smoking-related diagnoses, use of NSAIDs/aspirin, and use of statins. In addition to these adjustments, the analyses of oesophageal or cardia adenocarcinoma were adjusted for gastro-oesophageal reflux disease, obesity or diabetes, and Helicobacter pylori eradication treatment; analyses of gastric non-cardia adenocarcinoma adjusted for obesity or diabetes and Helicobacter pylori eradication treatment; and analyses of oesophageal squamous cell carcinoma adjusted for alcohol overconsumption-related diagnoses. Stratified analyses were performed for oesophageal or cardia adenocarcinoma (main outcome) by age (dichotomised by the median value), gastro-oesophageal reflux disease (yes and no), obesity or diabetes (yes and no), Helicobacter pylori eradication treatment (yes and no), tobacco smoking or smoking-related diagnoses (yes and no), and type of 5-ARIs (finasteride and dutasteride). We also tested the possible interaction of the use of 5-ARIs with each of these covariates by adding a multiplicative interaction term in the Cox regression. All models met the proportional-hazard assumption on the basis of Schoenfeld residuals. Two sensitivity analyses were performed to assess the robustness of the results: one excluding those individuals who entered the cohort in 2005 (the first year) and had less than 6 months of drug history, which was done in order to assess new 5-ARI users (incident users); and another that censored individuals who developed any cancer (except for non-malignant melanoma; ICD-7 codes 140-209 excluding 191 in the Cancer Registry) before the outcomes under study.
An experienced biostatistician (GS) followed a detailed study protocol and used the statistical software Stata (Release 16, StataCorp, College Station, TX) when performing the data management and statistical analyses. All analyses were two-sided.
Results
Study participants
The study included 191,156 users of 5-ARIs, together accumulating 1,094,334 exposed person-years at risk. These were compared with 1,911,560 non-users of 5-ARIs who contributed to a total of 9,874,357 unexposed person-years. The mean duration of 5-ARI use was 3.8 years (interquartile range 0.61–6.11 years). The two groups had similar characteristics, except for a slightly higher prevalence of gastro-oesophageal reflux disease and Helicobacter pylori eradication treatment and a lower prevalence of alcohol overconsumption-related diagnoses in the 5-ARIs users (Table 1). Among users of 5-ARIs 33.7% had no record of benign prostatic hyperplasia diagnosis compared to 78.9% in the non-user group (Supplementary Table 4).
Risk of oesophageal or cardia adenocarcinoma
A total of 345 users of 5-ARIs and 3328 non-users were diagnosed with oesophageal or cardia adenocarcinoma during the follow-up. The use of 5-ARIs was associated with a slightly decreased point estimate of oesophageal or cardia adenocarcinoma, although the association was not statistically significant (adjusted HR 0.92, 95% CI 0.82–1.02) (Table 2). In the stratified analyses, the use of 5-ARIs was associated with decreased HRs in participants with obesity or diabetes (adjusted HR 0.55, 95% CI 0.39–0.80). No such statistically significant associations were found in the stratified analyses by age, gastro-oesophageal reflux disease, Helicobacter pylori treatment, or tobacco smoking or smoking-related diagnoses, although all point estimates were below 1 (Table 3). The point estimates were similar for users of finasteride only (adjusted HR 0.91, 95% CI 0.81–1.03) and dutasteride only (adjusted HR 0.95, 95% CI 0.73–1.24) (Table 4).
Risk of oesophageal squamous cell carcinoma
The risk of oesophageal squamous cell carcinoma was lower in users of 5-ARIs than in non-users (adjusted HR 0.49, 95% CI 0.37–0.65) (Table 2).
Risk of gastric non-cardia adenocarcinoma
The use of 5-ARIs was associated with a slightly decreased point estimate of gastric non-cardia adenocarcinoma, but this was not statistically significant (adjusted HR 0.90, 95% CI 0.80–1.02) (Table 2).
Sensitivity analyses
The HRs for all outcomes remained virtually unchanged in the sensitivity analyses excluding participants entering the cohort in 2005 and without at least 6 months of drug history and also in analyses with censoring of participants who developed any cancer during follow-up (Table 5).
Discussion
This study suggests a decreased risk of oesophageal or cardia adenocarcinoma in men using 5-ARIs with obesity or diabetes diagnoses. The use of 5-ARIs was also associated with a decreased risk of oesophageal squamous cell carcinoma.
