
Abstract
Background
Preoperative chemotherapy containing anthracyclines and taxanes is well established in early-stage breast cancer. Previous studies have suggested that the chemotherapy sequence may matter but definitive evidence is missing. ABCSG trial 34 evaluated the activity of the MUC1 vaccine tecemotide when added to neoadjuvant treatment; the study provided the opportunity for the second randomisation to compare two different anthracycline/taxane sequences.
Methods
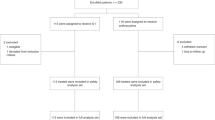
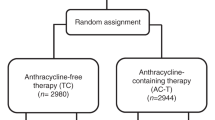
HER2-negative early-stage breast cancer patients were recruited to this randomised multicentre Phase 2 study. Patients in the chemotherapy cohort (n = 311) were additionally randomised to a conventional or reversed sequence of epirubicin/cyclophosphamide and docetaxel. Residual cancer burden (RCB) with/without tecemotide was defined as primary study endpoint; RCB in the two chemotherapy groups was a key secondary endpoint.
Results
No significant differences in terms of RCB 0/I (40.1% vs. 37.2%; P = 0.61) or pathologic complete response (pCR) rates (24.3% vs. 25%, P = 0.89) were observed between conventional or reverse chemotherapy sequence. No new safety signals were reported, and upfront docetaxel did not result in decreased rates of treatment delay or discontinuation.
Conclusion
Upfront docetaxel did not improve chemotherapy activity or tolerability; these results suggest that upfront neoadjuvant treatment with anthracyclines remains a valid option.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 24 print issues and online access
$259.00 per year
only $10.79 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout



Similar content being viewed by others

References
Bonadonna, G. Karnofsky memorial lecture. Conceptual and practical advances in the management of breast cancer. J. Clin. Oncol. 7, 1380–1397 (1998).
Kaufmann, M., von Minckwitz, G., Bear, H. D., Buzdar, A., McGale, P., Bonnefoi, H. et al. Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: new perspectives 2006. Ann. Oncol. 18, 1927–1934 (2007).
Bear, H. D., Anderson, S., Smith, R. E., Geyer, C. E. Jr., Mamounas, E. P., Fisher, B. et al. Sequential preoperative or postoperative docetaxel added to preoperative doxorubicin plus cyclophosphamide for operable breast cancer: National Surgical Adjuvant Breast and Bowel Project Protocol B-27. J. Clin. Oncol. 24, 2019–2027 (1999).
von Minckwitz, G., Untch, M., Blohmer, J. U., Costa, S. D., Eidtmann, H., Fasching, P. A. et al. Definition and impact of pathologic complete response on prognosis after neoadjuvant chemotherapy in various intrinsic breast cancer subtypes. J. Clin. Oncol. 30, 1796–1804 (2012).
Cortazar, P., Zhang, L., Untch, M., Mehta, K., Costantino, J. P., Wolmark, N. et al. Pathological complete response and long-term clinical benefit in breast cancer: the CTNeoBC pooled analysis. Lancet 384, 164–172 (2014).
Symmans, W. F., Peintinger, F., Hatzis, C., Rajan, R., Kuerer, H., Valero, V. et al. Measurement of residual breast cancer burden to predict survival after neoadjuvant chemotherapy. J. Clin. Oncol. 25, 4414–4422 (2007).
Wildiers, H., Forceville, K., Paridaens, R. & Joensuu, H. Taxanes and anthracyclines in early breast cancer: which first? Lancet Oncol. 11, 219–220 (2010).
Alvarez, R. H., Bianchini, G., Hsu, L., Cristofanilli, M., Esteva, F. J., Pusztai, L. et al. Clinical outcome of two sequences of administering paclitaxel (P) and anthracyclines (A) as primary systemic therapy (PST) and adjuvant chemotherapy (ACT) in breast cancer (BC) patients: a retrospective analysis from the M. D. Anderson Cancer Center (MDACC). Cancer Res. 70(24 Suppl), 384s (2010).
Puhalla, S., Mrozek, E., Young, D., Ottman, S., McVey, A., Kendra, K. et al. Randomized phase II adjuvant trial of dose-dense docetaxel before or after doxorubicin plus cyclophosphamide in axillary node-positive breast cancer. J. Clin. Oncol. 26, 1691–1697 (2008).
Guo, B., Villeneuve, D. J., Hembruff, S. L., Kirwan, A. F., Blais, D. E., Bonin, M. et al. Cross-resistance studies of isogenic drug-resistant breast tumor cell lines support recent clinical evidence suggesting that sensitivity to paclitaxel may be strongly compromised by prior doxorubicin exposure. Breast Cancer Res. Treat. 85, 31–51 (2004).
Chang, B. D., Broude, E. V., Dokmanovic, M., Zhu, H., Ruth, A., Xuan, Y. et al. A senescence-like phenotype distinguishes tumor cells that undergo terminal proliferation arrest after exposure to anticancer agents. Cancer Res. 59, 3761–3767 (1999).
Ewald, J. A., Desotelle, J. A., Wilding, G. & Jarrard, D. F. Therapy-induced senescence in cancer. J. Natl Cancer Inst. 102, 1536–1546 (2010).
