
Abstract
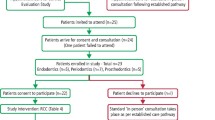
The COVID-19 outbreak has caused many challenges for the dental profession and workforce. With the suspension of routine dental services at the end of March 2020, there is a significant number of the general population with acute dental problems. In addition to these, there are patients who had treatment suspended partway through their treatment plans and therefore there is now a backlog of patients awaiting dental care. One challenge that will face the profession moving forward will be facilitating access to these patients and determining which patients should be seen as a priority for necessary dental care. This article looks at the role of real-time interactive video consultations in dental practice during the recovery and restoration phase of the COVID-19 outbreak and how they could facilitate the management of patients waiting to access dental care.
Similar content being viewed by others
Key points
-
Highlights the benefits of the use of real-time interactive video consultations over phone consultations alone.
-
Emphasises the uses that real-time interactive video consultations will have in the recovery and restoration phase of the COVID-19 outbreak.
-
Demonstrates the uses of real-time interactive video consultations in wider areas of dentistry, including with anxious patients or to review non-urgent stable patients.
-
Suggests the need for 'fit-for-purpose' video consultation solutions for primary care dental services.
Background
The World Health Organisation1 describes 'telehealth' as the delivery of healthcare (in real-time or asynchronously) by a service provider to a patient, when the two individuals are separated by distance, often using information technology (IT) systems for exchange of information. Telemedicine (a synonym for telehealth) and its use to improve healthcare access to patients has been discussed since the 1990s.1,2,3 With the more recent COVID-19 outbreak, more than ever, real-time interactive video consultations are being utilised by healthcare practitioners to deliver care and advice to patients. This 'real-time' approach is live and delivered synchronously while other forms of telehealth are delivered asynchronously.1 An example of this is a patient query delivered to an e-mail inbox which is managed at a later time point.
Current literature suggests a high satisfaction from both healthcare staff and service users.4 It also demonstrates that there is no difference in disease progression and that there are lower costs involved in this type of interaction, compared to traditional interactions.5,6 As discussed by Greenhalgh et al.,7 these studies focused on stable patients with chronic conditions, yet video consultations have had a role in management of acute conditions during this outbreak. Many studies also focus on secondary care environments and uptake of such techniques in primary care have tended to be low, but the benefits such as rapport building and convenience have been highlighted in a recent systematic review.8,9 The General Dental Council have highlighted how remote consultations online, via phone or via video can help to meet the demand by the public for more convenient access to healthcare. They also note a benefit on resources and to patients.10
The move to real-time interactive video consultations in the current climate has been a swift response based on the crisis that healthcare practitioners have found themselves in during COVID-19. Adaptation to this change in patient management can be difficult, considering that doctor-patient/dentist-patient face-to-face interactions have so far been the established method of healthcare. Although real-time interactive video consultations are superior to phone consultations, it is not felt to be a substitute for face-to-face interactions.11 Greenhalgh et al.12 described the potential shown by online platforms to deliver video-based patient interactions.
Real-time interactive video consultations are now integrated within healthcare systems of countries such as the United States and Australia.11 A number of trials have demonstrated that real-time interactive video consultations have a role within the healthcare settings and, in these cases, have also shown a benefit over simple mobile consultations.13,14 A more recent study by Randhawa et al.11 showed that video consultation was felt to be useful to general medical practitioners (GMPs), but perhaps was more appropriate to particular patient groups. A study carried out in primary care suggested that the demand for such consultation methods was likely to increase, but there was a need for improved technical infrastructure and case selection was imperative.15
Limitations
There are limitations to real-time interactive video consultations in diagnosing disease and assessing patient problems, particularly in a dental context. Clinicians can often be the biggest barrier to implementation, being resistant to change as a result of numerous influencing factors, having hesitations towards the quality of the patient interactions and being apprehensive of any technical difficulties.11,16
It is likely that dental teams will have hesitation and questions regarding a video consultation solution; examples are highlighted in Figure 1. Information governance regulations may cause clinicians to be anxious towards the privacy of real-time interactive video consultations. With litigation rates for dentists high, many will also be concerned about the liability they will hold should something go wrong, and there could be concerns surrounding a patient recording the consultation and the medico-legal implications that could have. In addition, clinical teams need to have confidence that a real-time video consultation solution is not going to have a large financial impact on an already stretched service; therefore, processes need to be in place for appropriate reimbursement or funding. In secondary care, NHS England and NHS Improvement have agreed that providers will have an equal tariff for both video consultations and face-to-face attendances.17