Among the strengths of the study are the population-based design, the complete follow-up, and high-quality and prospectively collected data that allowed adjustment for several covariates and stratified analyses. Confounding remains a limitation of this observational study. However, confounding by indication should not be a major issue because 5-ARIs and their indication of prostatic hyperplasia are not associated with the factors associated with any of the studied tumours. Moreover, the results were adjusted for all main risk factors, which did not influence the risk estimates. Yet, due to the lack of detailed data on several risk factors for oesophageal or gastric cancer, e.g. severity of gastro-oesophageal reflux disease and duration and intensity of tobacco smoking, residual confounding cannot be dismissed. Because we used the combined covariate of obesity and diabetes as a proxy for the under-recorded obesity data, we were not able to examine the specific interaction of 5-ARIs use with obesity and/or diabetes. Due to the inherent time-related bias in observational pharmaco-epidemiological studies, particularly because the duration of use or accumulated exposure closely correlate with the follow-up, we did not assess the duration of 5-ARIs use in relation to the risk of oesophageal or gastric cancer. Despite the large size of the cohort, another limitation was a limited statistical power in some of the analyses.
To our knowledge, only one previous study has investigated the associations between 5-ARIs use and the risk of oesophageal and gastric cancer. A Scottish nested case-control study found a reduced overall risk of oesophageal and gastric cancer among users of the 5-ARI finasteride (adjusted OR 0.68, 95% CI 0.50–0.94), but no association remained when oesophageal cancer and gastric cancer were analysed separately [16]. That study lacked data on histological types of the tumours and made no distinction between the sub-sites cardia and non-cardia gastric cancer. In contrast, the present study separately analysed histological types and anatomical sub-sites, which is warranted considering the major differences in aetiology and strengths of the male predominance between these tumours.
An obvious decreased risk of oesophageal or cardia adenocarcinoma was observed in 5-ARI users with obesity or diabetes. This finding suggests interactions between obesity and sex hormonal exposures. Obesity is a well-established risk factor for these tumours and obesity decreases circulating levels of testosterone and dihydrotestosterone [19,20,21]. As indicated by two recent prospective studies, low testosterone levels may increase the risk of oesophageal and cardia adenocarcinoma [9, 10]. Because 5-ARIs decrease levels of dihydrotestosterone with a compensatory effect leading to increased testosterone levels, it is possible that the obese individuals with lowered testosterone levels are more likely to benefit from the potential protective anti-carcinogenic effect of normal or elevated testosterone levels. Yet, the mechanisms are unclear, especially for dihydrotestosterone which is more potent than testosterone in binding to androgen receptors. However, this has not been associated with a risk of oesophageal or cardia adenocarcinoma [10].
A substantially reduced risk of oesophageal squamous cell carcinoma was observed in 5-ARIs users. It has been suggested that sex hormonal factors may play a role also in the aetiology of this tumour. Several studies have reported the expression of androgen receptors in oesophageal squamous cell carcinoma tissue and in vitro studies have shown that testosterone can induce the proliferation of oesophageal squamous cell carcinoma cell lines [22,23,24,25]. However, the epidemiologic evidence regarding associations between sex hormonal exposures and oesophageal squamous cell carcinoma is limited and inconclusive [26,27,28,29,30,31]. The present study indicates the role of anti-androgenic exposure in the aetiology of this cancer.
The results also suggested a weak association between the use of 5-ARIs and the risk of gastric non-cardia adenocarcinoma, although this was not statistically significant. Pre-clinical studies have indicated a limited role of sex hormones in gastric carcinogenesis [32,33,34], and the results of the current study do not support any strong risk reduction associated with 5-ARI use.
In conclusion, this population-based cohort study indicates that 5-ARI use is associated with a decreased risk of oesophageal or cardia adenocarcinoma in individuals with obesity or diabetes and a decreased risk of oesophageal squamous cell carcinoma, while no clear risk reduction was found for gastric non-cardia adenocarcinoma. The available evidence is currently too limited to support any changes in clinical practice or prompt any randomised clinical trials, but more large cohort studies examining the associations between 5-ARI use and the risk of oesophageal and gastric cancer are warranted.
Data availability
Data supporting the results are available upon request.
References
Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2018;68:394–424.
Lagergren J, Smyth E, Cunningham D, Lagergren P. Oesophageal cancer. Lancet. 2017;390:2383–96.