Camara, O., Rengsberger, M., Egbe, A., Koch, A., Gajda, M., Hammer, U. et al. The relevance of circulating epithelial tumor cells (CETC) for therapy monitoring during neoadjuvant (primary systemic) chemotherapy in breast cancer. Ann. Oncol. 18, 1484–1492 (2007).
Singer, C. F., Pfeiler, G., Hubalek, M., Bartsch, R., Stöger, H., Pichler, A. et al. Efficacy and safety of the therapeutic cancer vaccine tecemotide (L-BLP25) in early breast cancer: results from a prospective, randomized, neoadjuvant Phase II Study (ABCSG 34). Eur. J. Cancer 132, 43–52 (2020).
Sledge, G. W., Neuberg, D., Bernardo, P., Ingle, J. N., Martino, S., Rowinsky, E. K. et al. Phase III trial of doxorubicin, paclitaxel, and the combination of doxorubicin and paclitaxel as front-line chemotherapy for metastatic breast cancer: an intergroup trial (E1193). J. Clin. Oncol. 21, 588–592 (2003).
Murtaza, M., Dawson, S. J., Pogrebniak, K., Rueda, O. M., Provenzano, E., Grant, J. et al. Multifocal clonal evolution characterized using circulating tumour DNA in a case of metastatic breast cancer. Nat. Commun. 6, 8760 (2015).
Earl, H. M., Vallier, A. L., Hiller, L., Fenwick, N., Young, J., Iddawela, M. et al. Effects of the addition of gemcitabine, and paclitaxel-first sequencing, in neoadjuvant sequential epirubicin, cyclophosphamide, and paclitaxel for women with high-risk early breast cancer (Neo-tAnGo): an open-label, 2×2 factorial randomised phase 3 trial. Lancet Oncol. 15, 201–212 (2014).
Buzdar, A. U., Suman, V. J., Meric-Bernstam, F., Leitch, A. M., Ellis, M. J., Boughey, J. C. et al. Fluorouracil, epirubicin, and cyclophosphamide (FEC-75) followed by paclitaxel plus trastuzumab versus paclitaxel plus trastuzumab followed by FEC-75 plus trastuzumab as neoadjuvant treatment for patients with HER2-positive breast cancer (Z1041): a randomised, controlled, phase 3 trial. Lancet Oncol. 14, 1317–1325 (2013).
Staems, V., Singh, B., Tsangaris, T., Crawford, J. G., Novielli, A., Ellis, M. J. et al. A prospective randomized pilot study to evaluate predictors of response in serial core biopsies to single agent neoadjuvant doxorubicin or paclitaxel for patients with locally advanced breast cancer. Clin. Cancer Res 9, 124–133 (2003).
Taghian, A. G., Abi-Raad, R., Assaad, S. I., Casty, A., Ancukiewicz, M., Yeh, E. et al. Paclitaxel decreases the interstitial fluid pressure and improves oxygenation in breast cancers in patients treated with neoadjuvant chemotherapy: clinical implications. J. Clin. Oncol. 23, 1951–1961 (2005).
Miller, K. D., Soule, S. E., Calley, C., Emerson, R. E., Hutchins, G. D., Kopecky, K. et al. Randomized phase II trial of the anti-angiogenic potential of doxorubicin and docetaxel; primary chemotherapy as Biomarker Discovery Laboratory. Breast Cancer Res. Treat. 89, 187–197 (2005).
Thiery-Vuillemin, A., Llombart-Cussac, A., Chaigneau, L., Villanueva, C., Bazan, F., Montcuquet, P. et al. Sequential taxane and anthracycline-containing neoadjuvant regimens: the sequential order impact. Breast 20, 46–49 (2011).
Cardoso, F., Ferreira Filho, A. F., Crown, J., Dolci, S., Paesmans, M., Riva, A. et al. Doxorubicin followed by docetaxel versus docetaxel followed by doxorubicin in the adjuvant treatment of node positive breast cancer: results of a feasibility study. Anticancer Res. 21, 789–795 (2001).
Piedbois, P., Serin, D., Priou, F., Laplaige, P., Greget, S., Angellier, E. et al. Dose-dense adjuvant chemotherapy in node-positive breast cancer: docetaxel followed by epirubicin/cyclophosphamide (T/EC), or the reverse sequence (EC/T), every 2 weeks, versus docetaxel, epirubicin and cyclophosphamide (TEC) every 3 weeks. AERO B03 randomized phase II study. Ann. Oncol. 18, 52–57 (2007).
Wildiers, H., Dirix, L., Neven, P., Prové, A., Clement, P., Squifflet, P. et al. Delivery of adjuvant sequential dose-dense FEC-Doc to patients with breast cancer is feasible, but dose reductions and toxicity are dependent on treatment sequence. Breast Cancer Res. Treat. 114, 103–112 (2009).
Zaheed, M., Wilcken, N., Willson, M. L., O’Connell, D. L. & Goodwin, A. Sequencing of anthracyclines and taxanes in neoadjuvant and adjuvant therapy for early breast cancer. Cochrane Database Syst. Rev. CD012873 (2019).