Potential questions that may be raised by clinicians and dental teams
Regarding information governance requirements, NHSX encourage the use of real-time interactive video consultations, and the benefit of reducing transmission of COVID-19 has been highlighted by them. NHSX have stated that it is permissible to use platforms such as Skype, WhatsApp and FaceTime on personal devices (where there is no practical alternative) in the short term, in response to COVID-19. However, these are not specifically designed for purpose, and consideration needs to be given to patient confidentiality and storage of patient information. Consent by patients is implied through their acceptance to participate in a video consultation.18 The Information Commissioners Office also confirms that data protection and electronic communication laws do not hinder the ability of the NHS to use technology to deliver consultations to patients.19
Dentistry involves assessment and examination of the oral cavity. One limitation to real-time interactive video consultations in this context would be the difficulty in assessing the dentition and soft tissues, particularly in the posterior oral cavity. Considerations also need to be given to the image quality, the reliability of internet connection and patient factors such as ability to connect to the software delivering real-time interactive video consultations, lighting, manual dexterity, familiarity with mobile/tablet devices and the technology literacy of the service user to utilise technology-based consultations.11 There is, however, the ability to assess (to an extent) extraoral and intraoral swellings, grossly carious teeth, soft tissue lesions, mobile teeth, fractured prosthodontic work and orthodontic emergencies (Table 1). Additionally, the limitation of poor image quality and access could be mitigated through a combined approach, utilising real-time video with a 'store-and-forward' (asynchronous) approach.1
The ability to deliver advice and reassurance in some of these cases where immediate dental care is not required is imperative considering the likely demand on dental services as COVID-19 restrictions are eased. One area of assessment that would be challenging through a video platform is soft tissue lesions, and risk assessment has to be utilised to determine if a patient needs to be seen clinically. The texture of a lesion and its effect on adjacent structures cannot be ascertained from real-time interactive video consultations alone and can only be effectively assessed by clinical palpation. In addition, pigmented lesions may not present accurately in colour, leading to misdiagnosis.20 Therefore, video conferencing has a limited role in these cases and should be used with care.
Role within dental services
With uncertainty surrounding infection control requirements and social distancing principles as routine dentistry resumes, use of real-time interactive video consultations will likely play a key role in pre-assessment of patients. This could involve undertaking a history, updating the medical and social history, and discussing the likely treatment options and costs of treatment before the patient attends the clinic. This would not only reduce the time spent within the clinic, but would also give the patient sufficient time to consider the options before treatment commences.21 In those that are shielding or vulnerable, this would further limit their risk. There is potential for this patient care model to utilise skill mix within the dental team, with pre-appointment assessments carried out by an appropriately trained dental care professional, while the dentist continues to treat patients.
Extraoral lesions and swellings are one aspect of video consultation that does not rely heavily on a good-quality intraoral picture. Real-time interactive video consultations allow clinicians to assess the extent of extraoral swellings as well as make an assessment of systemic involvement (albeit limited) to determine the best place of care for a patient - either primary or secondary care. This in itself can reduce patient travel, reduce clinical time for a patient and clinician, and ensure the patient is directed to the service that is most appropriate to them; both patients and clinicians are likely to appreciate this. As discussed previously, use of colour photographs shared by a patient, asynchronously, alongside a real-time consultation could help to mitigate the issues with assessments of intraoral lesions.
There is the potential for real-time interactive video consultations to have a role within dentistry past the provision of emergency triage and the COVID-19 outbreak. Video consultations can be useful for anxious patients, inviting them to a virtual tour of the environment and introducing them to treating staff before them attending. Building rapport and reducing the anxiety of the unknown can significantly improve a patient's ability to accept treatment.22 Dental services can also utilise real-time interactive video consultations before domiciliary visits, giving them the opportunity to risk-assess the environment and to learn vital information about the patient and likely treatment required. Special care dentistry and community dental services can utilise video consultation solutions to determine the extent of a patient's impairment or disability, as well as their likely compliance with treatment. This can give services key information about the equipment they will be required to take into a patient's home, as well as (once again) limiting patient contact time.