Fitzmaurice C, Akinyemiju TF, Al Lami FH, Alam T, Alizadeh-Navaei R, Allen C, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 29 cancer groups, 1990 to 2016: a systematic analysis for the global burden of disease study. JAMA Oncol. 2018;4:1553–68.
Smyth EC, Nilsson M, Grabsch HI, van Grieken NC, Lordick F. Gastric cancer. Lancet. 2020;396:635–48.
Coleman HG, Xie SH, Lagergren J. The epidemiology of esophageal adenocarcinoma. Gastroenterology. 2018;154:390–405.
Xie SH, Lagergren J. The male predominance in esophageal adenocarcinoma. Clin Gastroenterol Hepatol. 2016;14:338–47.
Derakhshan MH, Liptrot S, Paul J, Brown IL, Morrison D, McColl KE. Oesophageal and gastric intestinal-type adenocarcinomas show the same male predominance due to a 17 year delayed development in females. Gut. 2009;58:16–23.
Petrick JL, Falk RT, Hyland PL, Caron P, Pfeiffer RM, Wood SN, et al. Association between circulating levels of sex steroid hormones and esophageal adenocarcinoma in the FINBAR Study. PLoS ONE. 2018;13:e0190325.
Xie SH, Ness-Jensen E, Rabbani S, Langseth H, Gislefoss RE, Mattsson F, et al. Circulating sex hormone levels and risk of esophageal adenocarcinoma in a prospective study in men. Am J Gastroenterol. 2020;115:216–23.
Petrick JL, Hyland PL, Caron P, Falk RT, Pfeiffer RM, Dawsey SM, et al. Associations between prediagnostic concentrations of circulating sex steroid hormones and esophageal/gastric cardia adenocarcinoma among men. J Natl Cancer Inst. 2019;111:34–41.
Arnold M, Soerjomataram I, Ferlay J, Forman D. Global incidence of oesophageal cancer by histological subtype in 2012. Gut. 2015;64:381–7.
Lou L, Wang L, Zhang Y, Chen G, Lin L, Jin X, et al. Sex difference in incidence of gastric cancer: an international comparative study based on the Global Burden of Disease Study 2017. BMJ Open. 2020;10:e033323.
Goldenberg L, So A, Fleshner N, Rendon R, Drachenberg D, Elhilali M. The role of 5-alpha reductase inhibitors in prostate pathophysiology: Is there an additional advantage to inhibition of type 1 isoenzyme? Can Urol Assoc J. 2009;3:S109–14.
Steers WD. 5alpha-reductase activity in the prostate. Urology. 2001;58:17–24.
Hong SK, Min GE, Ha SB, Doo SH, Kang MY, Park HJ, et al. Effect of the dual 5α-reductase inhibitor, dutasteride, on serum testosterone and body mass index in men with benign prostatic hyperplasia. BJU Int. 2010;105:970–4.
Busby J, Karasneh R, Murchie P, McMenamin Ú, Gadalla SM, Camargo MC, et al. The role of 5α-reductase inhibitors in gastro-oesophageal cancer risk: a nested case-control study. Pharmacoepidemiol Drug Saf. 2020;29:48–56.
Xie SH, Santoni G, Mattsson F, Ness-Jensen E, Lagergren J. Cohort profile: the Swedish Prescribed Drugs and Health Cohort (SPREDH). BMJ Open. 2019;9:e023155.
Eeg-Olofsson K, Miftaraj M, Svensson A-M, Linder, E, Almskog, I, Franzén, S, et al. Nationella Diabetesregistret ÅRSRAPPORT 2020 ÅRS RESULTAT. Västra götalandsregionen: Nationella Diabetesregistret (NDR); 2020.
Sartorius G, Spasevska S, Idan A, Turner L, Forbes E, Zamojska A, et al. Serum testosterone, dihydrotestosterone and estradiol concentrations in older men self-reporting very good health: the healthy man study. Clin Endocrinol. 2012;77:755–63.
Klaassen Z, Howard LE, Moreira DM, Andriole GL Jr, Terris MK, Freedland SJ. Association of obesity-related hemodilution of prostate-specific antigen, dihydrotestosterone, and testosterone. Prostate. 2017;77:466–70.
Amory JK, Wang C, Swerdloff RS, Anawalt BD, Matsumoto AM, Bremner WJ, et al. The effect of 5α-reductase inhibition with dutasteride and finasteride on semen parameters and serum hormones in healthy men. J Clin Endocrinol Metab. 2007;92:1659–65.