Untch, M., Jackisch, C., Schneeweiss, A., Conrad, B., Aktas, B., Denkert, C. et al. Nab-paclitaxel versus solvent-based paclitaxel in neoadjuvant chemotherapy for early breast cancer (GeparSepto-GBG 69): a randomised, phase 3 trial. Lancet Oncol. 17, 345–356 (2016).
Loibl, S., O’Shaughnessy, J., Untch, M., Sikov, W. M., Rugo, H. S., McKee, M. D. et al. Addition of the PARP inhibitor veliparib plus carboplatin or carboplatin alone to standard neoadjuvant chemotherapy in triple-negative breast cancer (BrighTNess): a randomised, phase 3 trial. Lancet Oncol. 19, 497–509 (2018).
Acknowledgements
The authors would like to thank Dr. Martina Putz for her support in preparing the final version of this paper.
Author information
Authors and Affiliations
Consortia
Contributions
Conception and design: C.S., R.B., P.D., F.F., M.G. and M.H. Development of methodology: V.B.R., P.D., M.F., S.F., M.G., R.G., Z.B.H. and M.R. Acquisition of the data: all authors. Interpretation of the data: all authors. Paper writing: all authors. Paper approval: all authors.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
The study was conducted according to the principles of the Declaration of Helsinki and the ICH Guidelines for Good Clinical Practice. The protocol was conducted under EU directive 2001/20/EC and approved by the Ethics Committee of the Medical University of Vienna, Borschkegasse 8b/6, A-1090 Vienna, Austria, as the leading ethics committee. All subjects provided their written informed consent to participate in the study.
Consent to publish
Not applicable.
Data availability
As the regulatory sponsor of this trial, ABCSG has data sovereignty and individual participant data (including de-identified participant data, participant data with identifiers, data dictionary or other specified datasets) will not be shared.
Competing interests
R.B. reports advisory roles at AstraZeneca, Celgene, Daiichi, Eisai, Eli-Lilly, MSD, Novartis, Pfizer, Pierre-Fabre, Puma, Roche, Samsung, lecture honoraria: Accord, AstraZeneca, BMS, Celgene, Eli-Lilly, Novartis, Pfizer, Pierre-Fabre, Roche, Sandoz and received research support from Daiichi, Novartis and Roche, all outside of the submitted work. M.H. reports honoraria and/or travel support from Amgen, AstraZeneca, Celgene, Eli-Lilly, Pfizer, Novartis, Roche all outside the submitted work. A.L.P. reports honoraria and/or travel support from Abbvie, Amgen, AstraZeneca, Bayer, Celgene, Gilead, Janssen, Eli-Lilly, MSD, Pfizer, Novartis, Roche, Sanofi and Takeda all outside the submitted work. D.E. reports honoraria/travel support from Amgen, AstraZeneca, Celgene, Eli-Lilly, MSD, Novartis, Pfizer, Roche and Myriad all outside of the submitted work. M.F. has received honoraria for advisory boards from AstraZeneca, Bayer, Biomedica, Boehringer Ingelheim, Eli-Lilly, Merck Sharp & Dohme, Myriad Genetics Inc., Pfizer and Roche. M.G. reports personal fees/travel support from Amgen, AstraZeneca, Celgene, Eli-Lilly, Invectys, Pfizer, Novartis, Puma, Nanostring, Roche, Medison, LifeBrain, all outside the submitted work; an immediate family member is employed by Sandoz. Z.B.-H. has advisory roles at Biomedica, Roche and Novartis, received lecture honoraria and travel support from Roche and research support from Boehringer Ingelheim. C.F.S., G.P., H.S., A.P., E.P., V.B.-R., R.G., M.R., M.K.T., V.W., P.S., P.D., F.F., R.E., R.J., M.B., C.T. and S.F. declare no competing interests.
Funding information
This study was supported by Merck KGaA, Darmstadt, Germany. The academic non-profit organisation ABCSG was the regulatory sponsor of this trial. Merck provided financial funding and tecemotide. The study was designed and conducted by ABCSG. Merck was not involved in the collection, management, analysis and interpretation of the data. ABCSG prepared and approved the paper and decided to submit the paper for the publication.
Additional information
Note This work is published under the standard license to publish agreement. After 12 months the work will become freely available and the license terms will switch to a Creative Commons Attribution 4.0 International (CC BY 4.0).
Publisher’s note Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Supplementary information
Rights and permissions
About this article

Cite this article
Bartsch, R., Singer, C.F., Pfeiler, G. et al. Conventional versus reverse sequence of neoadjuvant epirubicin/cyclophosphamide and docetaxel: sequencing results from ABCSG-34. Br J Cancer 124, 1795–1802 (2021). https://doi.org/10.1038/s41416-021-01284-2
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41416-021-01284-2
This article is cited by
-
The future of clinical trials—goals, ideas, and discussion
memo - Magazine of European Medical Oncology (2024)
-
Differential immunomodulatory effects of epirubicin/cyclophosphamide and docetaxel in breast cancer patients
Journal of Experimental & Clinical Cancer Research (2023)