In orthodontics, video consultations may play a significant role in reviewing non-urgent cases. Utilising this method of review, clinical time can be prioritised for those patients who require interventional treatment and those who have suffered problems during the COVID-19 outbreak. This concept could be applied to other specialities and used in the same way, to reduce footfall within practices and allow clinicians to begin clearing the backlog of patients that have accumulated.
Previously dentistry has been focused on treatment-orientated approaches, with lesser focus on oral health education. Video consultations in the longer term have a significant role to play in providing prevention advice and enabling the use of skill mix within the profession, with perhaps trained dental nurses delivering oral health advice specific to a patient's needs via a real-time video link. Visual cues can be picked up and advantages such as assessment of inhaler technique in medicine could be transferred to the dental setting in consideration of a patient's brushing technique, for example.23 Groups such as preschool children, older adults and patients located in rural areas (although limited by internet bandwidth) could benefit heavily from access to preventative messages through these means, considering the convenience and practicality for them. It would lessen the burden on clinicians and reduce clinical contact time within surgeries. A real-time video interaction could also work well with groups including antenatal classes, care homes, schools and hospital staff helping to educate and promote oral hygiene, with an ability to answer questions in a timely manner. Within telehealth, there is an opportunity for providing training (either clinical or non-clinical) and video consultations could provide a platform via which this could be delivered.
Once simple, real-time video consultation solutions are implemented, thoughts could be given to a whole system approach, similar to that of GPs, including ability for triage questionnaires to elicit dental problems and urgency, as well as the possibilities for remote prescribing, which has also come to the forefront during this outbreak. Integration of these systems within dentistry will ensure it is in keeping with that of GP services and will help to provide a more standardised approach to healthcare past the outbreak. When developed, links to consultants via video link could ease patient referrals into secondary care services, as an opinion can be sought 'there and then' through a solution such as Consultant Connect.24
Video consultation solutions for dentistry
The NHS has a selection of approved video consultation suppliers. Commissioners and GMP practices are able to select from the selected suppliers through the Digital Care Services (DCS) Framework. This service is deemed to be centrally funded and is therefore free of charge for GMP practices. The NHS reports that 'most GP practices, hospitals, mental health services and community care services' are now able to offer video consultations.25 Video consultations have been embedded within community care for some time and have shown considerable advantages in reducing strains on GP services as well as accident and emergency travel.23 Within dentistry, the NHS may have the potential to fund a pilot to confirm its use in service provision; however, future funding would be subject to further confirmation. Clinical commissioning groups and strategic transformation partnerships (STPs) can also access such services (selected through procurement processes) via the NHS England Dynamic Purchasing System (DPS).18 Between 2019 and 2020, £16 million was made available to STPs to support online consultations.23 In response to COVID-19, the need for mini-competition has been eliminated to facilitate implementation. NHS Digital gives assurance for the products to be appropriate for use in general practice and that there is flexibility on the supplier selected if found not to be 'fit for purpose'.18
Any video consultation solution for dentistry would likely require a number of features for both patients and clinicians (Table 2).
There are a number of video consultation solutions and some that are already working successfully within other areas of healthcare. Considerations need to be given before commissioning of these services for dental services. Some supplier systems require Health and Social Care Network (HSCN) connections and some suppliers also require access via NHS smartcards. Most dentists do not have access to this, so once again, economically and practically, these would not be an effective system to implement for dental services in the near future. Some solutions require the patient's NHS number - although not necessarily accessible for all dental patients automatically, this can be sought by asking the patient or the patient's GMP. Many video solutions proposed by the DCS framework integrate into a wider online system to access medical records such as the summary care records. However, these appear to be tailored to medical practitioners and primary care dental services are yet to be integrated within this. Utilising a system like this could incur significant delay at a time when a solution is required within a tight timeline. NHS England and NHS Improvement have already procured an 'Attend Anywhere' model for 12 months as a solution for NHS Trusts and Foundation Trusts to deliver care in secondary care settings through the video consultation platform.26 In Wales, this same solution is being utilised in GP practices and is being rolled out in primary care.27
The ophthalmology sector have advocated the use of video consultations during this outbreak.28 Their guidance looks at third-party systems, which have variable fees, subscription approaches and licensing requirements, but can be adapted for use.23,28 However, those approved by the NHS have already been approved and conform to required technical standards.29 Outside of the GP IT Futures framework, but included in the rapid procurement process via DPS, Boots UK have been utilising a video consultation service through the LIVI video consultation platform.30,31 LIVI has been partnering with GP practices to offer the ability of video consultations, and in March 2020, they launched a web-based platform which is available in ten different languages.30
Conclusion
With the current situation rapidly evolving, the need for dental services to have access to a video consultation solution to deliver a higher quality triaging service, allowing for services to be effectively provided to those most requiring it, will be vital. NHS England and NHS Improvement have highlighted their commitment to transforming outpatient attendances, as set out in the NHS Long Term Plan.32 That involves improving patient choice, including having the ability to choose to have a video consultation over a traditional face-to-face visit. The recommendation for NHS dental services to utilise a video consultation service will help with limiting patient contact in the recovery and restoration phase of the COVID-19 outbreak, as well as beyond this. This will provide practices with the ability to manage the backlog of patients who are currently unable to access dental care and to appropriately prioritise those that have acute problems requiring treatment, thereby facilitating the return of routine dental care over time.