Tihan T, Harmon JW, Wan X, Younes Z, Nass P, Duncan KL, et al. Evidence of androgen receptor expression in squamous and adenocarcinoma of the esophagus. Anticancer Res. 2001;21:3107–14.
Kalayarasan R, Ananthakrishnan N, Kate V, Basu D. Estrogen and progesterone receptors in esophageal carcinoma. Dis Esophagus. 2008;21:298–303.
Zhang Y, Pan T, Zhong X, Cheng C. Androgen receptor promotes esophageal cancer cell migration and proliferation via matrix metalloproteinase 2. Tumour Biol. 2015;36:5859–64.
Matsuoka H, Sugimachi K, Ueo H, Kuwano H, Nakano S, Nakayama M. Sex hormone response of a newly established squamous cell line derived from clinical esophageal carcinoma. Cancer Res. 1987;47:4134–40.
Freedman ND, Lacey JV Jr, Hollenbeck AR, Leitzmann MF, Schatzkin A, Abnet CC. The association of menstrual and reproductive factors with upper gastrointestinal tract cancers in the NIH-AARP cohort. Cancer. 2010;116:1572–81.
Bodelon C, Anderson GL, Rossing MA, Chlebowski RT, Ochs-Balcom HM, Vaughan TL. Hormonal factors and risks of esophageal squamous cell carcinoma and adenocarcinoma in postmenopausal women. Cancer Prev Res. 2011;4:840.
Yu H, Liu G, Zhao P, Zhu L. Hormonal and reproductive factors and risk of esophageal cancer in Chinese postmenopausal women: a case-control study. Asian Pac J Cancer Prev. 2011;12:1953–6.
Gallus S, Bosetti C, Franceschi S, Levi F, Simonato L, Negri E, et al. Oesophageal cancer in women: tobacco, alcohol, nutritional and hormonal factors. Br J Cancer. 2001;85:341–5.
Islami F, Cao Y, Kamangar F, Nasrollahzadeh D, Marjani H-A, Shakeri R, et al. Reproductive factors and risk of esophageal squamous cell carcinoma in northern Iran: a case–control study in a high-risk area and literature review. Eur J Cancer Prev. 2013;22:461–6.
Chen Z-H, Shao J-L, Lin J-R, Zhang X, Chen Q. Reproductive factors and oesophageal cancer in Chinese women: a case-control study. BMC Gastroenterol. 2011;11:49.
Gan L, He J, Zhang X, Zhang YJ, Yu GZ, Chen Y, et al. Expression profile and prognostic role of sex hormone receptors in gastric cancer. BMC Cancer. 2012;12:566.
Wu CW, Chi CW, Chang TJ, Lui WY, P’Eng FK. Sex hormone receptors in gastric cancer. Cancer. 1990;65:1396–400.
Zhang BG, Du T, Zang MD, Chang Q, Fan ZY, Li JF, et al. Androgen receptor promotes gastric cancer cell migration and invasion via AKT-phosphorylation dependent upregulation of matrix metalloproteinase 9. Oncotarget. 2014;5:10584–95.
Funding
This study was funded partly by the Swedish Cancer Society (grant number 190043), Swedish Research Council (grant number 2019-00209) and Grant of Science and Technology Development of Fujian Province, China (grant numbers 2019L3006, 2020L2009). Open access funding provided by Karolinska Institute.
Author information
Authors and Affiliations
Contributions
All authors designed the study. JL and SX collected the data for the study. GS analysed the data. SR interpreted the results and drafted the paper. All listed authors revised the paper and approved the final version of the article, including the authorship list. SX is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Corresponding author
Ethics declarations
Competing interests
The authors declare no competing interests.
Ethics approval and consent to participate
This study was approved by the Regional Ethical Review Board in Stockholm (reference number 2018/271-32). The study was performed in accordance with the Declaration of Helsinki.
Consent to publish
Not applicable.
Additional information
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons license, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons license and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this license, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rabbani, S., Santoni, G., Lagergren, J. et al. Use of anti-androgenic 5α-reductase inhibitors and risk of oesophageal and gastric cancer by histological type and anatomical sub-site. Br J Cancer 127, 892–897 (2022). https://doi.org/10.1038/s41416-022-01872-w
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-022-01872-w