References
World Health Organisation. Global diffusion of eHealth: Making universal health coverage achievable. 2016. Available online at https://www.who.int/goe/publications/global_diffusion/en/ (accessed July 2020).
McLaren P, Ball C J. Telemedicine: Lessons Remain unheeded. BMJ 1995; 310: 1390-1391.
Wootton R. Telemedicine in the National Health Service. J R Soc Med 1998; 91: 614-621.
Mair F, Whitten P. Information in practice. Br Med J 2000; 320: 1517-1520.
Armfield N R, Bradford M, Bradford N K. The clinical use of Skype - For which patients, with which problems and in which settings? A snapshot review of the literature. Int J Med Inform 2015; 84: 737-742.
Ignatowicz A, Atherton H, Bernstein C J et al. Internet videoconferencing for patient-clinician consultations in long-term conditions: A review of reviews and applications in line with guidelines and recommendations. Digit Heal 2019; 5: 1-27.
Greenhalgh T, Wherton J, Shaw S, Morrison C. Video consultations for covid-19. BMJ 2020; 368: 1-2.
Thiyagarajan A, Grant C, Griffiths F, Atherton H. Exploring patients' and clinicians' experiences of video consultations in primary care: a systematic scoping review. BJGP Open 2020; DOI: 10.3399/bjgpopen20X101020.
Brant H, Atherton H, Ziebland S, McKinstry B, Campbell J L, Salisbury C. Using alternatives to facetoface consultations: A survey of prevalence and attitudes in general practice. Br J Gen Pract 2016; DOI: 10.3399/bjgp16X685597.
General Dental Council. High level principles for good practice in remote consultations and prescribing. 2020. Available at https://www.gdc-uk.org/docs/default-source/guidance-documents/high-level-principles-remote-consultations-and-prescribing.pdf (accessed July 2020).
Randhawa R S, Chandan J S, Thomas T, Singh S. An exploration of the attitudes and views of general practitioners on the use of video consultations in a primary healthcare setting: a qualitative pilot study. Prim Heal Care Res Dev 2019; DOI: 10.1017/S1463423618000361.
Greenhalgh T, Vijayaraghavan S, Wherton J et al. Virtual online consultations: Advantages and limitations (VOCAL) study. BMJ Open 2016; DOI: 10.1136/bmjopen-2015-009388.
Capampangan D J, Wellik K E, Bobrow B J et al. Telemedicine Versus Telephone for Remote Emergency Stroke Consultations: A Critically Appraised Topic. Neurologist 2009; 15: 163-166.
Handschu R, Scibor M, Willaczek B et al. Telemedicine in acute stroke: Remote video-examination compared to simple telephone consultation. J Neurol 2008; 255: 1792-1797.
Donaghy E, Atherton H, Hammersley V et al. Acceptability, benefits, and challenges of video consulting: A qualitative study in primary care. Br J Gen Pract 2019; DOI: 10.3399/bjgp19X704141.
Watt R, McGlone P, Evans D et al. The facilitating factors and barriers influencing change in dental practice in a sample of English general dental practitioners. Br Dent J 2004; 197: 485-489.
NHS England and NHS Improvement. Clinical guide for the management of remote consultations and remote working in secondary care during the coronavirus pandemic. 2020. Available at https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/C0044-Specialty-Guide-Virtual-Working-and-Coronavirus-27-March-20.pdf (accessed July 2020).
NHS Digital. Approved video consultation systems. 2020. Available at https://digital.nhs.uk/services/future-gp-it-systems-and-services/approved-econsultation-systems (accessed July 2020).
Information Commissioner's Office. Data protection and coronavirus. 2020. Available at https://ico.org.uk/about-the-ico/news-and-events/news-and-blogs/2020/03/data-protection-and-coronavirus/ (accessed May 2020).
Khoury Z H, Sultan A S. Tele-Oral Oncology: Reinvigorating Telemedicine in Oral Cancer Care. J Cancer Allied Spec 2020; DOI: 10.37029/jcas.v6i1.299.
General Dental Council. Standards for the Dental Team. 2013. Available at https://standards.gdc-uk.org/Assets/pdf/Standards%20for%20the%20Dental%20Team.pdf (accessed July 2020).
Newton T, Asimakopoulou K, Daly B, Scambler S, Scott S. The management of dental anxiety: Time for a sense of proportion? Br Dent J 2012; 213: 271-274.
Bakhai M, Croney L, Waller O, Henshall N, Felstead C. Using Online Consultations In Primary Care: Implementation Toolkit. 2020. Available at https://www.england.nhs.uk/wp-content/uploads/2020/01/online-consultations-implementation-toolkit-v1.1-updated.pdf (accessed July 2020).
Consultant Connect. COVID-19 Recovery: 8 ways we can help. 2020. Available at https://www.consultantconnect.org.uk/wp-content/uploads/2020/05/COVID-recovery-One-pager-7.pdf (accessed July 2020).
NHS. Video Consultations. 2020. Available at https://www.nhs.uk/using-the-nhs/nhs-services/gps/video-consultations/ (accessed June 2020).
NHS England and NHS Improvement. Rapid scale up of video consultations in NHS trusts and foundation trusts. 2020. Available at https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/04/C0161-letter-to-royal-colleges-14-april-2020.pdf (accessed July 2020).
All Wales Clinical Dental Leads COVID-19 Group. Novel Coronavirus (C-19): De-escalation Standard Operating Processes for Primary Dental Care Settings in Wales. 2020. Available at https://bda.org/advice/Coronavirus/Documents/Wales%20de-escalation%20SOP.pdf (accessed July 2020).
Ghadiri N. Telemedicine Applications for Ophthalmology Consultations during a Pandemic Emergency. 2020. Available at https://www.rcophth.ac.uk/wp-content/uploads/2020/03/Telemedicine-Options-for-Ophthalmology-Consultations-COVID19.pdf (accessed July 2020).
British Medical Association. COVID-19: video consultations and homeworking. 2020. Available at https://www.bma.org.uk/advice-and-support/covid-19/adapting-to-covid/covid-19-video-consultations-and-homeworking (accessed June 2020).
NHS Support Federation. LIVI. 2020. Available online at https://www.nhsforsale.info/private-providers/livi/ (accessed July 2020).
NHS England and NHS Improvement. Procurement of pre-approved suppliers of online and video consultation systems for GP practices to support COVID-19. 2020. Available at https://www.england.nhs.uk/coronavirus/wp-content/uploads/sites/52/2020/03/C0079-Suppliers-of-online-and-video-consultations.pdf (accessed July 2020).
NHS. The NHS Long Term Plan. 2019. Available online at https://www.longtermplan.nhs.uk/publication/nhs-long-term-plan/ (accessed July 2020).
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article

Cite this article
Patel, T., Wong, J. The role of real-time interactive video consultations in dental practice during the recovery and restoration phase of the COVID-19 outbreak. Br Dent J 229, 196–200 (2020). https://doi.org/10.1038/s41415-020-1918-7
Published:
Issue Date:
DOI: https://doi.org/10.1038/s41415-020-1918-7
This article is cited by
-
Usefulness of Telemedicine for Disabled Children Receiving Feeding Therapy
Dysphagia (2023)
-
Establishment of Neural Series Transmission Keys (NSTKs) and Security in the Field of COVID-19 Telepediatric Oral Health
Wireless Personal Communications (2023)
-
Virtual consultations for oral surgery patients
BMC Oral Health (2022)
-
Teledentistry during COVID-19 pandemic: scientometric and content analysis approach
BMC Health Services Research (2022)
-
An evaluation of the impact of COVID-19 on the leadership behaviour of dental practice managers in England
BDJ Team (2022)
